Effectiveness and Safety of Topical Chlorhexidine and Vitamin E TPGS in the Treatment of Acanthamoeba Keratitis: A Survey on 29 Cases

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Experimental Section
2.1. Materials
2.2. Patients
2.3. Treatment Protocol
2.4. Outcomes
2.5. Statistical Analysis
3. Results
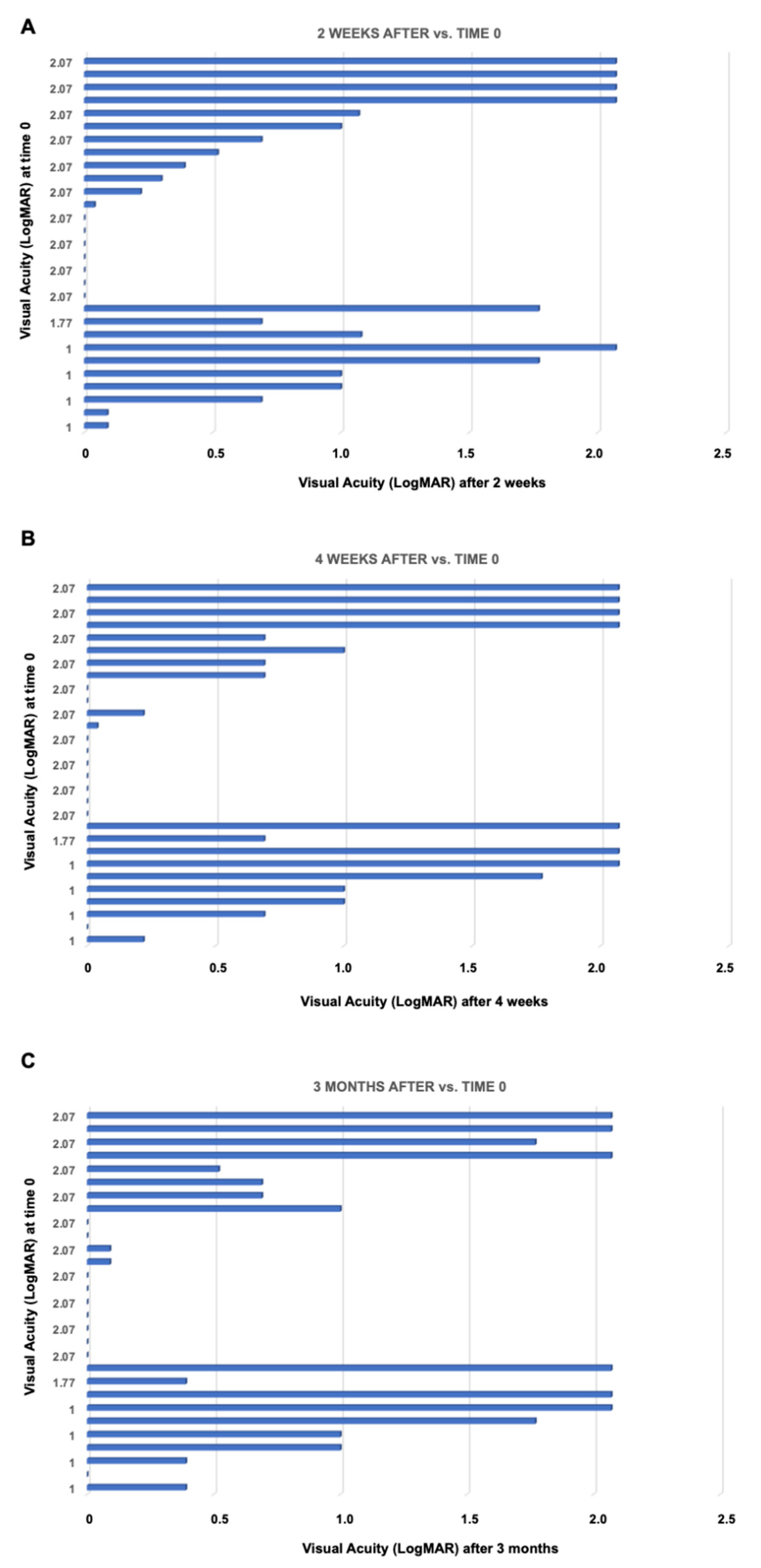
3.1. Visual Performance
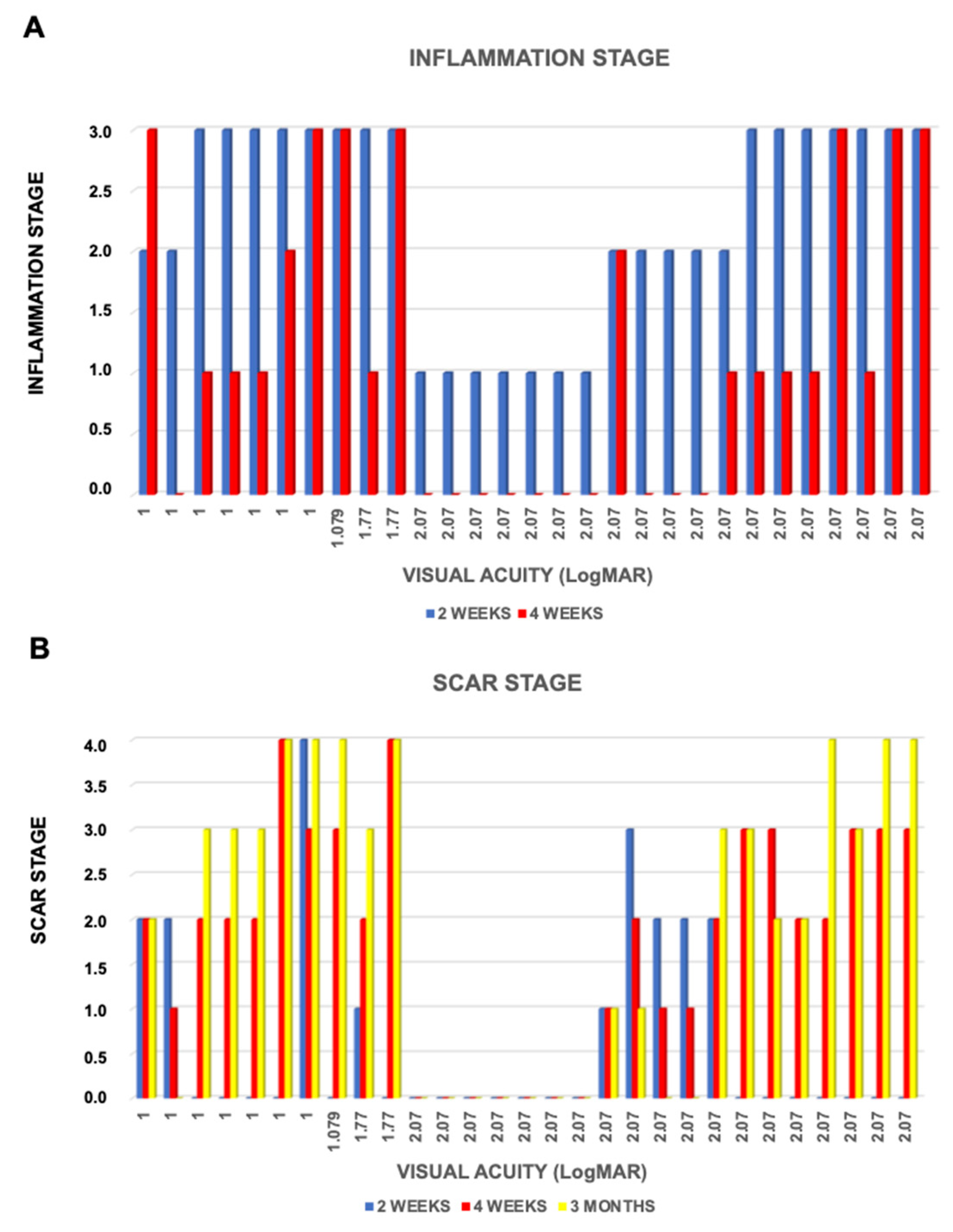
3.2. Inflammation
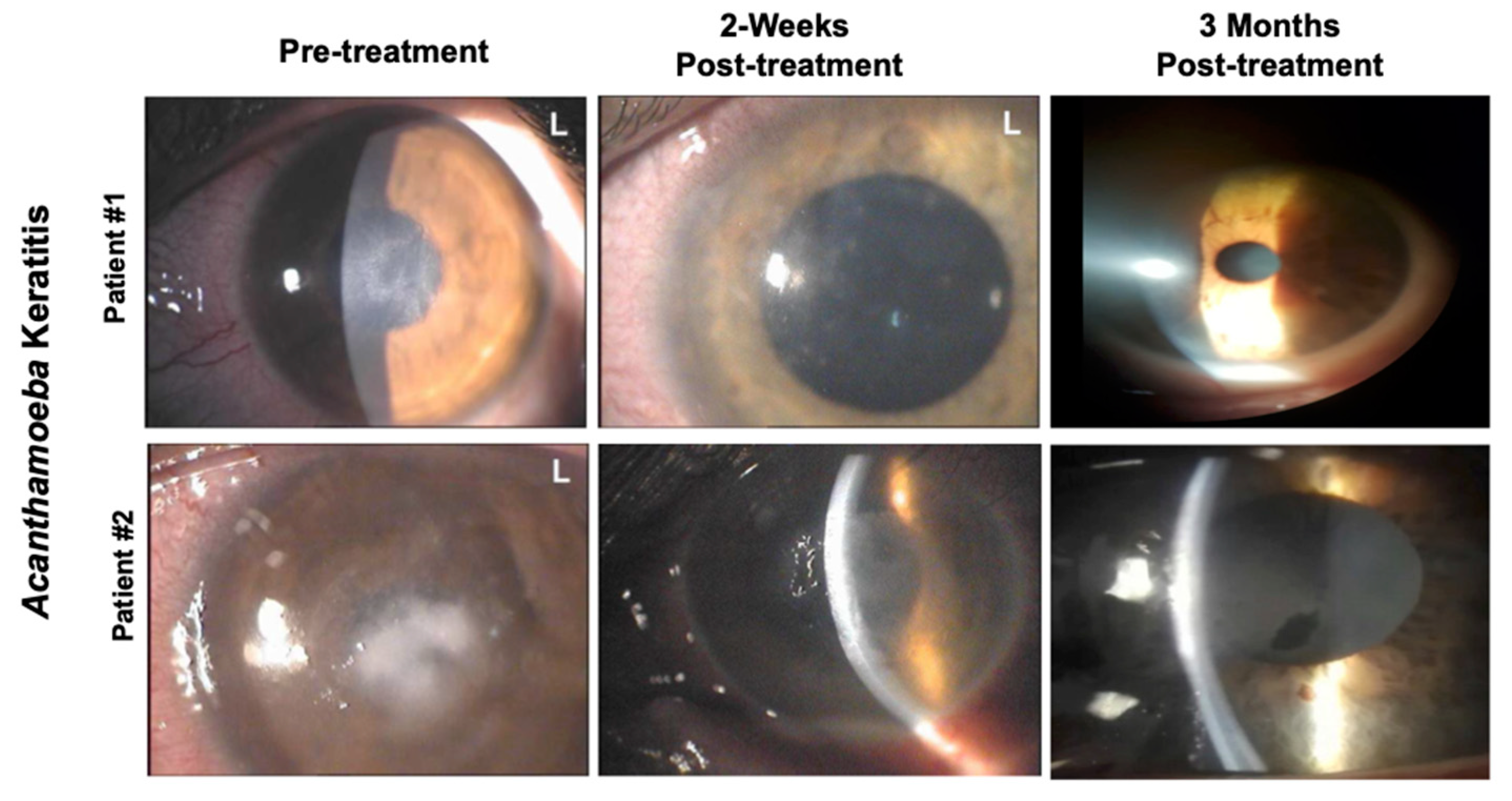
3.3. Corneal Scarring
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Data Availability Statement
References
- Visvesvara, G.S.; Moura, H.; Schuster, F.L. Pathogenic and opportunistic free-living amoebae: Acanthamoeba spp.; Balamuthia mandrillaris, Naegleria fowleri, and Sappinia diploidea. FEMS Immunol. Med. Microbiol. 2007, 50, 1–26. [Google Scholar] [PubMed] [Green Version]
- Lorenzo-Morales, J.; Khan, N.A.; Walochnik, J. An update on Acanthamoeba keratitis: Diagnosis, pathogenesis and treatment. Parasite 2015, 22, 10–15. [Google Scholar] [PubMed] [Green Version]
- Kot, K.; Łanocha-Arendarczyk, N.A.; Kosik-Bogacka, D.I. Amoebas from the genera Acanthamoeba and their pathogenic properties. Ann. Parasitol. 2018, 64, 299–308. [Google Scholar]
- Naginton, J.; Watson, P.G.; Playfair, T.J.; McGill, J.; Jones, B.R.; Steele, A.D. Amoebic infection of the eye. Lancet 1974, 2, 1537–1540. [Google Scholar] [PubMed]
- Stehr-Green, J.K.; Bailey, T.M.; Visvesvara, G.S. The epidemiology of Acanthamoeba keratitis in the United States. Am. J. Ophthalmol. 1989, 107, 331–369. [Google Scholar]
- Seal, D.V. Acanthamoeba keratitis update –incidence, molecular epidemiology and new drugs for treatment. Eye 2003, 17, 893–905. [Google Scholar]
