Modified Clavien–Dindo Classification and Outcome Prediction in Free Flap Reconstruction among Patients with Head and Neck Cancer

Abstract
:1. Introduction
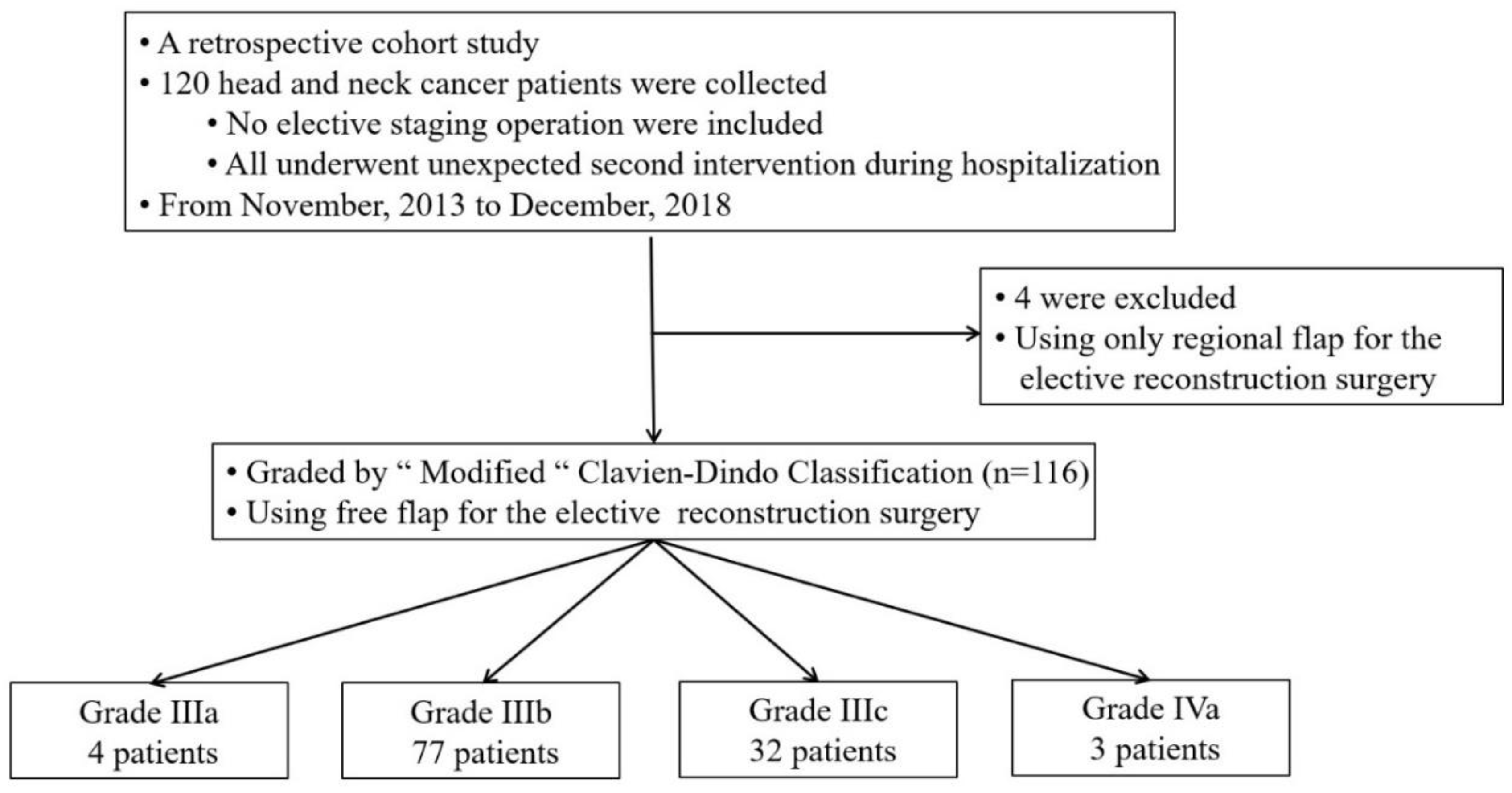
2. Material and Methods
Statistical Analysis
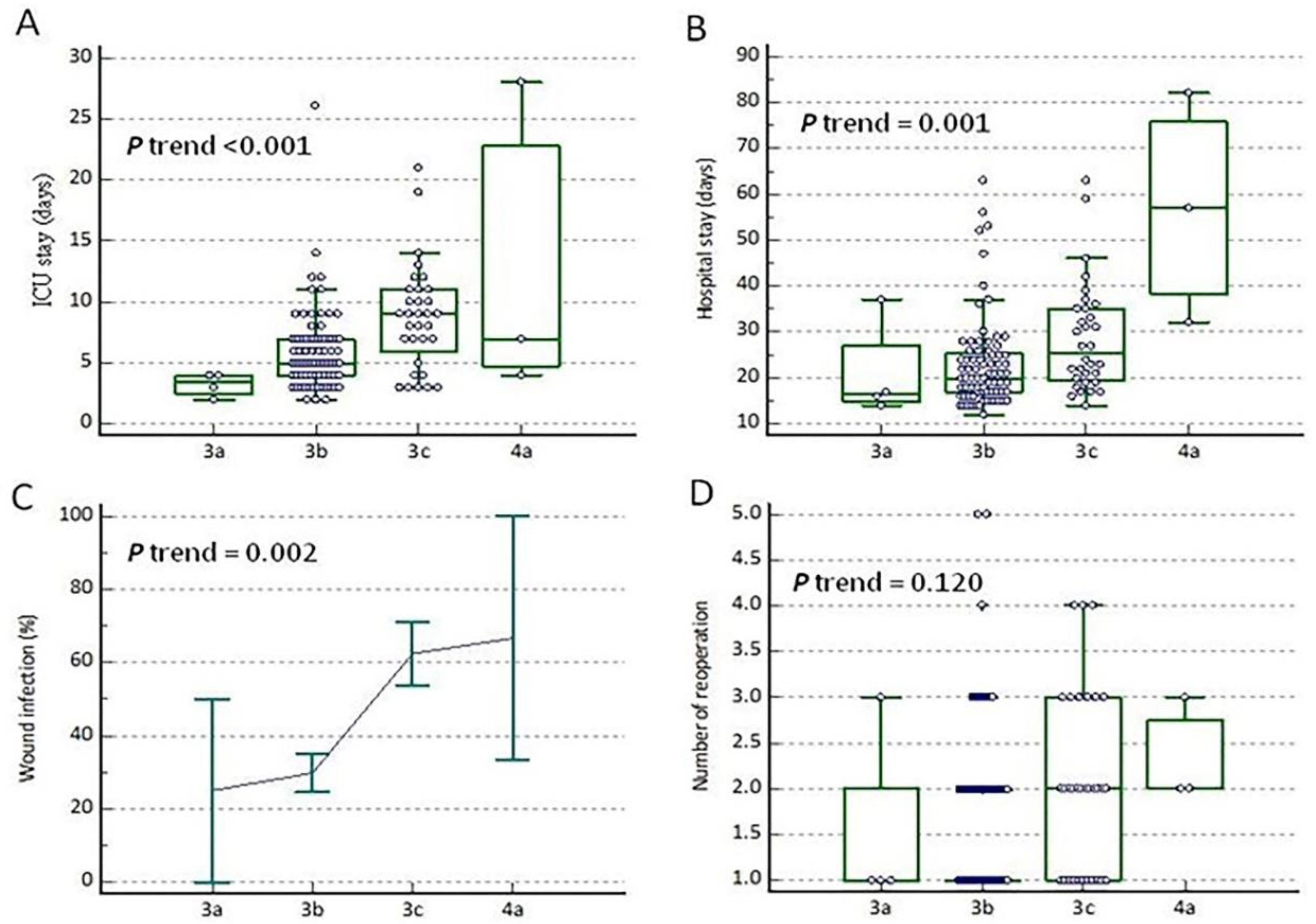
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of Surgical Complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.-A.; Barkun, J.; De Oliveira, M.L.; Vauthey, J.N.; Dindo, D.; Schulick, R.D.; De Santibañes, E.; Pekolj, J.; Slankamenac, K.; Bassi, C.; et al. The Clavien-Dindo Classification of Surgical Complications: Five-year experience. Ann. Surg. 2009, 250, 187–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perisanidis, C.; Herberger, B.; Papadogeorgakis, N.; Seemann, R.; Eder-Czembirek, C.; Tamandl, D.; Heinze, G.; Kyzas, P.A.; Kanatas, A.; Mitchell, D.; et al. Complications after free flap surgery: Do we need a standardized classification of surgical complications? Br. J. Oral Maxillofac. Surg. 2012, 50, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, E.; Sklar, M.C.; Eskander, A.; De Almeida, J.R.; Shrime, M.; Gullane, P.; Irish, J.; Gilbert, R.W.; Brown, D.H.; Higgins, K.M.; et al. Assessment of the Clavien-Dindo classification system for complications in head and neck surgery. Laryngoscope 2014, 124, 2726–2731. [Google Scholar] [CrossRef]
- Chassin, M.R.; Loeb, J.M.; Schmaltz, S.P.; Wachter, R.M. Accountability Measures—Using Measurement to Promote Quality Improvement. N. Engl. J. Med. 2010, 363, 683–688. [Google Scholar] [CrossRef] [Green Version]
- Mitropoulos, D.; Artibani, W.; Biyani, C.S.; Jensen, J.B.; Rouprêt, M.; Truss, M. Validation of the Clavien–Dindo Grading System in Urology by the European Association of Urology Guidelines Ad Hoc Panel. Eur. Urol. Focus 2018, 4, 608–613. [Google Scholar] [CrossRef]
- Sink, E.L.; Academic Network for Conservational Hip Outcomes Research Group; Leunig, M.; Zaltz, I.; Gilbert, J.C.; Clohisy, J. Reliability of a Complication Classification System for Orthopaedic Surgery. Clin. Orthop. Relat. Res. 2012, 470, 2220–2226. [Google Scholar] [CrossRef] [Green Version]
