Radiological Assessment and Outcome of Local Disease Progression after Neoadjuvant Chemotherapy in Children and Adolescents with Localized Osteosarcoma

Abstract
:1. Introduction
2. Experimental Section
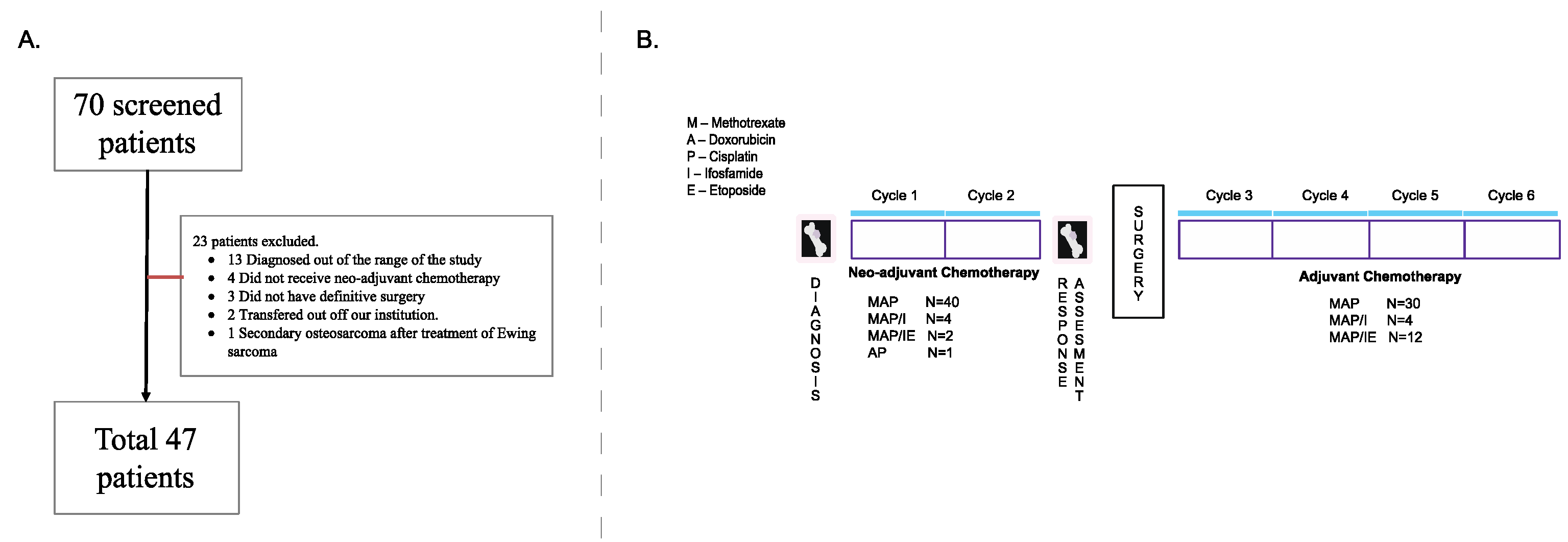
2.1. Patient Selection
2.2. Radiological Review
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Radiologist Agreement
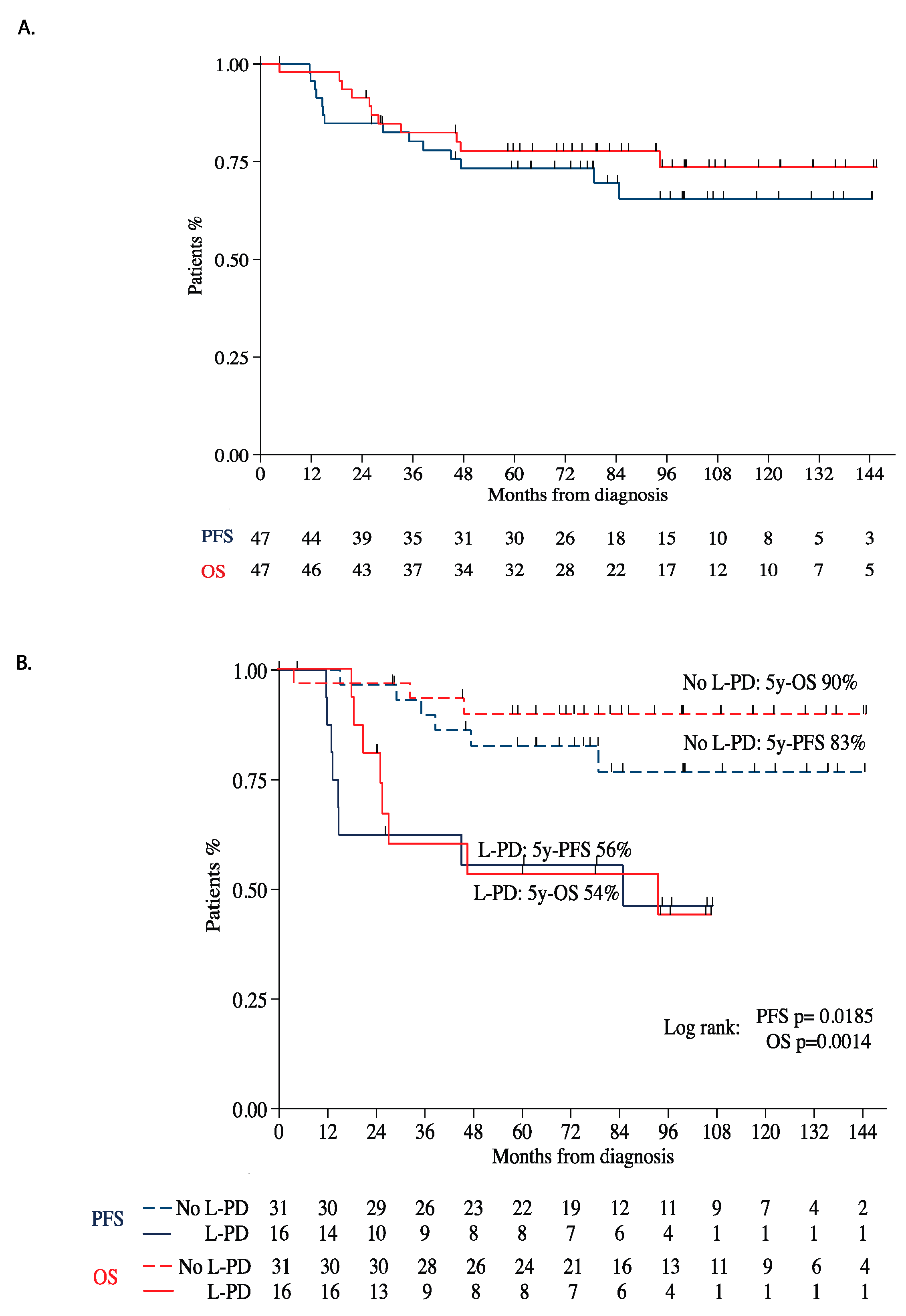
3.3. Outcome after L-PD
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mirabello, L.; Troisi, R.J.; Savage, S.A. Osteosarcoma incidence and survival rates from 1973 to 2004: Data from the Surveillance, Epidemiology, and End Results Program. Cancer 2009, 115, 1531–1543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Provisor, A.J.; Ettinger, L.J.; Nachman, J.B.; Krailo, M.D.; Makley, J.T.; Yunis, E.J.; Huvos, A.G.; Betcher, D.L.; Baum, E.S.; Kisker, C.T.; et al. Treatment of nonmetastatic osteosarcoma of the extremity with preoperative and postoperative chemotherapy: A report from the Children’s Cancer Group. J. Clin. Oncol. 1997, 15, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Goorin, A.M.; Schwartzentruber, D.J.; Devidas, M.; Gebhardt, M.C.; Ayala, A.G.; Harris, M.B.; Helman, L.J.; Grier, H.E.; Link, M.P. Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for nonmetastatic osteosarcoma: Pediatric Oncology Group Study POG-8651. J. Clin. Oncol. 2003, 21, 1574–1580. [Google Scholar] [CrossRef] [PubMed]
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.S.; Gorlick, R. Osteosarcoma: Current Treatment and a Collaborative Pathway to Success. J. Clin. Oncol. 2015, 33, 3029–3035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1,702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumors: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Whelan, J.S.; Bielack, S.S.; Marina, N.; Smeland, S.; Jovic, G.; Hook, J.M.; Krailo, M.; Anninga, J.K.; Butterfass-Bahloul, T.; Böhling, T.; et al. EURAMOS-1, an international randomised study for osteosarcoma: Results from pre-randomisation treatment. Ann. Oncol. 2015, 26, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Guenther, L.M.; Rowe, R.G.; Acharya, P.T.; Swenson, D.W.; Meyer, S.C.; Clinton, C.M.; Guo, D.; Sridharan, M.; London, W.B.; Grier, H.E.; et al. Response Evaluation Criteria in Solid Tumors (RECIST) following neoadjuvant chemotherapy in osteosarcoma. Pediatr. Blood Cancer 2018, 65, e26896. