Performance Assessment of SARS-CoV-2 PCR Assays Developed by WHO Referral Laboratories

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sensitivity
2.3. Specificity
2.4. SARS-CoV-2 Cell Culture Supernatants
2.5. Extraction and RT-PCR
3. Results
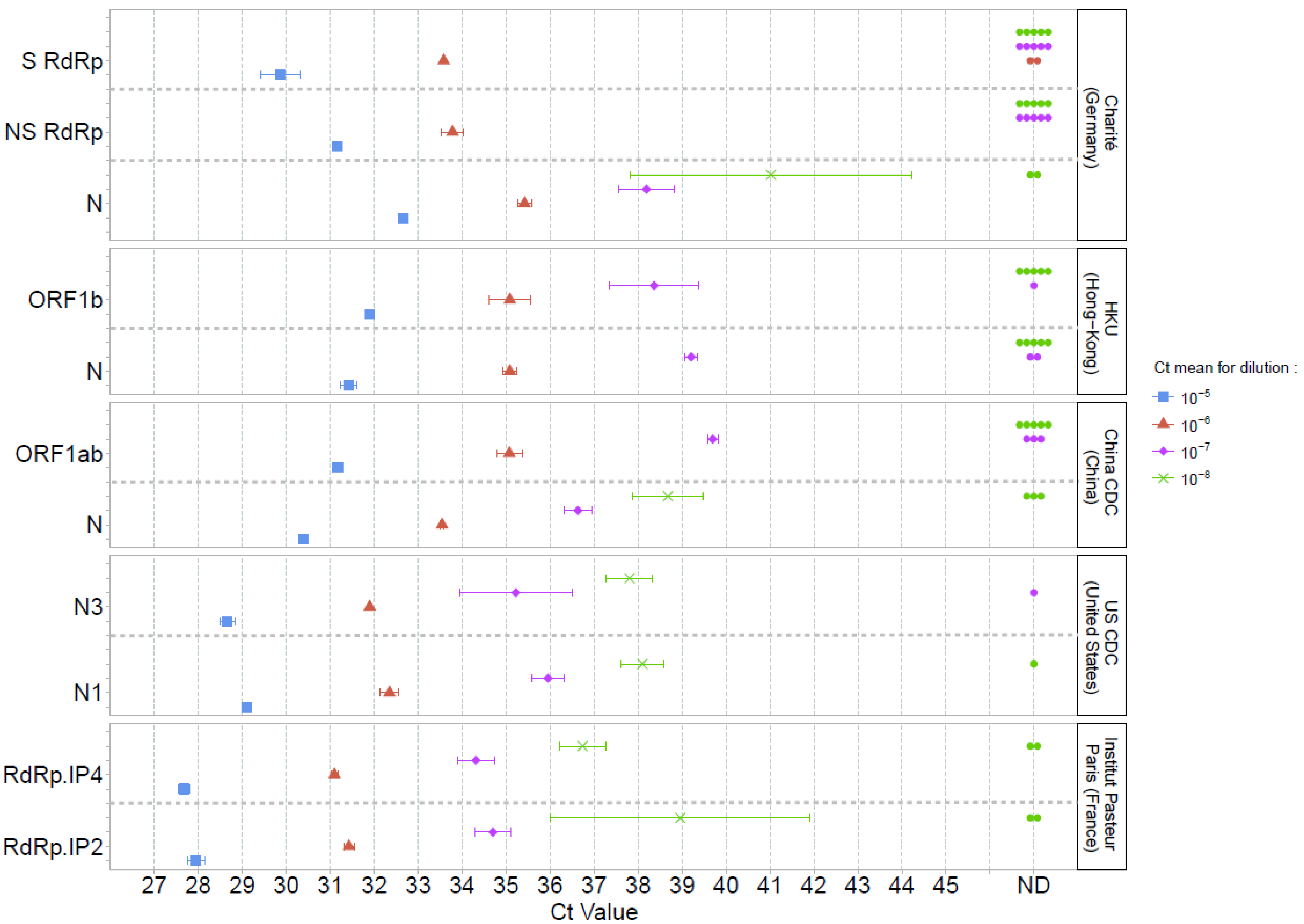
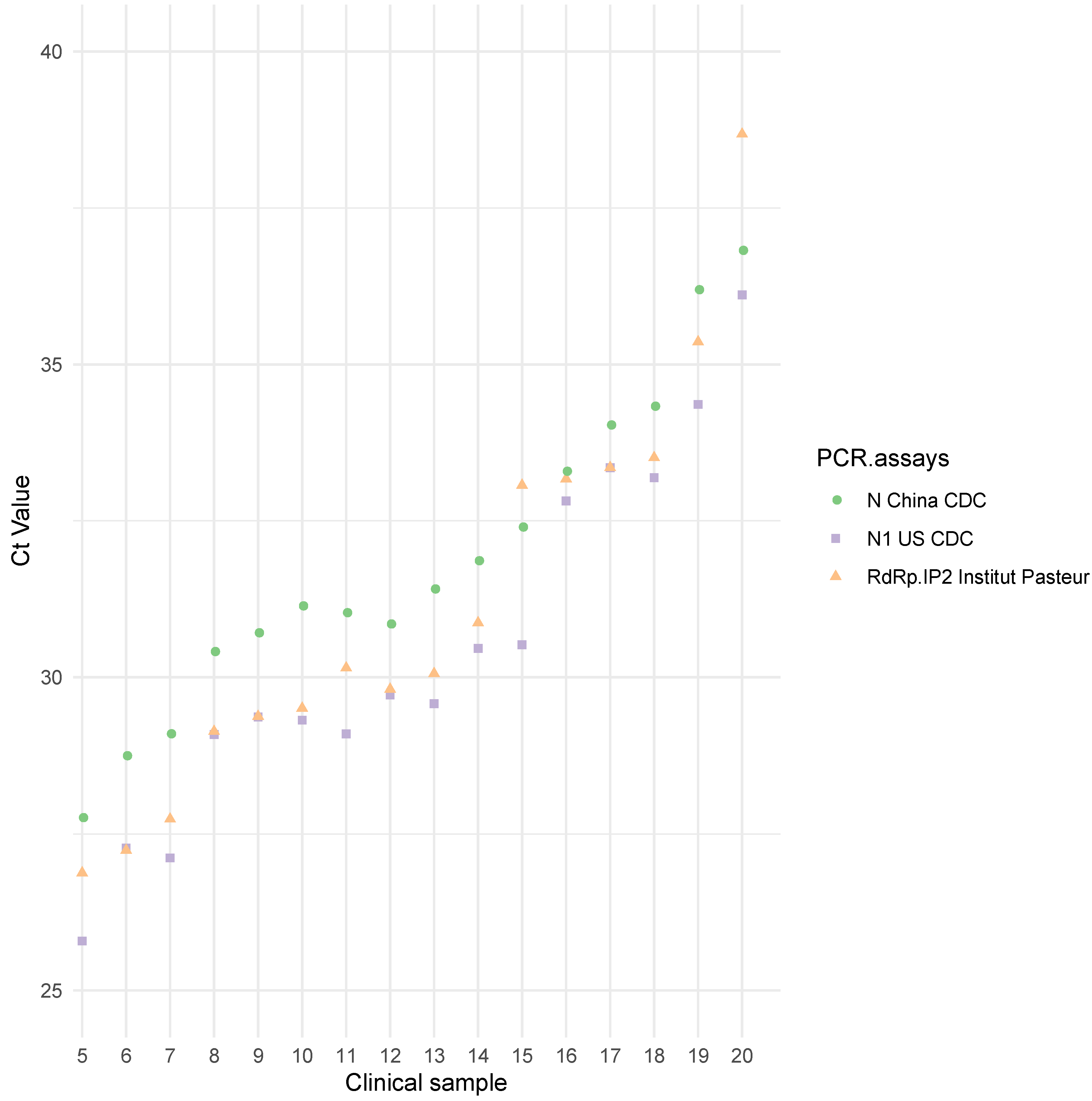
3.1. Sensitivity Comparison of the Five RT-PCR Assays
3.2. Limit of Detection for the Most Sensitive Assays
3.3. Specificity
3.4. Exploration of E Charité and N2 US CDC False-Positive Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses The species Severe acute respiratory syndrome related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [CrossRef] [PubMed] [Green Version]
- World Health Organization WHO Announces COVID-19 Outbreak a Pandemic. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 6 April 2020).