- Ivanovic, J.; Al-Hussaini, A.; Al-Shehab, D.; Threader, J.; Villeneuve, P.J.; Ramsay, T.; Maziak, D.E.; Gilbert, S.; Shamji, F.M.; Sundaresan, R.S.; et al. Evaluating the Reliability and Reproducibility of the Ottawa Thoracic Morbidity and Mortality Classification System. Ann. Thorac. Surg. 2011, 91, 387–393. [Google Scholar] [CrossRef]
- Dwyer, M.E.; Dwyer, J.T.; Cannon, G.M.; Stephany, H.A.; Schneck, F.X.; Ost, M.C. The Clavien-Dindo Classification of Surgical Complications is Not a Statistically Reliable System for Grading Morbidity in Pediatric Urology. J. Urol. 2016, 195, 460–464. [Google Scholar] [CrossRef]
- Zafereo, M.E.; Weber, R.S.; Lewin, J.S.; Roberts, D.B.; Hanasono, M.M. Complications and functional outcomes following complex oropharyngeal reconstruction. Head Neck 2009, 32, 1003–1011. [Google Scholar] [CrossRef]
- Lahtinen, S.L.; Koivunen, P.; Ala-Kokko, T.; Kaarela, O.; Ohtonen, P.; Laurila, P.; Liisanantti, J.H. Complications and outcome after free flap surgery for cancer of the head and neck. Br. J. Oral Maxillofac. Surg. 2018, 56, 684–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, N.F.; Markowitz, B.L.; Jarrahy, R.; Usa, U.L.A.C. Postoperative Medical Complications, Not Microsurgical Complications, Negatively Influence the Morbidity, Mortality, and True Costs after Microsurgical Reconstruction for Head and Neck Cancer. J. Reconstr. Microsurg. 2007, 22, 2053–2060. [Google Scholar] [CrossRef] [PubMed]
- Girod, A.; Brancati, A.; Mosseri, V.; Kriegel, I.; Jouffroy, T.; Rodriguez, J. Study of the length of hospital stay for free flap reconstruction of oral and pharyngeal cancer in the context of the new French casemix-based funding. Oral Oncol. 2010, 46, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Small, L.T.; Lampkin, M.; Vural, E.; Moreno, M.A. American Society of Anesthesiologists Class as Predictor for Perioperative Morbidity in Head and Neck Free Flaps. Otolaryngol. Neck Surg. 2019, 161, 91–97. [Google Scholar] [CrossRef]
- Las, D.E.; De Jong, T.; Zuidam, J.M.; Verweij, N.M.; Hovius, S.; Mureau, M.A.M. Identification of independent risk factors for flap failure: A retrospective analysis of 1530 free flaps for breast, head and neck and extremity reconstruction. J. Plast. Reconstr. Aesthetic Surg. 2016, 69, 894–906. [Google Scholar] [CrossRef]
