Differentiating Females with Rett Syndrome and Those with Multi-Comorbid Autism Spectrum Disorder Using Physiological Biomarkers: A Novel Approach

Abstract
:1. Introduction
2. Methods
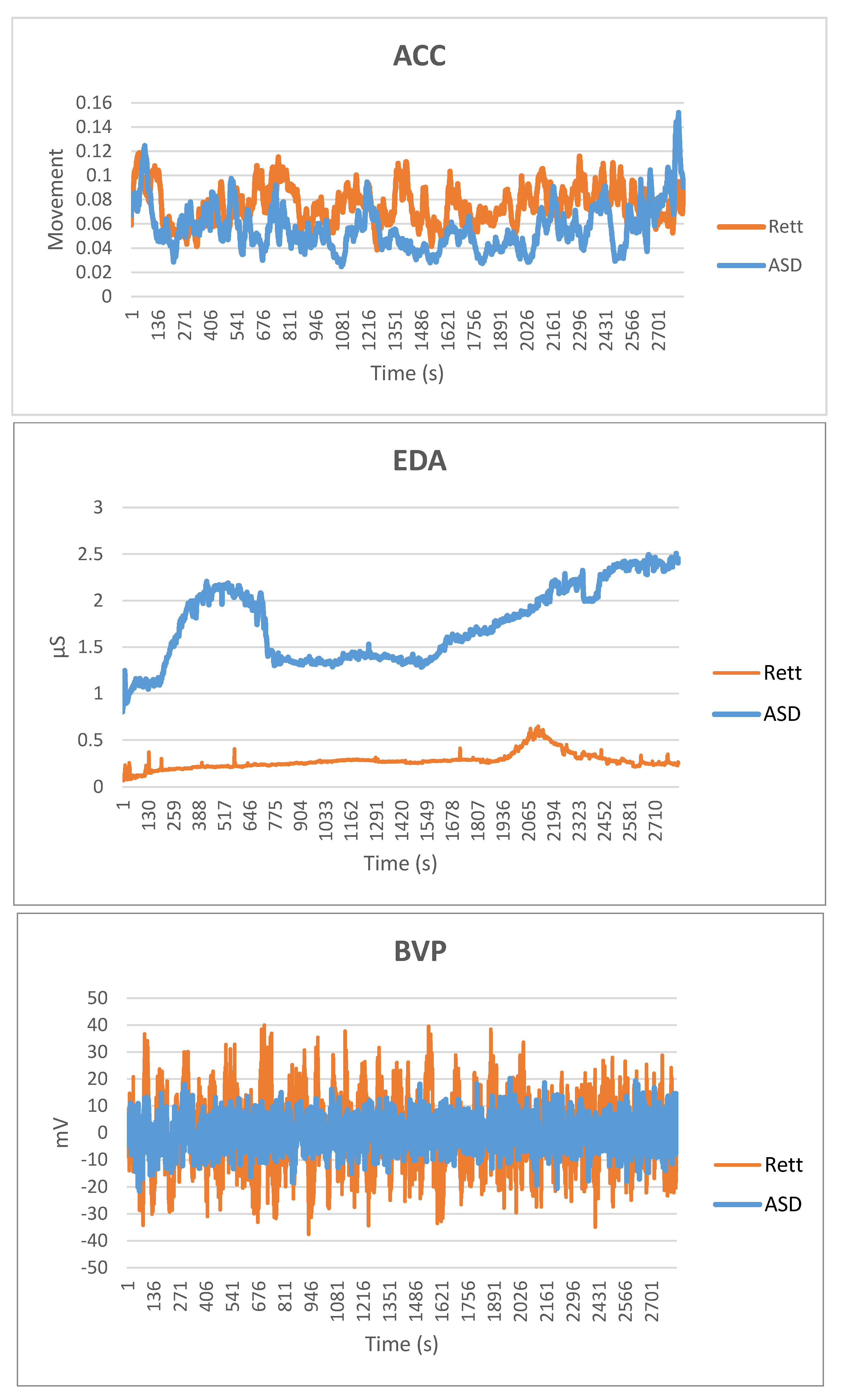
- Movement and/or 3-axis acceleration (Accelerometers (ACC) [g])
