Adipokines as Biomarkers of Atopic Dermatitis in Adults

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
Statistical Elaboration
3. Results
3.1. Adiponectin
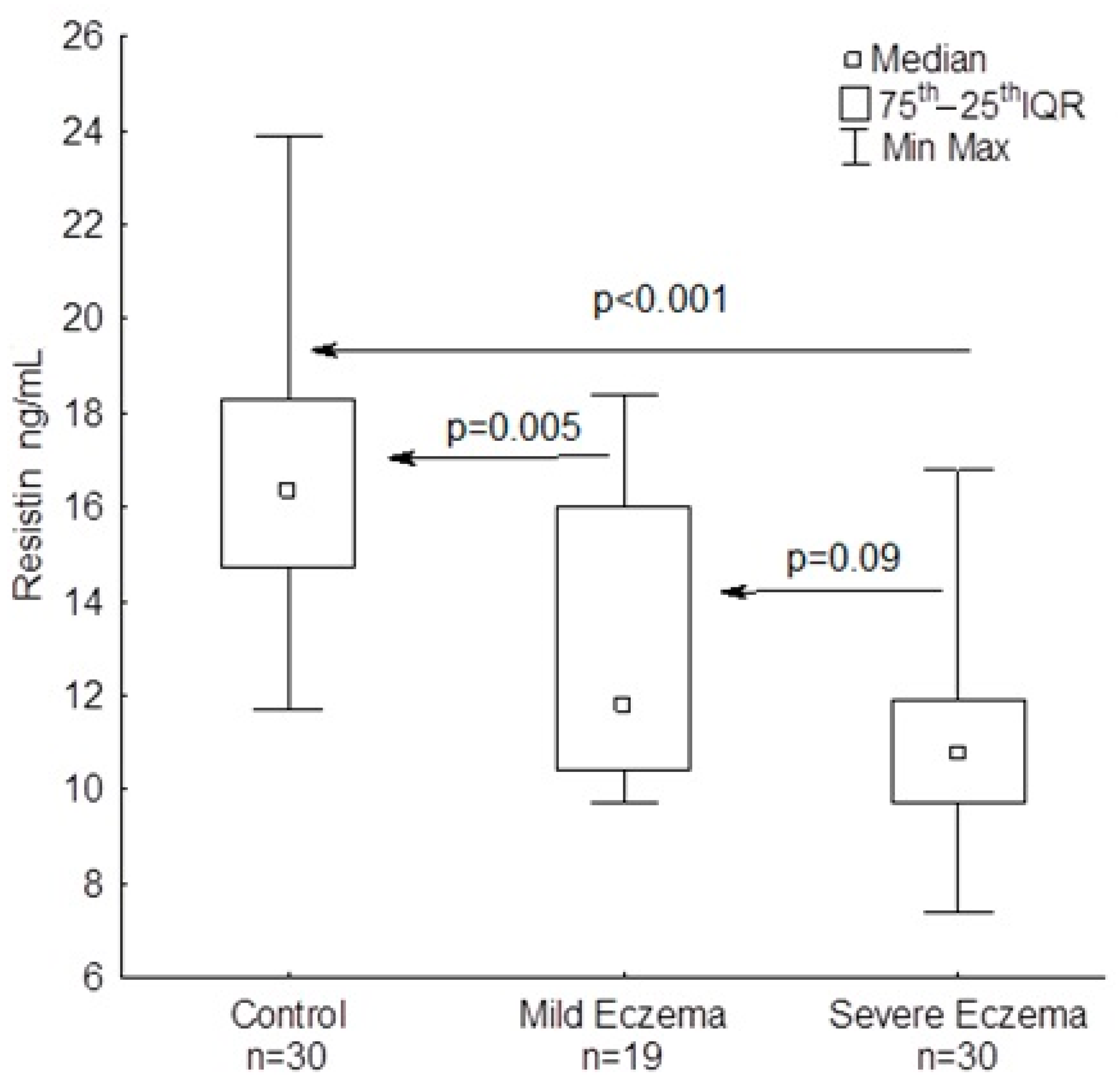
3.2. Resistin
3.3. Lipocalin-2
3.4. Leptin
3.5. Vaspin
4. Discussion
4.1. Potential Biomarkers of Eczema Severity
4.2. Other Adipokines and Body Mass
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Weidinger, S.; Beck, L.A.; Bieber, T.; Kabashima, K.; Irvine, A.D. Atopic dermatitis. Nat. Rev. Dis. Prim. 2018, 4, 1. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I. Comorbidities and the impact of atopic dermatitis. Ann. Allergy Asthma Immunol. 2019, 123, 144–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveira, C.; Torres, T. More than skin deep: The systemic nature of atopic dermatitis. Eur. J. Dermatol. 2019, 29, 250–258. [Google Scholar] [PubMed]
- Silverberg, J.I. Atopic dermatitis in adults. Med. Clin. N. Am. 2020, 104, 157–176. [Google Scholar] [CrossRef]
- Kwa, M.; Silverberg, J.I. Association between inflammatory skin disease, cardiovascular and cerebrovascular comorbidities in US adults: Analysis of Nationwide Inpatient Sample data. Am. J. Clin. Dermatol. 2017, 18, 813–823. [Google Scholar] [CrossRef]
- Silverberg, J.I.; Garg, N.K.; Paller, A.S.; Fishbein, A.B.; Zee, P.C. Sleep disturbances in adults with eczema are associated with impaired overall health: A US population-based study. J. Investig. Dermatol. 2015, 135, 56–66. [Google Scholar] [CrossRef] [Green Version]
- Harrop, J.; Chinn, S.; Verlato, G.; Olivieri, M.; Norbäck, D.; Wjst, M.; Janson, C.; Zock, J.-P.; Leynaert, B.; Gislason, D.; et al. Eczema, atopy and allergen exposure in adults: A population-based study. Clin. Exp. Allergy 2007, 37, 526–535. [Google Scholar] [CrossRef] [PubMed]
- Sybilski, A.J.; Raciborski, F.; Lipiec, A.; Tomaszewska, A.; Lusawa, A.; Samel-Kowalik, P.; Walkiewicz, A.; Krzych-Fałta, E.; Samoliński, B. Epidemiology of atopic dermatitis in Poland according to the Epidemiology of Allergic Disorders in Poland (ECAP) study. J. Dermatol. 2014, 42, 140–147. [Google Scholar] [CrossRef] [PubMed]
- Barbarot, S.; Auziere, S.; Gadkari, A.; Girolomoni, G.; Puig, L.; Simpson, E.L.; Margolis, D.J.; Bruin-Weller, M.; Eckert, L. Epidemiology of atopic dermatitis in adults: Results from an international survey. Allergy 2018, 73, 1284–1293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raciborski, F.; Jahnz-Rozyk, K.; Kłak, A.; Sybilski, A.J.; Grąbczewska, A.M.; Brzozowska, M.; Śliwczyński, A.M. Epidemiology and direct costs of atopic dermatitis in Poland based on the National Health Fund register (2008–2017). Adv. Dermatol. Alergol. 2019, 36, 727–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Furue, M.; Ulzii, D.; Vu, Y.H.; Tsuji, G.; Kido-Nakahara, M.; Nakahara, T. Pathogenesis of atopic dermatitis: Current paradigm. Iran. J. Immunol. 2019, 16, 97–107. [Google Scholar]
