Effectiveness of Active Therapy-Based Training to Improve the Balance in Patients with Fibromyalgia: A Systematic Review with Meta-Analysis


 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Design
2.2. Data Sources and Search Strategy
2.3. Study Selection and Inclusion Criteria
2.4. Data Extraction
2.5. Outcome Measures
2.6. Quality Assessment
2.7. Statistical Analysis
2.8. Additional Analysis
3. Results
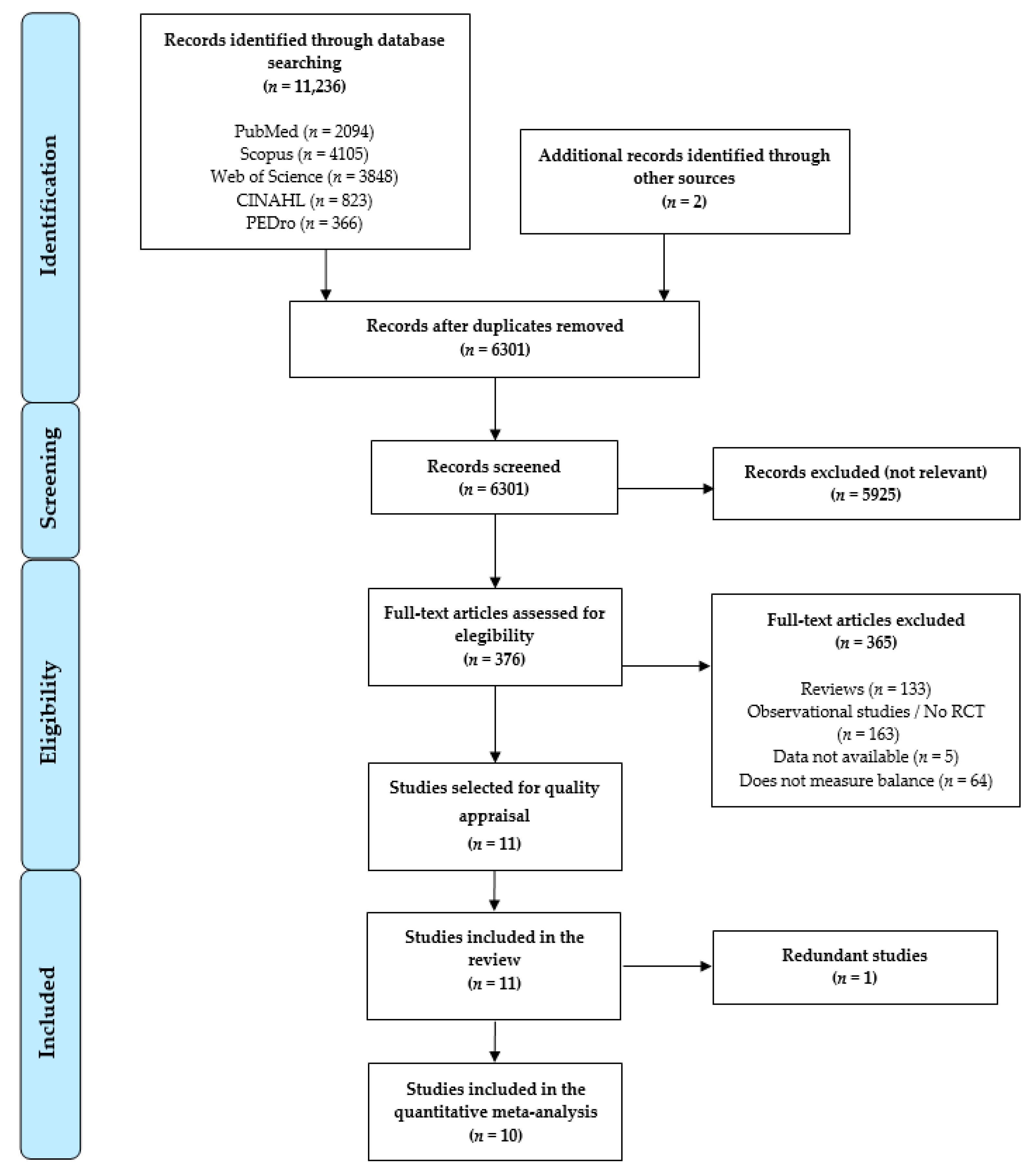
3.1. Study Selection
3.2. Characteristics of the Studies Included in the Review
3.3. Quality Assessment of the Studies Included in the Review
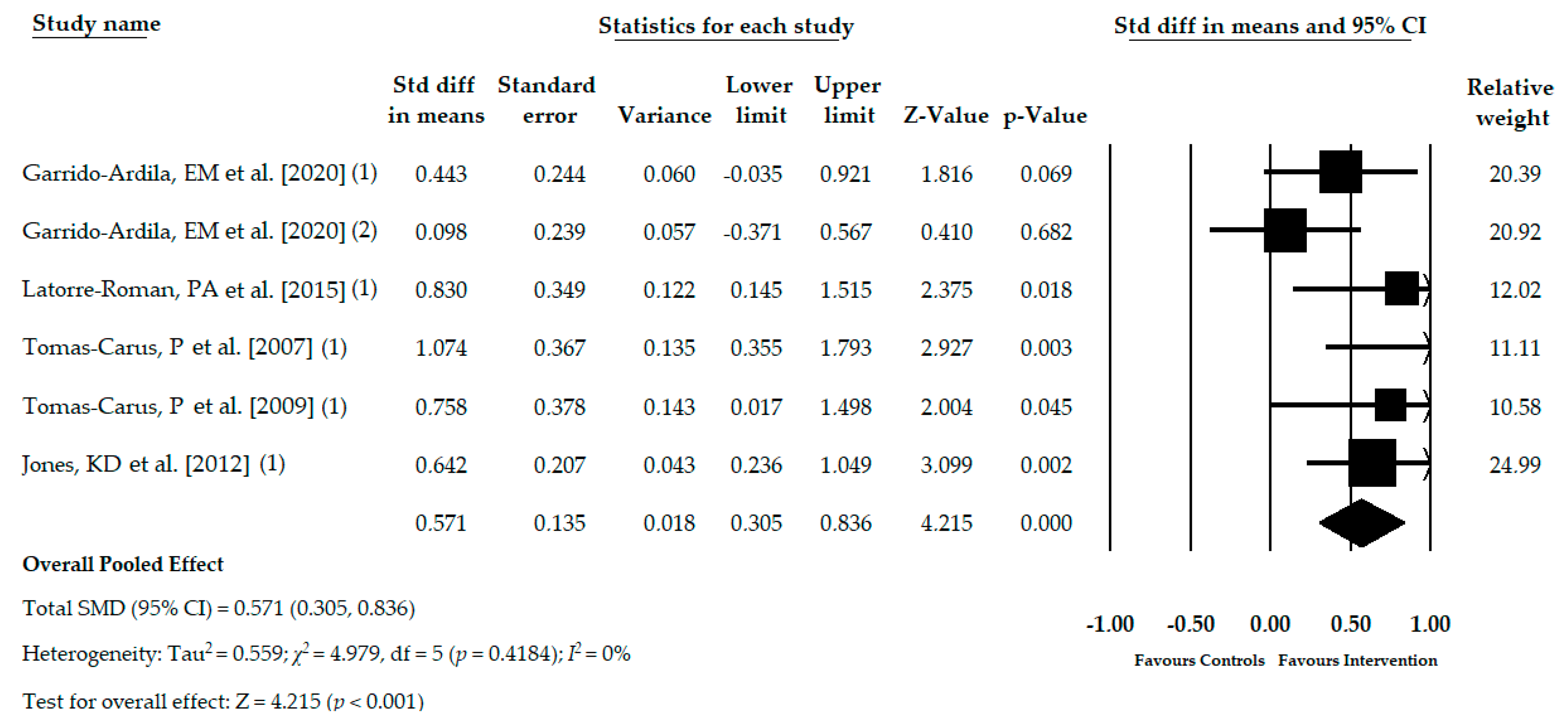
3.4. Meta-Analysis of the Immediate Effect of the ATBT in Monopedal Static Balance
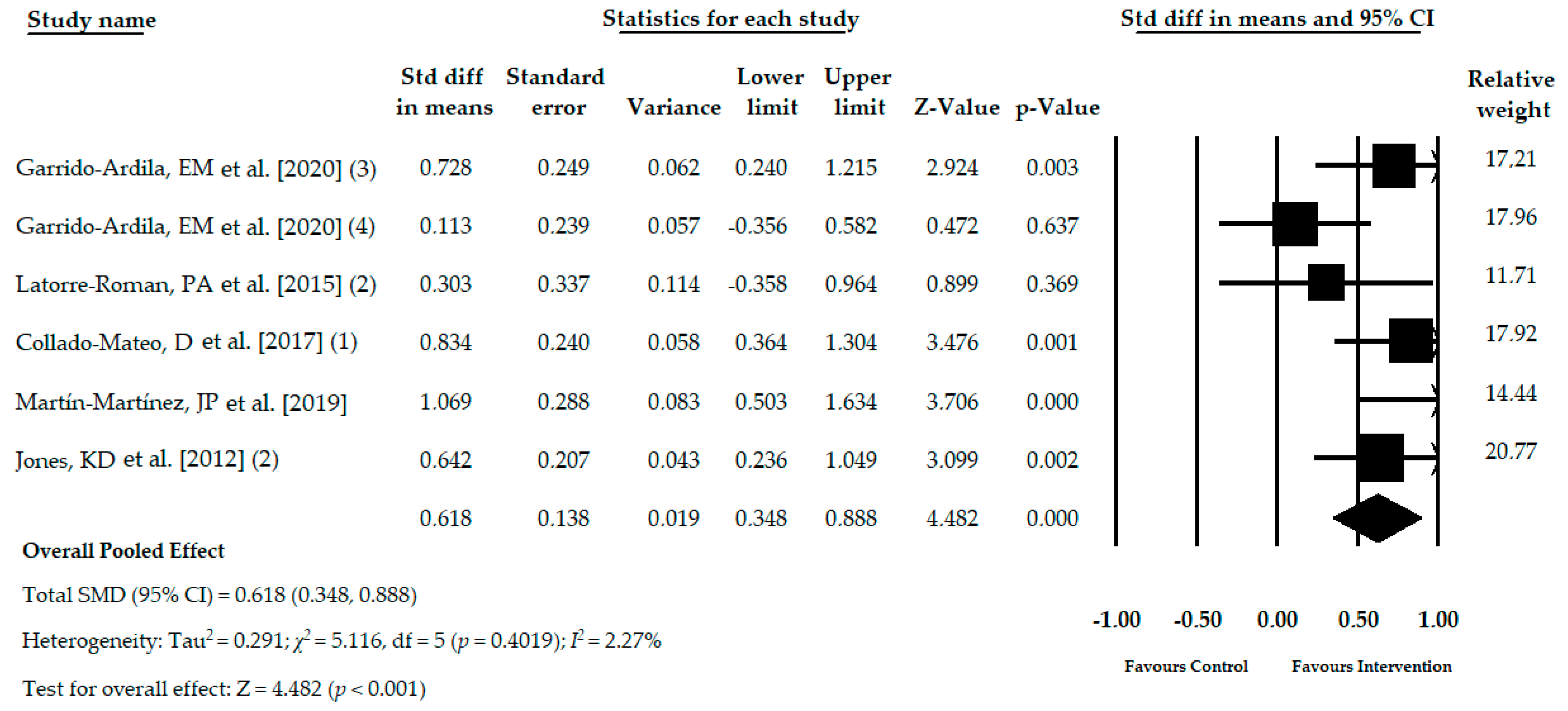
3.5. Meta-Analysis of the Immediate Effect of the ATBT in Dynamic Balance
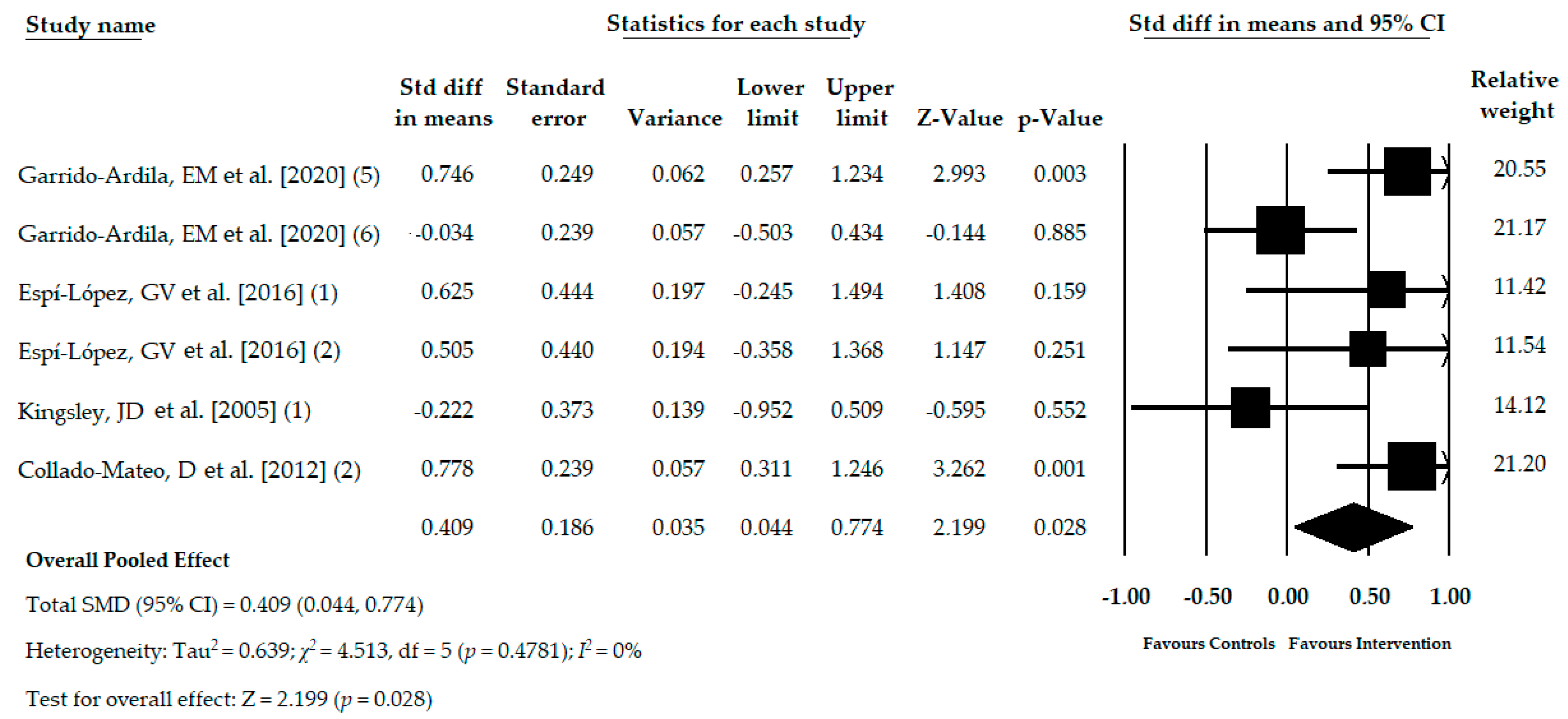
3.6. Meta-Analysis of the Immediate Effect of the ATBT in Functional Balance
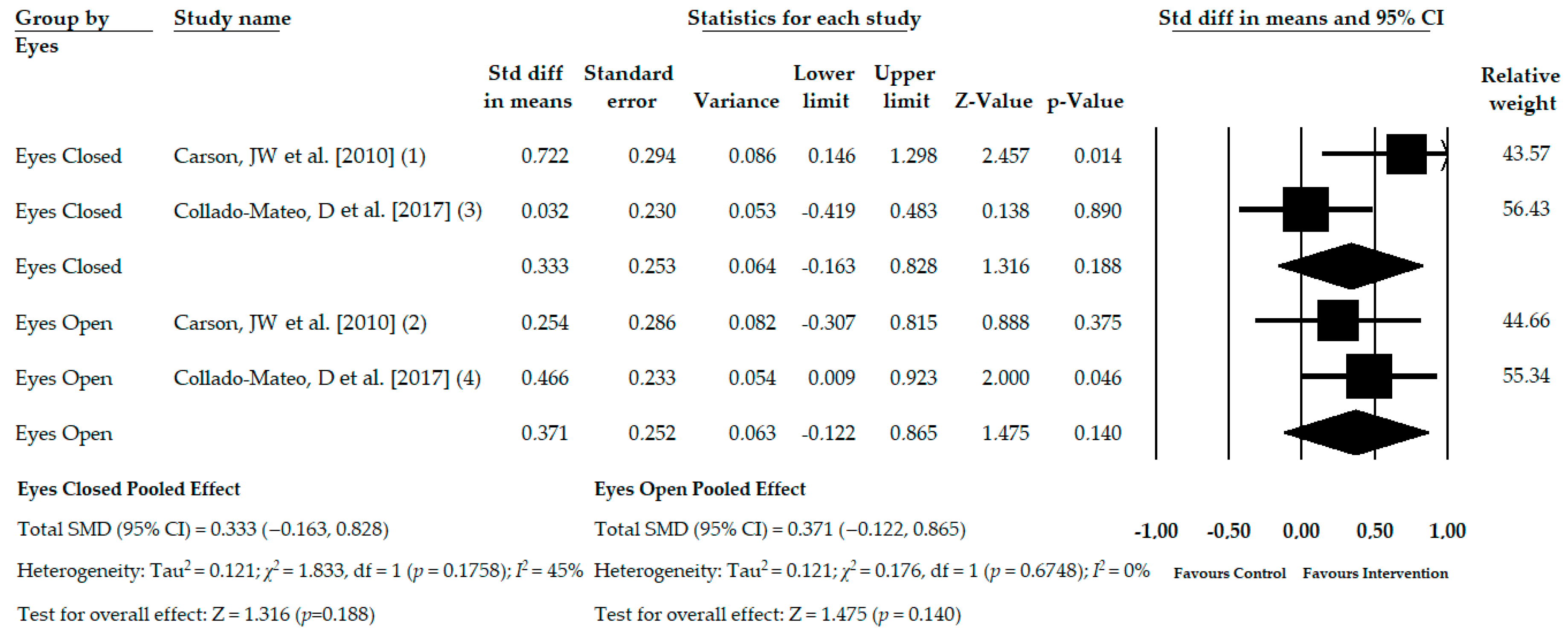
3.7. Meta-Analysis of the Immediate Effect of ATBT on Balance on an Unstable Support with Open and Closed Eyes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Galvez-Sánchez, C.M.; Reyes del Paso, G.A. Diagnostic Criteria for Fibromyalgia: Critical Review and Future Perspectives. J. Clin. Med. 2020, 9, 1219. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.P.; Santo, A.d.S.d.E.; Berssaneti, A.A.; Matsutani, L.A.; Yuan, S.L.K. Prevalence of fibromyalgia: Literature review update. Rev. Bras. Reum. Engl. Ed. 2017, 57, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Marcus, D.A.; Richards, K.L.; Chambers, J.F.; Bhowmick, A. Fibromyalgia Family and Relationship Impact Exploratory Survey. Musculoskelet. Care 2013, 11, 125–134. [Google Scholar] [CrossRef]
- Steiner, J.L.; Bigatti, S.M.; Hernandez, A.M.; Lydon-Lam, J.R.; Johnston, E.L. Social support mediates the relations between role strains and marital satisfaction in husbands of patients with fibromyalgia syndrome. Fam. Syst. Health 2010, 28, 209–223. [Google Scholar] [CrossRef]
- Mas, A.; Carmona, L.; Valverde, M.; Ribas, B.; EPISER Study Group. Prevalence and impact of fibromyalgia on function and quality of life in individuals from the general population: Results from a nationwide study in Spain. Clin. Exp. Rheumatol. 2008, 26, 519–526. [Google Scholar]
- Galvez-Sánchez, C.M.; Duschek, S.; Reyes del Paso, G.A. Psychological impact of fibromyalgia: Current perspectives. Psychol. Res. Behav. Manag. 2019, 12, 117–127. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Sancassiani, F.; Machado, S.; Ruggiero, V.; Cacace, E.; Carmassi, C.; Gesi, C.; Dell’Osso, L.; Carta, M.G. The management of fibromyalgia from a psychosomatic perspective: An overview. Int. Rev. Psychiatry 2017, 29, 473–488. [Google Scholar] [CrossRef]
