Effect of a Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease on Postoperative Nausea and Vomiting

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- Reoperation within 24 h
- unconscious patient;
- patients treated with a ventilator after surgery;
- patients with nausea or vomiting before surgery;
- patients with missing data in their medical records; and
- patients with preoperative PPI type changes.
2.2. PONV, PPI, GERD, and Other Variables
2.3. Statistics
3. Results
3.1. Study Population
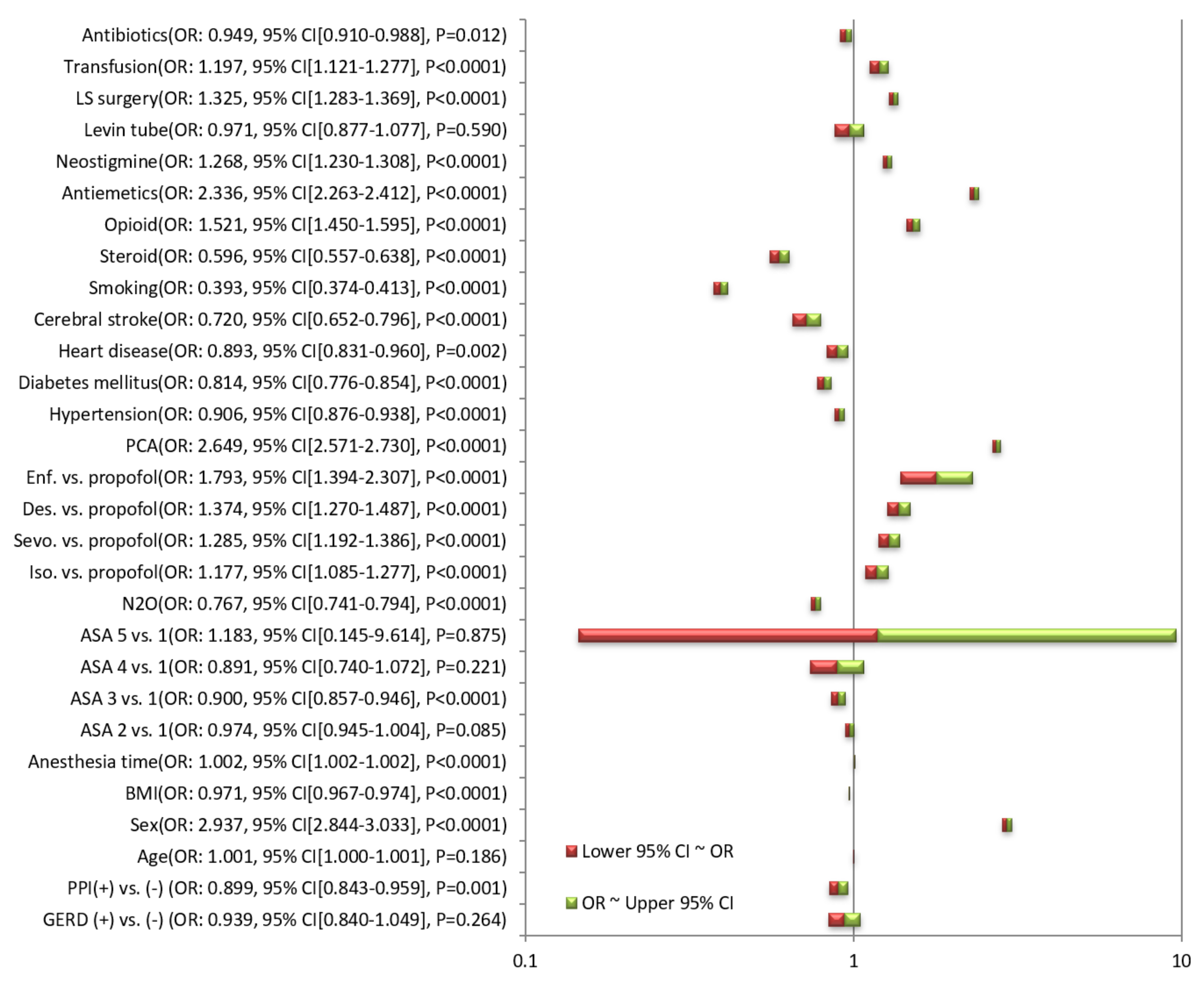
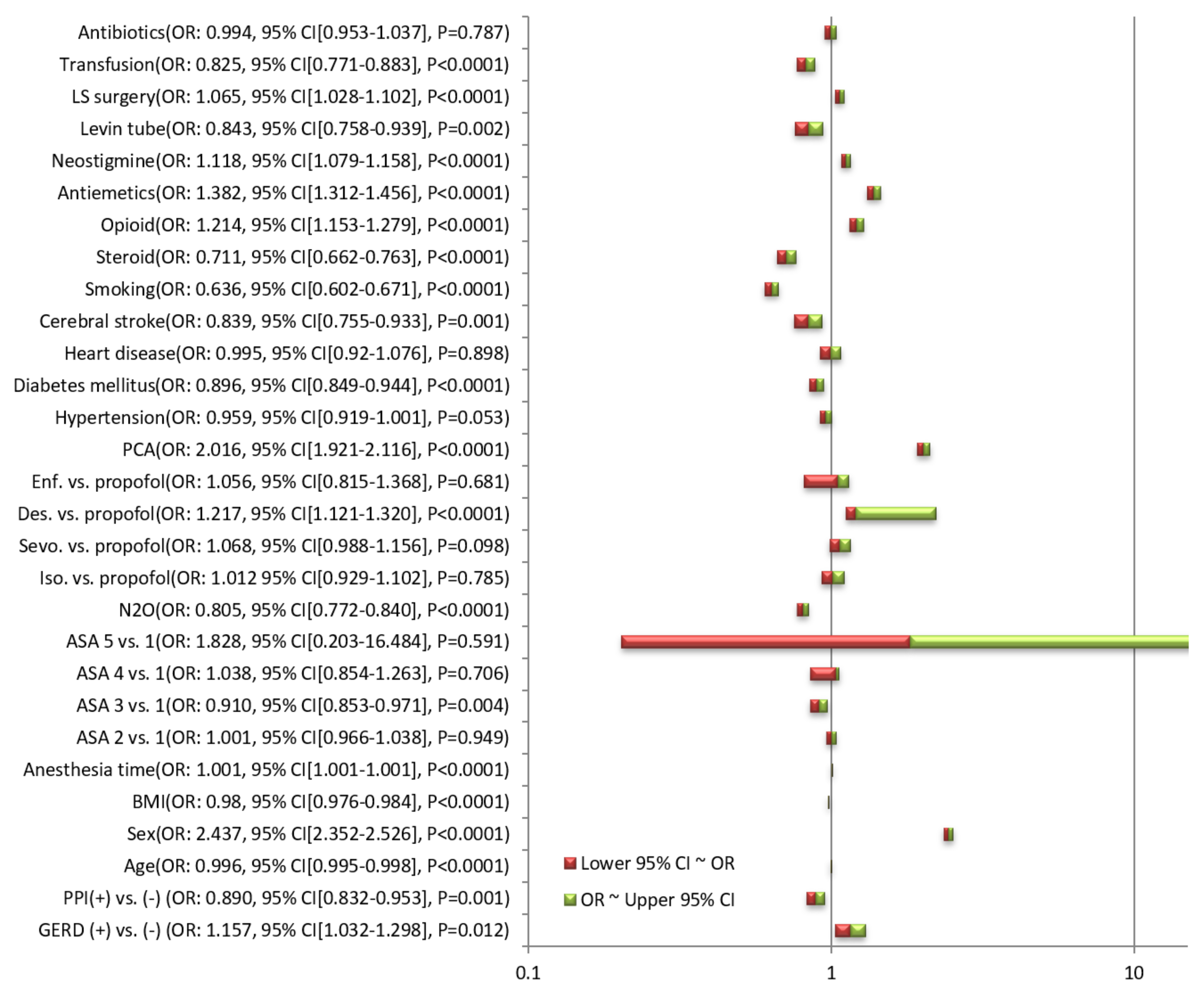
3.2. Odds Ratio for PONV
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Pierre, S.; Whelan, R. Nausea and vomiting after surgery. Contin. Educ. Anaesth. Crit. Care Pain 2012, 13, 28–32. [Google Scholar] [CrossRef] [Green Version]
- Koivuranta, M.; Läärä, E.; Snåre, L.; Alahuhta, S. A survey of postoperative nausea and vomiting. Anaesthesia 1997, 52, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Watcha, M.F.; White, P.F. Postoperative Nausea and Vomiting: Its Etiology, Treatment, and Prevention. Anesthesiol. J. Am. Soc. Anesthesiol. 1992, 77, 162–184. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J. Risk Factors for Postoperative Nausea and Vomiting. Anesth. Analg. 2006, 102, 1884–1898. [Google Scholar] [CrossRef] [PubMed]
- Apfel, C.C.; Stoecklein, K.; Lipfert, P. PONV: A problem of inhalational anaesthesia? Best Pract. Res. Clin. Anaesthesiol. 2005, 19, 485–500. [Google Scholar] [CrossRef]
- Smith, G.; Ng, A. Gastric reflux and pulmonary aspiration in anaesthesia. Minerva Anestesiol. 2003, 69, 402–406. [Google Scholar]
- Stefanidis, D.; Hope, W.W.; Kohn, G.P.; Reardon, P.R.; Richardson, W.S.; Fanelli, R.D.; Committee, S.G. Guidelines for surgical treatment of gastroesophageal reflux disease. Surg. Endosc. 2010, 24, 2647–2669. [Google Scholar] [CrossRef]
- Mythen, M.G. Postoperative gastrointestinal tract dysfunction. Anesth. Analg. 2005, 100, 196–204. [Google Scholar] [CrossRef]