- Broome, M.; Juilland, N.; Litzistorf, Y.; Monnier, Y.; Sandu, K.; Pasche, P.; Plinkert, P.K.; Federspil, P.A.; Netto, E. Factors Influencing the Incidence of Severe Complications in Head and Neck Free Flap Reconstructions. Plast. Reconstr. Surg. Glob. Open 2016, 4, e1013. [Google Scholar] [CrossRef]
- Choi, N.; Park, S.I.; Kim, H.; Sohn, I.; Jeong, H.-S. The impact of unplanned reoperations in head and neck cancer surgery on survival. Oral Oncol. 2018, 83, 38–45. [Google Scholar] [CrossRef]
- Clark, J.R.; McCluskey, S.A.; Hall, F.; Lipa, J.; Neligan, P.; Brown, D.; Irish, J.; Gullane, P.; Gilbert, R. Predictors of morbidity following free flap reconstruction for cancer of the head and neck. Head Neck 2007, 29, 1090–1101. [Google Scholar] [CrossRef]
- Ebner, J.J.; Mehra, T.; Gander, T.; Schumann, P.; Essig, H.; Zweifel, D.; Rücker, M.; Slankamenac, K.; Lanzer, M. Novel application of the Clavien-Dindo classification system and the comprehensive complications index® in microvascular free tissue transfer to the head and neck. Oral Oncol. 2019, 94, 21–25. [Google Scholar] [CrossRef] [PubMed]
- McMahon, J.; Maciver, C.; Smith, M.; Stathopoulos, P.; Wales, C.; McNulty, R.; Handley, T.P.; Devine, J.C. Postoperative complications after major head and neck surgery with free flap repair—prevalence, patterns, and determinants: A prospective cohort study. Br. J. Oral Maxillofac. Surg. 2013, 51, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Herle, P.; Shukla, L.; Morrison, W.A.; Shayan, R. Preoperative radiation and free flap outcomes for head and neck reconstruction: A systematic review and meta-analysis. ANZ J. Surg. 2015, 85, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, S.; Nakao, J.; Higashino, T.; Yoshimoto, S.; Hayashi, R.; Sakuraba, M. Clavien–Dindo classification for grading complications after total pharyngolaryngectomy and free jejunum transfer. PLoS ONE 2019, 14, e0222570. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.C.; Lin, P.-Y.; Chiang, Y.-C.; Chew, K.-Y.; Chen, C.-C.; Fujiwara, T.; Kuo, Y.-R. Influence of neck dissection and preoperative irradiation on microvascular head and neck reconstruction-Analysis of 853 cases. Microsurgery 2014, 34, 602–607. [Google Scholar] [CrossRef]
- Tsai, M.-H.; Chuang, H.-C.; Lin, Y.-T.; Lü, H.; Chen, W.-C.; Fang, F.-M.; Chien, C.-Y. Clinical impact of albumin in advanced head and neck cancer patients with free flap reconstruction—A retrospective study. PeerJ 2018, 6, e4490. [Google Scholar] [CrossRef]