- World Health Organization. Coronavirus Disease 2019 (COVID-19)—Situation Report—127. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200416-sitrep-87-covid-19.pdf?sfvrsn=9523115a_2 (accessed on 26 May 2020).
- Holmes, E.C. Novel 2019 Coronavirus Genome. Available online: http://virological.org/t/novel-2019-coronavirus-genome/319 (accessed on 24 March 2020).
- Corman, V.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L.; et al. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Corman, V.; Bleicker, T.; Brünink, S.; Drosten, C. Diagnostic Detection of 2019-nCoV by Real-Time RT-PCR; Charité Virology, Berlin, Germany. Available online: https://www.who.int/docs/default-source/coronaviruse/protocol-v2-1.pdf?sfvrsn=a9ef618c_2 (accessed on 24 March 2020).
- Cormac, S. Coronavirus and the Race to Distribute Reliable Diagnostics. Available online: https://0-www-nature-com.brum.beds.ac.uk/articles/d41587-020-00002-2 (accessed on 24 March 2020).
- Reusken, C.; Broberg, E.; Haagmans, B.; Meijer, A.; Corman, V.; Papa, A.; Charrel, R.; Drosten, C.; Koopmans, M.; Leitmeyer, K.; et al. Laboratory readiness and response for novel coronavirus (2019-nCoV) in expert laboratories in 30 EU/EEA countries, January 2020. Eurosurveillance 2020, 25, 2000082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Coronavirus Disease (COVID-19) Technical Guidance: Laboratory Testing for 2019-nCoV in Humans. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/laboratory-guidance (accessed on 30 March 2020).
- Chu, D.; Pan, Y.; Cheng, S.; Hui, K.; Krishnan, P.; Liu, Y.; Ng, D.; Wan, C.; Yang, P.; Wang, Q.; et al. Molecular diagnosis of a novel Coronavirus (2019-nCoV) causing an outbreak of pneumonia. Clin. Chem. 2020, 66, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HKU Med. Detection of 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases by RT-PCR. Available online: https://www.who.int/docs/default-source/coronaviruse/peiris-protocol-16-1-20.pdf?sfvrsn=af1aac73_4 (accessed on 24 March 2020).
- China CDC. China CDC Primers and Probes for Detection 2019-nCoV. Available online: http://ivdc.chinacdc.cn/kyjz/202001/t20200121_211337.html (accessed on 24 March 2020).
- Centers for Disease Control and Prevention. A CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. Available online: https://www.fda.gov/media/134922/download (accessed on 24 March 2020).
- Institut Pasteur, Paris. Protocol: Real-Time RT-PCR Assays for the Detection of SARS-CoV-2. Available online: https://www.who.int/docs/default-source/coronaviruse/real-time-rt-pcr-assays-for-the-detection-of-sars-cov-2-institut-pasteur-paris.pdf?sfvrsn=3662fcb6_2 (accessed on 24 March 2020).
- Barron, A.; Olshevsky, C.; Cohen, M. Characteristics of the BGM line of cells from African green monkey kidney. Brief report. Arch. Gesamte Virusforsch. 1970, 32, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Reed, L.; Muench, H. A Simple Method of Estimating Fifty Per Cent Endpoints. Am. J. Epidemiol. 1938, 27, 493–497. [Google Scholar] [CrossRef]
- Baraduc, M.; Baume, A.; Bouvet, F.; Canis, C.; Cattoen, S.; Charachon, V.; Cocquerelle, R.; Courcol, C.; de Champs, M.; Ferroni, N.; et al. SFM comparaison de methodes. In Comite Qualite (QUAMIC) de la Société Francaise de Microbiologie—Recommandations 2014; Société Francaise de Microbiologie: Paris, France, 2014; p. 146. [Google Scholar]
- Vogels, C.; Brito, A.; Wyllie, A.; Fauver, J.; Ott, I.; Kalinich, C.; Petrone, M.; Landry, M.; Foxman, E.; Grubaugh, N. Analytical sensitivity and efficiency comparisons of SARS-COV-2 qRT-PCR assays (Preprint). Prepr. MedRxiv. Available online: https://www.medrxiv.org/content/10.1101/2020.03.30.20048108v1.full.pdf (accessed on 2 April 2020).
