Could Inflammatory Indices and Metabolic Syndrome Predict the Risk of Cancer Development? Analysis from the Bagnacavallo Population Study

 , , , ,
, , , ,
Abstract
:1. Background
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Munn, L.L. Cancer and inflammation. Wiley Interdiscip. Rev. Syst. Biol. Med. 2017, 9, e1370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, S.R.; Cook, E.J.; Goulder, F.; Justin, T.A.; Keeling, N.J. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.C.; Kim, S.H.; Oh, S.Y.; Lee, S.; Lee, J.H.; Choi, J.H.; Park, K.J.; Roh, M.S.; Kim, S.G.; Kim, H.J. Clinical significance of preoperative neutrophil-lymphocyte versus platelet-lymphocyte ratio in patients with operable colorectal cancer. Biomarkers 2012, 17, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Yamanaka, T.; Matsumoto, S.; Teramukai, S.; Ishiwata, R.; Nagai, Y.; Fukushima, M. The baseline ratio of neutrophils to lymphocytes is associated with patients’ prognosis in advanced gastric cancer. Oncology 2007, 73, 215–220. [Google Scholar] [CrossRef]
- Hu, B.; Tang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection of hepatocellular carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [Green Version]
- Casadei Gardini, A.; Scarpi, E.; Faloppi, L.; Scartozzi, M.; Silvestris, N.; Santini, D.; de Stefano, G.; Marisi, G.; Negri, F.V.; Foschi, F.G.; et al. Immune inflammation indicators and implication for immune modulation strategies in advanced hepatocellular carcinoma patients receiving sorafenib. Oncotarget 2016, 7, 67142. [Google Scholar]
- Casadei Gardini, A.; Foschi, F.G.; Conti, F.; Petracci, E.; Vukotic, R.; Marisi, G.; Buonfiglioli, F.; Vitale, G.; Ravaioli, F.; Gitto, S.; et al. Immune inflammation indicators and ALBI score to predict liver cancer in HCV-patients treated with direct-activating antivirals. Dig. Liver Dis. 2019, 51, 681–688. [Google Scholar] [CrossRef] [Green Version]
- Sarraf, K.M.; Belcher, E.; Raevsky, E.; Nicholson, A.G.; Goldstraw, P.; Lim, E. Neutrophil/lymphocyte ratio and its association with survival after complete resection in non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2009, 137, 425–428. [Google Scholar] [CrossRef] [Green Version]
- Asher, V.; Lee, J.; Innamaa, A.; Bali, A. Preoperative platelet lymphocyte ratio as an independent prognostic marker in ovarian cancer. Clin. Transl. Oncol. 2011, 13, 499–503. [Google Scholar] [CrossRef]
- Grandl, G.; Wolfrum, C. Hemostasis, endothelial stress, inflammation, and the metabolic syndrome. Semin. Immunopathol. 2018, 40, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M.; Becker, D.; Clark, L.T.; Cooper, R.S.; Denke, M.A.; Howard, J.; Hunninghake, D.B.; Illimgworth, R.; Luepker, R.V.; Mcbride, P.; et al. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [Green Version]
