Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. 99 mTc-Tetrofosmin SPECT-MPI
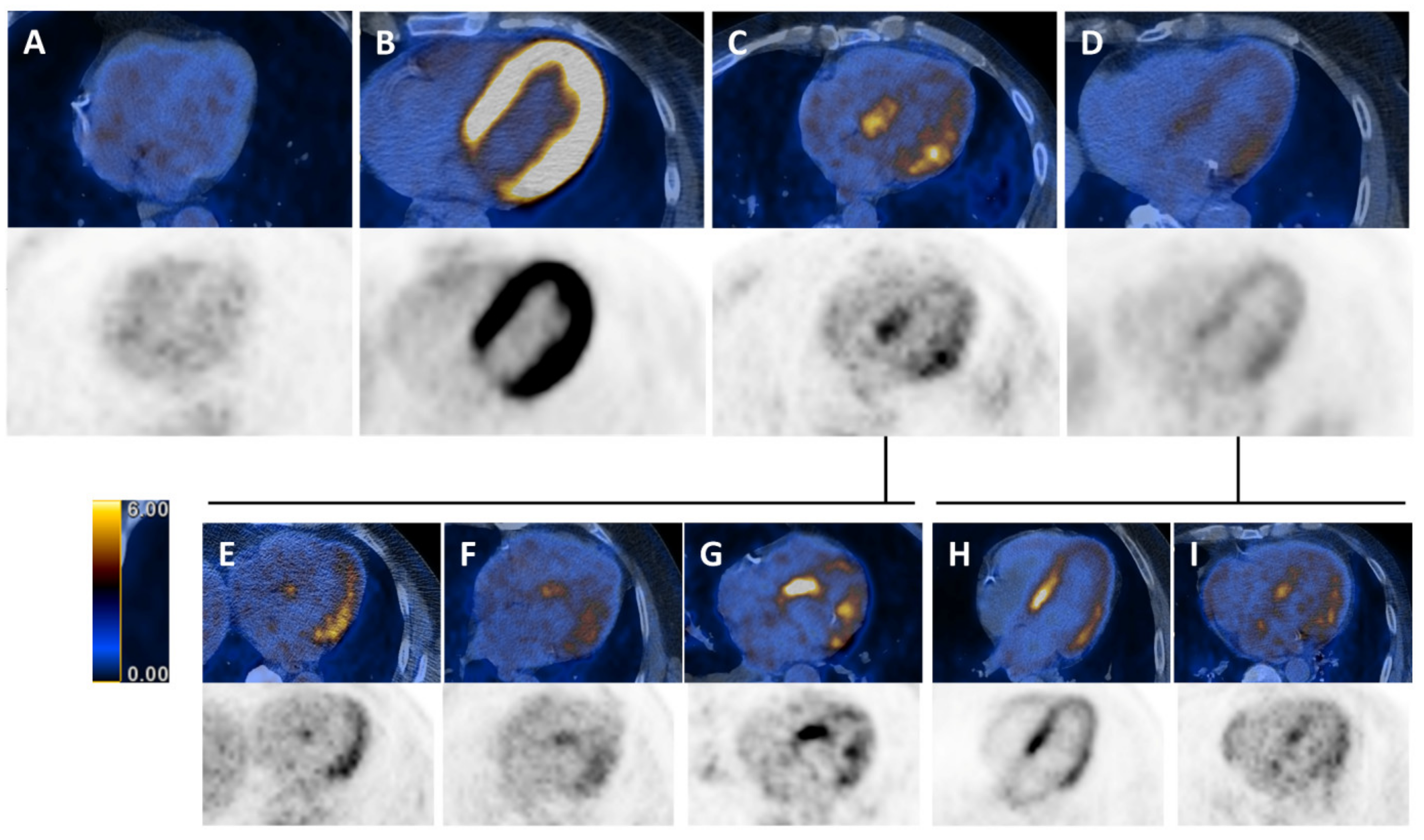
2.3. Whole-Body 18F-FDG PET/CT and Assessment of Myocardial 18F-FDG Uptake
2.4. Statistical Analysis
3. Results
3.1. Study Population
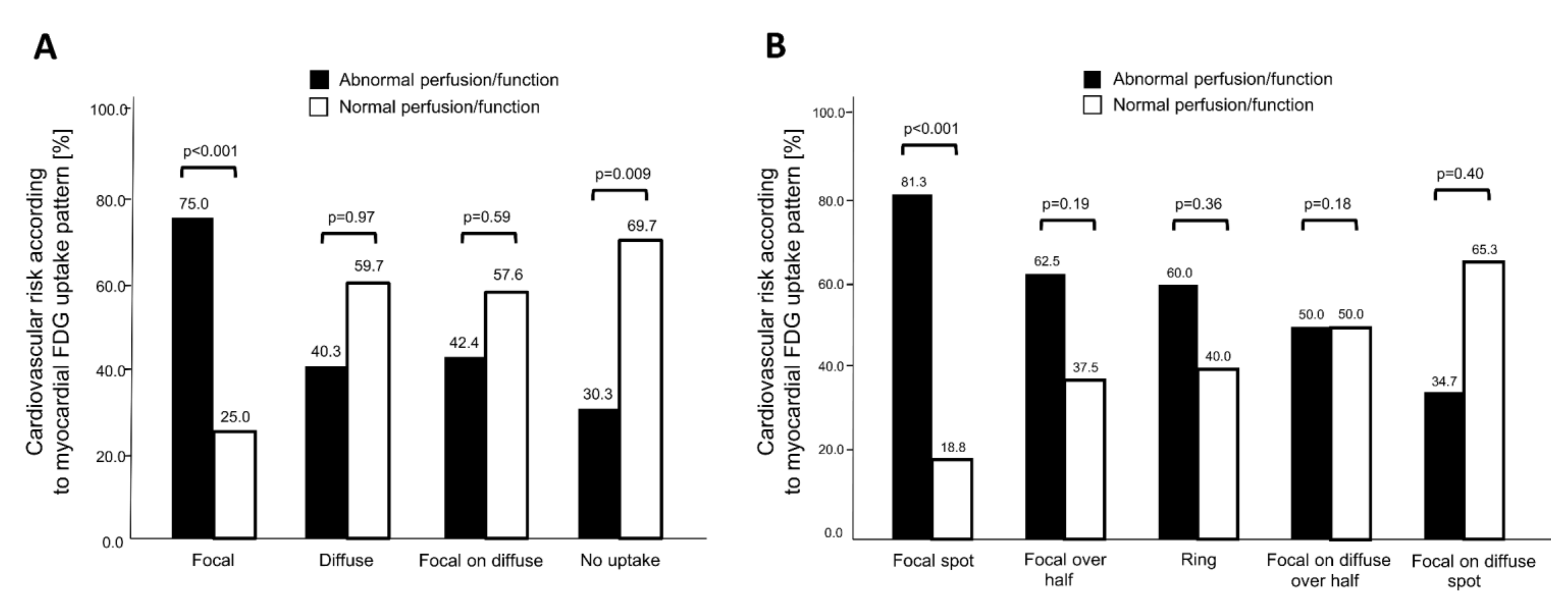
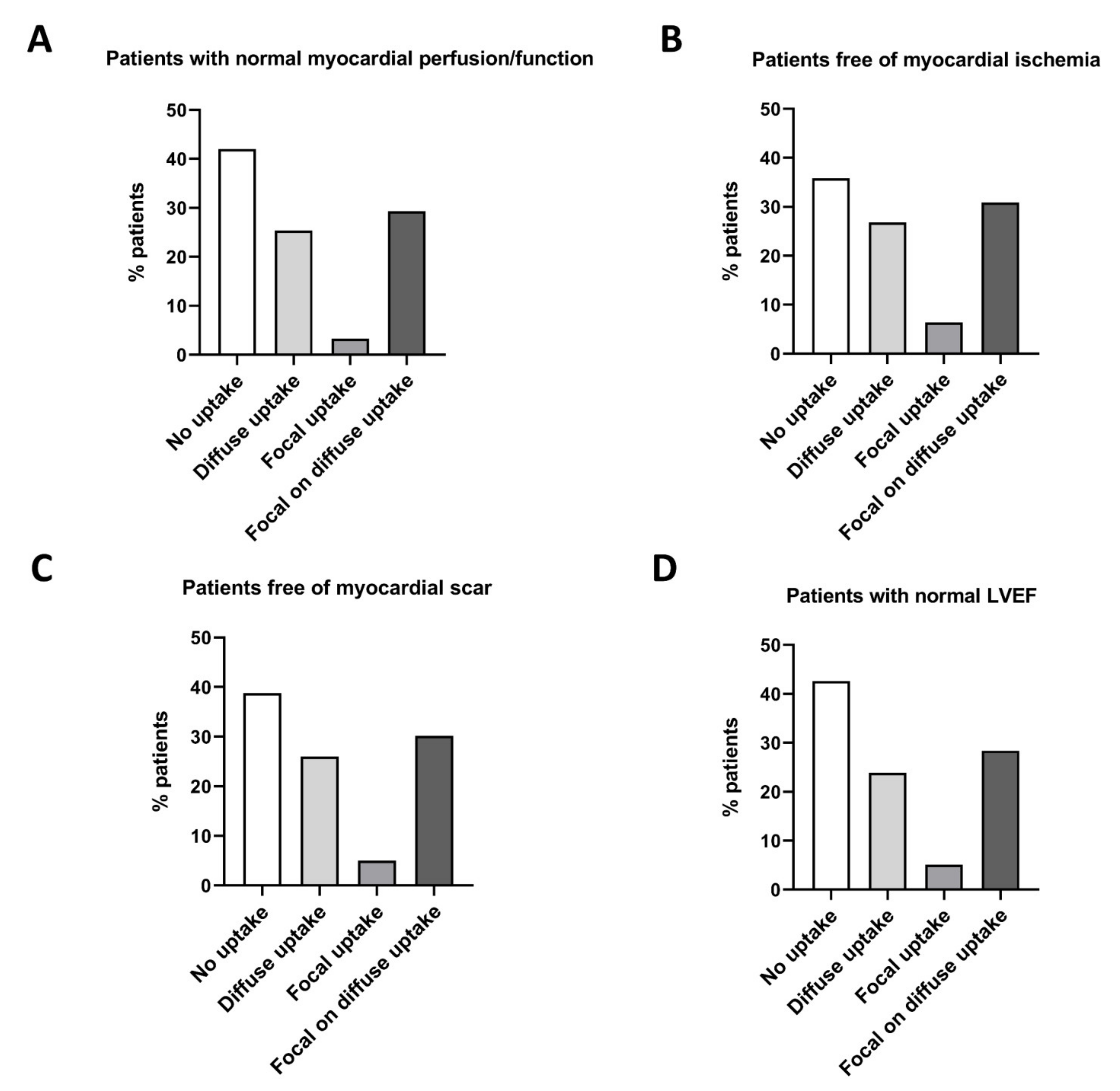
3.2. Association of 18F-FDG Uptake Patterns with Impaired Myocardial Function
3.3. Prognostic Value of Myocardial 18F-FDG Uptake in Patients Undergoing Oncologic PET/CT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Lardinois, D.; Weder, W.; Hany, T.F.; Kamel, E.M.; Korom, S.; Seifert, B.; von Schulthess, G.K.; Steinert, H.C. Staging of non-small-cell lung cancer with integrated positron-emission tomography and computed tomography. N. Engl. J. Med. 2003, 348, 2500–2507. [Google Scholar] [CrossRef] [Green Version]
- Fischer, B.; Lassen, U.; Mortensen, J.; Larsen, S.; Loft, A.; Bertelsen, A.; Ravn, J.; Clementsen, P.; Hogholm, A.; Larsen, K.; et al. Preoperative staging of lung cancer with combined PET-CT. N. Engl. J. Med. 2009, 361, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, P.; Attal, M.; Caillot, D.; Macro, M.; Karlin, L.; Garderet, L.; Facon, T.; Benboubker, L.; Escoffre-Barbe, M.; Stoppa, A.M.; et al. Prospective Evaluation of Magnetic Resonance Imaging and [(18)F]Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography at Diagnosis and Before Maintenance Therapy in Symptomatic Patients With Multiple Myeloma Included in the IFM/DFCI 2009 Trial: Results of the IMAJEM Study. J. Clin. Oncol. 2017, 35, 2911–2918. [Google Scholar] [CrossRef] [PubMed]
- Lordick, F.; Ott, K.; Krause, B.J.; Weber, W.A.; Becker, K.; Stein, H.J.; Lorenzen, S.; Schuster, T.; Wieder, H.; Herrmann, K.; et al. PET to assess early metabolic response and to guide treatment of adenocarcinoma of the oesophagogastric junction: The MUNICON phase II trial. Lancet Oncol. 2007, 8, 797–805. [Google Scholar] [CrossRef]
- Fuchs, M.; Goergen, H.; Kobe, C.; Kuhnert, G.; Lohri, A.; Greil, R.; Sasse, S.; Topp, M.S.; Schafer, E.; Hertenstein, B.; et al. Positron Emission Tomography-Guided Treatment in Early-Stage Favorable Hodgkin Lymphoma: Final Results of the International, Randomized Phase III HD16 Trial by the German Hodgkin Study Group. J. Clin. Oncol. 2019, 37, 2835–2845. [Google Scholar] [CrossRef]