- Peinado-Rubia, A.; Osuna-Pérez, M.C.; Rodríguez-Almagro, D.; Zagalaz-Anula, N.; López-Ruiz, M.C.; Lomas-Vega, R. Impaired Balance in Patients with Fibromyalgia Syndrome: Predictors of the Impact of This Disorder and Balance Confidence. Int. J. Environ. Res. Public Health 2020, 17, 3160. [Google Scholar] [CrossRef]
- Jones, K.D.; Horak, F.B.; Winters-Stone, K.; Irvine, J.M.; Bennett, R.M. Fibromyalgia is associated with impaired balance and falls. J. Clin. Rheumatol. Pr. Rep. Rheum. Musculoskelet. Dis. 2009, 15, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, K.D.; King, L.A.; Mist, S.D.; Bennett, R.M.; Horak, F.B. Postural control deficits in people with fibromyalgia: A pilot study. Arthritis Res. 2011, 13, R127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meireles, S.A.; Antero, D.C.; Kulczycki, M.M.; Skare, T.L. Prevalence of falls in fibromyalgia patients. Acta Ortop. Bras. 2014, 22, 163–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutledge, D.N.; Martinez, A.; Traska, T.K.; Rose, D.J. Fall experiences of persons with fibromyalgia over 6 months. J. Adv. Nurs. 2013, 69, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Sosa-Reina, M.D.; Nunez-Nagy, S.; Gallego-Izquierdo, T.; Pecos-Martín, D.; Monserrat, J.; Álvarez-Mon, M. Effectiveness of Therapeutic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Biomed. Res. Int. 2017, 2017, 1–14. [Google Scholar] [CrossRef]
- Andrade, A.; De Azevedo Klumb Steffens, R.; Sieczkowska, S.M.; Peyré Tartaruga, L.A.; Torres Vilarino, G. A systematic review of the effects of strength training in patients with fibromyalgia: Clinical outcomes and design considerations. Adv. Rheumatol. 2018, 58, 36. [Google Scholar] [CrossRef] [Green Version]
- Bidonde, J.; Busch, A.J.; Schachter, C.L.; Webber, S.C.; Musselman, K.E.; Overend, T.J.; Góes, S.M.; Dal Bello-Haas, V.; Boden, C. Mixed exercise training for adults with fibromyalgia. Cochrane Database Syst. Rev. 2019. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Intervention Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef] [Green Version]
- Atkins, D.; Best, D.; Briss, P.A.; Eccles, M.; Falck-Ytter, Y.; Flottorp, S.; Guyatt, G.H.; Harbour, R.T. Grading quality of evidence and strength of recommendations. BMJ 2004, 328, 1490. [Google Scholar] [CrossRef] [Green Version]
