Improvement of Gait after 4 Weeks of Wearable Focal Muscle Vibration Therapy for Individuals with Diabetic Peripheral Neuropathy

 ,
,
Abstract
:1. Introduction
2. Experimental Section
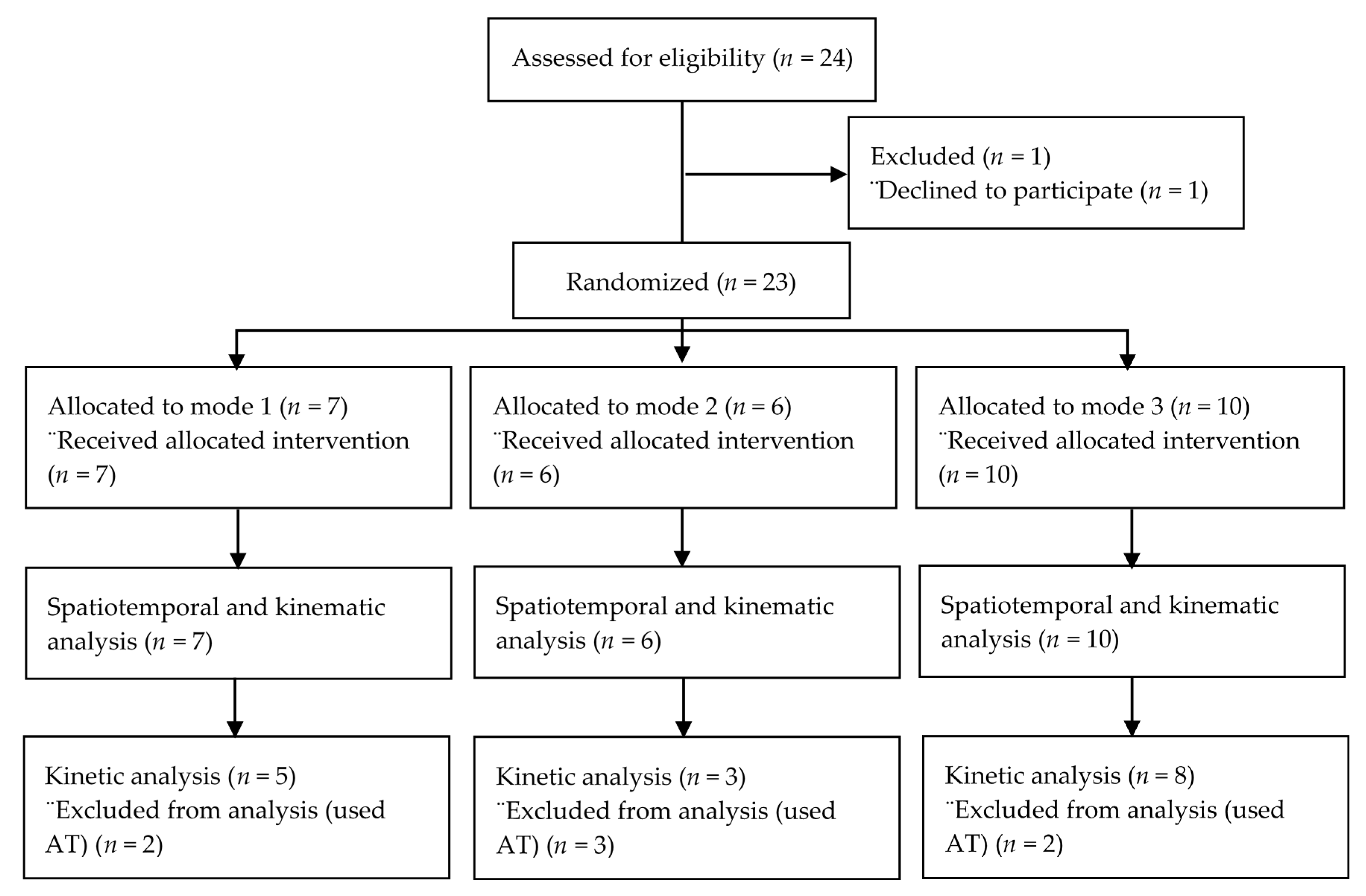
2.1. Participants
2.2. Gait Measurement Methods
2.3. Gait Outcome Measures
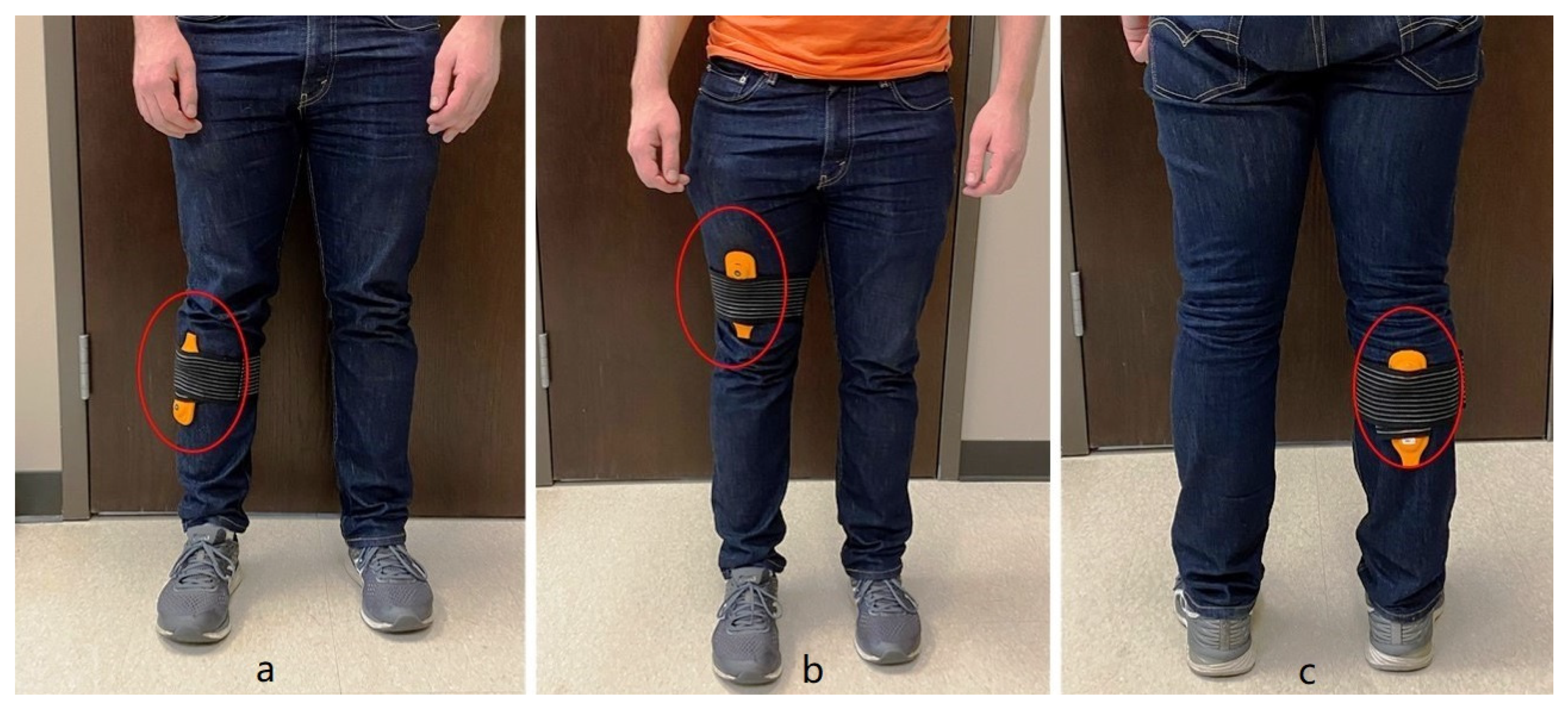
2.4. Intervention Protocol
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sun, J.; Wang, Y.; Zhang, X.; Zhu, S.; He, H. Prevalence of peripheral neuropathy in patients with diabetes: A systematic review and meta-analysis. Prim. Care Diabetes 2020, 14, 435–444. [Google Scholar] [CrossRef]
- Gordois, A.; Scuffham, P.; Shearer, A.; Oglesby, A.; Tobian, J.A. The Health Care Costs of Diabetic Peripheral Neuropathy in the U.S. Diabetes Care 2003, 26, 1790–1795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juster-Switlyk, K.; Smith, A.G. Updates in diabetic peripheral neuropathy. F1000Research 2016, 5, 738. [Google Scholar] [CrossRef] [PubMed]
- Harati, Y. Diabetic Peripheral Neuropathies. Methodist Debakey Cardiovasc. J. 2010, 6, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Jernigan, S.D.; Pohl, P.S.; Mahnken, J.D.; Kluding, P.M. Diagnostic Accuracy of Fall Risk Assessment Tools in People With Diabetic Peripheral Neuropathy. Phys. Ther. 2012, 92, 1461–1470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vinik, A.I.; Nevoret, M.L.; Casellini, C.; Parson, H. Diabetic Neuropathy. Endocrinol. Metab. Clin. N. Am. 2013, 42, 747–787. [Google Scholar] [CrossRef]
- Badr, N.M.H.; Fouad, S.A.; Hamdy, B. Gait Analysis in Patients with Diabetic Peripheral Neuropathy. Med. J. Cairo. Univ. 2010, 78. Available online: http://erepository.cu.edu.eg/index.php/MJCU/article/view/1129/1103 (accessed on 22 July 2020).