- Jaarsma, C.; Leiner, T.; Bekkers, S.C.; Crijns, H.J.; Wildberger, J.E.; Nagel, E.; Nelemans, P.J.; Schalla, S. Diagnostic performance of noninvasive myocardial perfusion imaging using single-photon emission computed tomography, cardiac magnetic resonance, and positron emission tomography imaging for the detection of obstructive coronary artery disease: A meta-analysis. J. Am. Coll. Cardiol. 2012, 59, 1719–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebhard, C.E.; Maredziak, M.; Portmann, A.; Bengs, S.; Haider, A.; Fiechter, M.; Herzog, B.A.; Messerli, M.; Treyer, V.; Kudura, K.; et al. Heart rate reserve is a long-term risk predictor in women undergoing myocardial perfusion imaging. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2032–2041. [Google Scholar] [CrossRef]
- Haider, A.; Bengs, S.; Maredziak, M.; Messerli, M.; Fiechter, M.; Giannopoulos, A.A.; Treyer, V.; Schwyzer, M.; Kamani, C.H.; Patriki, D.; et al. Heart rate reserve during pharmacological stress is a significant negative predictor of impaired coronary flow reserve in women. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1257–1267. [Google Scholar] [CrossRef] [PubMed]
- Joshi, N.V.; Vesey, A.T.; Williams, M.C.; Shah, A.S.; Calvert, P.A.; Craighead, F.H.; Yeoh, S.E.; Wallace, W.; Salter, D.; Fletcher, A.M.; et al. 18F-fluoride positron emission tomography for identification of ruptured and high-risk coronary atherosclerotic plaques: A prospective clinical trial. Lancet 2014, 383, 705–713. [Google Scholar] [CrossRef] [Green Version]
- Fiechter, M.; Haider, A.; Bengs, S.; Maredziak, M.; Burger, I.A.; Roggo, A.; Portmann, A.; Schade, K.; Warnock, G.I.; Treyer, V.; et al. Sex-dependent association between inflammation, neural stress responses, and impaired myocardial function. Eur. J. Nucl. Med. Mol. Imaging 2019. [Google Scholar] [CrossRef]
- Fiechter, M.; Bengs, S.; Roggo, A.; Haider, A.; Maredziak, M.; Portmann, A.; Treyer, V.; Burger, I.A.; Messerli, M.; Patriki, D.; et al. Association between vertebral bone mineral density, myocardial perfusion, and long-term cardiovascular outcomes: A sex-specific analysis. J. Nucl. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Rischpler, C.; Dirschinger, R.J.; Nekolla, S.G.; Kossmann, H.; Nicolosi, S.; Hanus, F.; van Marwick, S.; Kunze, K.P.; Meinicke, A.; Götze, K.; et al. Prospective Evaluation of 18F-Fluorodeoxyglucose Uptake in Postischemic Myocardium by Simultaneous Positron Emission Tomography/Magnetic Resonance Imaging as a Prognostic Marker of Functional Outcome. Circ. Cardiovasc. Imaging 2016, 9, e004316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aikawa, T.; Naya, M.; Manabe, O.; Obara, M.; Matsushima, S.; Tamaki, N.; Tsutsui, H. Incidental focal myocardial 18F-FDG uptake indicating asymptomatic coronary artery disease. J. Nucl. Cardiol. 2016, 23, 596–598. [Google Scholar] [CrossRef] [Green Version]