- Meader, N.; King, K.; Llewellyn, A.; Norman, G.; Brown, J.; Rodgers, M.; Moe-Byrne, T.; Higgins, J.P.; Sowden, A.; Stewart, G. A checklist designed to aid consistency and reproducibility of GRADE assessments: Development and pilot validation. Syst. Rev. 2014, 3, 82. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, H.; Hedges, L.V.; Valentine, J.C. The Handbook of Research Synthesis and Meta-Analysis; Russell Sage Foundation: New York, NY, USA, 2009. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Faraone, S.V. Interpreting estimates of treatment effects: Implications for managed care. P T 2008, 33, 700–711. [Google Scholar] [PubMed]
- Rücker, G.; Schwarzer, G. Beyond the forest plot: The drapery plot. Res. Synth. Methods 2020. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.; Thompson, S.; Deeks, J.; Altman, D. Statistical heterogeneity in systematic reviews of clinical trials: A critical appraisal of guidelines and practice. J. Health Serv. Res. Policy 2002, 7, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test measures of funnel plot asymmetry. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Garrido-Ardila, E.M.; González-López-Arza, M.V.; Jiménez-Palomares, M.; García-Nogales, A.; Rodríguez-Mansilla, J. Effectiveness of acupuncture vs. core stability training in balance and functional capacity of women with fibromyalgia: A randomized controlled trial. Clin. Rehabil. 2020, 34, 630–645. [Google Scholar] [CrossRef]
- Latorre Román, P.Á.; Santos e Campos, M.A.; García-Pinillos, F. Effects of functional training on pain, leg strength, and balance in women with fibromyalgia. Mod. Rheumatol. 2015, 25, 943–947. [Google Scholar] [CrossRef]
- Tomas-Carus, P.; Hakkinen, A.; Gusi, N.; Leal, A.; Hakkinen, K.; Ortega-Alonso, A. Aquatic Training and Detraining on Fitness and Quality of Life in Fibromyalgia. Med. Sci. Sport Exerc. 2007, 39, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.D.; Sherman, C.A.; Mist, S.D.; Carson, J.W.; Bennett, R.M.; Li, F. A randomized controlled trial of 8-form Tai chi improves symptoms and functional mobility in fibromyalgia patients. Clin. Rheumatol. 2012, 31, 1205–1214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomas-Carus, P.; Gusi, N.; Hakkinen, A.; Hakkinen, K.; Raimundo, A.; Ortega-Alonso, A. Improvements of muscle strength predicted benefits in HRQOL and postural balance in women with fibromyalgia: An 8-month randomized controlled trial. Rheumatology 2009, 48, 1147–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Espí-López, G.V.; Inglés, M.; Ruescas-Nicolau, M.