- Braun, S.; Bitton-Worms, K.; LeRoith, D. The link between the metabolic syndrome and cancer. Int. J. Biol. Sci. 2011, 7, 1003–1015. [Google Scholar] [CrossRef]
- Giovannucci, E. Metabolic syndrome, hyperinsulinemia, and colon cancer: A review. Am. J. Clin. Nutr. 2007, 86, s836–s842. [Google Scholar] [CrossRef] [Green Version]
- Cowey, S.; Hardy, R.W. The metabolic syndrome: A high risk state for cancer? Am. J. Pathol. 2006, 169, 1505–1522. [Google Scholar] [CrossRef]
- Lee, J.S.; Cho, S.I.; Park, H.S. Metabolic syndrome and cancer-related mortality among Korean men and women. Ann. Oncol. 2010, 21, 640–645. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Kantola, T.; Klintrup, K.; Vayrynen, J.P.; Vornanen, J.; Bloigu, R.; Karhu, T.; Herzig, K.H.; Näpänkangas, J.; Mäkela, J.; Karttunen, T.J.; et al. Stage-dependent alterations of the serum cytokine pattern in colorectal carcinoma. Br. J. Cancer 2012, 107, 1729–1736. [Google Scholar] [CrossRef] [Green Version]
- Di Carlo, E.; Forni, G.; Musiani, P. Neutrophils in the antitumoral immune response. Chem. Immunol. Allergy 2003, 83, 182–203. [Google Scholar]
- Foschi, F.G.; Bedogni, G.; Domenicali, M.; Giacomoni, P.; Dell’Aglio, A.C.; Dazzani, F.; Lanzi, A.; Conti, F.; Savini, S.; Saini, G.; et al. Prevalence of and risk factors for fatty liver in the general population of Northen Italy: the Bagnacavallo Study. BMC Gastroenterol. 2018, 18, 177. [Google Scholar] [CrossRef] [Green Version]
- Bedogni, G.; Miglioli, L.; Masutti, F.; Tiribelli, C.; Marchesini, G.; Bellentani, S. Prevalence of and risk factors for nonalcoholic fatty liver disease: The Dionysos nutrition and liver study. Hepatology 2005, 42, 44–52. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1991. [Google Scholar]
- Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults. The Evidence Report; National Institutes of Health Diabetes Research: Bethesda, MD, USA, 1998; Volume 6, pp. 51S–209S.
- Bedogni, G.; Kahn, H.S.; Bellentani, S.; Tiribelli, C. A simple index of lipid overaccumulation is a good marker of liver steatosis. BMC Gastroenterol. 2010, 10, 98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Falcini, F.; Colamartini, A.; Ravaioli, A.; Caprara, L.; Balducci, G.; Vitali, B.; Giorgetti, S.; Rinaldi, E.; Foca, F.; Ravegnani, M.; et al. Cancer Incidence in Romagna, Italy (2008–2012). In Cancer Incidence in Five Continents; Forman, D., Bray, F., Brewster, D.H., Gombe Mbalawa, C., Kohler, B., Piñeros, M., Steliarova-Foucher, E., Swaminathan, R., Ferlay, J., Eds.; Volume X (electronic version); International Agency for Research on Cancer: Lyon, France, 2014; Available online: http://ci5.iarc.fr (accessed on 24 July 2018).