- Yang, G.; Seok, J.K.; Kang, H.C.; Cho, Y.Y.; Lee, H.S.; Lee, J.Y. Skin barrier abnormalities and immune dysfunction in atopic dermatitis. Int. J. Mol. Sci. 2020, 21, 2867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahlgren, C.F. Itch and atopic dermatitis: Clinical and experimental studies. Acta Derm. Venercol. Suppl. 1991, 165, 1–53. [Google Scholar]
- Choi, J.E.; Di Nardo, A. Skin neurogenic inflammation. Semin. Immunopathol. 2018, 40, 249–259. [Google Scholar] [CrossRef] [PubMed]
- Gaspari, A.A.; Lotze, M.T.; Rosenberg, S.A.; Stern, J.B.; Katz, S.I. Dermatologic changes associated with interleukin-2 administration. JAMA 1987, 258, 1624–1629. [Google Scholar] [CrossRef]
- Ferrucci, S.; Casazza, G.; Angileri, L.; Tavecchio, S.; Germiniasi, F.; Berti, E.; Marzano, A.V.; Genovese, G. Clinical response and quality of life in patients with severe atopic dermatitis treated with dupilumab: A single-center real-life experience. J. Clin. Med. 2020, 9, 791. [Google Scholar] [CrossRef] [Green Version]
- Moniaga, C.S.; Tominaga, M.; Takamori, K. Mechanisms and Management of Itch in Dry Skin. Acta Derm. Venereol. 2020, 100, adv00024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thijs, J.; van Seggelen, W.; Bruijnzeel-Koomen, C.; de Bruin-Weller, M.; Hijnen, D. New developments in biomarkers for atopic dermatitis. J. Clin. Med. 2015, 4, 479–487. [Google Scholar] [CrossRef]
- Francisco, V.; Pino, J.; Gonzalez-Gay, M.A.; Mera, A.; Lago, F.; Gómez, R.; Mobasheri, A.; Gualillo, O. Adipokines and inflammation: Is it a question of weight? Br. J. Pharmacol. 2018, 175, 1569–1579. [Google Scholar] [CrossRef]
- Ali, Z.; Suppli Ulrik, C.; Agner, T.; Thomsen, S.F. Is atopic dermatitis associated with obesity? A systematic review of observational studies. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1246–1255. [Google Scholar] [CrossRef]
- Granata, M.; Skarmoutsou, E.; Trovato, C.; Rossi, G.A.; Mazzarino, M.C.; D’Amico, F. Obesity, type 1 diabetes, and psoriasis: An autoimmune triple flip. Pathobiology 2017, 84, 71–79. [Google Scholar] [CrossRef]
- Banihani, S.A.; Elmadhoun, R.A.; Khabour, O.F.; Alzoubi, K.H. The rs2167270 polymorphism of leptin gene is associated with atopic dermatitis. Dermatoendocrinology 2018, 10, e1454191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimata, H. Elevated serum leptin in AEDS. Allergy 2002, 57, 179–184. [Google Scholar] [CrossRef]
- Nagel, G.; Koenig, W.; Rapp, K.; Wabitsch, M.; Zoellner, I.; Weiland, S.K. Associations of adipokines with asthma, rhinoconjunctivitis, and eczema in German schoolchildren. Pediatr. Allergy Immunol. 2009, 20, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Wu, W.H.; Bae, J.M.; Son, S.-J.; Lee, J.H.; Han, T.Y. Serum leptin and adiponectin levels in atopic dermatitis (AD) and their relation to disease severity. J. Am. Acad. Dermatol. 2016, 75, 629–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Dermatol. Venerol. 1980, 92, 44–47. [Google Scholar]