- Caburet, C.; Farigon, N.; Mulliez, A.; Mom, T.; Boirie, Y.; Gilain, L.; Saroul, N. Impact of nutritional status at the outset of assessment on postoperative complications in head and neck cancer. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, S1879-7296(19), 30208. [Google Scholar] [CrossRef]
- Takase, S.; Takada, A.; Tsutsumi, M.; Matsuda, Y. Biochemical markers of chronic alcoholism. Alcohol 1985, 2, 405–410. [Google Scholar] [CrossRef]
- Teppo, A.-M.; Maury, C. Serum prealbumin, transferrm and immunoglobulins in fatty liver, alcoholic cirrhosis and primary biliary cirrhosis. Clin. Chim. Acta 1983, 129, 279–286. [Google Scholar] [CrossRef]
- Shum, J.; Markiewicz, M.R.; Park, E.; Bui, T.; Lubek, J.; Bell, R.B.; Dierks, E.J. Low Prealbumin Level Is a Risk Factor for Microvascular Free Flap Failure. J. Oral Maxillofac. Surg. 2014, 72, 169–177. [Google Scholar] [CrossRef]
- Chiu, Y.-H.; Chang, D.-H.; Perng, C.-K. Vascular Complications and Free Flap Salvage in Head and Neck Reconstructive Surgery. Ann. Plast. Surg. 2017, 78, S83–S88. [Google Scholar] [CrossRef] [PubMed]
- Kucur, C.; Durmus, K.; Uysal, I.O.; Old, M.; Agrawal, A.; Arshad, H.; Teknos, T.N.; Ozer, E. Management of complications and compromised free flaps following major head and neck surgery: Analysis of 150 Cases of Reexploration. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Kao, H.-K.; Chang, K.-P.; Ching, W.-C.; Tsao, C.-K.; Cheng, M.-H.; Wei, F.-C. The impacts of liver cirrhosis on head and neck cancer patients undergoing microsurgical free tissue transfer: An evaluation of flap outcome and flap-related complications. Oral Oncol. 2009, 45, 1058–1062. [Google Scholar] [CrossRef] [PubMed]
- Handschel, P.D.D.J.; Burghardt, S.; Naujoks, C.; Kübler, N.R.; Giers, G. Parameters predicting complications in flap surgery. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 589–594. [Google Scholar] [CrossRef]
- Lahtinen, S.L.; Koivunen, P.; Ala-Kokko, T.; Laurila, P.; Kaarela, O.; Liisanantti, J.H. Quality of life after free flap surgery for cancer of the head and neck in patients with or without postoperative complications. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 2575–2584. [Google Scholar] [CrossRef]