-A.; Moreno-Segura, N. Effect of low-impact aerobic exercise combined with music therapy on patients with fibromyalgia. A pilot study. Complement. Med. 2016, 28, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Kingsley, J.D.; Panton, L.B.; Toole, T.; Sirithienthad, P.; Mathis, R.; McMillan, V. The Effects of a 12-Week Strength-Training Program on Strength and Functionality in Women With Fibromyalgia. Arch. Phys. Med. Rehabil. 2005, 86, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Collado-Mateo, D.; Dominguez-Muñoz, F.J.; Adsuar, J.C.; Merellano-Navarro, E.; Gusi, N. Exergames for women with fibromyalgia: A randomised controlled trial to evaluate the effects on mobility skills, balance and fear of falling. PeerJ 2017, 5, e3211. [Google Scholar] [CrossRef] [Green Version]
- Carson, J.W.; Carson, K.M.; Jones, K.D.; Bennett, R.M.; Wright, C.L.; Mist, S.D. A pilot randomized controlled trial of the Yoga of Awareness program in the management of fibromyalgia. Pain 2010, 151, 530–539. [Google Scholar] [CrossRef]
- Martín-Martínez, J.P.; Villafaina, S.; Collado-Mateo, D.; Pérez-Gómez, J.; Gusi, N. Effects of 24-week exergame intervention on physical function under single- and dual-task conditions in fibromyalgia: A randomized controlled trial. Scand. J. Med. Sci. Sports 2019, 29, 1610–1617. [Google Scholar] [CrossRef]
- Thomas, E.; Battaglia, G.; Patti, A.; Brusa, J.; Leonardi, V.; Palma, A.; Bellafiore, M. Physical activity programs for balance and fall prevention in elderly A systematic review. Medicine 2019, 98, e16218. [Google Scholar] [CrossRef]
- Halabchi, F.; Alizadeh, Z.; Sahraian, M.A.; Abolhasani, M. Exercise prescription for patients with multiple sclerosis; potential benefits and practical recommendations. BMC Neurol. 2017, 17, 185. [Google Scholar] [CrossRef]
- Shen, X.; Wong-Yu, I.S.K.; Mak, M.K.Y. Review Effects of Exercise on Falls, Balance, and Gait Ability in Parkinson’s Disease: A Meta-analysis. Neurorehabil. Neural Repair 2015, 30, 512–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrade, A.; Dominski, F.H.; Sieczkowska, S.M. What we already know about the effects of exercise in patients with fibromyalgia: An umbrella review. Semin. Arthritis Rheum. 2020. [Google Scholar] [CrossRef] [PubMed]
- Lj, G.; Moore, R.; Clarke, C.; Martin, D.; Colvin, L.; Smith, B. Physical activity and exercise for chronic pain in adults: An overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 14, CD011279. [Google Scholar] [CrossRef]
- Vøllestad, N.K.; Mengshoel, A.M. Relationships between neuromuscular functioning, disability and pain in fibromyalgia. Disabil. Rehabil. 2005, 27, 667–673. [Google Scholar] [CrossRef]
