Accuracy of Conventional and Machine Learning Enhanced Chest Radiography for the Assessment of COVID-19 Pneumonia: Intra-Individual Comparison with CT

 ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Patient Population
2.2. Image Acquisition
2.2.1. Conventional Chest Radiography
2.2.2. CT Protocol
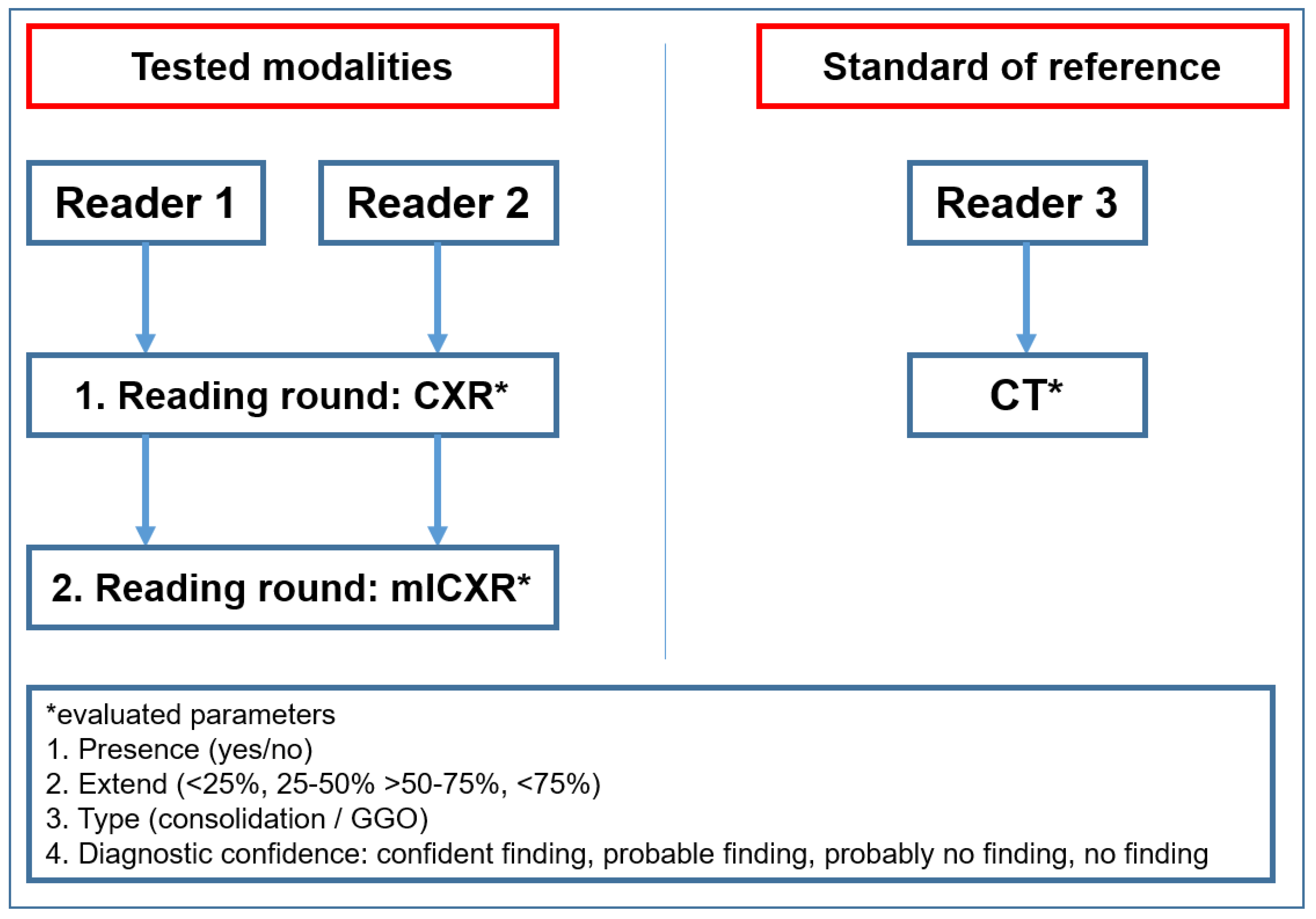
2.3. Image Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Population
3.2. Clinical Findings in COVID-19 Patients
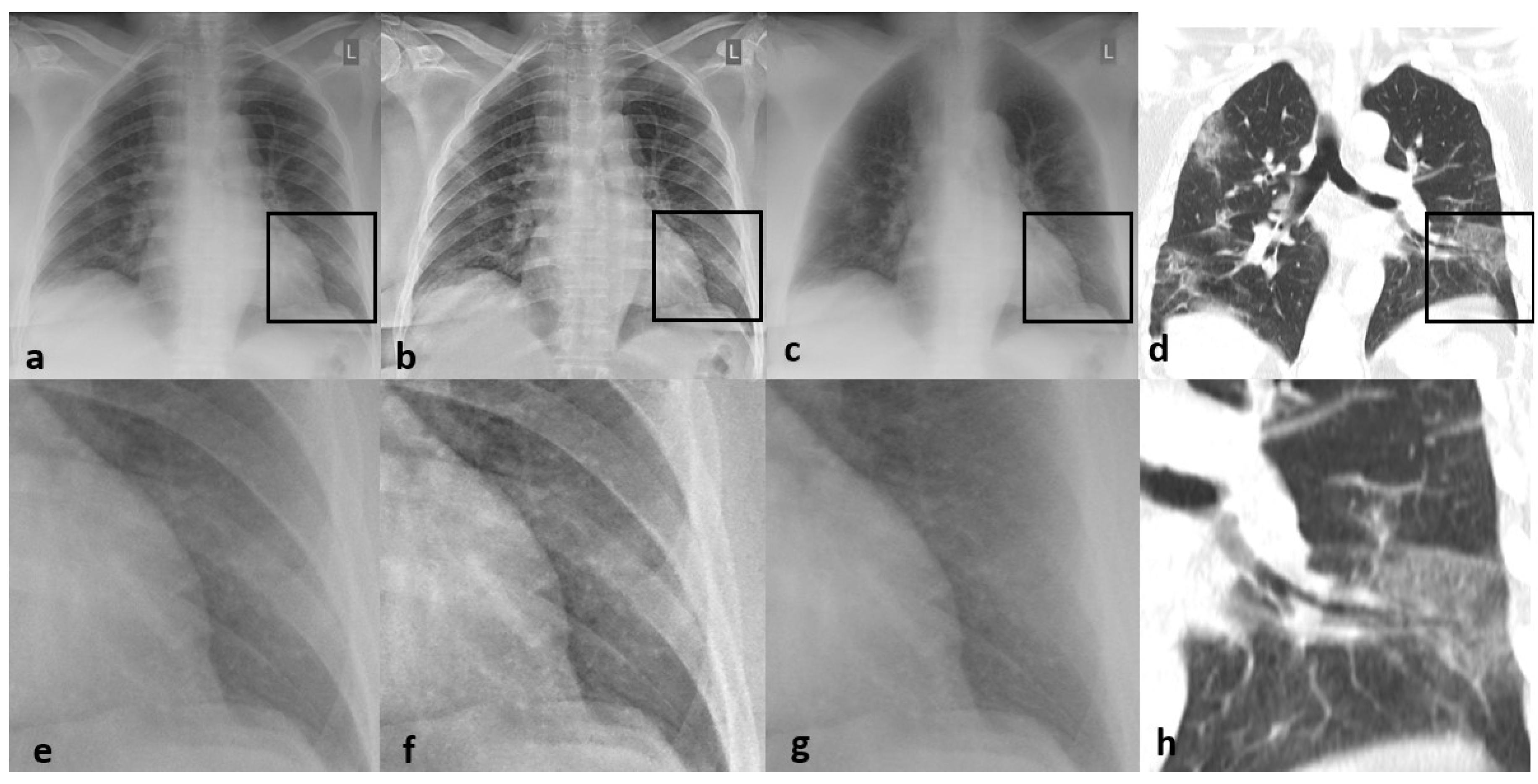
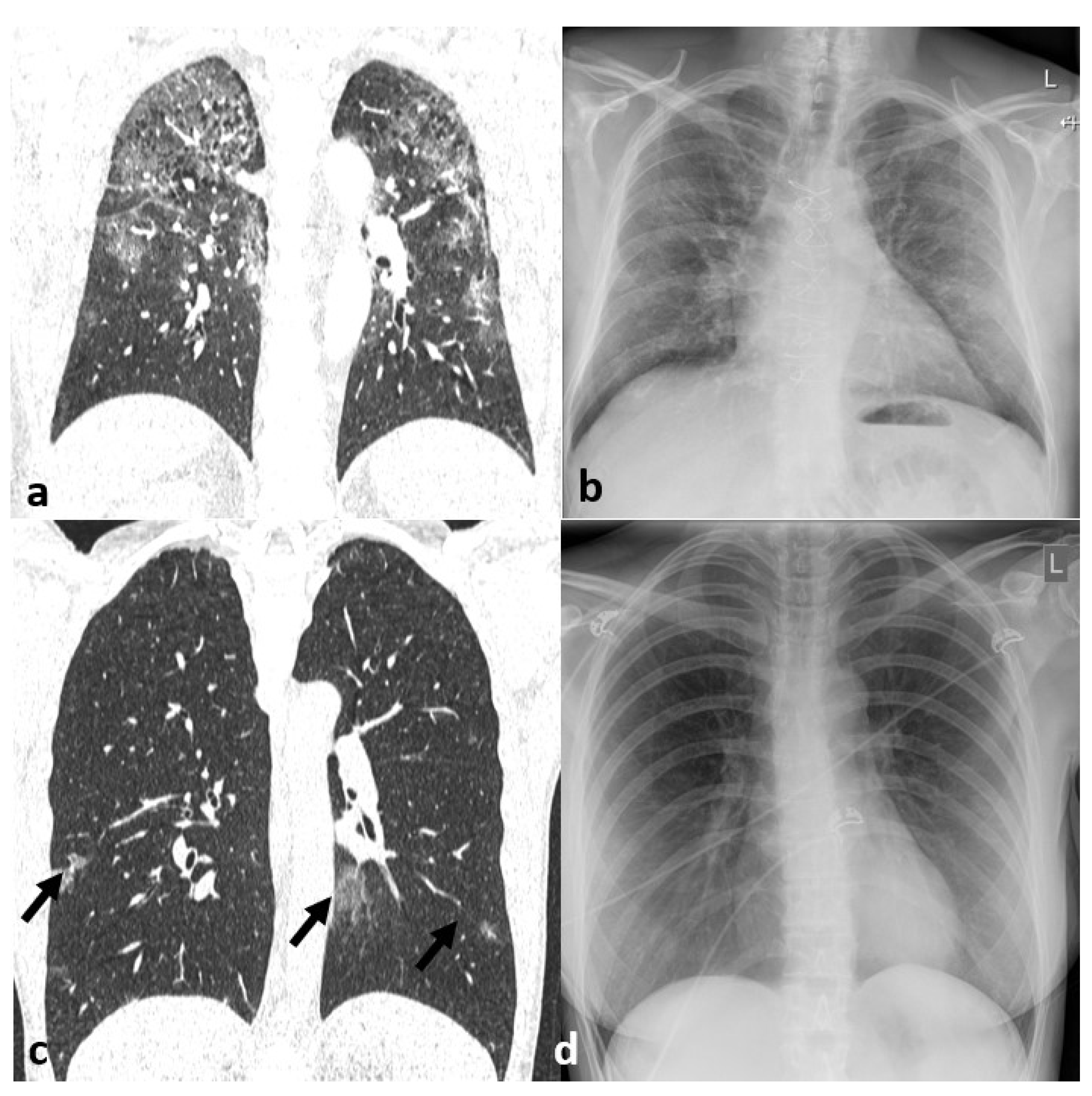
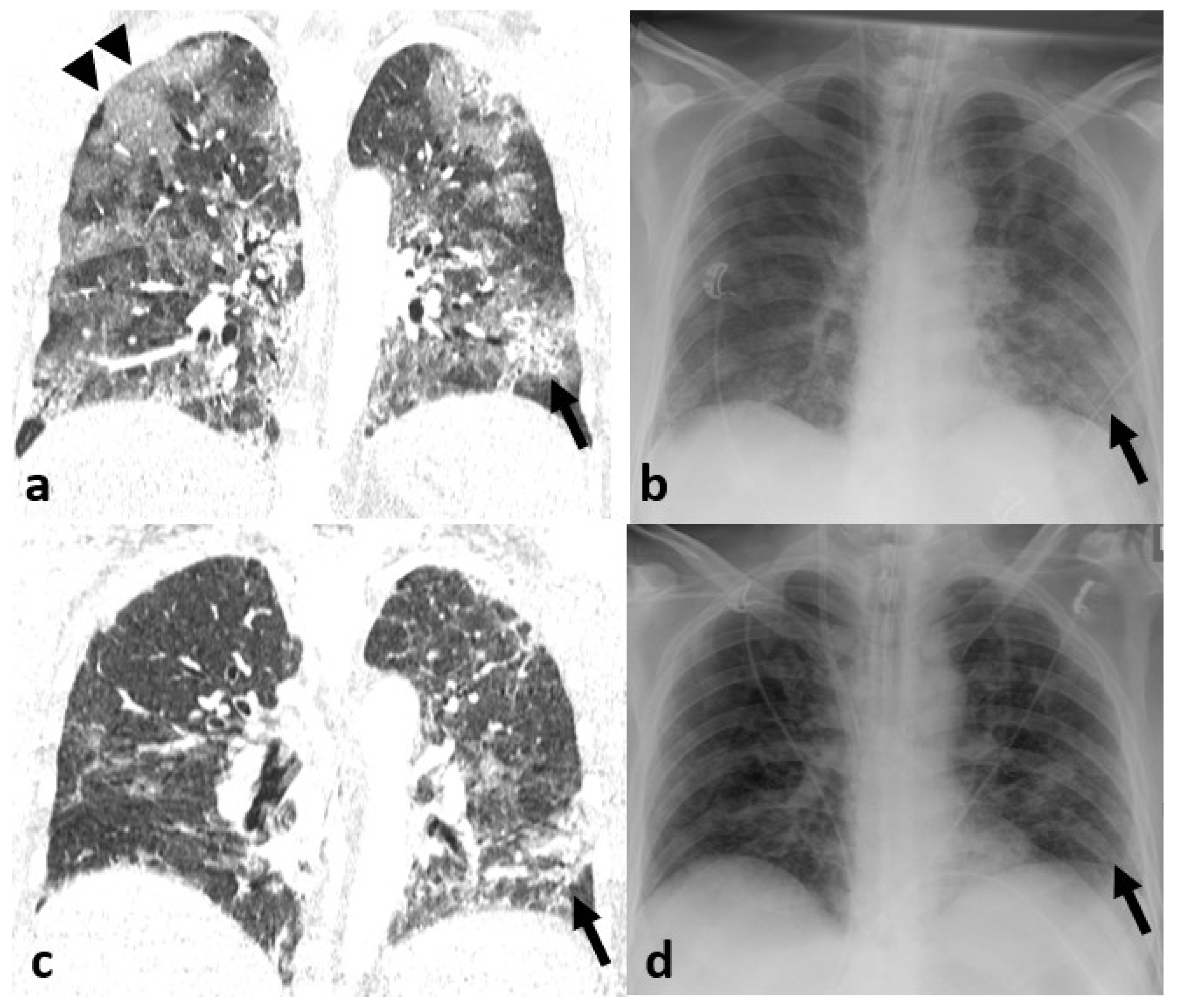
3.3. Imaging Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Xu, X.; Yu, C.; Qu, J.; Zhang, L.; Jiang, S.; Huang, D.; Chen, B.; Zhang, Z.; Guan, W.; Ling, Z.; et al. Imaging and clinical features of patients with 2019 novel coronavirus SARS-CoV-2. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1275–1280. [Google Scholar] [CrossRef] [Green Version]
- ACR Recommendations for the Use of Chest Radiography and Computed Tomography (CT) for Suspected COVID-19 Infection. Available online: https://www.acr.org/Advocacy-and-Economics/ACR-Position-Statements/Recommendations-for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection (accessed on 26 April 2020).