- Foldes, F.F.; Kepes, E.R.; Arthur, G. Severe gastrointestinal distension during nitrous oxide and oxygen anesthesia. JAMA 1965, 194, 1146–1148. [Google Scholar] [CrossRef]
- Shin, J.M.; Sachs, G. Pharmacology of proton pump inhibitors. Curr. Gastroenterol. Rep. 2008, 10, 528–534. [Google Scholar] [CrossRef] [Green Version]
- Farrell, B.; Pottie, K.; Thompson, W.; Boghossian, T.; Pizzola, L.; Rashid, F.J.; Rojas-Fernandez, C.; Walsh, K.; Welch, V.; Moayyedi, P. Deprescribing proton pump inhibitors: evidence-based clinical practice guideline. Can. Fam. Physician 2017, 63, 354–364. [Google Scholar] [PubMed]
- Raeder, J.; Dahl, V.; Bjoernestad, E.; Edlund, G.; Modin, S.; Naucler, E.; Bergheim, R.; Kilhamn, J. Does esomeprazole prevent post-operative nausea and vomiting? Acta Anaesthesiol. Scand. 2007, 51, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Weilbach, C.; Kahler, K.; Thissen, U.; Rahe-Meyer, N.; Piepenbrock, S. Esomeprazole for the prevention of postoperative nausea and vomiting. A randomized, placebo-controlled trial. Eur. J. Anaesthesiol. 2006, 23, 338–340. [Google Scholar] [CrossRef] [PubMed]
- Powell, P.W.W.; Vasudevan, M.; Rall, M.; Carrithers, J.A. Gastroesophageal Reflux Disease as a Predictor for Post Operative Nausea and Vomiting. In Proceedings of the 2010 Annual Meeting of the American Society of Anesthesiologists, San Diego, CA, USA, 16–20 October 2010; p. A213. [Google Scholar]
- Sachs, G.; Shin, J.M.; Howden, C.W. Review article: the clinical pharmacology of proton pump inhibitors. Aliment. Pharmacol. Ther. 2006, 23, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Fellenius, E.; Berglindh, T.; Sachs, G.; Olbe, L.; Elander, B.; Sjostrand, S.E.; Wallmark, B. Substituted benzimidazoles inhibit gastric acid secretion by blocking (H+ + K+)ATPase. Nature 1981, 290, 159–161. [Google Scholar] [CrossRef] [PubMed]