- Clavien, P.A.; Sanabria, J.R.; Strasberg, S.M. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 1992, 111, 518–526. [Google Scholar]



{kind=link}
{kind=link}
| Complications | Grade IIIa | Grade IIIb | Grade IIIc | Grade IVa | Total |
|---|---|---|---|---|---|
| Hematoma evacuation | 0 | 29 (37.7%) * | 5 (15.6%) | 0 | 34 (29.3%) |
| Wound dehiscence | 3 (75%) * | 12 (15.6%) | 8 (25%) | 1 (33.3%) | 24 (20.7%) |
| Vascular complication | 1 (25%) | 57 (74%) * | 32 (100%) | 3 (100%) | 93 (80.2%) |
| Lymph leakage | 0 | 2 (2.6%) * | 0 | 0 | 2 (1.7%) |
| Fistula formation | 0 | 3 (3.9%) | 2 (6.3%) | 1 (33.3%) | 6 (5.2%) |
| Grade IIIb | Grade IIIc | p | |
|---|---|---|---|
| Characteristics | |||
| Patient number | 77 | 32 | - |
| Age (years) | 56.3 ± 10.6 | 56.0 ± 11.1 | 0.901 |
| Male | 72 (93.5) | 27 (84.4) | 0.154 |
| Body mass index (kg/m2) | 23.7 ± 4.6 | 24.8 ± 3.3 | 0.263 |
| Current or former smoker | 62 (80.5) | 24 (75.0) | 0.608 |
| Alcoholism | 56 (72.7) | 16 (50.0) | 0.028 * |
| Comorbidity | |||
| Diabetes mellitus | 23 (29.9) | 10 (31.3) | 1.000 |
| Hypertension | 37 (48.1) | 14 (43.8) | 0.833 |
| ASA classification | 1.000 | ||
| 1–2 | 40 (51.9) | 17 (53.1) | |
| 3–4 | 37 (48.1) | 15 (46.9) | |
| Charlson Comorbidity Index score | 4.2 ± 1.7 | 3.8 ± 1.5 | 0.219 |
| Previous operation | 29 (37.7) | 19 (59.4) | 0.056 |
| Previous C/T | 22 (28.6) | 11 (34.4) | 0.648 |
| Previous R/T | 26 (33.8) | 12 (37.5) | 0.826 |
| Surgical etiology | |||
| Primary malignancy | 49 (63.6) | 14 (43.8) | 0.088 |
| Recurrent/Residual cancer | 20 (26.0) | 14 (43.8) | 0.075 |
| Previous free flap reconstruction | 10 (13.0) | 5 (15.6) | 0.763 |
| Cancer status | |||
| T stage | 0.520 | ||
| 1–2 | 32 (42.7) | 11 (34.4) | |
| 3–4 | 43 (57.3) | 21 (65.6) | |
| N stage | 0.667 | ||
| 0–1 | 40 (55.6) | 19 (61.3) | |
| >1 | 32 (44.4) | 12 (38.7) | |
| Overall cancer stage | 0.321 | ||
| Early | 19 (25.3) | 5 (15.6) | |
| Advanced | 56 (74.7) | 27 (84.4) | |
| Associated surgical procedures | |||
| Tracheostomy | 64 (83.1) | 27 (84.4) | 1.000 |
| Neck dissection | 55 (71.4) | 18 (56.3) | 0.179 |
| Outcome | Grade IIIb | Grade IIIc | p | B or Odds Ratio (95% CI) | p |
|---|---|---|---|---|---|
| Categorical variable | |||||
| Wound infection (%) | 23 (29.9) | 20 (62.5) | 0.002 * | 3.91 (1.65–9.30) | 0.002 * |
