A Randomized Clinical Trial to Evaluate the Effect of Canephron N in Comparison to Ciprofloxacin in the Prevention of Postoperative Lower Urinary Tract Infections after Midurethral Sling Surgery

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
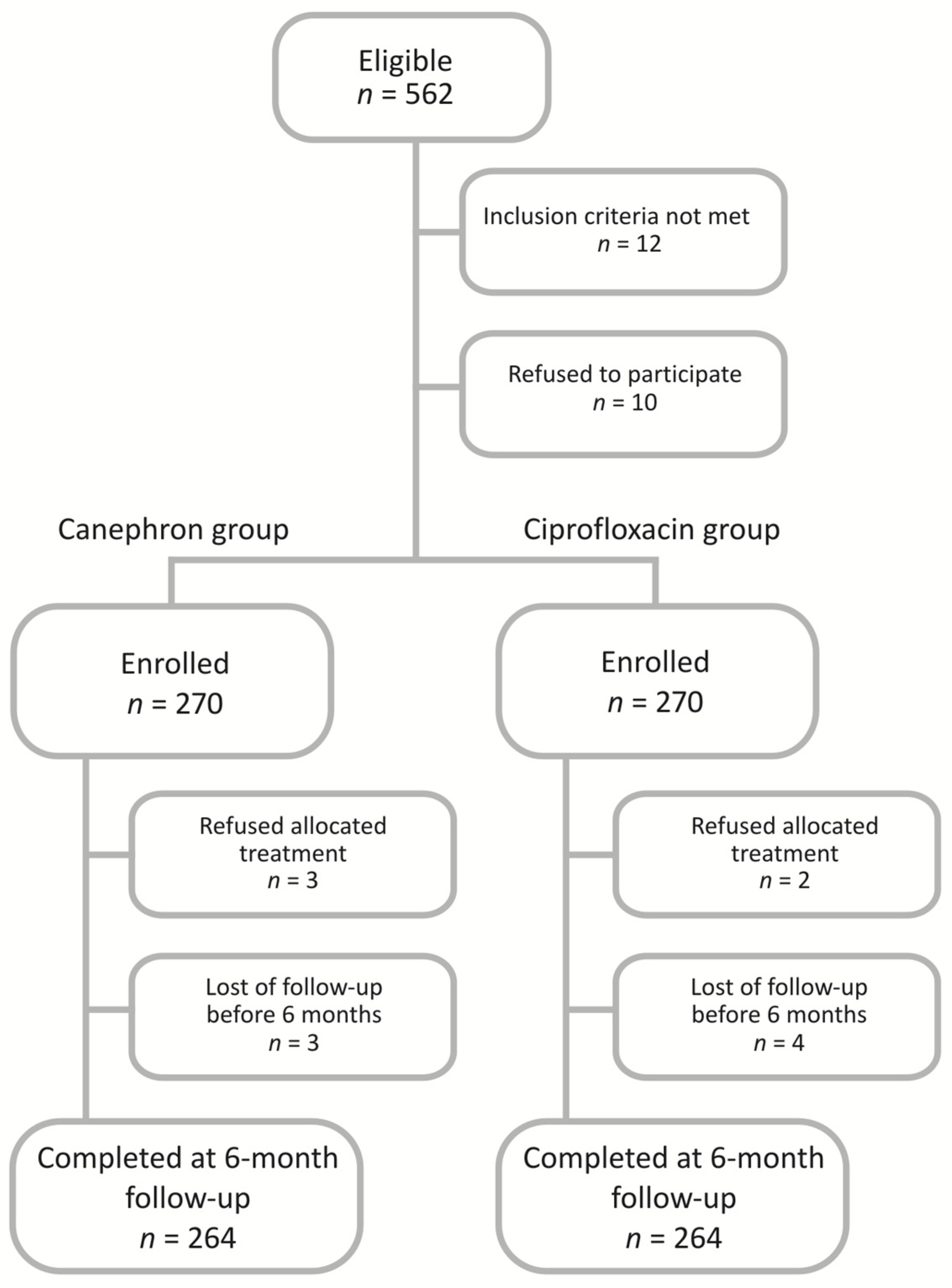
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Foxman, B. Recurring urinary tract infection: Incidence and risk factors. Am. J. Public Health 1990, 80, 331–333. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 28 August 2020).