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Statistical Methods for Rates and Proportions, 2nd ed.; Wiley: New York, NY, USA, 1981. [Google Scholar]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; Berg, H.V.D.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.H.; Kim, K.W.; Goo, J.M.; Kim, D.-W.; Hahn, S. Observer variability in RECIST-based tumor burden measurements: A meta-analysis. Eur. J. Cancer 2016, 53, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Tan, Y.; Bell, D.J.; Marley, S.E.; Guo, P.; Mann, H.; Scott, M.; Schwartz, L.H.; Ghiorghiu, D.C. Exploring intra- and inter-reader variability in uni-dimensional, bi-dimensional, and volumetric measurements of solid tumors on CT scans reconstructed at different slice intervals. Eur. J. Radiol. 2013, 82, 959–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorlick, R.; Khanna, C. Osteosarcoma. J. Bone Miner Res. 2010, 25, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Gorlick, R.T.J.; Marina, N. Bone Tumors, 6th ed.; BC Decker: Hamilton, ON, Canada, 2003; pp. 2383–2406. [Google Scholar]
- Jones, K.B.; Ferguson, P.C.; Lam, B.; Biau, D.J.; Hopyan, S.; Deheshi, B.; Griffin, A.M.; White, L.; Wunder, J.S. Effects of neoadjuvant chemotherapy on image-directed planning of surgical resection for distal femoral osteosarcoma. J. Bone Jt. Surg. Am. 2012, 94, 1399–1405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bacci, G.; Mercuri, M.; Longhi, A.; Ferrari, S.; Bertoni, F.; Versari, M.; Picci, P. Grade of chemotherapy-induced necrosis as a predictor of local and systemic control in 881 patients with non-metastatic osteosarcoma of the extremities treated with neoadjuvant chemotherapy in a single institution. Eur. J. Cancer 2005, 41, 2079–2085. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.; Wilhelm, M.; Conyers, R.; Herschtal, A.; Whelan, J.; Bielack, S.; Kager, L.; Kühne, T.; Sydes, M.R.; Gelderblom, H.; et al. Benefits and adverse events in younger versus older patients receiving neoadjuvant chemotherapy for osteosarcoma: Findings from a meta-analysis. J. Clin. Oncol. 2013, 31, 2303–2312. [Google Scholar] [CrossRef] [PubMed]
- Oka, K.; Yakushiji, T.; Sato, H.; Hirai, T.; Yamashita, Y.; Mizuta, H. The value of diffusion-weighted imaging for monitoring the chemotherapeutic response of osteosarcoma: A comparison between average apparent diffusion coefficient and minimum apparent diffusion coefficient. Skelet. Radiol 2010, 39, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Drape, J.L. Advances in magnetic resonance imaging of musculoskeletal tumors. Orthop. Traumatol. Surg. Res. 2013, 99, S115–S123. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Patient Demographics | N = 47 | |