- Okumus, M.; Gokoglu, F.; Kocaoglu, S.; E Ceceli, Z.R.Y. Muscle performance in patients with fibromyalgia—PubMed. Singap. Med. J. 2006, 47, 752–756. [Google Scholar]
- Muehlbauer, T.; Gollhofer, A.; Granacher, U. Associations between Measures of Balance and Lower-Extremity Muscle Strength/Power in Healthy Individuals across the Lifespan: A Systematic Review and Meta-Analysis. Sport Med. 2015, 45, 1671–1692. [Google Scholar] [CrossRef] [Green Version]
- Góes, S.M.; Leite, N.; Shay, B.L.; Homann, D.; Stefanello, J.M.F.; Rodacki, A.L.F. Functional capacity, muscle strength and falls in women with fibromyalgia. Clin. Biomech. 2012, 27, 578–583. [Google Scholar] [CrossRef]
- De Lima, L.O.; Zicarelli, C.A.M.; Matsumura, A.S.; Moroti-Perugini, L.R.; De Castro Teixeira, D.; Fernandes, K.B.P.; De Oliveira Perrucini, P.D.; Poli-Frederico, R.C. Lower limb muscle strength and serotonin receptor gene polymorphism as factors associated in women with fibromyalgia. Adv. Rheumatol. 2019, 59, 59. [Google Scholar] [CrossRef]
- Grayston, R.; Czanner, G.; Elhadd, K.; Goebel, A.; Frank, B.; Üçeyler, N.; Malik, R.A.; Alam, U. A systematic review and meta-analysis of the prevalence of small fiber pathology in fibromyalgia: Implications for a new paradigm in fibromyalgia etiopathogenesis. Semin. Arthritis Rheum. 2019, 48, 933–940. [Google Scholar] [CrossRef]
- Zhang, S.; Manor, B.; Li, L. H-index is important for postural control for people with impaired foot sole sensation. PLoS ONE 2015, 10, e0121847. [Google Scholar] [CrossRef]
- Busch, A.J.; Webber, S.C.; Brachaniec, M.; Bidonde, J.; Bello-Haas, V.D.; Danyliw, A.D.; Overend, T.J.; Richards, R.S.; Sawant, A.; Schachter, C.L. Exercise therapy for fibromyalgia. Curr. Pain Headache Rep. 2011, 15, 358–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohm, S.; Mersmann, F.; Bierbaum, S.; Dietrich, R.; Arampatzis, A. Cognitive demand and predictive adaptational responses in dynamic stability control. J. Biomech. 2012, 45, 2330–2336. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Gao, Y.; Wang, J. Effects of vision and cognitive load on anticipatory and compensatory postural control. Hum. Mov. Sci. 2019, 64, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Bell, T.; Trost, Z.; Buelow, M.T.; Clay, O.; Younger, J.; Moore, D.; Crowe, M. Meta-analysis of cognitive performance in fibromyalgia. J. Clin. Exp. Neuropsychol. 2018, 40, 698–714. [Google Scholar] [CrossRef]