- Sadosky, A.; Mardekian, J.; Parsons, B.; Hopps, M.; Bienen, E.J.; Markman, J. Healthcare utilization and costs in diabetes relative to the clinical spectrum of painful diabetic peripheral neuropathy. J. Diabetes Complicat. 2015, 29, 212–217. [Google Scholar] [CrossRef]
- Alam, U.; Riley, D.R.; Jugdey, R.S.; Azmi, S.; Rajbhandari, S.; D’Août, K.; Malik, R.A. Diabetic Neuropathy and Gait: A Review. Diabetes Ther. 2017, 8, 1253–1264. [Google Scholar] [CrossRef] [Green Version]
- Gomes, A.A.; Onodera, A.N.; Otuzi, M.E.I.; Pripas, D.; Mezzarane, R.A.; NSacco, I.C. Electromyography and kinematic changes of gait cycle at different cadences in diabetic neuropathic individuals. Muscle Nerve 2011, 44, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Hazari, A.; Maiya, A.G.; Shivashankara, K.N.; Agouris, I.; Monteiro, A.; Jadhav, R.; Kumar, S.; Shashi Kumar, C.G.; Mayya, S.S. Kinetics and kinematics of diabetic foot in type 2 diabetes mellitus with and without peripheral neuropathy: A systematic review and meta-analysis. Springerplus 2016, 5, 1819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustapa, A.; Justine, M.; Mohd Mustafah, N.; Jamil, N.; Manaf, H. Postural Control and Gait Performance in the Diabetic Peripheral Neuropathy: A Systematic Review. BioMed Res. Int. 2016, 2016, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Martinelli, A.R.; Mantovani, A.M.; Nozabieli, A.J.L.; Ferreira, D.M.A.; Barela, J.A.; de Camargo, M.R.; Fregonesi, C.E.P.T. Muscle strength and ankle mobility for the gait parameters in diabetic neuropathies. Foot 2013, 23, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.; Saltzman, C.L.; Yack, H.J. Relationships between segmental foot mobility and plantar loading in individuals with and without diabetes and neuropathy. Gait Posture 2010, 31, 251–255. [Google Scholar] [CrossRef] [Green Version]
- Rahman, M.A.; Aziz, Z.; Rajendra Acharya, U.; Ha, T.P.; Kannathal, N.; Ng, E.Y.; Law, C.; Subramaniam, T.; Shuen, W.Y.; Fang, S.C. Analysis of plantar pressure in diabetic type 2 subjects with and without neuropathy. Itbm-Rbm 2006, 27, 46–55. [Google Scholar] [CrossRef]
- Mueller, M.J.; Minor, S.D.; Sahrmann, S.A.; Schaaf, J.A.; Strube, M.J. Differences in the gait characteristics of patients with diabetes and peripheral neuropathy compared with age-matched controls. Phys. Ther. 1994, 74, 299–313. [Google Scholar] [CrossRef]
- Winter, D.A. Biomechanics and Motor Control of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Morrison, S.; Colberg, S.R.; Parson, H.K.; Vinik, A.I. Exercise improves gait, reaction time and postural stability in older adults with type 2 diabetes and neuropathy. J. Diabetes Complicat. 2014, 28, 715–722. [Google Scholar] [CrossRef]
- Melese, H.; Alamer, A.; Hailu, M.; Kahsay, G. Effectiveness of Exercise Therapy on Gait Function in Diabetic Peripheral Neuropathy Patients: A Systematic Review of Randomized Controlled Trials. Diabetes Metab. Syndr. Obes. Targets Ther. 2020, 13, 2753–2764. [Google Scholar] [CrossRef]
- Hong, J.; Barnes, M.J.; Kessler, N.J. Case study: Use of vibration therapy in the treatment of diabetic peripheral small fiber neuropathy. Int. J. Diabetes Mellit. 2015, 3, 72–75. [Google Scholar] [CrossRef] [Green Version]