- Wang, Y.; Dong, C.; Hu, Y.; Li, C.; Ren, Q.; Zhang, X.; Shi, H.; Zhou, M. Temporal Changes of CT Findings in 90 Patients with COVID-19 Pneumonia: A Longitudinal Study. Radiology 2020, 296, E55–E64. [Google Scholar] [CrossRef] [Green Version]
- Abbasi-Oshaghi, E.; Mirzaei, F.; Farahani, F.; Khodadadi, I.; Tayebinia, H. Diagnosis and treatment of coronavirus disease 2019 (COVID-19): Laboratory, PCR, and chest CT imaging findings. Int. J. Surg. 2020, 79, 143–153. [Google Scholar] [CrossRef]
- Graat, E.M.; Hendrikse, A.K.; Spronk, P.E.; Korevaar, J.C.; Stoker, J.; Schultz, M.J. Chest radiography practice in critically ill patients: A postal survey in the Netherlands. BMC Med. Imaging 2006, 6, 8. [Google Scholar] [CrossRef] [Green Version]
- Martini, K.; Baessler, M.; Baumueller, S.; Frauenfelder, T. Diagnostic accuracy and added value of dual-energy subtraction radiography compared to standard conventional radiography using computed tomography as standard of reference. PLoS ONE 2017, 12, e0174285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.N.; Al-Jahdali, H.; Al-Ghanem, S.; Gouda, A. Reading chest radiographs in the critically ill (Part I): Normal chest radiographic appearance, instrumentation and complications from instrumentation. Ann. Thorac. Med. 2009, 4, 75–87. [Google Scholar] [CrossRef]
- Wei, P.-F. Diagnosis and Treatment Protocol for Novel Coronavirus Pneumonia (Trial Version 7). Chin. Med. J. 2020, 133, 1087–1095. [Google Scholar]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, J.R.; Horner, P.E.; Primack, S.L. ICU Imaging. Clin. Chest Med. 2008, 29, 59–76. [Google Scholar] [CrossRef] [PubMed]
- Franquet, T. Imaging of pneumonia: Trends and algorithms. Eur. Respir. J. 2001, 18, 196–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canella, C.; Philippe, P.; Pansini, V.M.; Salleron, J.; Flipo, R.-M.; Cotten, A. Use of Tomosynthesis for Erosion Evaluation in Rheumatoid Arthritic Hands and Wrists 1. Radiology 2011, 258, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Manji, F.; Wang, J.; Norman, G.; Wang, Z.; Koff, D. Comparison of dual energy subtraction chest radiography and traditional chest X-rays in the detection of pulmonary nodules. Quant. Imaging Med. Surg. 2016, 6, 1–5. [Google Scholar] [PubMed]
- Kuhlman, J.E.; Collins, J.; Brooks, G.N.; Yandow, D.R.; Broderick, L.S. Dual-Energy Subtraction Chest Radiography: What to Look for beyond Calcified Nodules. RadioGraphics 2006, 26, 79–92. [Google Scholar] [CrossRef] [PubMed]