- Dou, K.F.; Yang, M.F.; Yang, Y.J.; Jain, D.; He, Z.X. Myocardial 18F-FDG uptake after exercise-induced myocardial ischemia in patients with coronary artery disease. J. Nucl. Med. 2008, 49, 1986–1991. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, N.; Rimoldi, O.E.; Beanlands, R.S.; Camici, P.G. Assessment of myocardial ischaemia and viability: Role of positron emission tomography. Eur. Heart J. 2010, 31, 2984–2995. [Google Scholar] [CrossRef]
- Accordino, M.K.; Neugut, A.I.; Hershman, D.L. Cardiac effects of anticancer therapy in the elderly. J. Clin. Oncol. 2014, 32, 2654–2661. [Google Scholar] [CrossRef] [Green Version]
- Sturgeon, K.M.; Deng, L.; Bluethmann, S.M.; Zhou, S.; Trifiletti, D.M.; Jiang, C.; Kelly, S.P.; Zaorsky, N.G. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur. Heart J. 2019. [Google Scholar] [CrossRef] [Green Version]
- Fiechter, M.; Roggo, A.; Burger, I.A.; Bengs, S.; Treyer, V.; Becker, A.; Maredziak, M.; Haider, A.; Portmann, A.; Messerli, M.; et al. Association between resting amygdalar activity and abnormal cardiac function in women and men: A retrospective cohort study. Eur. Heart J. Cardiovasc. Imaging 2019, 20, 625–632. [Google Scholar] [CrossRef]
- Pazhenkottil, A.P.; Nkoulou, R.N.; Ghadri, J.R.; Herzog, B.A.; Buechel, R.R.; Kuest, S.M.; Wolfrum, M.; Fiechter, M.; Husmann, L.; Gaemperli, O.; et al. Prognostic value of cardiac hybrid imaging integrating single-photon emission computed tomography with coronary computed tomography angiography. Eur. Heart J. 2011, 32, 1465–1471. [Google Scholar] [CrossRef] [Green Version]
- Hesse, B.; Tagil, K.; Cuocolo, A.; Anagnostopoulos, C.; Bardies, M.; Bax, J.; Bengel, F.; Busemann Sokole, E.; Davies, G.; Dondi, M.; et al. EANM/ESC procedural guidelines for myocardial perfusion imaging in nuclear cardiology. Eur. J. Nucl. Med. Mol. Imaging 2005, 32, 855–897. [Google Scholar] [CrossRef]
- Verberne, H.J.; Acampa, W.; Anagnostopoulos, C.; Ballinger, J.; Bengel, F.; De Bondt, P.; Buechel, R.R.; Cuocolo, A.; van Eck-Smit, B.L.; Flotats, A.; et al. EANM procedural guidelines for radionuclide myocardial perfusion imaging with SPECT and SPECT/CT: 2015 revision. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1929–1940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, D.S.; Kiat, H.; Friedman, J.D.; Wang, F.P.; van Train, K.; Matzer, L.; Maddahi, J.; Germano, G. Separate acquisition rest thallium-201/stress technetium-99m sestamibi dual-isotope myocardial perfusion single-photon emission computed tomography: A clinical validation study. J. Am. Coll. Cardiol. 1993, 22, 1455–1464. [Google Scholar] [CrossRef] [Green Version]