- Munguía-Izquierdo, D.; Legaz-Arrese, A. Exercise in warm water decreases pain and improves cognitive function in middle-aged women with fibromyalgia. Clin. Exp. Rheumatol. 2007, 25, 823–830. [Google Scholar]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-Analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Mura, G.; Carta, M.G.; Sancassiani, F.; Machado, S.; Prosperini, L. Active exergames to improve cognitive functioning in neurological disabilities: A systematic review and meta-analysis. Eur. J. Phys. Rehabil. Med. 2018, 54, 450–462. [Google Scholar] [CrossRef]
- Pérez-de-Heredia-Torres, M.; Huertas-Hoyas, E.; Martínez-Piédrola, R.; Palacios-Ceña, D.; Alegre-Ayala, J.; Santamaría-Vázquez, M.; Fernández-de-Las-Peñas, C. Balance deficiencies in women with fibromyalgia assessed using computerised dynamic posturography: A cross-sectional study in Spain. BMJ Open 2017, 7, e016239. [Google Scholar] [CrossRef]
- Serrador, J.M.; Quigley, K.S.; Zhao, C.; Findley, T.; Natelson, B.H. Balance deficits in Chronic Fatigue Syndrome with and without fibromyalgia. NeuroRehabilitation 2018, 42, 235–246. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Databases | Search Strategy |
|---|---|
| PubMed Medline | (fatigue syndrome, chronic[mh] OR fatigue syndrome, chronic[tiab] OR fibromyalgia[mh] OR fibromyalgia[tiab]) AND (exercise[mh] OR exercise[tiab] OR exercise therapy[mh] OR exercise therapy[tiab] OR physical exercise[tiab] OR physical activity[tiab] OR training[tiab]) |
| SCOPUS | TITLE-ABS-KEY ((“chronic fatigue syndrome” OR “fibromyalgia” OR “fibromyalgia syndrome”) AND (“exercise” OR “exercise” OR “physical exercise” OR “physical activity” OR “exercise therapy” OR “training”)) |
| Web of Science | TOPIC: (* chronic fatigue syndrome * OR * fibromyalgia * OR * fibromyalgia syndrome *) AND TOPIC: (* exercise * OR * physical exercise * OR * physical activity * OR * exercise therapy * OR * training *) |
| CINAHL | AB (“chronic fatigue syndrome” OR fibromyalgia) AND AB (exercise OR “exercise therapy” OR “physical activity” OR training) |
| PEDro | Fibromyalgia AND exercise |
| Experimental Group | Control Group | Outcome | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample Characteristics | Intervention Characteristics | Sample Characteristics | Control Type | Balance Condition | Test | |||||||||||||
| Author and Year | Country | K | N | Ne | Mean Age | Mean BMI | % Fem | Type | Weeks | Ses /Week | Min | Nc | Mean Age | Mean BMI | % Fem | |||
| Garrido-Ardila, EM et al. (2020) [32] | Spain | 6 | 103 | 36 | 56.1 | - | 100% | Core Stability | 6 | 2 | 30 | 33 | 54.4 | - | 100% | NI | -Monopedal static -Dynamic -Functional | -OLST -TGUGT -BBS |