- Bunsuwansakul, C.; Mahboob, T.; Hounkong, K.; Laohaprapanon, S.; Chitapornpan, S.; Jawjit, S.; Yasiri, A.; Barusrux, S.; Bunluepuech, K.; Sawangjaroen, N.; et al. Acanthamoeba in Southeast Asia—Overview and Challenges. Korean J. Parasitol. 2019, 57, 341–357. [Google Scholar]
- Maycock, N.J.; Jayaswal, R. Update on Acanthamoeba Keratitis: Diagnosis, Treatment, and Outcomes. Cornea 2016, 35, 713–720. [Google Scholar]
- Lam, D.S.; Lyon, D.; Poon, A.S.; Rao, S.K.; Fan, D.S. Polyhexamethylene biguanide (0.02%) alone is not adequate for treating chronic Acanthameoba keratitis. Eye 2000, 14, 678–679. [Google Scholar]
- Kitagawa, K.; Nakamura, T.; Takahashi, N.; Oikawa, Y.; Ikeda, T. A novel combination treatment of chlorhexidine gluconate, natamycin (pimaricin) and debridement for a Acanthamoeba keratitis. Jpn. J. Ophthalmol. 2003, 47, 616–617. [Google Scholar]
- Oldenburg, C.E.; Acharya, N.R.; Tu, E.Y.; Zegans, M.E.; Mannis, M.J.; Gaynor, B.D.; Whitcher, J.P.; Lietman, T.M.; Keenan, J.D. Practice patterns and opinions in the treatment of Acanthamoeba keratitis. Cornea 2011, 30, 1363–1368. [Google Scholar] [PubMed] [Green Version]
- Bacon, A.S.; Frazer, D.G.; Dart, J.K.; Matheson, M.; Ficker, L.A.; Wright, P. A review of 72 consecutive cases of Acanthamoeba keratitis, 1984–1992. Eye 1993, 7, 719–725. [Google Scholar] [PubMed]
- Lim, N.; Goh, D.; Bunce, C.; Xing, W.; Fraenkel, G.; Poole, T.R.; Ficker, L. Comparison of polyhexamethylene biguanide and chlorhexidine as monotherapy agents in the treatment of Acanthamoeba keratitis. Am. J. Ophthalmol. 2008, 145, 130–135. [Google Scholar] [PubMed]
- Alkharashi, M.; Lindsley, K.; Law, H.A.; Sikder, S. Medical interventions for acanthamoeba keratitis. Cochrane Database Syst. Rev. 2015, 2015, CD010792. [Google Scholar]