- Haider, A.; Possner, M.; Messerli, M.; Bengs, S.; Osto, E.; Maredziak, M.; Portmann, A.; Fiechter, M.; Giannopoulos, A.A.; Treyer, V.; et al. Quantification of intrathoracic fat adds prognostic value in women undergoing myocardial perfusion imaging. Int. J. Cardiol. 2019, 292, 258–264. [Google Scholar] [CrossRef]
- Siegrist, P.T.; Gaemperli, O.; Koepfli, P.; Schepis, T.; Namdar, M.; Valenta, I.; Aiello, F.; Fleischmann, S.; Alkadhi, H.; Kaufmann, P.A. Repeatability of cold pressor test-induced flow increase assessed with H(2)(15)O and PET. J. Nucl. Med. 2006, 47, 1420–1426. [Google Scholar] [PubMed]
- Wyss, C.A.; Koepfli, P.; Fretz, G.; Seebauer, M.; Schirlo, C.; Kaufmann, P.A. Influence of altitude exposure on coronary flow reserve. Circulation 2003, 108, 1202–1207. [Google Scholar] [CrossRef] [Green Version]
- Koepfli, P.; Wyss, C.A.; Namdar, M.; Klainguti, M.; von Schulthess, G.K.; Luscher, T.F.; Kaufmann, P.A. Beta-adrenergic blockade and myocardial perfusion in coronary artery disease: Differential effects in stenotic versus remote myocardial segments. J. Nucl. Med. 2004, 45, 1626–1631. [Google Scholar]
- Fiechter, M.; Haider, A.; Bengs, S.; Maredziak, M.; Burger, I.A.; Roggo, A.; Portmann, A.; Warnock, G.I.; Schade, K.; Treyer, V.; et al. Sex Differences in the Association between Inflammation and Ischemic Heart Disease. Thromb. Haemost. 2019, 119, 1471–1480. [Google Scholar] [CrossRef]
- Burger, I.A.; Lohmann, C.; Messerli, M.; Bengs, S.; Becker, A.; Maredziak, M.; Treyer, V.; Haider, A.; Schwyzer, M.; Benz, D.C.; et al. Age- and sex-dependent changes in sympathetic activity of the left ventricular apex assessed by 18F-DOPA PET imaging. PLoS ONE 2018, 13, e0202302. [Google Scholar] [CrossRef]
- Nose, H.; Otsuka, H.; Otomi, Y.; Terazawa, K.; Takao, S.; Iwamoto, S.; Iwase, T.; Yamada, H.; Sata, M.; Harada, M. The physiological uptake pattern of (18)F-FDG in the left ventricular myocardium of patients without heart disease. J. Med. Investig. 2014, 61, 53–58. [Google Scholar] [CrossRef] [Green Version]
- Floyd, J.D.; Nguyen, D.T.; Lobins, R.L.; Bashir, Q.; Doll, D.C.; Perry, M.C. Cardiotoxicity of cancer therapy. J. Clin. Oncol. 2005, 23, 7685–7696. [Google Scholar] [CrossRef]