| 34 | 56.1 | - | 100% | Acupunc | ||||||||||||||
| LaTorre-Román, PA et al. (2015) [33] | Spain | 2 | 36 | 20 | 51.7 | 26.2 | 100% | Active-functional training | 18 | 3 | 60 | 16 | 50.2 | 26.5 | 100% | NI | -Monopedal static -Dynamic | -OLST -TGUGT |
| Tomas-Carus, P et al. (2007) [34] | Spain | 2 | 34 | 17 | 51 | 27 | 100% | Aquatic PA | 12 | 3 | 60 | 17 | 51 | 27 | 100% | NI | -Monopedal static | -OLST |
| Jones, KD et al. (2012) [35] | USA | 2 | 98 | 51 | 53.3 | 30.9 | 97% | Tai Chi | 12 | 2 | 90 | 47 | 54.8 | 30.1 | 93% | Health education | -Monopedal static -Dynamic | -OLST -TGUGT |
| Tomas-Carus, P et al. (2009) [36] | Spain | 1 | 30 | 15 | 50.7 | 28.8 | 100% | Aquatic PA | 32 | 3 | 60 | 15 | 50.9 | 26.6 | 100% | NI | -Monopedal static | -OLST |
| Espí-López, GV et al. (2016) [37] | Spain | 2 | 35 | 13 | 53.1 | 27 | 93% | PE + music | 8 | 2 | 60 | 9 | 57.1 | 26.3 | 100% | NI | -Functional | -BBS |
| 13 | 51.2 | 26.3 | 93% | PE not music | ||||||||||||||
| Kingsley, JD et al. (2005) [38] | USA | 1 | 29 | 14 | 45 | 30.3 | 100% | PE | 12 | 2 | 30 | 15 | 47 | 32 | 100% | NI | -Functional | -CS-PFP balance |
| Collado-Mateo, D et al. (2017) [39] | Spain | 4 | 76 | 41 | 52.4 | 25.7 | 100% | Exerg. PE | 8 | 2 | 60 | 35 | 52.5 | 27.7 | 100% | NI | -Functional -Dynamic -Unstable support | -FRT -TGUGT -CTSIB |
| Carson, JW et al. (2010) [40] | USA | 2 | 50 | 22 | 51.4 | - | 100% | Yoga | 8 | 1 | - | 28 | 55.8 | 28 | 100% | Usual Care | -Unstable support | -SCBT |
| Martín-Martínez, JP et al. (2019) [41] | Spain | 1 | 55 | 28 | 54.04 | 27.36 | 100 | Exerg. PE | 24 | 2 | 60 | 27 | 53.4 | 28.8 | 100 | NI | -Dynamic | -TGUGT |
| Selection Bias | Performance Bias | Detection Bias | Attrition Bias | Reporting Bias | Other Bias | ||
|---|---|---|---|---|---|---|---|
| Author and Year | Random Sequence Generation | Concealment of Randomization Sequence | Blinding of Participants | Blinding of Outcomes Assessors | Incomplete Outcome Data | Selective Reporting | Other, Ideally Prespecified |
| Garrido-Ardila, EM et al. (2020) [32] | - | - | + | - | - | - | - |
| LaTorre-Román, PA et al. (2015) [33] | - | ? | + | ? | ? | - | - |
| Tomas-Carus, P et al. (2007) [34] | - | ? | + | ? | ? | - | - |
| Jones, KD et al. (2012) [35] | - | + | + | + | ? | - | - |
| Tomas-Carus, P et al. (2009) [36] | ? | - | + | - | - | - | - |
| Espí-López, GV et al. (2016) [37] | - | - | + | - | - | - | - |
| Kingsley, JD et al. (2005) [38] | - | ? | + | - | - | - | - |