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed] [Green Version]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Balkwill, F.; Charles, K.A.; Mantovani, A. Smoldering and polarized inflammation in the initiation and promotion of malignant disease. Cancer Cell. 2005, 7, 211–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Vijayalekshmi, R.V.; Sung, B. Targeting inflammatory pathways for prevention and therapy of cancer: Short-term friend, long-term foe. Clin. Cancer Res. 2009, 15, 425–430. [Google Scholar] [CrossRef] [Green Version]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Turkson, J.; Jove, R. STAT proteins: Novel molecular targets for cancer drug discovery. Oncogene 2000, 19, 613–6626. [Google Scholar] [CrossRef] [Green Version]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: A decade of experience in patients with cancer. Cancer Treat Rev. 2013, 39, 534–540. [Google Scholar] [CrossRef]
- McCourt, M.; Wang, J.H.; Sookhai, S.; Redmond, H.P. Proinflammatory mediators stimulate neutrophil-directed angiogenesis. Arch Surg. 1999, 134, 1325–1331. [Google Scholar] [CrossRef] [PubMed]
- McCourt, M.; Wang, J.H.; Sookhai, S.; Redmond, H.P. Activated human neutrophils release hepatocyte growth factor/scatter factor. Eur. J. Surg. Oncol. 2001, 27, 396–403. [Google Scholar] [CrossRef]
- Jablonska, E.; Kiluk, M.; Markiewicz, W.; Piotrowski, L.; Grabowska, Z.; Jablonski, J. TNF-alpha, IL-6 and their soluble receptor serum levels and secretion by neutrophils in cancer patients. Arch. Immunol. Ther. Exp. (Warsz.) 2001, 49, 63–69. [Google Scholar]
- Schaider, H.; Oka, M.; Bogenrieder, T.; Nesbit, M.; Satyamoorthy, K.; Berking, C.; Matsushima, K.; Herlyn, M. Differential response of primary and metastatic melanomas to neutrophils attracted by IL-8. Int. J. Cancer 2003, 103, 335–343. [Google Scholar] [CrossRef]
- Shamamian, P.; Schwartz, J.D.; Pocock, B.J.; Monea, S.; Whiting, D.; Marcus, S.G.; Mignatti, P. Activation of progelatinase A (MMP-2) by neutrophil elastase, cathepsin G, and proteinase-3: A role for inflammatory cells in tumor invasion and angiogenesis. J. Cell Physiol. 2001, 189, 197–206. [Google Scholar] [CrossRef]
- Scapini, P.; Nesi, L.; Morini, M.; Tanghetti, E.; Belleri, M.; Noonan, D.; Presta, M.; Albini, A.; Cassatella, M.A. Generation of biologically active angiostatin kringle 1–3 by activated human neutrophils. J. Immunol. 2002, 168, 5798–5804. [Google Scholar] [CrossRef] [Green Version]
- Petrie, H.T.; Klassen, L.W.; Kay, H.D. Inhibition of human cytotoxic T lymphocyte activity in vitro by autologous peripheral blood granulocytes. J. Immunol. 1985, 134, 230–234. [Google Scholar]
- El-Hag, A.; Clark, R.A. Immunosuppression by activated human neutrophils. Dependence on the myeloperoxidase system. J. Immunol. 1987, 139, 2406–2413. [Google Scholar] [PubMed]
- Cristina, F.; Glenn, D. Dual role for immunity in gastrointestinal cancers. J. Clin. Oncol. 2010, 28, 4045–4051. [Google Scholar]