- Electrodermal Activity (EDA) in micro Siemens (µS)
- Blood Volume Pulse (BVP) in nanoWatt (nW)
- (1)
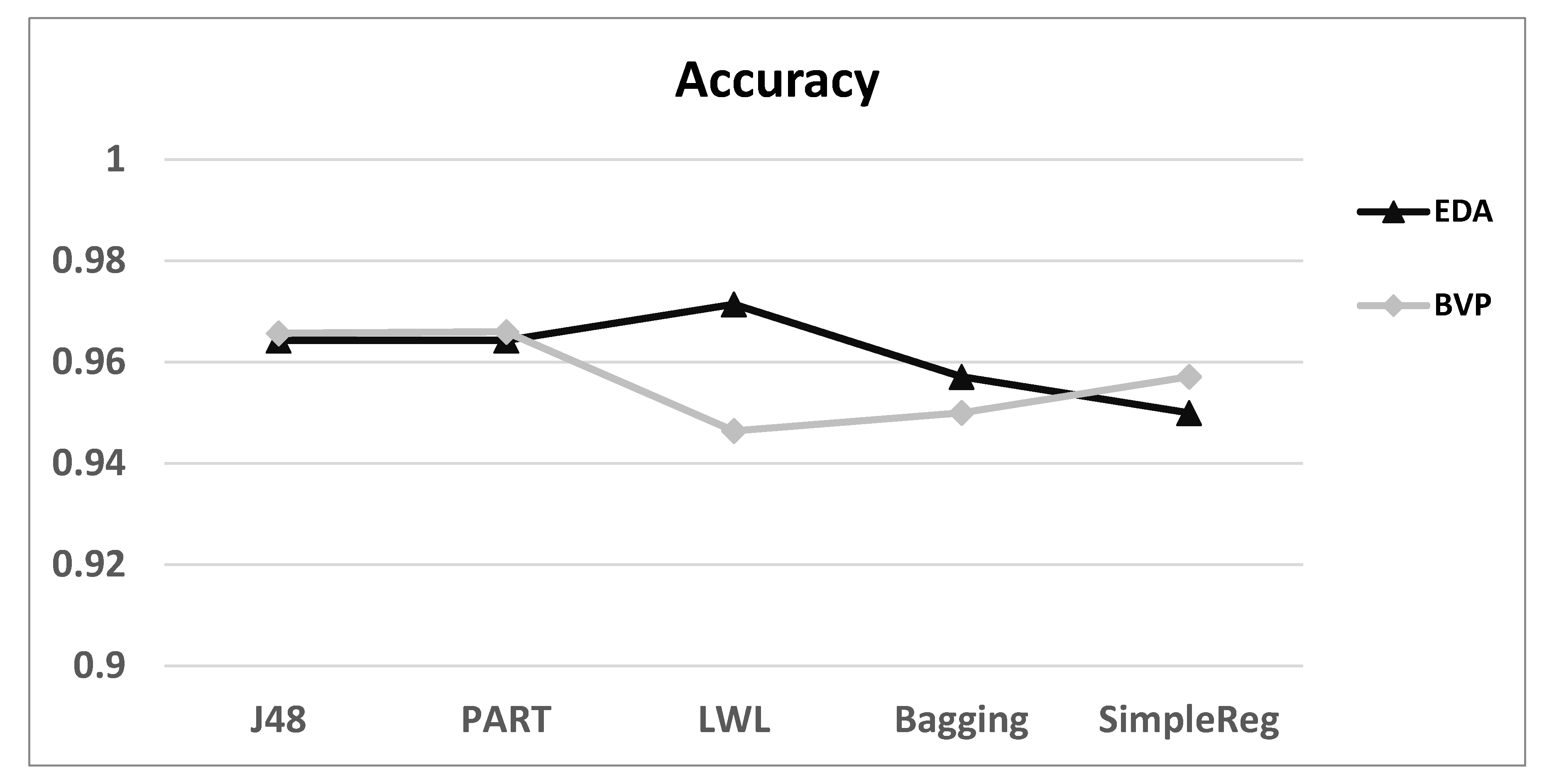
- Accuracy: The accuracy measure provides information about the percentage of participants that were classified correctly by the model, regardless of whether they are characterised as ASD or Rett.