- Ostacolo, C.; Caruso, C.; Tronino, D.; Troisi, S.; Laneri, S.; Pacente, L.; Del Prete, A.; Sacchi, A. Enhancement of corneal permeation of riboflavin-5ʹ- phosphate through vitamin E TPGS: A promising approach in corneal trans-epithelial cross linking treatment. Int. J. Pharm. 2013, 440, 148–153. [Google Scholar] [PubMed]
- Paradiso, P.; Serro, A.P.; Saramago, B.; Colaço, R.; Chauhan, A. Controlled Release of Antibiotics from Vitamin E-Loaded Silicone-Hydrogel Contact Lenses. J. Pharm. Sci. 2016, 105, 1164–1172. [Google Scholar] [PubMed]
- Caruso, C.; Porta, A.; Tosco, A.; Eletto, D.; Pacente, L.; Bartollino, S.; Costagliola, C. A Novel Vitamin E TPGS-Based Formulation Enhances Chlorhexidine Bioavailability in Corneal Layers. Pharmaceutics 2020, 12, 642. [Google Scholar]
- Ren, M.; Wu, X. Evaluation of three different methods to establish animal models of Acanthamoeba keratitis. Yonsei Med. J. 2010, 51, 121–127. [Google Scholar]
- Ibrahim, Y.W.; Boase, D.L.; Cree, I.A. Factors affecting the epidemiology of Acanthamoeba keratitis. Ophthalmic Epidemiol. 2007, 14, 53–60. [Google Scholar]
- Tananuvat, N.; Techajongjintana, N.; Somboon, P.; Wannasan, A. The First Acanthamoeba keratitis Case of Non-Contact Lens Wearer with HIV Infection in Thailand. Korean J. Parasitol. 2019, 57, 505–511. [Google Scholar]
- Tu, E.Y.; Joslin, C.E.; Sugar, J.; Shoff, M.E.; Booton, G.C. Prognostic factors affecting visual outcome in Acanthamoeba keratitis. Ophthalmology 2008, 115, 1998–2003. [Google Scholar] [PubMed] [Green Version]
- Polat, Z.A.; Walochnik, J.; Obwaller, A.; Vural, A.; Dursun, A.; Arici, M.K. Miltefosine and polyhexamethylene biguanide: A new drug combination for the treatment of Acanthamoeba keratitis. Clin. Experimen. Ophthalmol. 2014, 42, 151–158. [Google Scholar]
- Vontobel, S.F.; Abad-Villar, E.M.; Kaufmann, C.; Zinkernagel, A.S.; Hauser, P.C.; Thiel, M.A. Corneal Penetration of Poly-hexamethylene Biguanide and Chlorhexidine Digluconate. J. Clin. Exp. Ophthalmol. 2015, 6, 430–435. [Google Scholar]