- Minamimoto, R.; Morooka, M.; Miyata, Y.; Ito, K.; Okasaki, M.; Hara, H.; Okazaki, O.; Moroi, M.; Kubota, K. Incidental focal FDG uptake in heart is a lighthouse for considering cardiac screening. Ann. Nucl. Med. 2013, 27, 572–580. [Google Scholar] [CrossRef]
- Chavez-MacGregor, M.; Niu, J.; Zhang, N.; Elting, L.S.; Smith, B.D.; Banchs, J.; Hortobagyi, G.N.; Giordano, S.H. Cardiac Monitoring During Adjuvant Trastuzumab-Based Chemotherapy Among Older Patients With Breast Cancer. J. Clin. Oncol. 2015, 33, 2176–2183. [Google Scholar] [CrossRef] [Green Version]
- Lu, X.; Zhao, Y.; Chen, C.; Han, C.; Xue, L.; Xing, D.; Huang, O.; Tao, M. BNP as a marker for early prediction of anthracycline-induced cardiotoxicity in patients with breast cancer. Oncol. Lett. 2019, 18, 4992–5001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanderian, A.S.; Francis, G.S. Cardiac troponins and chronic kidney disease. Kidney Int. 2006, 69, 1112–1114. [Google Scholar] [CrossRef] [Green Version]
- Tarkin, J.M.; Joshi, F.R.; Rudd, J.H. PET imaging of inflammation in atherosclerosis. Nat. Rev. Cardiol. 2014, 11, 443–457. [Google Scholar] [CrossRef] [PubMed]
- Birnie, D.H.; Kandolin, R.; Nery, P.B.; Kupari, M. Cardiac manifestations of sarcoidosis: Diagnosis and management. Eur. Heart J. 2016, 38, 2663–2670. [Google Scholar] [CrossRef] [Green Version]
- Gewirtz, H.; Dilsizian, V. Myocardial viability. Circ. Res. 2017, 120, 1197–1212. [Google Scholar] [CrossRef] [PubMed]
- Ohira, H.; Tsujino, I.; Ishimaru, S.; Oyama, N.; Takei, T.; Tsukamoto, E.; Miura, M.; Sakaue, S.; Tamaki, N.; Nishimura, M. Myocardial imaging with 18F-fluoro-2-deoxyglucose positron emission tomography and magnetic resonance imaging in sarcoidosis. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Pak, K.; Kim, K. Diagnostic performance of F-18 FDG PET for detection of cardiac sarcoidosis; A systematic review and meta-analysis. J. Nucl. Cardiol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Ishimaru, S.; Tsujino, I.; Takei, T.; Tsukamoto, E.; Sakaue, S.; Kamigaki, M.; Ito, N.; Ohira, H.; Ikeda, D.; Tamaki, N.; et al. Focal uptake on 18F-fluoro-2-deoxyglucose positron emission tomography images indicates cardiac involvement of sarcoidosis. Eur. Heart J. 2005, 26, 1538–1543. [Google Scholar] [CrossRef]
- Stanley, W.C.; Recchia, F.A.; Lopaschuk, G.D. Myocardial substrate metabolism in the normal and failing heart. Physiol. Rev. 2005, 85, 1093–1129. [Google Scholar] [CrossRef]