- Kessler, N.J.; Hong, J. Whole body vibration therapy for painful diabetic peripheral neuropathy: A pilot study. J. Bodyw. Mov. Ther. 2013, 17, 518–522. [Google Scholar] [CrossRef] [PubMed]
- Kessler, N.J.; Lockard, M.M.; Fischer, J. Whole body vibration improves symptoms of diabetic peripheral neuropathy. J. Bodyw. Mov. Ther. 2020, 24, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Hong, J. Whole Body Vibration Therapy for Diabetic Peripheral Neuropathic Pain. Health Sci. J. 2011, 5, 66. [Google Scholar]
- Lee, K. Effects of whole-body vibration therapy on perception thresholds of type 2 diabetic patients with peripheral neuropathy: A randomized controlled trial. J. Phys. Ther. Sci. 2017, 29, 1684–1688. [Google Scholar] [CrossRef] [Green Version]
- Kordi Yoosefinejad, A.; Shadmehr, A.; Olyaei, G.; Talebian, S.; Bagheri, H.; Mohajeri-Tehrani, M.R. Short-term effects of the whole-body vibration on the balance and muscle strength of type 2 diabetic patients with peripheral neuropathy: A quasi-randomized-controlled trial study. J. Diabetes Metab. Disord. 2015, 14, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Abercromby, A.F.J.; Amonette, W.E.; Layne, C.S.; Mcfarlin, B.K.; Hinman, M.R.; Paloski, W.H. Vibration Exposure and Biodynamic Responses during Whole-Body Vibration Training. Med. Sci. Sport Exerc. 2007, 39, 1794–1800. [Google Scholar] [CrossRef]
- Win, M.M.T.M.; Fukai, K.; Nyunt, H.H.; Linn, K.Z. Hand and foot exercises for diabetic peripheral neuropathy: A randomized controlled trial. Nurs. Health Sci. 2020, 22, 416–426. [Google Scholar] [CrossRef]
- Murillo, N.; Valls-Sole, J.; Vidal, J.; Opisso, E.; Medina, J.; Kumru, H. Focal vibration in neurorehabilitation. Eur. J Phys. Rehabil. Med. 2014, 50, 231–242. [Google Scholar]
- Li, W.; Li, C.; Xu, Q.; Ji, L. Effects of Focal Vibration over Upper Limb Muscles on the Activation of Sensorimotor Cortex Network: An EEG Study. J. Healthc. Eng. 2019, 2019, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Pazzaglia, C.; Camerota, F.; Germanotta, M.; Di Sipio, E.; Celletti, C.; Padua, L. Efficacy of focal mechanic vibration treatment on balance in Charcot-Marie-Tooth 1A disease: A pilot study. J. Neurol. 2016, 263, 1434–1441. [Google Scholar] [CrossRef]
- McKinney, Z.; Heberer, K.; Fowler, E.; Greenberg, M.; Nowroozi, B.N.; Grundfest, W.S. Initial biomechanical evaluation of wearable tactile feedback system for gait rehabilitation in peripheral neuropathy. MMVR 2014, 196, 271–277. [Google Scholar]
- Ahmad, I.; Verma, S.; Noohu, M.M.; Shareef, M.Y.; Ejaz Hussain, M. Sensorimotor and gait training improves proprioception, nerve function, and muscular activation in patients with diabetic peripheral neuropathy: A randomized control trial. J. Musculoskelet Neuronal Interact 2020, 20, 234–248. [Google Scholar] [PubMed]
- Feng, Y.; Schlösser, F.J.; Sumpio, B.E. The Semmes Weinstein monofilament examination as a screening tool for diabetic peripheral neuropathy. J. Vasc. Surg. 2009, 50, 675–682.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temporal Distance Calculations for Gait—Visual3D Wiki Documentation. Available online: https://c-motion.com/v3dwiki/index.php?title=Temporal_Distance_Calculations_for_Gait#Cadence (accessed on 6 October 2020).