- Stamm, W.E. Urinary Tract Infections, 4th ed.; Bennett, J.V., Brachman, P.S., Eds.; Lippincott-Raven: Philadelphia, PA, USA, 1998; pp. 477–483. [Google Scholar]
- Foxman, B. Urinary tract infection syndromes: Occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect. Dis. Clin. N. Am. 2014, 28, 11–13. [Google Scholar] [CrossRef]
- Lo, E.; Nicolle, L.; Classen, D.; Arias, K.M.; Podgorny, K.; Anderson, D.J.; Burstin, H.; Calfee, D.P.; Coffin, S.E.; Dubberke, E.R.; et al. Strategies to prevent catheter associated urinary tract infections in acute care hospitals. Infect. Cont. Hosp. Epid. 2008, 29, S41–S50. [Google Scholar] [CrossRef]
- Crowe, H.; Clift, R.; Duggan, G.; Bolton, D.; Costello, A. Randomised study of the effect of midnight removal of urinary catheters. Urol. Nurs. 1994, 14, 18–20. [Google Scholar]
- Kamilya, G.; Seal, S.L.; Mukherji, J.; Bhattacharyya, S.K.; Hazra, A. A randomized controlled trial comparing short versus long-term catheterization after uncomplicated vaginal prolapse surgery. J. Obstet. Gynaecol. Res. 2010, 36, 154–158. [Google Scholar] [CrossRef]
- Foxman, B.; Cronenwett, A.E.W.; Spino, C.; Berger, M.B.; Morgan, D.M. Cranberry juice capsules and urinary tract infection after surgery: Results of a randomized trial. Am. J. Obstet. Gynecol. 2015, 213, 194.e1. [Google Scholar] [CrossRef] [Green Version]
- Jonsson Funk, M.; Levin, P.J.; Wu, J.M. Trends in the surgical management of stress urinary incontinence. Obstet. Gynecol. 2012, 119, 845–851. [Google Scholar] [CrossRef] [Green Version]
- Tew, L.; Pomfret, I.; King, D. Infection risks associated with urinary catheters. Nurs. Stand. 2005, 20, 55–61. [Google Scholar] [CrossRef]
- Tambyah, P.A.; Halvorson, K.T.; Maki, D.G. A prospective study of pathogenesis of catheter associated urinary tract infections. Mayo Clin. Proc. 1999, 74, 131–136. [Google Scholar] [CrossRef]
- Saint, S.; Greene, M.T.; Krein, S.L.; Rogers, M.A.; Ratz, D.; Fowler, K.E.; Edson, B.S.; Watson, S.R.; Meyer-Lucas, B.; Masuga, M.; et al. A program to prevent catheter-associated urinary tract infection in acute care. N. Engl. J. Med. 2016, 374, 2111–2119. [Google Scholar] [CrossRef]
- Singh, R.; Hokenstad, E.D.; Wiest, S.R.; Kim-Fine, S.; Weaver, A.L.; McGree, M.E.; Klingele, C.J.; Trabuco, E.C.; Gebhart, J.B. Randomized controlled trial of silver-alloy-impregnated suprapubic catheters versus standard suprapubic catheters in assessing urinary tract infection rates in urogynecology patients. Int. Urogynecol. J. 2019, 30, 779–787. [Google Scholar] [CrossRef]
- Milan, P.B.; Ivan, I.M. Catheter-associated and nosocomial urinary tract infections: Antibiotic resistance and influence on commonly used antimicrobial therapy. Int. Urol. Nephrol. 2009, 41, 461–464. [Google Scholar] [CrossRef]
- Naber, K.G. Efficacy and safety of the phytotherapeutic drug Canephron® N in prevention and treatment of urogenital and gestational disease: Review of clinical experience in Eastern Europe and Central Asia. Res. Rep. Urol. 2013, 5, 39–46. [Google Scholar]