- Miner, P.; Katz, P.O.; Chen, Y.; Sostek, M. Gastric acid control with esomeprazole, lansoprazole, omeprazole, pantoprazole, and rabeprazole: A five-way crossover study. Am. J. Gastroenterol. 2003, 98, 2616–2620. [Google Scholar] [CrossRef]
- Röhss, K.; Lind, T.; Wilder-Smith, C. Esomeprazole 40 mg provides more effective intragastric acid control than lansoprazole 30 mg, omeprazole 20 mg, pantoprazole 40 mg and rabeprazole 20 mg in patients with gastro-oesophageal reflux symptoms. Eur. J. Clin. Pharmacol. 2004, 60, 531–539. [Google Scholar] [CrossRef]
- Li, X.-Q.; Andersson, T.B.; Ahlström, M.; Weidolf, L. Comparison of inhibitory effects of the proton pump-inhibiting drugs omeprazole, esomeprazole, lansoprazole, pantoprazole, and rabeprazole on human cytochrome P450 activities. Drug Metab. Dispos. 2004, 32, 821–827. [Google Scholar] [CrossRef]
- Olkkola, K.T.; Ahonen, J. Midazolam and other Benzodiazepines. In Modern Anesthetics; Schüttler, J., Schwilden, H., Eds.; Springer: Berlin/Heidelberg, Germany, 2008; pp. 335–360. [Google Scholar]
- Seo, K.A.; Lee, S.J.; Kim, K.B.; Bae, S.K.; Liu, K.H.; Kim, D.H.; Shin, J.G. Ilaprazole, a new proton pump inhibitor, is primarily metabolized to ilaprazole sulfone by CYP3A4 and 3A5. Xenobiotica Fate Foreign Compd. Biol. Syst. 2012, 42, 278–284. [Google Scholar] [CrossRef]
- Kahrilas, P.J.; Shaheen, N.J.; Vaezi, M.F. American Gastroenterological Association Institute Technical Review on the Management of Gastroesophageal Reflux Disease. Gastroenterology 2008, 135, 1392–1413. [Google Scholar] [CrossRef]
- Koek, G.; Tack, J.; Sifrim, D.; Lerut, T.; Janssens, J. The role of acid and duodenal gastroesophageal reflux in symptomatic GERD. Am. J. Gastroenterol. 2001, 96, 2033–2040. [Google Scholar] [CrossRef] [PubMed]
- Brzana, R.J.; Koch, K.L. Gastroesophageal reflux disease presenting with intractable nausea. Ann. Intern. Med. 1997, 126, 704–707. [Google Scholar] [CrossRef]