- Chiles, N.S.; Phillips, C.L.; Volpato, S.; Bandinelli, S.; Ferrucci, L.; Guralnik, J.M.; Patel, K.V. Diabetes, peripheral neuropathy, and lower-extremity function. J. Diabetes Complicat. 2014, 28, 91–95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, J.K.; Thies, S.B.; DeMott, T.K.; Ashton-Miller, J.A. A Comparison of Gait Characteristics between Older Women with and Without Peripheral Neuropathy in Standard and Challenging Environments. J. Am. Geriatr. Soc. 2004, 52, 1532–1537. [Google Scholar] [CrossRef] [Green Version]
- Camerota, F.; Celletti, C.; Suppa, A.; Galli, M.; Cimolin, V.; Filippi, G.M.; La Torre, G.; Albertini, G.; Stocchi, F.; De Pandis, M.F. Focal Muscle Vibration Improves Gait in Parkinson’s Disease: A Pilot Randomized, Controlled Trial. Mov. Disord. Clin. Pract. 2016, 3, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Camerota, F.; Celletti, C.; Di Sipio, E.; De Fino, C.; Simbolotti, C.; Germanotta, M.; Mirabella, M.; Padua, L.; Nociti, V. Focal muscle vibration, an effective rehabilitative approach in severe gait impairment due to multiple sclerosis. J. Neurol. Sci. 2017, 372, 33–39. [Google Scholar] [CrossRef]
- Melai, T.; Schaper, N.C.; IJzerman, T.H.; Willems, P.J.B.; de Lange, T.L.H.; Meijer, K.; Lieverse, A.G.; Savelberg, H.H.C.M. Strength Training Affects Lower Extremity Gait Kinematics, Not Kinetics, in People With Diabetic Polyneuropathy. J. Appl. Biomech. 2014, 30, 221–230. [Google Scholar] [CrossRef]
- Martínez-Amat, A.; Hita-Contreras, F.; Lomas-Vega, R.; Caballero-Martínez, I.; Alvarez, P.J.; Martínez-López, E. Effects of 12-Week Proprioception Training Program on Postural Stability, Gait, and Balance in Older Adults. J. Strength Cond. Res. 2013, 27, 2180–2188. [Google Scholar] [CrossRef]
- Peppe, A.; Paravati, S.; Baldassarre, M.G.; Bakdounes, L.; Spolaor, F.; Guiotto, A.; Pavan, D.; Sawacha, Z.; Bottino, S.; Clerici, D.; et al. Proprioceptive Focal Stimulation (Equistasi®) May Improve the Quality of Gait in Middle-Moderate Parkinson’s Disease Patients. Double-Blind, Double-Dummy, Randomized, Crossover, Italian Multicentric Study. Front. Neurol. 2019, 10, 998. [Google Scholar] [CrossRef]
- Filippi, G.M.; Brunetti, O.; Botti, F.M.; Panichi, R.; Roscini, M.; Camerota, F.; Cesari, M.; Pettorossi, V.E. Improvement of Stance Control and Muscle Performance Induced by Focal Muscle Vibration in Young-Elderly Women: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2009, 90, 2019–2025. [Google Scholar] [CrossRef] [PubMed]
- Feltroni, L.; Monteleone, S.; Petrucci, L.; Carlisi, E.; Mazzacane, B.; Schieppati, M.; Dalla, E.T. Potentiation of muscle strength by focal vibratory stimulation on quadriceps femoris. G. Ital. Med. Lav. Ergon. 2018, 40, 90–96. [Google Scholar] [PubMed]