- Künstle, G.; Brenneis, C.; Haunschild, J. Efficacy of Canephron® N against bacterial adhesion, inflammation and bladder hyperactivity. Eur. Urol. Suppl. 2013, 12, e671. [Google Scholar] [CrossRef]
- Künstle, G.; Brenneis, C.; Pergola, C.; Werz, O.; Haunschild, J. Anti-inflammatory effects of Canephron® N and effectiveness in a model of interstitial cystitis. Urologe 2013, 52 (Suppl. S1), e97. [Google Scholar]
- Marcon, J.; Schubert, S.; Stief, C.G.; Magistro, G. In vitro efficacy of phytotherapeutics suggested for prevention and therapy of urinary tract infections. Infection 2019, 47, 937–944. [Google Scholar] [CrossRef]
- Nausch, B.; Pace, S.; Pein, H.; Koeberle, A.; Rossi, A.; Künstle, G.; Werz, O. The standardized herbal combination BNO 2103 contained in Canephron® N alleviates inflammatory pain in experimental cystitis and prostatitis. Phytomedicine 2019, 60, 152987. [Google Scholar] [CrossRef]
- Miotla, P.; Wawrysiuk, S.; Naber, K.; Markut-Miotla, E.; Skorupski, P.; Skorupska, K.; Rechberger, T. Should We Always Use Antibiotics after Urodynamic Studies in High-Risk Patients? Biomed. Res. Int. 2018, 2018, 1607425. [Google Scholar] [CrossRef] [Green Version]
- Wagenlehner, F.M.; Abramov-Sommariva, D.; Höller, M.; Steindl, H.; Naber, K.G. Non-Antibiotic Herbal Therapy (BNO 1045) versus Antibiotic Therapy (Fosfomycin Trometamol) for the Treatment of Acute Lower Uncomplicated Urinary Tract Infections in Women: A Double-Blind, Parallel-Group, Randomized, Multicentre, Non-Inferiority Phase III Trial. Urol. Int. 2018, 101, 327–336. [Google Scholar]
- Rechberger, T.; Futyma, K.; Jankiewicz, K.; Adamiak, A.; Bogusiewicz, M.; Bartuzi, A.; Miotła, P.; Skorupski, P.; Tomaszewski, J. Tape fixation: An important surgical step to improve success rate of anti-incontinence surgery. J. Urol. 2011, 186, 180–184. [Google Scholar] [CrossRef] [Green Version]
- Kelleher, C.J.; Cardozo, L.D.; Khullar, V.; Salvatore, S. A new questionnaire to assess the quality of life of urinary incontinent women. Br. J. Obstet. Gynaecol. 1997, 104, 1374–1379. [Google Scholar] [CrossRef] [PubMed]
- Shumaker, S.A.; Wyman, J.F.; Uebersax, J.S.; McClish, D.; Fantl, J.A. Health related quality of life measures for women with urinary incontinence: The urogenital distress inventory and the incontinence impact questionnaire. Qual. Life Res. 1994, 3, 291–306. [Google Scholar] [CrossRef]
- Uebersax, J.S.; Wyman, J.F.; Shumaker, S.A.; McClish, D.K.; Fantl, J.A. Short forms to assess life quality symptom distress for urinary incontinence in women: The incontinence impact questionnaire and the urogenital distress inventory. Neurourol. Urodyn. 1995, 14, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Skorupska, K.; Rechberger, T.; Bogusiewicz, M.; Adamiak-Godlewska, A.; Kwiatkowska, A.; Miotla, P. Current trends in urogynecological surgeries in Poland. Int. Urogynecol. J. 2020, 31, 1627–1632. [Google Scholar] [CrossRef] [Green Version]