- Gill, S.K.; Maltepe, C.; Koren, G. The effect of heartburn and acid reflux on the severity of nausea and vomiting of pregnancy. Can. J. Gastroenterol. Hepatol. 2009, 23, 270–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cotton, B.; Smith, G. The lower oesophageal sphincter and anaesthesia. Br. J. Anaesth. 1984, 56, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Lind, J.; Crispin, J.; McIver, D. The effect of atropine on the gastroesophageal sphincter. Can. J. Physiol. Pharmacol. 1968, 46, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Moses, L.E. Measuring effects without randomized trials? Options, problems, challenges. Med. Care 1995, 33, As8–As14. [Google Scholar]
- Pocock, S.J.; Elbourne, D.R. Randomized trials or observational tribulations? Mass Med. Soc. 2000, 342, 1907–1909. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Concato, J.; Shah, N.; Horwitz, R.I. Randomized, controlled trials, observational studies, and the hierarchy of research designs. N. Engl. J. Med. 2000, 342, 1887–1892. [Google Scholar] [CrossRef] [Green Version]
- Benson, K.; Hartz, A.J. A comparison of observational studies and randomized, controlled trials. N. Engl. J. Med. 2000, 342, 1878–1886. [Google Scholar] [CrossRef]
- Lauer, M.S. Primary angioplasty—Time is of the essence. JAMA 2000, 283, 2988–2989. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| No-PONV (n = 181,078) | PONV (n = 21,361) | p-Value | ||
|---|---|---|---|---|
| Mean age (y) | 49.2 ± 16.8 | 49.3 ± 16.1 | 0.172 | |
| Women | 90,677 (50.1%) | 15,947 (74.7%) | <0.0001 | |
| Mean BMI | 24.2 ± 3.8 | 23.8 ± 3.7 | <0.0001 | |
| Mean anesthesia time (min) | 136.7 ± 93.0 | 154.9 ± 90.9 | <0.0001 | |
| ASA physical status | 1 | 77,889 (43.0%) | 9408 (44.0%) | 0.001 |
| 2 | 82,280 (45.4%) | 9680 (45.3%) | ||
| 3 | 19,731 (10.9%) | 2146 (10.0%) | ||
| 4 | 1171 (0.6%) | 126 (0.6%) | ||
| 5 | 7 (0.0%) | 1 (0.0%) | ||
| N2O | 46,680 (25.8%) | 4494 (21.0%) | <0.0001 | |
| Anesthetic maintenance agent | Isoflurane | 30,114 (16.6%) | 3281 (15.4%) | <0.0001 |
| Sevoflurane | 102,197 (56.4%) | 12,156 (56.9%) | ||
| Desflurane | 39,766 (22.0%) | 5057 (23.7%) | ||