- Templeton, A.J.; McNamara, M.G.; Seruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106, dju124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kao, S.C.; Pavlakis, N.; Harvie, R.; Vardy, J.L.; Boyer, M.J.; van Zandwijk, N.; Clarke, S.J. High blood neutrophil-to-lymphocyte ratio is an indicator of poor prognosis in malignant mesothelioma patients undergoing systemic therapy. Clin. Cancer Res. 2010, 16, 5805–5813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chua, W.; Charles, K.A.; Baracos, V.E.; Clarke, S.J. Neutrophil/lymphocyte ratio predicts chemotherapy outcomes in patients with advanced colorectal cancer. Br. J. Cancer 2011, 104, 1288–1295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, D.D. New links between inflammation and thrombosis. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1321–1324. [Google Scholar] [CrossRef] [PubMed]
- Stone, R.L.; Nick, A.M.; McNeish, I.A.; Balkwill, F.; Han, H.D.; Bottsford-Miller, J.; Rupairmoole, R.; Armaiz-Pena, G.N.; Pecot, C.V.; Coward, J.; et al. Paraneoplastic thrombocytosis in ovarian cancer. N. Engl. J. Med. 2012, 366, 610–618. [Google Scholar] [CrossRef] [Green Version]
- Imai, T.; Koike, K.; Kubo, T.; Kikuchi, T.; Amano, Y.; Takagi, M.; Okumura, N.; Nakahata, T. Interleukin-6 supports human megakaryocytic proliferation and differentiation in vitro. Blood 1991, 78, 1969–1974. [Google Scholar] [CrossRef] [Green Version]
- Lippitz, B.E. Cytokine patterns in patients with cancer: A systematic review. Lancet Oncol. 2013, 14, e218–e228. [Google Scholar] [CrossRef]
- Klinger, M.H.; Jelkmann, W. Role of blood platelets in infection and inflammation. J. Interferon Cytokine Res. 2002, 22, 913–922. [Google Scholar] [CrossRef]
- Labelle, M.; Begum, S.; Hynes, R.O. Platelets guide the formation of early metastatic niches. Proc. Natl. Acad. Sci. USA 2014, 111, E3053–E3061. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.J.; Ace, O.; Mcmanara, M.G.; Al-Mubarak, M.; Vera-Badillo, F.E.; Hermanns, T.; Seruga, B.; Ocana, A.; Tannock, I.F.; Amir, E. Role of Platelet-to-lymphocyte ratio in solid tumors: A systematic review and meta-analysis. Cancer Epidemiol. Biomarkers Prev. 2014, 23, 1204–1212. [Google Scholar] [CrossRef] [Green Version]
- Placke, T.; Salih, H.R.; Kopp, H.G. GITR ligand provided by thrombopoietic cells inhibits NK cell antitumor activity. J. Immunol. 2012, 189, 154–160. [Google Scholar] [CrossRef] [Green Version]
- Labelle, M.; Begum, S.; Hynes, R.O. Direct signaling between platelets and cancer cells induces an epithelial–mesenchymal-like transition and promotes metastasis. Cancer Cell. 2011, 20, 576–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schumacher, D.; Strilic, B.; Sivaraj, K.K.; Wettschureck, N.; Offermanns, S. Platelet-derived nucleotides promote tumor-cell transendothelial migration and metastasis via P2Y2 receptor. Cancer Cell. 2013, 24, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gil-Bernabe, A.M.; Ferjancic, S.; Tlalka, M.; Zhao, L.; Allen, P.D.; Im, J.H.; Watson, K.; Hill, S.A.; Amirkhosravi, A.; Francis, J.L.; et