- Marschall, J.; Carpenter, C.R.; Fowler, S.; Trautner, B.W. CDC Prevention Epicenters Program. Antibiotic Prophylaxis for Urinary Tract Infections After Removal of Urinary Catheter: Meta-Analysis. BMJ 2013, 346, f3147. [Google Scholar] [CrossRef] [Green Version]
- Davidov, M.I.; Bunova, N.E. Comparative assessment of Canephron N and ciprofloxacin as monotherapy of acute uncomplicated cystitis in women. Urologiia 2018, 4, 24–32. [Google Scholar] [CrossRef]
- Savas, L.; Guvel, S.; Onlen, Y.; Savas, N.; Duran, N. Nosocomial urinary tract infections: Microorganisms, antibiotic sensitivities and risk factors. West Indian Med. J. 2006, 55, 188–193. [Google Scholar] [CrossRef]
- Dudeck, M.A.; Horan, T.C.; Peterson, K.D.; Allen-Bridson, K.; Morrell, G.; Anttila, A.; Pollock, D.A.; Edwards, J.R. National Healthcare Safety Network (NHSN) report, data summary for 2011, device-associated module. Am. J. Infect. Control 2013, 41, 286–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, L.E.; Hall, E.; Carberry, C.L. Cystoscopy at the time of incontinence and prolapse surgery. Curr. Opin. Obstet. Gynecol. 2018, 30, 441–445. [Google Scholar] [CrossRef]
- Falagas, M.E.; Athanasiou, S.; Iavazzo, C.; Tokas, T.; Antsaklis, A. Urinary tract infections after pelvic floor gynecological surgery: Prevalence and effect of antimicrobial prophylaxis. A systematic review. Int. Urogynecol. J. Pelvic. Floor. Dysfunct. 2008, 19, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Glavind, K.; Morup, L.; Madsen, H.; Glavind, J. A prospective, randomised, controlled trial comparing 3 hour and 24 hour postoperative removal of bladder catheter and vaginal pack following vaginal prolapse surgery. Acta Obstet. Gynecol. Scand. 2007, 86, 1122–1125. [Google Scholar] [CrossRef] [PubMed]
- Foon, R.; Toozs-Hobson, P.; Latthe, P. Prophylactic antibiotics to reduce the risk of urinary tract infections after urodynamic studies. Cochrane Database Syst. Rev. 2012, 10, CD008224. [Google Scholar] [CrossRef] [PubMed]
- Naber, K.G.; Bonkat, G.; Wagenlehner, F.M.E. The EAU and AUA/CUA/SUFU Guidelines on Recurrent Urinary Tract Infections: What is the Difference? Eur. Urol. 2020, 29, S0302-2838(20)30461-9. [Google Scholar]
- Carapeti, E.A.; Andrews, S.M.; Bentley, P.G. Randomised study of sterile versus non sterile urethral catheterisation. Ann. R. Coll. Surg. Engl. 1996, 78, 59–60. [Google Scholar]
- Nickel, J.C.; Feero, P.; Costerton, J.W.; Wilson, E. Incidence and importance of bacteriuria in postoperative, short-term urinary catheterization. Can. J. Surg. 1989, 32, 131–132. [Google Scholar]
- Liedberg, H.; Lundberg, T. Silver-alloy coated catheters reduce catheter associated bacteriuria. Br. J. Urol. 1990, 65, 379–381. [Google Scholar] [CrossRef]