- Gomes, A.A.; Ackermann, M.; Ferreira, J.P.; Orselli, M.I.V.; Sacco, I.C.N. Muscle force distribution of the lower limbs during walking in diabetic individuals with and without polyneuropathy. J. Neuroeng. Rehabil. 2017, 14, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menz, H.B.; Lord, S.R.; St George, R.; Fitzpatrick, R.C. Walking stability and sensorimotor function in older people with diabetic peripheral neuropathy. Arch. Phys. Med. Rehabil. 2004, 85, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Niitsu, M.; Kamo, T.; Otake, S.; Nishida, Y. Effect of Exercise with Rhythmic Auditory Stimulation on Muscle Coordination and Gait Stability in Patients with Diabetic Peripheral Neuropathy: A Randomized Controlled Trial. Open J. Ther. Rehabil. 2019, 7, 79. [Google Scholar] [CrossRef] [Green Version]
- Saleh, M.S.; Rehab, N.I. Effect of ankle proprioceptive training on gait and risk of fall in patients with diabetic neuropathy: A randomized controlled trial. Int. J. Diabetes Res. 2019, 2, 40–45. [Google Scholar]
- El-Refay, B.H.; Ali, O.I. Efficacy of Exercise Rehabilitation Program in Improving Gait of Diabetic Neuropathy Patients. Med. J. Cairo Univ. 2014, 82, 225–232. [Google Scholar]



{kind=link}
{kind=link}
| Demographic Variables | All | Group 1 | Group 2 | Group 3 | p-Value a |
|---|---|---|---|---|---|
| Number | 23 | 7 | 6 | 10 | - |
| Age (years) | 66.74 (10.76) | 66.71 (13.35) | 66.50 (5.75) | 66.90 (12.08) | 0.53 |
| Weight (lbs.) | 219 (58.14) | 194.14 (44.21) | 240.33 (62.49) | 223.60 (63.11) | 0.36 |
| Height (inches) | 67.46 (3.58) | 65.86 (3.90) | 67.50 (4.28) | 68.55 (2.77) | 0.39 |
| Length of diabetes diagnosis (years) | 17.78 (8.45) | 16.43 (5.56) | 21 (13.31) | 16.90 (6.69) | 0.58 |
| Sex (F/M) | 14/9 | 5/2 | 3/3 | 6/4 | - |
| Race | |||||
| Caucasian | 21 | 6 | 6 | 9 | - |
| African-American | 1 | 0 | 0 | 1 | - |
| Euro-Asian | 1 | 1 | 0 | 0 | - |
| Parameter m = meters s = second | All Participants (n = 23) | Participants Receiving Mode 1 (Sinusoidal Vibration) (n = 7) | Participants Receiving Mode 2 (Pulsing Vibration) (n = 6) | Participants Receiving Mode 3 (Continuous Vibration) (n = 10) | |
|---|---|---|---|---|---|
| Gait speed (m/s) | pre | 0.82 (0.38) | 0.68 (0.23) | 0.58 (0.26) | 1.07 (0.40) |
| post | 0.90 (0.31) ac | 0.85 (0.30) | 1.02 (0.30) | 0.90 (0.31) | |
| Stride length (m) | pre | 0.93 (0.32) | 0.77 (0.38) | 0.80 (0.18) | 1.13 (0.23) |
| post | 1.03 (0.26) b | 1.04 (0.22) | 0.93 (0.19) | 1.09 (0.31) | |
| Stride width (m) | pre | 0.18 ± 0.04 | 0.18 (0.04) | 0.20 (0.04) | 0.18 (0.03) |
| post | 0.19 ± 0.03 b | 0.18 (0.03) | 0.19 (0.04) | 0.19 (0.03) | |
| Stride time (s) | pre | 1.32 (0.31) | 1.37 (0.33) | 1.51 (0.42) | 1.16 (0.10) |
| post | 1.22 (0.26) ac | 1.30 (0.32) | 1.35 (0.33) | 1.08 (0.04) | |
| Cadence (steps/min) | pre | 95.04 (17.40) | 91.22 (19.36) | 84.97 (21.39) | 103.76 (8.35) |
| post | 102.0 (16.3) ac | 96.73 (18.55) | 94.49 (22.09) | 110.08 (4.21) | |
| Left stance time (s) | pre | 0.88 (0.29) | 0.94 (0.26) | 1.09 (0.37) | 0.71 (0.11) |
| post | 0.82 (0.21) ac | 0.86 (0.24) | 0.94 (0.29) | 0.71 (0.05) | |
| Right stance time (s) | pre | 0.86 (0.31) | 0.87 (0.34) | 1.06 (0.42) | 0.74 (0.08) |
| post | 0.80 (0.21) bc | 0.85 (0.24) | 0.88 (0.29) | 0.70 (0.03) | |