| Age | ||
| Median (range) in years | 12.9 (4.8–16.6) | |
| Gender | ||
| Male | 20 (42.5%) | |
| Location | ||
| Lower extremity | 40 (85.1%) | |
| Upper extremity | 5 (10.6%) | |
| Other * | 2 (4.26%) | |
| Treatment Information | Type of surgery | |
| Amputation | 12 (25.5%) | |
| Endoprosthesis | 29 (61.7%) | |
| Rotationplasty | 6 (12.8%) | |
| Pathological Necrosis | ||
| <90% | 22(46.81%) | |
| >90% | 25(53.19%) | |
| Neoadjuvant Chemotherapy | ||
| MAP | 40 (85.1%) | |
| Other (MAP/IE, MAP/I, AP) | 7 (14.9%) | |
| Adjuvant Chemotherapy | N = 46 ** | |
| MAP | 30 (65.2%) | |
| Other | 16 (34.8%) | |
| Chemo Changed postop | 10 (21.7%) |
| RECIST | EURAMOS | ||||||
|---|---|---|---|---|---|---|---|
| R#2 | R#2 | ||||||
| R#1 | No L-PD | L-PD | R#1 | No L-PD | L-PD | ||
| No L-PD | 42 | 1 | No L-PD | 31 | 2 | ||
| L-PD | 0 | 4 | L-PD | 7 | 7 | ||
| Interrater Agreement | Agreement | Kappa | Interrater Agreement | Agreement | Kappa | ||
| 97.9% | 0.87 | 80.9% | 0.48 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonseca, A.; Ryan, A.L.; Gibson, P.; Hendershot, E.; Hopyan, S.; Ranson, M.; Stimec, J.; Gupta, A.A. Radiological Assessment and Outcome of Local Disease Progression after Neoadjuvant Chemotherapy in Children and Adolescents with Localized Osteosarcoma. J. Clin. Med. 2020, 9, 4070. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9124070
Fonseca A, Ryan AL, Gibson P, Hendershot E, Hopyan S, Ranson M, Stimec J, Gupta AA. Radiological Assessment and Outcome of Local Disease Progression after Neoadjuvant Chemotherapy in Children and Adolescents with Localized Osteosarcoma. Journal of Clinical Medicine. 2020; 9(12):4070. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9124070
Chicago/Turabian StyleFonseca, Adriana, Anne L. Ryan, Paul Gibson, Eleanor Hendershot, Sevan Hopyan, Marilyn Ranson, Jennifer Stimec, and Abha A. Gupta. 2020. "Radiological Assessment and Outcome of Local Disease Progression after Neoadjuvant Chemotherapy in Children and Adolescents with Localized Osteosarcoma" Journal of Clinical Medicine 9, no. 12: 4070. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9124070