- (2)
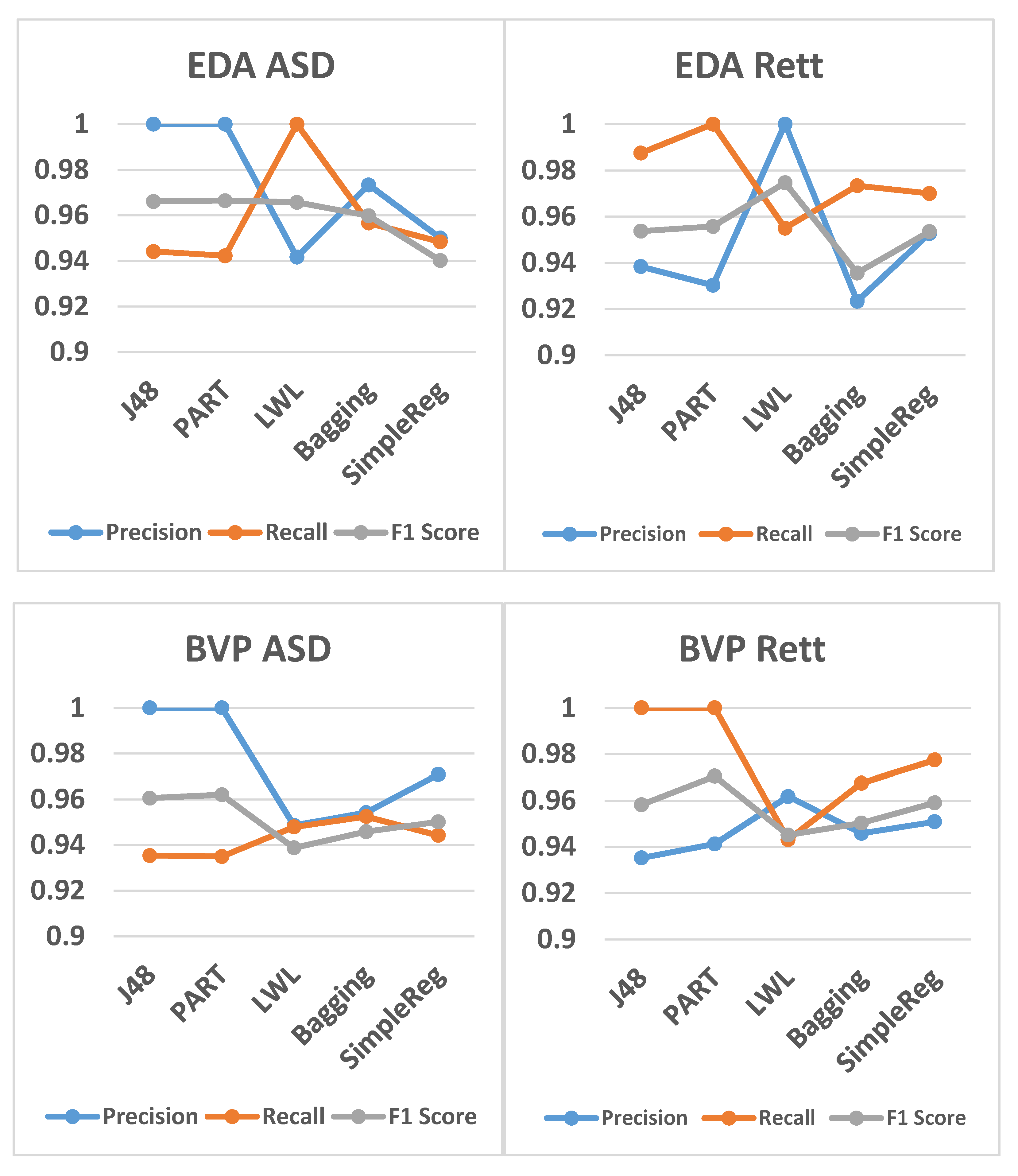
- Precision (Specificity): The precision measure offers information about how many participants the model classified with the correct diagnosis when predicting the label X, where X can be ‘ASD’ or ‘Rett’.