| Collado-Mateo, D et al. (2017) [39] | - | - | + | - | - | - | - |
| Carson, JW et al. (2010) [40] | - | - | + | - | - | - | - |
| Martín-Martínez, JP et al. (2019) [41] | - | - | + | - | - | - | - |
| Summary of Findings | Quality of Evidence (GRADE) | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pooled Effect | Het. | Publication Bias | ||||||||||||||
| K | N | Ns | SMD | 95% CI | I2 (p) | Funnel Plot Egger Test (p) | Trim and Fill | Risk of Bias | Incons. | Indirect. | Imprec. | Pub. Bias | Quality | |||
| Adj SMD | % of Var | |||||||||||||||
| Monopedal Static Balance | ||||||||||||||||
| Overall | 6 | 336 | 56 | 0.571 | 0.305, 0.836 | 0% (0.4184) | Asym. (0.11) | 0.477 | 20% | Medium | No | No | Yes | Likely | Low | |
| Dynamic Balance | ||||||||||||||||
| Overall | 6 | 403 | 78.5 | 0.618 | 0.348, 0.888 | 2.2% (0.4019) | Sym. (0.49) | 0.618 | 0% | Medium | Not rel. | No | Yes | Unlikely | Moderate | |
| Functional Balance | ||||||||||||||||
| Overall | 6 | 288 | 48 | 0.409 | 0.044, 0.744 | 0% (0.4781) | Sym. (0.79) | 0.409 | 0% | Medium | No | No | Yes | Unlikely | Moderate | |
| Bipedal Balance on an Unstable Support | ||||||||||||||||
| Eyes condition | EO | 2 | 126 | 63 | 0.371 | −0.122, 0.865 | 0% (0.6748) | - | - | - | Medium | No | No | Yes | Likely | Very low |
| EC | 2 | 126 | 63 | 0.333 | −0.163, 0.828 | 45% (0.1758) | - | - | - | Medium | Medium | No | Yes | Likely | Very low | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del-Moral-García, M.; Obrero-Gaitán, E.; Rodríguez-Almagro, D.; Rodríguez-Huguet, M.; Osuna-Pérez, M.C.; Lomas-Vega, R. Effectiveness of Active Therapy-Based Training to Improve the Balance in Patients with Fibromyalgia: A Systematic Review with Meta-Analysis. J. Clin. Med. 2020, 9, 3771. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113771
Del-Moral-García M, Obrero-Gaitán E, Rodríguez-Almagro D, Rodríguez-Huguet M, Osuna-Pérez MC, Lomas-Vega R. Effectiveness of Active Therapy-Based Training to Improve the Balance in Patients with Fibromyalgia: A Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2020; 9(11):3771. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113771
Chicago/Turabian StyleDel-Moral-García, María, Esteban Obrero-Gaitán, Daniel Rodríguez-Almagro, Manuel Rodríguez-Huguet, María Catalina Osuna-Pérez, and Rafael Lomas-Vega. 2020. "Effectiveness of Active Therapy-Based Training to Improve the Balance in Patients with Fibromyalgia: A Systematic Review with Meta-Analysis" Journal of Clinical Medicine 9, no. 11: 3771. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113771