| Continuous variable | |||||
| Reoperation times during the current hospitalization | 1.4 ± 0.8 | 2.0 ± 1.0 | <0.001 * | 2.21 (1.45, 2.97) | <0.001 * |
| ICU stay (day) | 6.0 ± 3.4 | 8.7 ± 4.3 | 0.001 * | 2.71 (1.17, 4.24) | 0.001 * |
| Hospital stay (day) | 23.1 ± 10.1 | 28.6 ± 11.9 | 0.015 * | 0.20 (0.15, 0.25) | <0.001 * |
| Grade | Definition |
|---|---|
| I | Any deviation from the normal postoperative course without the need for pharmacological treatment or surgical, endoscopic, or radiological interventions |
| II | Requiring pharmacological treatment with drugs other than those permitted for grade I complication (would include blood transfusions and total parenteral nutrition) |
| III | Requiring surgical, endoscopic, or radiological intervention |
| IIIa | Intervention not under general anesthesia |
| IIIb | Intervention under general anesthesia |
| IIIc | “Partial or total free flap failure after intervention” needing further surgery under general anesthesia |
| IV | Life-threatening complication (including complications of the central nervous system) that requires management in a high dependency or intensive therapy unit |
| IVa | Single organ dysfunction (including dialysis) |
| IVb | Multiorgan dysfunction |
| V | Death |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jan, W.-L.; Chen, H.-C.; Chang, C.-C.; Chen, H.-H.; Shih, P.-K.; Huang, T.-C. Modified Clavien–Dindo Classification and Outcome Prediction in Free Flap Reconstruction among Patients with Head and Neck Cancer. J. Clin. Med. 2020, 9, 3770. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113770
Jan W-L, Chen H-C, Chang C-C, Chen H-H, Shih P-K, Huang T-C. Modified Clavien–Dindo Classification and Outcome Prediction in Free Flap Reconstruction among Patients with Head and Neck Cancer. Journal of Clinical Medicine. 2020; 9(11):3770. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113770
Chicago/Turabian StyleJan, Wei-Ling, Hung-Chi Chen, Chang-Cheng Chang, Hsin-Han Chen, Pin-Keng Shih, and Tsung-Chun Huang. 2020. "Modified Clavien–Dindo Classification and Outcome Prediction in Free Flap Reconstruction among Patients with Head and Neck Cancer" Journal of Clinical Medicine 9, no. 11: 3770. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113770