- (3)
- Recall (Sensitivity): The recall measure offers information about how many participants out of all participants with label X were correctly classified by the model. Precision and recall are metrics that provide label-specific information.
- (4)
- F1 Score: The F1 Score combines the precision and recall measures, since precision and recall provide different information.
2.1. Filtering and Feature Extraction
2.2. Model Learning and Prediction
- 1.
- Trees (algorithms that use decision trees):
- J48: an algorithm for building a decision tree [33].
- 2.
- Rules (algorithms that apply decision rules):
- PART: Class for generating a PART decision list. Uses separate-and-conquer. Builds a partial C4.5 decision tree in each iteration and makes the "best" leaf into a rule [34].
- 3.
- Lazy (algorithms that use lazy learning):
- LWL: Locally weighted learning. Uses an instance-based algorithm to assign instance weights. Can do classification (e.g., using naive Bayes) or regression (e.g., using linear regression) [35].
- 4.
- Meta (algorithms that apply or combine multiple algorithms (ensemble methods)):
- Bagging: an ensemble algorithm that learns base models on subsets of the training data with the purpose of reducing variance and avoiding overfitting [36].
- 5.
- Function (algorithms that estimate a function):
- Simple logistic regression: Classifier for building linear logistic regression models, with simple regression functions as base learners [37]. Note that this is analogous to linear regression, except that the dependant variable is nominal (as it is in our case) and not a measurement.
2.3. Ethics Approval and Consent to Participate
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fehr, S.; Bebbington, A.; Nassar, N.; Downs, J.; Ronen, G.M.; De Klerk, N.; Leonard, H. Trends in the diagnosis of Rett syndrome in Australia. Pediatr. Res. 2011, 70, 313–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neul, J.L.; Kaufmann, W.E.; Glaze, D.G.; Christodoulou, J.; Clarke, A.J.; Bahi-Buisson, N.; Leonard, H.; Bailey, M.E.; Schanen, N.C.; Zappella, M.; et al. Rett syndrome: Revised diagnostic criteria and nomenclature. Ann. Neurol. 2010, 68, 944–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amir, R.E.; Van den Veyver, I.B.; Wan, M.; Tran, C.Q.; Francke, U.; Zoghbi, H.Y. Rett Syndrome is Caused by Mutations in X-linked MECP2, Encoding Methyl-CpG-Binding Protein 2. Available online: http://genetics.nature.com (accessed on 19 February 2020).
- Gabel, H.W.; Kinde, B.; Stroud, H.; Gilbert, C.S.; Harmin, D.A.; Kastan, N.R.; Hemberg, M.; Ebert, D.H.; Greenberg, M.E. Disruption of DNA-methylation-dependent long gene repression in Rett syndrome. Nature 2015, 522, 89–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Julu, P.O.O.; Kerr, A.M.; Apartopoulos, F.; Al-Rawas, S.; Engerström, I.W.; Engerström, L.; Jamal, G.A.; Hansen, S. Characterisation of Breathing and Associated Central Autonomic Dysfunction in the Rett disorder. Available online: www.archdischild.com (accessed on 19 February 2020).