- Sahiner, B.; Chan, H.-P.; Hadjiiski, L.M.; Cascade, P.N.; Kazerooni, E.A.; Chughtai, A.R.; Poopat, C.; Song, T.; Frank, L.; Stojanovska, J.; et al. Effect of CAD on Radiologists’ Detection of Lung Nodules on Thoracic CT Scans: Analysis of an Observer Performance Study by Nodule Size. Acad. Radiol. 2009, 16, 1518–1530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghesi, A.; Maroldi, R. COVID-19 outbreak in Italy: Experimental chest X-ray scoring system for quantifying and monitoring disease progression. Radiol. Med. 2020, 125, 509–513. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female, n (%) | 21 (35%) |
| Median age, years (range) | 61 (38–81) |
| Infective consolidation, n (%) | 39 (65.0%) |
| Median time interval CXR to CT, hours (range) | 12 (0–36) |
| Mean time since symptom-onset, days | 7.2 ± 8.9 |
| Body mass index, n (%) | |
| ≤25 kg/m2 | 6 (14.6%) |
| <25–30 kg/m2 | 10 (24.4%) |
| >30 kg/m2 | 25 (61.0%) |
| Cardiovascular disease, n (%) | 8 (19.5%) |
| Arterial hypertension, n (%) | 13 (31.7%) |
| Diabetes mellitus, n (%) | 11 (26.8%) |
| Chronic renal dysfunction, n (%) | 9 (22.0%) |
| Chronic pulmonary disease, n (%) | 3 (7.3%) |
| Hepatitis or Liver cirrhosis, n (%) | 3 (7.3%) |
| Malignancy, n (%) | 6 (14.6%) |
| ARDS, n (%) | 19 (46.3%) |
| Treatment type at diagnosis, n (%) | |
| Out of hospital | 1 (2.4%) |
| In hospital | 26 (63.4%) |
| ICU without mechanic ventilation | 4 (9.8%) |
| ICU with mechanic ventilation | 5 (12.2%) |
| CXR | mlCXR | CT | |||
|---|---|---|---|---|---|
| Reader 1 | Reader 2 | Reader 1 | Reader 2 | Reader 3 | |
| Overall evaluated cases, (n, %) | 60 (100.0) | 60 (100.0) | 60 (100.0) | 60 (100.0) | 60 (100.0) |
| Presence of pneumonia | |||||
| Overall, (n, %) | 31 (51.7) | 28 (46.7) | 42 (70.0) | 35 (58.3) | 39 (65.0) |
| GGO, (n, %) | - | - | - | - | 37 (61.7) |
| Classic consolidation, (n, %) | - | - | - | - | 16 (26.7) |
| Extend of lung changes in cases with signs of COVID19-pneumonia | |||||
| <25%, (n, %) | 1 (3.2) | 3 (10.7) | 6 (14.3) | 5 (14.3) | 2 (5.1) |
| 25–50%, (n, %) | 11 (35.5) | 12 (42.9) | 20 (47.6) | 13 (37.1) | 15 (38.5) |
| >50–75%, (n, %) | 11 (35.5) | 9 (32.1) | 16 (38.1) | 16 (45.7) | 9 (23.1) |
| >75%, (n, %) | 7 (22.6) | 4 (14.3) | 0 (0) | 1 (2.9) | 13 (33.3) |
| CXR | mlCXR | ||||
|---|---|---|---|---|---|
| Reader 1 | Reader 2 | Reader 1 | Reader 2 | p-Value | |
| Diagnostic accuracy | 0.031 | ||||
| Sensitivity, (95%CI) | 79.5 (63–90) | 71.8 (55–84) | 92.3 (78–98) | 89.7 (75–97) | |
| Specificity, (95%CI) | 100.0 (81–100) | 100.0 (81–100) | 71.4 (48–88) | 71.4 (48–88) | |
| PPV, (95%CI) | 100.0 (86–100) | 100.0 (85–100) | 85.7 (71–94) | 85.4 (70–94) | |
| NPV, (95%CI) | 72.4 (53–87) | 65.6 (47–81) | 83.3 (58–96) | 78.9 (54–93) | |
| Inter-reader agreement, kappa | 0.834 | 0.805 | |||
| Diagnostic confidence | 0.013 | ||||