- Dorbala, S.; Di Carli, M.F.; Delbeke, D.; Abbara, S.; DePuey, E.G.; Dilsizian, V.; Forrester, J.; Janowitz, W.; Kaufmann, P.A.; Mahmarian, J.; et al. SNMMI/ASNC/SCCT guideline for cardiac SPECT/CT and PET/CT 1.0. J. Nucl. Med. 2013, 54, 1485–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankar, L.K.; Hoffman, J.M.; Bacharach, S.; Graham, M.M.; Karp, J.; Lammertsma, A.A.; Larson, S.; Mankoff, D.A.; Siegel, B.A.; Van den Abbeele, A.; et al. Consensus recommendations for the use of 18F-FDG PET as an indicator of therapeutic response in patients in National Cancer Institute Trials. J. Nucl. Med. 2006, 47, 1059–1066. [Google Scholar]
- Maurer, A.H.; Burshteyn, M.; Adler, L.P.; Steiner, R.M. How to differentiate benign versus malignant cardiac and paracardiac 18F FDG uptake at oncologic PET/CT. Radiographics 2011, 31, 1287–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, L.R.; Gropler, R.J. Radionuclide imaging of myocardial metabolism. Circ. Cardiovasc. Imaging 2010, 3, 211–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camici, P.; Araujo, L.I.; Spinks, T.; Lammertsma, A.A.; Kaski, J.C.; Shea, M.J.; Selwyn, A.P.; Jones, T.; Maseri, A. Increased uptake of 18F-fluorodeoxyglucose in postischemic myocardium of patients with exercise-induced angina. Circulation 1986, 74, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Total Cohort n = 302 | No Myocardial 18F-FDG Uptake n = 109 | Diffuse Myocardial 18F-FDG Uptake n = 77 | Focal Myocardial 18F-FDG Uptake n = 24 | Focal on Diffuse Myocardial 18F-FDG Uptake n = 92 | p-Value |
|---|---|---|---|---|---|---|
| Male sex, n (%) | 210 (71.4) | 75 (68.8) | 50 (64.9) | 18 (75.0) | 67 (72.8) | 0.58 |
| Age, mean ± SD | 66.8 ± 10.2 | 66.2 ± 11.1 | 66.9 ± 9.5 | 65.1 ± 10.6 | 68.0 ± 9.7 | 0.49 |
| BMI, mean ± SD | 26.2 ± 5.3 | 26.2 ± 5.1 | 25.1 ± 5.1 | 28.6 ± 5.4 | 26.4 ± 5.3 | 0.05 |
| Active malignancy, n (%) | 193 (63.9) | 80 (73.4) | 43 (55.8) | 14 (58.3) | 56 (60.9) | 0.07 |
| Diabetes, n (%) | 56 (18.5) | 23 (21.1) | 8 (10.4) | 5 (20.8) | 20 (21.7) | 0.21 |
| Hypertension, n (%) | 142 (47.0) | 46 (42.2) | 40 (51.9) | 11 (45.8) | 45 (48.9) | 0.59 |
| Smoking, n (%) | 93 (30.9) | 35 (32.1) | 20 (26.0) | 9 (37.5) | 29 (31.9) | 0.69 |
| Dyslipidemia, n (%) | 73 (24.2) | 25 (22.9) | 19 (24.7) | 6 (25.0) | 23 (25.0) | 0.98 |
| Positive family history, n (%) | 25 (8.3) | 9 (8.3) | 7 (9.1) | 5 (20.8) | 4 (4.3) | 0.074 |
| Known CAD, n (%) | 117 (38.7) | 45 (41.3) | 27 (35.1) | 13 (54.2) | 32 (34.8) | 0.29 |