- Kerr, A.M.; Armstrong, D.D.; Prescott, R.J.; Doyle, D.K.D. Rett syndrome: Analysis of deaths in the British survey. Eur. Child Adolesc. Psychiatry 1997, 6 (Suppl. S1), 71–74. [Google Scholar] [PubMed]
- Singh, J.; Lanzarini, E.; Santosh, P. Autonomic dysfunction and sudden death in patients with Rett syndrome: A systematic review. J. Psychiatry Neurosci. 2020, 45, 150–181. [Google Scholar] [CrossRef]
- Singh, J.; Santosh, P. Key issues in Rett syndrome: Emotional, behavioural and autonomic dysregulation (EBAD)—A target for clinical trials. Orphanet J. Rare Dis. 2018, 13, 128. [Google Scholar] [CrossRef] [Green Version]
- Guideri, F.; Acampa, M.; DiPerri, T.; Zappella, M.; Hayek, Y. Progressive cardiac dysautonomia observed in patients affected by classic Rett syndrome and not in the preserved speech variant. J. Child Neurol. 2001, 16, 370–373. [Google Scholar] [CrossRef]
- MacKay, J.; Downs, J.; Wong, K.; Heyworth, J.; Epstein, A.; Leonard, H. Autonomic breathing abnormalities in Rett syndrome: Caregiver perspectives in an international database study. J. Neurodev. Disord. 2017, 9, 15. [Google Scholar] [CrossRef]
- Pini, G.; Bigoni, S.; Congiu, L.; Romanelli, A.M.; Scusa, M.F.; Di Marco, P.; Benincasa, A.; Morescalchi, P.; Ferlini, A.; Bianchi, F.; et al. Rett syndrome: A wide clinical and autonomic picture. Orphanet J. Rare Dis. 2016, 11, 132. [Google Scholar] [CrossRef] [Green Version]
- Leonard, H.; Cobb, S.; Downs, J. Clinical and biological progress over 50 years in Rett syndrome. Nat. Rev. Neurol. 2017, 13, 37–51. [Google Scholar] [CrossRef] [Green Version]
- Tarquinio, D.C.; Hou, W.; Berg, A.; Kaufmann, W.E.; Lane, J.B.; Skinner, S.A.; Motil, K.J.; Neul, J.L.; Percy, A.K.; Glaze, D.G. Longitudinal course of epilepsy in Rett syndrome and related disorders. Brain 2017, 140, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Singh, J.; Santosh, P.J. Psychopharmacology of Neurodevelopmental Disorders in Children. In Child and Adolescent Psychiatry: Asian Perspectives; Springer: Berlin, Germany, 2017; pp. 63–77. [Google Scholar] [CrossRef]
- Sagar-Ouriaghli, I.; Lievesley, K.; Santosh, P.J. Propranolol for treating emotional, behavioural, autonomic dysregulation in children and adolescents with autism spectrum disorders. J. Psychopharmacol. 2018, 32, 325–362. [Google Scholar] [CrossRef] [PubMed]
- Santosh, P.J.; Bell, L.; Lievesley, K.; Singh, J.; Fiori, F. Paradoxical physiological responses to propranolol in a Rett syndrome patient: A case report. BMC Pediatr. 2016, 16, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. DSM-5. Diagnostic and Statistical Manual of Mental Disorders. 2013. Available online: https://symbiose.uqo.ca/apps/LoginSigparb/LoginPourRessources.aspx?url=http://www.psychiatryonline.org/%5Cnhttp://sbiproxy.uqac.ca/login?url=http://dsm.psychiatryonline.org/book.aspx?bookid=556 (accessed on 19 February 2020).
- Theoharides, T.C.; Athanassiou, M.; Panagiotidou, S.; Doyle, R. Dysregulated brain immunity and neurotrophin signaling in Rett syndrome and autism spectrum disorders. J. Neuroimmunol. 2015, 279, 33–38. [Google Scholar] [CrossRef]
- Schwartzman, J.S.; Rde, L.V.; D’Antino, M.E.; Santos, S. The eye-tracking of social stimuli in patients with Rett syndrome and autism spectrum disorders: A pilot study. Arq. Neuro-Psiquiatr. 2015, 73, 402–407. [Google Scholar] [CrossRef] [PubMed]