- Guo, Y.; Luo, J.; Tan, S.; Otieno, B.O.; Zhang, Z. The applications of Vitamin E TPGS in drug delivery. Eur. J. Pharm. Sci. 2013, 49, 175–186. [Google Scholar] [PubMed]
- Costagliola, C.; Libondi, T.; Menzione, M.; Rinaldi, E.; Auricchio, G. Vitamin E and red blood cell glutathione. Metabolism 1985, 34, 712–714. [Google Scholar] [PubMed]
- Carrijo-Carvalho, L.C.; Sant’ana, V.P.; Foronda, A.S.; de Freitas, D.; de Souza Carvalho, F.R. Therapeutic agents and biocides for ocular infections by free-living amoebae of Acanthamoeba genus. Surv. Ophthalmol. 2017, 62, 203–218. [Google Scholar]
- Illingworth, C.D.; Cook, S.D.; Karabatsas, C.H.; Easty, D.L. Acanthamoeba keratitis: Risk factors and outcome. Br. J. Ophthalmol. 1995, 79, 1078–1082. [Google Scholar]
- Duguid, I.G.; Dart, J.K.; Morlet, N.; Allan, B.D.; Matheson, M.; Ficker, L.; Tuft, S. Outcome of acanthamoeba keratitis treated with polyhexamethyl biguanide and propamidine. Ophthalmology 1997, 104, 1587–1592. [Google Scholar]
- Butler, T.K.; Males, J.J.; Robinson, L.P.; Wechsler, A.W.; Sutton, G.L.; Cheng, J.; Taylor, P.; McClellan, K. Six-year review of Acanthamoeba keratitis in New South Wales, Australia: 1997–2002. Clin. Exp. Ophthalmol. 2005, 33, 41–46. [Google Scholar]
- Seal, D.; Hay, J.; Kirkness, C.; Morrell, A.; Booth, A.; Tullo, A.; Ridgway, A.; Armstrong, M. Successful medical therapy of Acanthamoeba keratitis with topical chlorhexidine and propamidine. Eye 1996, 10, 413–421. [Google Scholar]
- Osato, M.; Robinson, N.; Wilhelmus, K.; Jones, D. Morphogenesis of Acanthamoeba castellanii: Titration of the steroid effect. Investig. Ophthalmol. Vis. Sci. 1986, 27, 37. [Google Scholar]