al. Recruitment of monocytes/macrophages by tissue factor-mediated coagulation is essential for metastatic cell survival and premetastatic niche establishment in mice. Blood 2012, 119, 3164–3175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.N.; Goyal, H.; Yu, S.; Luo, H. Prognostic value of systemic immune-inflammation index (SII) in cancers: A systemic review and meta-analysis. J. Lab. Precis. Med. 2018, 3, 29. [Google Scholar] [CrossRef]
- Russo, A.; Autelitano, M.; Bisanti, L. Metabolic syndrome and cancer risk. Eur. J. Cancer 2008, 44, 293–297. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [Green Version]
- Harding, J.; Sooriyakumaran, M.; Anstey, K.J.; Adams, R.; Balkau, B.; Briffa, T.; Davis, T.M.; Davis, W.A.; Dobson, A.; Giles, G.G.; et al. The metabolic syndrome and cancer: Is the metabolic syndrome useful for predicting cancer risk above and beyond its individual components? Diabetes Metab. 2015, 41, 463–469. [Google Scholar] [CrossRef]
- Pothiwala, P.; Jain, S.K.; Yaturu, S. Metabolic syndrome and cancer. Metab. Syndr. Relat. Disord. 2009, 7, 279–288. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| CHARACTERISTICS | PATIENTS, n. (%) |
|---|---|
| Gender | |
| Female | 2008 (52.7) |
| Male | 1802 (47.3) |
| Age, median (range) | 47 (40–55) |
| Education | |
| ≤Middle degree | 1794 (47.1) |
| ≥High degree | 2016 (52.9) |
| Smoke | |
| Never | 1889 (49.6) |
| Smoker/Former smoker | 1910 (50.1) |
| Unknown | 11 (0.3) |
| Physical activity | |
| No activity | 2192 (57.5) |
| Activity | 1617 (42.4) |
| Unknown | 1 (0.1) |
| Waist circumference cm, median (range) | 100 (93–107) |
| Triglycerides mg/dL, median (range) | 96 (68–140) |
| HDL mg/dL, median (range) | 61 (50–72) |
| Diastolic blood pressure (mmHg) median (range) | 70 (70–90) |
| Systolic blood pressure (mmHg) median (range) | 100 (90–130) |
| Glucose mg/dL, median (range) | 89 (83–96) |
| NLR, median (range) | 1.46 (1.14–1.87) |
| PLR, median (range) | 101 (82–125) |
| SII, median (range) | 345,662 (258,573–465,454) |
| n. | n. Cancer | 1-CFS, % | p-Value | Crude HR | 95% CI | ||
|---|---|---|---|---|---|---|---|
| Diagnosis of MS | |||||||
| No | 3261 | 167 | 5.6 | 1.00 | reference | ||
| Yes | 549 | 36 | 7.8 | 0.155 | 1.30 | 0.91 | 1.86 |
| High Waist circumference | |||||||
| No | 1209 | 56 | 5.0 | 1.00 | reference | ||
| Yes | 2601 | 147 | 6.4 | 0.190 | 1.23 | 0.90 | 1.67 |
| High Triglycerides | |||||||
| No | 2971 | 165 | 6.1 | 1.00 | reference | ||
| Yes | 839 | 38 | 5.3 | 0.254 | 0.81 | 0.57 | 1.16 |
| Low HDL | |||||||
| No | 3364 | 177 | 5.9 | 1.00 | reference | ||
| Yes | 446 | 26 | 6.2 | 0.636 | 1.10 | 0.73 | 1.67 |
| High Blood pressure | |||||||
| No | 3187 | 161 | 5.7 | 1.00 | reference | ||
| Yes | 623 | 42 | 7.1 | 0.085 | 1.35 | 0.96 | 1.89 |
| High Glucose | |||||||
| No | 3174 | 157 | 5.5 | 1.00 | reference | ||