| Overall certainty | 40 (66.7) | 36 (60.0) | 52 (86.7) | 50 (83.3) | |
| Overall un-certainty | 20 (33.3) | 24 (40.0) | 8 (13.3) | 10 (16.7) | |
| Def. COVID-19 pneumonia | 25 (41.7) | 21 (35.0) | 37 (61.7) | 37 (57.8) | |
| Probable COVID-19 pneumonia | 9 (15.0) | 13 (21.7) | 8 (13.3) | 9 (15.0) | |
| Probably no COVID-19 pneumonia | 11 (18.3) | 11 (18.3) | 2 (3.3) | 1 (1.7) | |
| Def. no COVID-19 pneumonia | 15 (25.0) | 15 (25.9) | 12 (20.0) | 13 (21.1) | |
| Accuracy of disease extent estimation | 0.590 | ||||
| Exact estimation | 23 (52.3) | 19 (43.2) | 33 (75.0) | 34 (77.3) | |
| Under-estimation | 16 (36.4) | 21 (47.7) | 14 (31.8) | 17 (38.6) | |
| Over-estimation | 5 (11.4) | 4 (9.1) | 7 (15.9) | 4 (9.1) | |
| Inter-reader agreement, kappa | 0.650 | 0.856 | |||
| CXR | mlCXR | Kappa | |||
|---|---|---|---|---|---|
| Reader 1 | Reader 2 | Reader 1 | Reader 2 | ||
| GGO on CT | 0.669 | ||||
| Sensitivity, (95%CI) | 37.5 (16–64) | 40.0 (20–64) | 61.7 (47–79) | 67.6 (50–81) | |
| Specificity, (95%CI) | 93.2 (8–98) | 93 (80–98) | 95.7 (76–99) | 91 (70–98) | |
| PPV, (95%CI) | 66.7 (31–91) | 73 (39–93) | 96.0 (78–99) | 93 (74–99) | |
| NPV, (95%CI) | 80.4 (66–90) | 77 (63–87) | 62.9 (45–78) | 64 (45–79) | |
| Consolidation on CT | 0.865 | ||||
| Sensitivity, (95%CI) | 70.3 (53–84) | 81.3 (54–95) | 100 (77–100) | 81.3 (54–95) | |
| Specificity, (95%CI) | 95.7 (76–100) | 91.1 (77–97) | 98 (86–100) | 90.9 (77–97) | |
| PPV, (95%CI) | 96.3 (79–100) | 76.5 (50–92) | 94 (71–100) | 76.5 (50–92) | |
| NPV, (95%CI) | 66.7 (48–81) | 93.3 (80–98) | 100 (90–100) | 93.0 (80–98) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, K.; Blüthgen, C.; Walter, J.E.; Messerli, M.; Nguyen-Kim, T.D.L.; Frauenfelder, T. Accuracy of Conventional and Machine Learning Enhanced Chest Radiography for the Assessment of COVID-19 Pneumonia: Intra-Individual Comparison with CT. J. Clin. Med. 2020, 9, 3576. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113576
Martini K, Blüthgen C, Walter JE, Messerli M, Nguyen-Kim TDL, Frauenfelder T. Accuracy of Conventional and Machine Learning Enhanced Chest Radiography for the Assessment of COVID-19 Pneumonia: Intra-Individual Comparison with CT. Journal of Clinical Medicine. 2020; 9(11):3576. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113576
Chicago/Turabian StyleMartini, Katharina, Christian Blüthgen, Joan E. Walter, Michael Messerli, Thi Dan Linh Nguyen-Kim, and Thomas Frauenfelder. 2020. "Accuracy of Conventional and Machine Learning Enhanced Chest Radiography for the Assessment of COVID-19 Pneumonia: Intra-Individual Comparison with CT" Journal of Clinical Medicine 9, no. 11: 3576. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113576