| Previous MI, n (%) | 54 (18.9) | 17 (15.6) | 16 (20.8) | 8 (33.3) | 16 (17.4) | 0.23 |
| Previous PCI/CABG, n (%) | 82 (27.2) | 32 (29.4) | 18 (23.4) | 7 (29.2) | 25 (27.2) | 0.83 |
| Symptoms, n (%) Typical angina Atypical angina Dyspnea None | 30 (9.9) 23 (7.6) 39 (12.9) 210 (69.5) | 9 (8.3) 8 (7.3) 18 (16.5) 74 (67.9) | 7 (9.1) 2 (2.6) 10 (13.0) 58 (75.3) | 6 (25.0) 3 (12.5) 1 (4.2) 14 (58.3) | 8 (8.7) 10 (10.9) 10 (10.9) 64 (69.6) | 0.114 |
| Chronic pain, n (%) | 90 (30.1) | 33 (31.1) | 20 (26.0) | 11 (45.8) | 26 (28.3) | 0.30 |
| Depression, n (%) | 19 (6.5) | 6 (5.8) | 8 (10.4) | 1 (4.3) | 4 (4.5) | 0.43 |
| Medication, n (%) Statin Betablocker ACE inhibitors/ARBs Aspirin Corticosteroids Analgesics | 126 (44.5) 146 (51.6) 156 (55.1) 128 (45.2) 40 (14.2) 135 (47.9) | 43 (42.6) 52 (51.5) 48 (47.5) 43 (42.6) 17 (16.8) 51 (50.5) | 33 (45.2) 36 (49.3) 46 (63.0) 37 (50.7) 9 (12.3) 40 (54.8) | 13 (59.1) 14 (63.6) 16 (72.7) 11 (50.0) 4 (18.2) 10 (45.5) | 37 (42.5) 44 (50.6) 46 (52.9) 37 (42.5) 10 (11.6) 34 (39.5) | 0.53 0.69 0.07 0.65 0.67 0.25 |
| Creatinine (µM/L), mean ± SD | 116.3 ± 124.0 | 102.0 ± 94.1 | 118.1 ± 126.9 | 173.0 ± 210.3 | 117.3 ± 122.0 | 0.11 |
| CRP (mg/L), mean ± SD | 24.6 ± 43.5 | 28.5 ± 47.6 | 19.5 ± 39.0 | 29.1 ± 37.6 | 22.8 ± 43.4 | 0.59 |
| WCB count (10*/µ/L), mean ± SD | 7.8 ± 3.3 | 8.2 ± 3.3 | 7.3 ± 3.2 | 8.0 ± 4.4 | 7.8 ± 2.9 | 0.44 |
| NT proBNP (ƞg/L), mean ± SD | 3604.2 ± 13345.4 | 903.0 ± 1406.3 | 13584.3 ± 27932.0 | 2306.2 ± 2229.4 | 718.4 ± 808.6 | 0.045 |
| Baseline Characteristics | Total Cohort n = 302 | Normal Myocardial Perfusion/Function n = 181 | Abnormal Myocardial Perfusion/Function n = 121 | p-Value |
|---|---|---|---|---|
| Male sex, n (%) | 210 (71.4) | 113 (38.4) | 97 (33.0) | 0.002 |
| Age, mean ± SD | 66.8 ± 10.2 | 66.5 ± 10.5 | 67.4 ± 9.8 | 0.45 |
| BMI, mean ± SD | 26.2 ± 5.3 | 26.1 ± 5.2 | 26.3 ± 5.3 | 0.74 |
| Active malignancy, n (%) | 193 (63.9) | 118 (39.1) | 75 (24.8) | 0.33 |
| Diabetes, n (%) | 56 (18.5) | 33 (10.9) | 23 (7.6) | 0.49 |
| Hypertension, n (%) | 142 (47.0) | 84 (27.8) | 58 (19.2) | 0.44 |
| Smoking, n (%) | 93 (30.9) | 54 (17.9) | 39 (13.0) | 0.39 |
| Dyslipidemia, n (%) | 73 (24.2) | 42 (13.9) | 31 (10.3) | 0.36 |
| Positive family history, n (%) | 25 (8.3) | 15 (5.0) | 10 (3.3) | 0.59 |
| Known CAD, n (%) | 117 (38.7) | 51 (16.9) | 66 (21.9) | <0.001 |
| Previous MI, n (%) | 54 (18.9) | 15 (5.0) | 42 (13.9) | <0.001 |
| Previous PCI/CABG, n (%) | 82 (27.2) | 34 (11.3) | 48 (15.9) | <0.001 |
| Chronic pain, n (%) | 90 (30.1) | 51 (17.1) | 39 (13.0) | 0.27 |