- Park, D.H.; Palay, D.A.; Daya, S.M.; Stulting, R.D.; Krachmer, J.H.; Holland, E.J. The role of topical corticosteroids in the management of Acanthamoeba keratitis. Cornea 1997, 16, 277–283. [Google Scholar] [PubMed]
- O’Day, D.M.; Head, W.S. Advances in the management of keratomycosis and Acanthamoeba keratitis. Cornea 2000, 19, 681–687. [Google Scholar] [PubMed]
- Dart, J.K.; Saw, V.P.; Kilvington, S. Acanthamoeba keratitis: Diagnosis and treatment update 2009. Am. J. Ophthalmol. 2009, 148, 487–499. [Google Scholar]
- Carnt, N.; Robaei, D.; Watson, S.L.; Minassian, D.C.; Dart, J.K. The Impact of Topical Corticosteroids Used in Conjunction with Antiamoebic Therapy on the Outcome of Acanthamoeba Keratitis. Ophthalmology 2016, 123, 984–990. [Google Scholar] [PubMed]
- Chew, H.F.; Yildiz, E.H.; Hammersmith, K.M.; Eagle, R.C.; Rapuano, C.J., Jr.; Laibson, P.R.; Ayres, B.D.; Jin, Y.P.; Cohen, E.J. Clinical outcomes and prognostic factors associated with Acanthamoeba keratitis. Cornea 2011, 30, 435–441. [Google Scholar]
- Kelley, P.S.; Dossey, A.P.; Patel, D.; Whitson, J.T.; Hogan, R.N.; Cavanagh, H.D. Secondary glaucoma associated with advanced Acanthamoeba keratitis. Eye Contact Lens. 2006, 32, 178–182. [Google Scholar]
- Jeong, H.J.; Lee, S.J.; Kim, J.H.; Xuan, Y.H.; Lee, K.H.; Park, S.K.; Choi, S.H.; Chung, D.I.; Kong, H.H.; Ock, M.S.; et al. Acanthamoeba: Keratopathogenicity of isolates from domestic tap water in Korea. Exp. Parasitol. 2007, 117, 357–367. [Google Scholar]
- Radford, C.F.; Minassian, D.C.; Dart, J.K. Acanthamoeba keratitis in England and Wales: Incidence, outcome, and risk factors. Br. J. Ophthalmol. 2002, 86, 536–542. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| N° | % | Value | Mean ± SD | |
|---|---|---|---|---|
| Total Patients | 29 | 100 | ||
| Female | 20 | 68.96 | ||
| Male | 9 | 31.04 | ||
| Average age (years) | 27.03 | 10.61 | ||