- Mögling, R.; Meijer, A.; Berginc, N.; Bruisten, S.; Charrel, R.; Coutard, B.; Eckerle, I.; Enouf, V.; Hungnes, O.; Korukluoglu, G.; et al. Early release—Delayed laboratory response to COVID-19 caused by molecular diagnostic contamination. Emerg. Infect. Dis. J. CDC. 2020, 26, 1843. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Country (Institute) | Target | Oligonucleotide | Sequence | Amplicon Size a | Polymerase | Thermocycler Used in the Reference Publication | Volume of RNA Extract |
|---|---|---|---|---|---|---|---|
| Charité (Germany) [5,6] | RdRp b | Charité_RdRp_F | GTGARATGGTCATGTGTGGCGG | 100 bp | SuperScript™ III Platinum® One-Step Quantitative RT-PCR System | Light Cycler ® 480II (Roche) or Applied Biosystems ViiA™7 (Therom Fisher) | 5 µL |
| Charité_S_RdRp_P c | FAM-CAGGTGGAACCTCATCAGGAGATGC-BBQ | ||||||
| Charité_NS_RdRp_P d | FAM-CCAGGTGGWACRTCATCMGGTGATGC-BBQ | ||||||
| Charité_RdRp_R | CARATGTTAAASACACTATTAGCATA | ||||||
| E e | Charité_E_F | ACAGGTACGTTAATAGTTAATAGCGT | 113 bp | ||||
| Charité_E_P | FAM-ACACTAGCCATCCTTACTGCGCTTCG-BBQ | ||||||
| Charité_E_R | ATATTGCAGCAGTACGCACACA | ||||||
| N | Charité_N_F | CACATTGGCACCCGCAATC | 128 bp | ||||
| Charité_N_P | FAM-ACTTCCTCAAGGAACAACATTGCCA-BBQ | ||||||
| Charité_N_R | GAGGAACGAGAAGAGGCTTG | ||||||
| HKU (Hong Kong) [10,11] | ORF1b-nsp14 f | HKU_ORF_F | TGGGGYTTTACRGGTAACCT | 132 bp | TaqMan Fast Virus Master mix | Applied Biosystems ViiA™7 (Therom Fisher) | 4 µL |
| HKU_ORF_P | FAM-TAGTTGTGATGCWATCATGACTAG-TAMRA | ||||||
| HKU_ORF_R | AACRCGCTTAACAAAGCACTC | ||||||
| N e | HKU_N_F | TAATCAGACAAGGAACTGATTA | 110 bp | ||||
| HKU_N_P | FAM-GCAAATTGTGCAATTTGCGG-TAMRA | ||||||
| HKU_N_R | CGAAGGTGTGACTTCCATG | ||||||
| China CDC (China) [12] | N | ChinaCDC_N_F | GGGGAACTTCTCCTGCTAGAAT | 99 bp | Unspecified | Unspecified | Unspecified |
| ChinaCDC_N_P | FAM-TTGCTGCTGCTTGACAGATT-TAMRA | ||||||
| ChinaCDC_N_R | CAGACATTTTGCTCTCAAGCTG | ||||||
| ORF1ab-nsp10 | ChinaCDC_ORF_F | CCCTGTGGGTTTTACACTTAA | 119 bp | ||||
| ChinaCDC_ORF_P | FAM-CCGTCTGCGGTATGTGGAAAGGTTATGG-BHQ1 | ||||||
| ChinaCDC_ORF_R | ACGATTGTGCATCAGCTGA | ||||||
| US CDC (United States) [13] | N1 c | USCDC_N1_F | GACCCCAAAATCAGCGAAAT | 72 bp | TaqPath™ 1-Step RT-qPCR Master Mix, CG (Thermo Fisher) | Applied Biosystems™ 7500 Fast (Thermo Fisher) | 5 µL |
| USCDC_N1_P | FAM-ACCCCGCATTACGTTTGGTGGACC-BHQ1 | ||||||
| USCDC_N1_R | TCTGGTTACTGCCAGTTGAATCTG | ||||||
| N2 c | USCDC_N2_F | TTACAAACATTGGCCGCAAA | 67 bp | ||||
| USCDC_N2_P | FAM-ACAATTTGCCCCCAGCGCTTCAG-BHQ1 | ||||||
| USCDC_N2_R | GCGCGACATTCCGAAGAA | ||||||
| N3 d | USCDC_N3_F | GGGAGCCTTGAATACACCAAAA | 72 bp | ||||