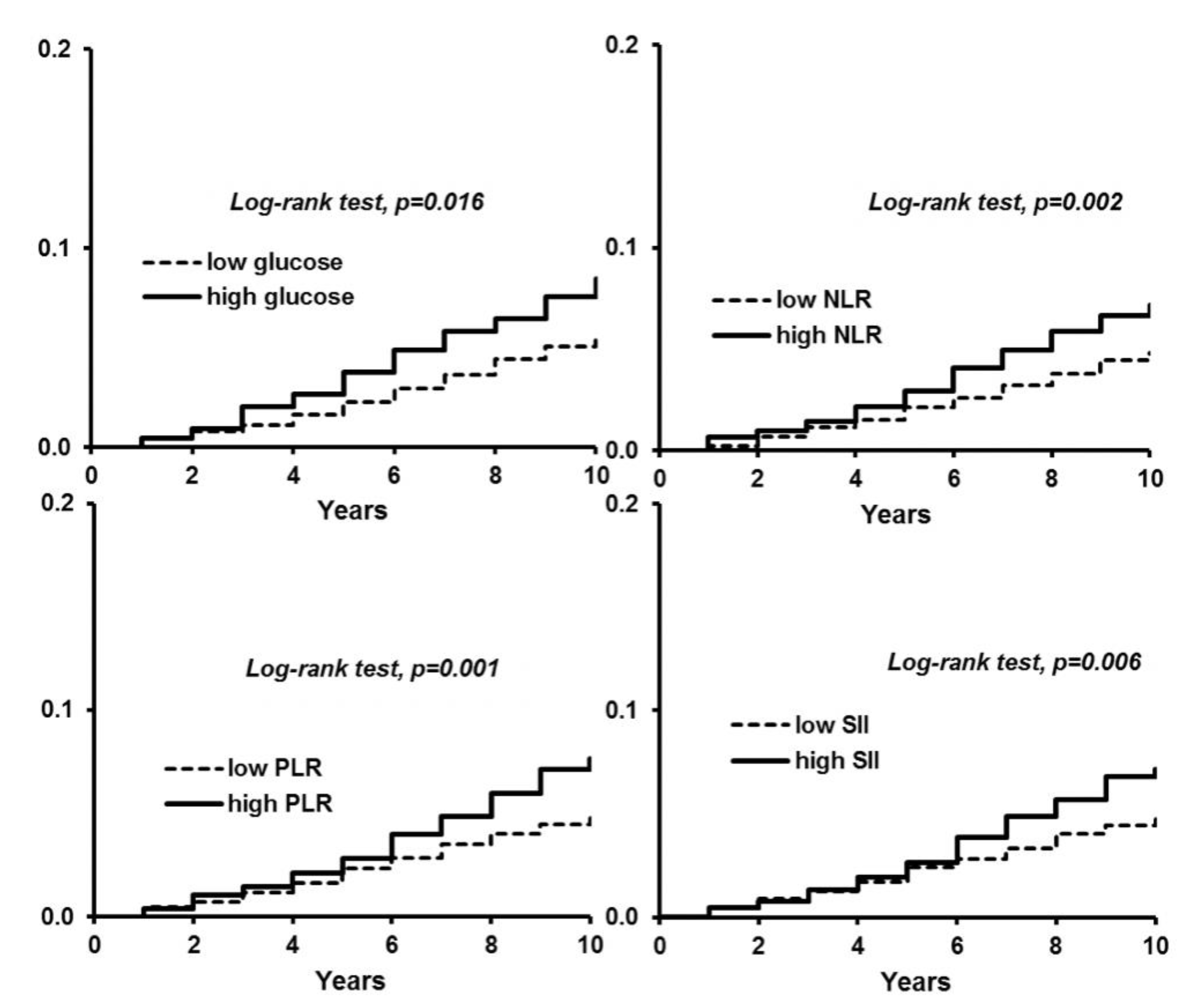
| Yes | 636 | 46 | 8.5 | 0.016 | 1.49 | 1.08 | 2.07 |
| NLR ≥ 1.5 | |||||||
| No | 2006 | 86 | 4.8 | 1.00 | reference | ||
| Yes | 1804 | 117 | 7.2 | 0.002 | 1.54 | 1.16 | 2.03 |
| PLR ≥ 110.6 | |||||||
| No | 2346 | 103 | 4.9 | 1.00 | reference | ||
| Yes | 1464 | 100 | 7.6 | 0.001 | 1.58 | 1.20 | 2.07 |
| SII ≥ 365,776 | |||||||
| No | 2102 | 93 | 4.9 | 1.00 | reference | ||
| Yes | 1708 | 110 | 7.2 | 0.006 | 1.47 | 1.11 | 1.94 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| HR | (95% CI) | HR | 95% CI | |
| Diagnosis of MS | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 1.01 | (0.70–1.45) | 0.98 | (0.68–1.43) |
| High Waist circumference | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 1.06 | (0.77–1.44) | 0.96 | (0.68–1.35) |
| High Triglycerides | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 0.73 | (0.51–1.04) | 0.74 | (0.62–1.07) |
| Low HDL | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 1.07 | (0.71–1.61) | 1.00 | (0.66–1.53) |
| High Blood pressure | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 0.93 | (0.65–1.32) | 0.91 | (0.64–1.30) |
| High Glucose | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 1.16 | (0.83–1.62) | 1.19 | (0.84–1.68) |
| NLR ≥ 1.5 | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 1.52 | (1.15–2.01) | 1.53 | (1.15–2.02) |
| PLR ≥ 110.6 | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 1.59 | (1.21–2.09) | 1.53 | (1.18–2.07) |
| SII ≥ 365,776 | ||||
| No | 1.00 | reference | 1.00 | reference |
| Yes | 1.51 | (1.15–1.99) | 1.47 | (1.11–1.94) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rimini, M.; Casadei-Gardini, A.; Ravaioli, A.; Rovesti, G.; Conti, F.; Borghi, A.; Dall’Aglio, A.C.; Bedogni, G.; Domenicali, M.; Giacomoni, P.; et al. Could Inflammatory Indices and Metabolic Syndrome Predict the Risk of Cancer Development? Analysis from the Bagnacavallo Population Study. J. Clin. Med. 2020, 9, 1177. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041177
Rimini M, Casadei-Gardini A, Ravaioli A, Rovesti G, Conti F, Borghi A, Dall’Aglio AC, Bedogni G, Domenicali M, Giacomoni P, et al. Could Inflammatory Indices and Metabolic Syndrome Predict the Risk of Cancer Development? Analysis from the Bagnacavallo Population Study. Journal of Clinical Medicine. 2020; 9(4):1177. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041177
Chicago/Turabian StyleRimini, Margherita, Andrea Casadei-Gardini, Alessandra Ravaioli, Giulia Rovesti, Fabio Conti, Alberto Borghi, Anna Chiara Dall’Aglio, Giorgio Bedogni, Marco Domenicali, Pierluigi Giacomoni, and et al. 2020. "Could Inflammatory Indices and Metabolic Syndrome Predict the Risk of Cancer Development? Analysis from the Bagnacavallo Population Study" Journal of Clinical Medicine 9, no. 4: 1177. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9041177