| Enflurane | 464 (0.3%) | 77 (0.4%) | ||
| Propofol | 8,537 (4.7%) | 790 (3.7%) | ||
| GERD | 3184 (1.8%) | 353 (1.7%) | 0.264 | |
| PPI | 10040 (5.5%) | 1071 (5.0%) | 0.001 | |
| PCA | 78,560 (43.4%) | 14,311(67.0%) | <0.0001 | |
| Hypertension | 43,951 (24.3%) | 4809 (22.5%) | <0.0001 | |
| Diabetes mellitus | 20,659 (11.4%) | 2027 (9.5%) | <0.0001 | |
| Heart disease | 7983 (4.4%) | 845 (4.0%) | 0.002 | |
| Cerebral stroke | 4952 (2.7%) | 424 (2.0%) | <0.0001 | |
| Smoking | 34,950 (19.3%) | 1836 (8.6%) | <0.0001 | |
| Opioid use during surgery | 155,963 (86.1%) | 19,316 (90.4%) | <0.0001 | |
| Steroid | 12,659 (7.0%) | 916 (4.3%) | <0.0001 | |
| Antiemetics | 99,149 (54.8%) | 15,780 (73.9%) | <0.0001 | |
| Neostigmine use | 48,579 (26.8%) | 6780 (31.7%) | <0.0001 | |
| Levin tube | 3638 (2.0%) | 417 (2.0%) | 0.574 | |
| Laparoscopic surgery | 38,401 (21.2%) | 5616 (26.3%) | <0.0001 | |
| Transfusion | 7780 (4.3%) | 1089 (5.1%) | <0.0001 | |
| Antibiotics | 157,137 (86.8%) | 18,405 (86.2%) | 0.012 |
| Odds Ratio (95% CI) | p-Value | ||
|---|---|---|---|
| Adjusted through forward selection of variables | GERD (-) | Reference | |
| GERD (+) | 1.157 (1.031–1.297) | 0.013 | |
| PPI (-) | Reference | ||
| PPI (+) | 0.891 (0.833–0.954) | 0.001 | |
| Adjusted through backward elimination of variables | GERD (-) | Reference | |
| GERD (+) | 1.157 (1.032–1.297) | 0.013 | |
| PPI (-) | Reference | ||
| PPI (+) | 0.890 (0.832–0.953) | 0.001 |
| GERD (−) (n = 198,902) | GERD (+) (n = 3537) | |
|---|---|---|
| Omeprazole | 219 (0.1%) | 26 (0.7%) |
| Pantoprazole | 2873 (1.4%) | 118 (3.3%) |
| Lansoprazole | 4029 (2.0%) | 156 (4.4%) |
| Rabeprazole | 353 (0.2%) | 17 (0.5%) |
| Esomeprazole | 3011 (1.5%) | 156 (4.4%) |
| Ilaprazole | 113 (0.1%) | 4 (0.1%) |
| Dexlansoprazole | 28 (0.0%) | 5 (0.1%) |
| GERD (−) (n = 198,902) | p Value | GERD (+) (n = 3537) | p Value | ||
|---|---|---|---|---|---|
| Unadjusted | No PPI | Reference | Reference | ||