| USCDC_N3_P | FAM-AYCACATTGGCACCCGCAATCCTG-BHQ1 | ||||||
| USCDC_N3_R | TGTAGCACGATTGCAGCATTG | ||||||
| Institut Pasteur, Paris (France) [14] | RdRp IP2 (Flo2) | Pasteur_IP2_F | ATGAGCTTAGTCCTGTTG | 108 bp | SuperScript™ III Platinum® One-Step Quantitative RT-PCR System | LightCycler ® 480 (Roche) | 5 µL |
| Pasteur_IP2_P | HEX-AGATGTCTTGTGCTGCCGGTA-BHQ1 | ||||||
| Pasteur_IP2_R | CTCCCTTTGTTGTGTTGT | ||||||
| RdRp IP4 (Flo4) | Pasteur_IP4_F | GGTAACTGGTATGATTTCG | 107 bp | ||||
| Pasteur_IP4_P | FAM-TCATACAAACCACGCCAGG-BHQ1 | ||||||
| Pasteur_IP4_R | CTGGTCAAGGTTAATATAGG |
| Institute (Country) | Charité (Germany) [5,6] | HKU (Hong Kong) [10,11] | China CDC (China) [12] | US CDC (United States) [13] | Institut Pasteur, Paris (France) [14] | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amplification Cycles | T °C | Time (min) | Number of Cycles | T °C | Time (min) | Number of Cycles | T°C | Time (min) | Number of Cycles | T °C | Time (min) | Number of Cycles | T °C | Time (min) | Number of Cycles |
| Uracil-N-glycosylase activation | Unspecified | 25 | 02:00 | 1 | |||||||||||
| Reverse transcription | 55 | 10:00 | 1 | 50 | 05:00 | 1 | 50 | 15:00 | 55 | 20:00 | 1 | ||||
| RT inactivation/Enzyme activation | 95 | 03:00 | 95 | 00:20 | 95 | 02:00 | 95 | 03:00 | |||||||
| Denaturation | 95 | 00:15 | 45 | 95 | 00:05 | 40 | 95 | 00:03 | 45 | 95 | 00:15 | 50 | |||
| Annealing/Extending | 58 | 00:30 | 60 | 00:30 | 55 | 00:30 | 58 | 00:30 | |||||||
| Cooling | 40 | 00:30 | 1 | ||||||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Etievant, S.; Bal, A.; Escuret, V.; Brengel-Pesce, K.; Bouscambert, M.; Cheynet, V.; Generenaz, L.; Oriol, G.; Destras, G.; Billaud, G.; et al. Performance Assessment of SARS-CoV-2 PCR Assays Developed by WHO Referral Laboratories. J. Clin. Med. 2020, 9, 1871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061871
Etievant S, Bal A, Escuret V, Brengel-Pesce K, Bouscambert M, Cheynet V, Generenaz L, Oriol G, Destras G, Billaud G, et al. Performance Assessment of SARS-CoV-2 PCR Assays Developed by WHO Referral Laboratories. Journal of Clinical Medicine. 2020; 9(6):1871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061871
Chicago/Turabian StyleEtievant, Sibyle, Antonin Bal, Vanessa Escuret, Karen Brengel-Pesce, Maude Bouscambert, Valérie Cheynet, Laurence Generenaz, Guy Oriol, Gregory Destras, Geneviève Billaud, and et al. 2020. "Performance Assessment of SARS-CoV-2 PCR Assays Developed by WHO Referral Laboratories" Journal of Clinical Medicine 9, no. 6: 1871. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9061871