| Left swing time (s) | pre | 0.43 (0.08) | 0.43 (0.08) | 0.42 (0.05) | 0.43 (0.09) |
| post | 0.40 (0.06) a | 0.43 (0.07) | 0.41 (0.06) | 0.37 (0.04) | |
| Right swing time (s) | pre | 0.43 (0.08) | 0.45 (0.12) | 0.44 (0.06) | 0.42 (0.05) |
| post | 0.42 (0.06) b | 0.44 (0.06) | 0.44 (0.08) | 0.39 (0.04) | |
| Double limb support (s) | pre | 0.47 (0.25) | 0.51 (0.21) | 0.66 (0.36) | 0.32 (0.06) |
| post | 0.42 (0.20) ac | 0.43 (0.19) | 0.54 (0.29) | 0.33 (0.06) | |
| Parameter L = Left; R = Right | Total (n = 23) | Mode 1 (Sinusoidal Vibration) (n = 7) | Mode 2 (Pulsing Vibration) (n = 6) | Mode 3 (Continuous Vibration) (n = 10) | |
|---|---|---|---|---|---|
| L peak knee flexion (°) | pre | 53.16 (9.31) | 53.13 (9.79) | 49.29 (7.52) | 55.50 (10.02) |
| post | 57.10 (9.31) a | 56.67 (11.99) | 56.15 (9.02) | 57.96 (8.31) | |
| L peak dorsiflexion (°) | pre | 19.70 (4.34) | 22.83 (1.91) | 17.80 (7.25) | 18.64 (1.79) |
| post | 19.32 (6.03) b | 21.15 (1.13) | 16.25 (10.71) | 19.89 (3.88) | |
| L peak plantarflexion (°) | pre | −12.37 (8.68) | −9.02 (7.51) | −15.84 (8.84) | −12.64 (9.30) |
| post | −12.70 (9.26) a | −13.81 (6.84) | −12.84 (11.63) | −11.84 (10.08) | |
| R peak knee flexion (°) | pre | 52.09 (9.51) | 53.68 (8.65) | 48.16 (8.85) | 53.34 (10.66) |
| post | 56.22 (11.92) b | 58.99 (11.94) | 48.59 (16.14) | 58.85 (11.92) | |
| R peak dorsiflexion (°) | pre | 21.12 (2.87) | 21.36 (0.83) | 23.71 (3.09) | 19.40 (2.57) |
| post | 19.49 (6.32) b | 19.76 (2.33) | 16.89 (11.53) | 20.86 (3.66) | |
| R peak plantarflexion (°) | pre | −11.50 (10.62) | −12.75 (9.53) | −9.21 (15.21) | −12.00 (9.04) |
| post | −12.87 (8.15) a | −12.99 (4.54) | −17.38 (9.70) | −10.09 (8.15) | |
| Total (n = 16) | Mode 1 (sinusoidal vibration) (n = 5) | Mode 2 (pulsing vibration) (n = 3) | Mode 3 (continuous vibration) (n = 8) | ||
| L peak knee flexor moment (N∙m/Kg) | pre | −0.61 (0.35) | −0.68 (0.39) | −0.61 (0.17) | −0.56 (0.40) |
| post | −0.78 (0.35) a,c | −0.94 (0.24) | −0.76 (0.06) | −0.68 (0.44) | |
| L peak plantar flexor moment (N∙m/Kg) | pre | 1.08 (0.18) | 1.16 (0.15) | 0.87 (0.07) | 1.11 (0.18) |
| post | 1.17 (0.31) b | 1.08 (0.22) | 1.29 (0.52) | 1.17 (0.30) | |
| L peak ankle power (W/Kg) | pre | 2.24 (0.90) | 2.48 (1.09) | 1.70 (0.68) | 2.29 (0.88) |
| post | 2.54 (1.02) b | 2.88 (0.95) | 1.91 (1.19) | 2.56 (1.03) | |
| R peak knee flexor moment (N∙m/Kg) | pre | −0.57 (0.34) | −0.74 (0.23) | −0.67 (0.21) | −0.43 (0.40) |
| post | −0.66 (0.41) a,c | −0.81 (0.20) | −0.81 (0.10) | −0.51 (0.53) | |
| R peak plantar flexor moment (N∙m/Kg) | pre | 1.08 (0.23) | 0.97 (0.22) | 0.94 (0.02) | 1.19 (0.22) |
| post | 1.08 (0.16) b | 1.07 (0.14) | 0.98 (0.06) | 1.13 (0.19) | |
| R peak ankle power (W/Kg) | pre | 2.19 (0.97) | 1.91 (0.82) | 1.61 (0.79) | 2.58 (1.03) |
| post | 2.45 (0.92) b | 2.50 (0.57) | 1.96 (0.93) | 2.61 (1.12) | |
| Parameter m = meters s = second | Non-AT User (n = 16) | AT User (n = 9) | |
|---|---|---|---|
| Gait speed (m/s) | pre | 0.93 (0.35) | 0.58 (0.35) |
| post | 0.98 (0.25) | 0.71 (0.37) | |