| Depression, n (%) | 19 (6.5) | 11 (3.8) | 8 (2.7) | 0.49 |
| CRP (mg/L), mean ± SD | 24.6 ± 43.5 | 27.3 ± 51.6 | 26.3 ± 44.4 | 0.89 |
| WCB count (10*/µ/L), mean ± SD | 7.8 ± 3.3 | 7.8 ± 2.7 | 7.8 ± 3.3 | 0.94 |
| NT proBNP (ƞg/L), mean ± SD | 3604 ± 13,345 | 612 ± 946 | 6956 ± 19,045 | 0.08 |
| Stepwise Logistic Regression Model for Abnormal Myocardial Function/Perfusion in Total Cohort (n = 302) | |||
|---|---|---|---|
| Independent Variables | OR | OR (95% CI) | p-Value |
| Model 1 Previous MI | 6.50 | 3.11–13.58 | <0.001 |
| Model 2 Focal myocardial 18F-FDG uptake Previous MI | 4.72 6.37 | 1.59–14.01 3.02–13.44 | 0.005 <0.001 |
| Model 3 Male sex Focal myocardial 18F-FDG uptake Previous MI | 2.15 5.32 6.27 | 1.13–4.08 1.73–16.34 2.94–13.38 | 0.020 0.003 <0.001 |
| A. Stepwise Logistic Regression Model for Reversible Perfusion Defect in Total Cohort (n = 302) * | |||
|---|---|---|---|
| Independent Variables | OR | OR (95% CI) | p-Value |
| Model 1 Focal myocardial 18F-FDG uptake | 4.17 | 1.53–11.4 | 0.005 |
| B. Stepwise logistic regression model for irreversible perfusion defect in total cohort (n = 302) * | |||
| Independent variables | OR | OR (95% CI) | p-value |
| Model 1 Focal myocardial 18F-FDG uptake | 3.78 | 1.47–9.69 | 0.006 |
| C. Stepwise logistic regression model for LVEF <50% in total cohort (n = 302) * | |||
| Independent variables | OR | OR (95% CI) | p-value |
| Model 1 No myocardial 18F-FDG uptake | 0.36 | 0.19–0.67 | 0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haider, A.; Bengs, S.; Schade, K.; Wijnen, W.J.; Portmann, A.; Etter, D.; Fröhlich, S.; Warnock, G.I.; Treyer, V.; Burger, I.A.; et al. Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT. J. Clin. Med. 2020, 9, 2279. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072279
Haider A, Bengs S, Schade K, Wijnen WJ, Portmann A, Etter D, Fröhlich S, Warnock GI, Treyer V, Burger IA, et al. Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT. Journal of Clinical Medicine. 2020; 9(7):2279. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072279
Chicago/Turabian StyleHaider, Ahmed, Susan Bengs, Katharina Schade, Winandus J. Wijnen, Angela Portmann, Dominik Etter, Sandro Fröhlich, Geoffrey I. Warnock, Valerie Treyer, Irene A. Burger, and et al. 2020. "Myocardial 18F-FDG Uptake Pattern for Cardiovascular Risk Stratification in Patients Undergoing Oncologic PET/CT" Journal of Clinical Medicine 9, no. 7: 2279. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9072279