- Santosh, P.; Gringras, P.; Baird, G.; Fiori, F.; Sala, R. Development and psychometric properties of the parent version of the Profile of Neuropsychiatric Symptoms (PONS) in children and adolescents. BMC Pediatr. 2015, 15, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbarino, M.; Lai, M.; Bender, D.; Picard, R.W.; Tognett, S. Empatica E3—A wearable wireless multi-sensor device for real-time computerized biofeedback and data acquisition. In Proceedings of the 4th International Conference on Wireless Mobile Communication and Healthcare, Athens, Greece, 3–5 November 2014; pp. 3–6. [Google Scholar]
- Trobec, R.; Rashkovska, A.; Avbelj, V. Two proximal skin electrodes—A respiration rate body sensor. Sensors 2012, 12, 13813–13828. [Google Scholar] [CrossRef] [Green Version]
- Gjoreski, M.; Luštrek, M.; Gams, M.; Gjoreski, H. Monitoring stress with a wrist device using context. J. Biomed. Inform. 2017, 73, 159–170. [Google Scholar] [CrossRef]
- Ragot, M.; Martin, N.; Em, S.; Pallamin, N.; Diverrez, J.M. Emotion Recognition Using Physiological Signals: Laboratory vs. Wearable Sensors. In Advances in Human Factors in Wearable Technologies and Game Design; Ahram, T., Falcão, C., Eds.; AHFE 2017; Advances in Intelligent Systems and Computing; Springer: Cham, Switzerland, 2018; Volume 608. [Google Scholar]
- Taj-Eldin, M.; Ryan, C.; O’Flynn, B.; Galvin, P. A Review of Wearable Solutions for Physiological and Emotional Monitoring for Use by People with Autism Spectrum Disorder and Their Caregivers. Sensors (Basel) 2018, 18, 4271. [Google Scholar] [CrossRef] [Green Version]
- Camacho, D.M.; Collins, K.M.; Powers, R.K.; Costello, J.C.; Collins, J.J. Next-Generation Machine Learning for Biological Networks. Cell 2018, 173, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Hall, M.; Frank, E.; Holmes, G.; Pfahringer, B.; Reutemann, P.; Witten, I. WEKA data mining software: An update. ACM SIGKDD Explor. Newsl. 2008, 11, 10–18. [Google Scholar] [CrossRef]
- Dawson, M.E.; Schell, A.M.; Filion, D.L. The electrodermal system. In The Handbook of Psychophysiology; Cacioppo, J.T., Tassinary, L.G., Berntson, G.G., Eds.; Cambridge University Press: New York, NY, USA, 2007; pp. 159–181. [Google Scholar]
- Van Lier, H.G.; Pieterse, M.E.; Garde, A.; Postel, M.G.; de Haan, H.A.; Vollenbroek-Hutten, M.M. A standardized validity assessment protocol for physiological signals from wearable technology: Methodological underpinnings and an application to the E4 biosensor. Behav. Res. Methods 2019. [Google Scholar] [CrossRef]
- Available online: https://www.empatica.com (accessed on 19 February 2020).
- Witten, I.; Frank, E. Data Mining: Practical Machine Learning Tools and Techniques, 2nd ed.; Morgan Kaufmann Publishers Inc.: San Francisco, CA, USA, 2005. [Google Scholar]
- Quinlan, J.R. C4.5: Programs for Machine Learning; Morgan Kaufmann Publishers Inc.: San Francisco, CA, USA, 1993. [Google Scholar]
- Quinlan, J.R. Improved use of continuous attributes, in C4.5. J. Artif. Intell. Res. 1996, 4, 77–90. [Google Scholar] [CrossRef] [Green Version]
- Frank, E.; Witten, I. Generating Accurate Rule Sets Without Global Optimization. In Fifteenth International Conference on Machine Learning; Morgan Kaufmann Publishers Inc.: San Francisco, CA, USA, 1998; pp. 144–151. [Google Scholar]
- Frank, E.; Hall, M.; Pfahringer, B. Locally Weighted Naive Bayes, In 19th Conference in Uncertainty in Artificial Intelligence; Morgan Kaufmann Publishers Inc.: San Francisco, CA, USA, 2003; pp. 249–256. [Google Scholar]
- Breiman, L. Technical Report No. 421. Mach. Learn. 1994, 1–19. [Google Scholar]
- Sumner, M.; Frank, E.; Hall, M. Speeding up Logistic Model Tree Induction. In European Conference on Principles of Data Mining and Knowledge Discovery; Springer: Berlin, Germany, 2005; pp. 675–683. [Google Scholar]