- Wawrysiuk, S.; Naber, K.; Rechberger, T.; Miotla, P. Prevention and treatment of uncomplicated lower urinary tract infections in the era of increasing antimicrobial resistance-non-antibiotic approaches: A systemic review. Arch. Gynecol. Obstet. 2019, 300, 821–828. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Canephron Group n = 264 | Ciprofloxacin Group n = 264 | |
|---|---|---|
| Age (years), M ± SD | 53.45 ± 11.54 | 52.76 ± 12.43 |
| BMI (kg/m2), M ± SD | 28.02 ± 3.95 | 27.71 ± 4.29 |
| ICIQ Short Form | 14.35 ± 4.08 | 14.98 ± 3.30 |
| CANEPHRON N group | (T0) Before | (T1) 3 Months | (T2) 6 Months | ANOVA | Post hoc |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | |||
| UDI-6 | 64.03 ± 18.98 | 14.79 ± 22.21 | 15.78 ± 22.77 | F(2.526) = 641.24 p < 0.001 | T1 vs. T2: p < 0.001 T1 vs. T3: p < 0.001 T2 vs. T3: p = 0.80 |
| IIQ-7 | 62.82 ± 24.30 | 14.45 ± 27.11 | 15.10 ± 28.15 | F(2.526) = 470.33 p < 0.001 | T1 vs. T2: p < 0.001 T1 vs. T3: p < 0.001 T2 vs. T3: p = 0.93 |
| ICIQ—Short Form | 14.35 ± 4.08 | 3.06 ± 5.03 | 3.83 ± 5.77 | F(2.524) = 693.34 p < 0.001 | T1 vs. T2: p < 0.001 T1 vs. T3: p < 0.001 T2 vs. T3: p = 0.06 |
| CIPROFLOXACIN Group | (T0) Before | (T1) 3 Months | (T2) 6 Months | ANOVA | Post hoc |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ±SD | |||
| UDI-6 | 67.21 ± 9.68 | 13.87 ± 0.43 | 14.60 ± 2.14 | F(2.526)= 761.21 p < 0.001 | T1 vs. T2: p < 0.001 T1 vs. T3: p < 0.001 T2 vs. T3: p = 0.89 |
| IIQ-7 | 64.57 ± 2.26 | 12.95 ± 6.08 | 13.76 ± 2.89 | F(2.526)= 564.78 p < 0.001 | T1 vs. T2: p < 0.001 T1 vs. T3: p < 0.001 T2 vs. T3: p = 0.89 |
| ICIQ Short Form | 14.98 ± 3.30 | 2.26 ± 5.29 | 3.00 ± 5.24 | F(2.526)= 879.42 p < 0.001 | T1 vs. T2: p < 0.001 T1 vs. T3: p < 0.001 T2 vs. T3: p = 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rechberger, E.; Rechberger, T.; Wawrysiuk, S.; Miotla, P.; Kulik- Rechberger, B.; Kuszka, A.; Wróbel, A. A Randomized Clinical Trial to Evaluate the Effect of Canephron N in Comparison to Ciprofloxacin in the Prevention of Postoperative Lower Urinary Tract Infections after Midurethral Sling Surgery. J. Clin. Med. 2020, 9, 3391. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113391
Rechberger E, Rechberger T, Wawrysiuk S, Miotla P, Kulik- Rechberger B, Kuszka A, Wróbel A. A Randomized Clinical Trial to Evaluate the Effect of Canephron N in Comparison to Ciprofloxacin in the Prevention of Postoperative Lower Urinary Tract Infections after Midurethral Sling Surgery. Journal of Clinical Medicine. 2020; 9(11):3391. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113391
Chicago/Turabian StyleRechberger, Ewa, Tomasz Rechberger, Sara Wawrysiuk, Pawel Miotla, Beata Kulik- Rechberger, Andrzej Kuszka, and Andrzej Wróbel. 2020. "A Randomized Clinical Trial to Evaluate the Effect of Canephron N in Comparison to Ciprofloxacin in the Prevention of Postoperative Lower Urinary Tract Infections after Midurethral Sling Surgery" Journal of Clinical Medicine 9, no. 11: 3391. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113391