| Stride length (m) | pre | 0.97 (0.34) | 0.86 (0.28) |
| post | 1.07 (0.26) | 0.95 (0.27) | |
| Stride width (m) | pre | 0.18 (0.04) | 0.19 (0.03) |
| post | 0.19 (0.03) | 0.19 (0.04) | |
| Stride time (s) | pre | 1.17 (0.10) | 1.65 (0.37) |
| post | 1.10 (0.08) | 1.48 (0.34) | |
| Cadence (steps/min) | pre | 103.00 (8.60) | 76.84 (19.10) |
| post | 108.80 (7.52) | 86.29 (20.54) | |
| Left stance time (s) | pre | 0.77 (0.09) | 1.13 (0.42) |
| post | 0.72 (0.07) | 1.03 (0.28) | |
| Right stance time (s) | pre | 0.73 (0.06) | 1.16 (0.39) |
| post | 0.70 (0.06) | 1.01 (0.27) | |
| Left swing time (s) | pre | 0.40 (0.04) | 0.50 (0.09) |
| post | 0.38 (0.03) | 0.44 (0.08) | |
| Right swing time (s) | pre | 0.41 (0.05) | 0.48 (0.11) |
| post | 0.40 (0.,04) | 0.46 (0.09) | |
| Double limb support (s) | pre | 0.37 (0.07) | 0.69 (0.37) |
| post | 0.33 (0.06) | 0.61 (0.25) | |
| L peal knee flexion (°) | pre | 54.18 (8.94) | 50.83 (10.41) |
| post | 59.60 (6.86) | 51.38 (12.05) | |
| L peak dorsiflexion (°) | pre | 20.45 (2.56) | 17.98 (6.91) |
| post | 20.69 (3.59) | 16.19 (9.20) | |
| L peak plantarflexion (°) | pre | −14.58 (6.49) | −7.31 (11.32) |
| post | −13.81 (8.76) | −10.17 (10.58) | |
| R peak knee flexion (°) | pre | 53.87 (9.61) | 48.03 (8.53) |
| post | 59.74 (7.32) | 48.15 (16.67) | |
| R peak dorsiflexion (°) | pre | 20.86 (2.10) | 21.74 (4.31) |
| post | 21.04 (3.05) | 15.95 (10.10) | |
| R peak plantarflexion (°) | pre | −13.57 (9.20) | −6.77 (12.83) |
| post | −11.56 (7.61) | −15.87 (9.13) | |
| L peak knee flexor moment (N·m/Kg) | pre | −0.61 (0.35) | * |
| post | −0.78 (0.35) | * | |
| L peak plantar flexor moment (N·m/Kg) | pre | 1.08 (0.18) | * |
| post | 1.17 (0.31) | * | |
| L peak ankle power (W/Kg) | pre | 2.24 (0.90) | * |
| post | 2.54 (1.02) | * | |
| R peak knee flexor moment (N∙m/Kg) | pre | −0.57 (0.34) | * |
| post | −0.66 (0.41) | * | |
| R peak plantar flexor moment (N∙m/Kg) | pre | 1.08 (0.23) | * |
| post | 1.08 (0.16) | * | |
| R peak ankle power (W/Kg) | pre | 2.19 (0.97) | * |
| post | 2.45 (0.92) | * | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rippetoe, J.; Wang, H.; James, S.A.; Dionne, C.; Block, B.; Beckner, M. Improvement of Gait after 4 Weeks of Wearable Focal Muscle Vibration Therapy for Individuals with Diabetic Peripheral Neuropathy. J. Clin. Med. 2020, 9, 3767. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113767
Rippetoe J, Wang H, James SA, Dionne C, Block B, Beckner M. Improvement of Gait after 4 Weeks of Wearable Focal Muscle Vibration Therapy for Individuals with Diabetic Peripheral Neuropathy. Journal of Clinical Medicine. 2020; 9(11):3767. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113767
Chicago/Turabian StyleRippetoe, Josiah, Hongwu Wang, Shirley A. James, Carol Dionne, Bethany Block, and Matthew Beckner. 2020. "Improvement of Gait after 4 Weeks of Wearable Focal Muscle Vibration Therapy for Individuals with Diabetic Peripheral Neuropathy" Journal of Clinical Medicine 9, no. 11: 3767. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113767