| OR (95% CI) | Omeprazole | 0.664 (0.399–1.104) | 0.114 | <0.0001 | 0.998 |
| Pantoprazole | 0.792 (0.694–0.903) | <0.0001 | 1.137 (0.631–2.048) | 0.669 | |
| Lansoprazole | 0.884 (0.795–0.984) | 0.023 | 1.350 (0.832–2.192) | 0.224 | |
| Rabeprazole | 0.986 (0.701–1.386) | 0.934 | 1.224 (0.279–5.380) | 0.789 | |
| Esomeprazole | 1.033 (0.920–1.159) | 0.585 | 1.198 (0.723–1.986) | 0.484 | |
| Ilaprazole | 0.390 (0.159–0.955) | 0.039 | <0.0001 | 0.999 | |
| Dexlansoprazole | 0.312 (0.042–2.295) | 0.252 | <0.0001 | 0.999 | |
| Fully adjusted | No PPI | Reference | Reference | ||
| OR (95% CI) | Omeprazole | 0.819 (0.488–1.373) | 0.449 | <0.0001 | 0.998 |
| Pantoprazole | 0.856 (0.748–0.980) | 0.025 | 1.020 (0.540–1.928) | 0.951 | |
| Lansoprazole | 0.801 (0.718–0.894) | <0.0001 | 1.019 (0.603–1.722) | 0.945 | |
| Rabeprazole | 0.890 (0.628–1.262) | 0.513 | 0.643 (0.138–3.001) | 0.575 | |
| Esomeprazole | 1.085 (0.963–1.223) | 0.180 | 0.982 (0.565–1.706) | 0.948 | |
| Ilaprazole | 0.391 (0.158–0.966) | 0.042 | <0.0001 | 0.999 | |
| Dexlansoprazole | 0.355 (0.048–2.645) | 0.312 | <0.0001 | 0.999 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, Y.S.; Choi, J.W.; Lee, H.S.; Kim, J.H.; Kim, Y.; Lee, J.J. Effect of a Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease on Postoperative Nausea and Vomiting. J. Clin. Med. 2020, 9, 825. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030825
Kwon YS, Choi JW, Lee HS, Kim JH, Kim Y, Lee JJ. Effect of a Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease on Postoperative Nausea and Vomiting. Journal of Clinical Medicine. 2020; 9(3):825. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030825
Chicago/Turabian StyleKwon, Young Suk, Jun Woo Choi, Ho Seok Lee, Jong Ho Kim, Youngmi Kim, and Jae Jun Lee. 2020. "Effect of a Preoperative Proton Pump Inhibitor and Gastroesophageal Reflux Disease on Postoperative Nausea and Vomiting" Journal of Clinical Medicine 9, no. 3: 825. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9030825