- Fisher, R.A.; Yates, F. Statistical Tables for Biological, Agricultural and Medical Research, 6th ed.; Oliver & Boyd: Edinburgh, UK; London, UK, 1963. [Google Scholar]
- Van Steensel, F.J.; Bögels, S.M.; Perrin, S. Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clin. Child Fam. Psychol. Rev. 2011, 14, 302–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kushki, A.; Brian, J.; Dupuis, A.; Anagnostou, E. Functional autonomic nervous system profile in children with autism spectrum disorder. Mol. Autism. 2014, 5, 39. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| ASD with ID Participants | ||||
| Patient No. | Age | Gender | Diagnoses | Medications |
| 1 | 19 | F |
| Sertraline Propranolol Vitamin D |
| 2 | 9 | F |
| Sertraline Omeprazole Ranitidine Melatonin Alimemazine |
| 3 | 16 | F |
| Aripiprazole |
| 4 | 17 | F |
| Clozapine Sodium valproate Aripiprazole |
| 5 | 13 | F |
| Aripiprazole Buspirone |
| 6 | 15 | F |
| Carbamazepine Topiramate Clobazam Perampanel Melatonin |
| 7 | 16 | F |
| Lansoprazole Levetiracetam Clobazam Lacosamide |
| 8 | 11 | F |
| Risperidone Carbamazepine Sertraline Melatonin Omeprazole Spironolactone Potassium |
| 9 | 13 | F |
| Sodium valproate Baclofen Trihexyphendyl Omeprazole Domperidone Risperidone Citalopram Propranolol |
| 10 | 16 | F |
| Fluoxetine Buspirone Risperidone Aripiprazole Trihexyphenidyl Cholecalciferol Lactulose Lansoprazole Levothyroxine |
| Rett Participants | ||||
| Patient Nr. | Age | Gender | Diagnoses | Medications |
| 1 | 17 | F |
| Sertraline Gaviscon Omeprazole Lactulose |
| 2 | 5 | F |
| Melatonin |
| 3 | 18 | F |
| Sodium valproate Lamotrigine Clobazam Azithromycin Buspirone Trihexyphenidyl Baclofen Ondasetron Ranitidine Sodium picosulfate |
| 4 | 8 | F |
| Osmotic laxatives |
| 5 | 9 | F |
| Sodium valproate |
| 6 | 20 | F |
| Sodium valproate |
| 7 | 9 | F |
| Ranitidine Melatonin Osmotic laxatives |
| 8 | 6 | F |
| None |
| 9 | 15 | F |
| Omeprazole Melatonin Lamotrigine Diazepam Clobazam Pizotifen |
| 10 | 14 | F |
| Movicol Vitamin D |
| ASD Participants | |||
| Activity Levels | Autonomic Function | ||
| Cases | ACC | EDA | BVP |
| 1 | |||
| 2 | |||
| 3 | |||
| 4 | |||
| 5 | |||
| 6 | |||
| 7 | |||
| 8 | |||
| 9 | |||
| 10 | |||
| Rett Participants | |||
| Activity Levels | Autonomic Function | ||
| Cases | ACC | EDA | BVP |
| 1 | |||
| 2 | |||
| 3 | |||
| 4 | |||
| 5 | |||
| 6 | |||
| 7 | |||
| 8 | |||
| 9 | |||
| 10 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iakovidou, N.; Lanzarini, E.; Singh, J.; Fiori, F.; Santosh, P. Differentiating Females with Rett Syndrome and Those with Multi-Comorbid Autism Spectrum Disorder Using Physiological Biomarkers: A Novel Approach. J. Clin. Med. 2020, 9, 2842. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092842
Iakovidou N, Lanzarini E, Singh J, Fiori F, Santosh P. Differentiating Females with Rett Syndrome and Those with Multi-Comorbid Autism Spectrum Disorder Using Physiological Biomarkers: A Novel Approach. Journal of Clinical Medicine. 2020; 9(9):2842. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092842
Chicago/Turabian StyleIakovidou, Nantia, Evamaria Lanzarini, Jatinder Singh, Federico Fiori, and Paramala Santosh. 2020. "Differentiating Females with Rett Syndrome and Those with Multi-Comorbid Autism Spectrum Disorder Using Physiological Biomarkers: A Novel Approach" Journal of Clinical Medicine 9, no. 9: 2842. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092842