| Contact lens wear | 16 | 55.17 | ||
| Organic material trauma (plant) | 7 | 24.13 | ||
| Dust contamination | 2 | 6.89 | ||
| Water contamination | 1 | 3.44 | ||
| Unknown contamination | 3 | 10.37 | ||
| Already in therapy | 17 | 58.62 | ||
| Ocular pain | 29 | 100 | ||
| Epitheliopathy | 29 | 100 | ||
| Peri-keratic vessels dilatation | 29 | 100 | ||
| Stromal infiltrates | 29 | 100 | ||
| Sub-epithelial infiltrates | 5 | 17.24 | ||
| Satellite stromal infiltrates | 9 | 31.03 | ||
| Ring stromal infiltrates | 8 | 27.58 | ||
| “Round dot in a ring” stromal pattern | 16 | 55.17 | ||
| Uveitis | 11 | 37.93 | ||
| Ipopion | 3 | 10.34 | ||
| Average best corrected visual acuity (LogMAR) | 1.76 | 0.47 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caruso, C.; Eletto, D.; Rinaldi, M.; Pacente, L.; Troisi, S.; Semeraro, F.; dell’Omo, R.; Costagliola, C. Effectiveness and Safety of Topical Chlorhexidine and Vitamin E TPGS in the Treatment of Acanthamoeba Keratitis: A Survey on 29 Cases. J. Clin. Med. 2020, 9, 3775. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113775
Caruso C, Eletto D, Rinaldi M, Pacente L, Troisi S, Semeraro F, dell’Omo R, Costagliola C. Effectiveness and Safety of Topical Chlorhexidine and Vitamin E TPGS in the Treatment of Acanthamoeba Keratitis: A Survey on 29 Cases. Journal of Clinical Medicine. 2020; 9(11):3775. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113775
Chicago/Turabian StyleCaruso, Ciro, Daniela Eletto, Michele Rinaldi, Luigi Pacente, Salvatore Troisi, Francesco Semeraro, Roberto dell’Omo, and Ciro Costagliola. 2020. "Effectiveness and Safety of Topical Chlorhexidine and Vitamin E TPGS in the Treatment of Acanthamoeba Keratitis: A Survey on 29 Cases" Journal of Clinical Medicine 9, no. 11: 3775. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9113775