- Oranje, A.P.; Glazenburg, E.J.; Wolkerstorfer, A.; de Waard-van der Spek, F.B. Practical issues on interpretation of scoring atopic dermatitis: The SCORAD index, objective SCORAD and the three-item severity score. Br. J. Dermatol. 2007, 157, 645–648. [Google Scholar] [CrossRef]
- Schoch, D.; Sommer, R.; Augustin, M.; Ständer, S.; Blome, C. Patient-reported outcome measures in pruritus: A systematic review of measurement properties. J. Investig. Dermatol. 2017, 137, 2069–2077. [Google Scholar] [CrossRef] [Green Version]
- Ständer, S.; Augustin, M.; Reich, A.; Blome, C.; Ebata, T.; Phan, N.Q.; Szpietowski, J.C. Pruritus assessment in clinical trials: Consensus recommendations from the International Forum for the Study of Itch (IFSI) Special Interest Group Scoring Itch in Clinical Trials. Acta Derm. Venereol. 2013, 93, 509–514. [Google Scholar] [CrossRef]
- Patino, C.M.; Ferreira, J.C. Test for trend: Evaluating dose-response effects in association studies. J. Bras. Pneumol. 2016, 42, 240. [Google Scholar] [CrossRef] [Green Version]
- Fang, H.; Judd, R.L. Adiponectin regulation and function. Compr. Physiol. 2018, 8, 1031–1063. [Google Scholar] [PubMed]
- Jung, Y.R.; Lee, J.-H.; Sohn, K.-C.; Lee, Y.; Seo, Y.-J.; Kim, C.-D.; Lee, J.-H.; Hong, S.-P.; Seo, S.-J.; Kim, S.-J.; et al. Adiponectin signaling regulates lipid production in human sebocytes. PLoS ONE 2017, 12, e0169824. [Google Scholar] [CrossRef] [PubMed]
- Kyriakou, A.; Patsatsi, A.; Sotiriadis, D.; Goulis, D.G. Serum leptin, resistin, and adiponectin concentrations in psoriasis: A meta-analysis of observational studies. Dermatology 2017, 233, 378–389. [Google Scholar] [CrossRef] [PubMed]
- Mostafazadeh, M.; Haiaty, S.; Rastqar, A.; Keshvari, M. Correlation between resistin level and metabolic syndrome component: A review. Horm. Metab. Res. 2018, 50, 521–536. [Google Scholar] [CrossRef]
- Curat, C.A.; Wegner, V.; Sengens, C.; Miranville, A.; Tonus, C.; Busse, R.; Bouloumié, A. Macrophages in human visceral adipose tissue: Increased accumulation in obesity and source of resistin and visfatin. Diabetologia 2006, 49, 744–747. [Google Scholar] [CrossRef]
- Pine, G.M.; Batugedara, H.M.; Nair, M.G. Here, there and everywhere: Resistin-like molecules in infection, inflammation, and metabolic disorders. Cytokine 2018, 110, 442–451. [Google Scholar] [CrossRef] [Green Version]
- Lehrke, M.; Reiley, M.P.; Millington, C.S.; Iqbal, N.; Rader, D.J.; Lazar, M.A. An inflammatory cascade leading to hyperresitinemia in humans. PLoS Med. 2004, 1, e45. [Google Scholar] [CrossRef]
- Hsu, W.Y.; Chao, Y.W.; Tsai, Y.L.; Lien, C.C.; Chang, C.F.; Deng, M.C.; Ho, L.T.; Kwok, C.F.; Juan, C.C. Resistin induces monocyte-endothelial cell adhesion by increasing ICAM-1 and VCAM-1 expression in endothelial cells via p38MAPK-dependent pathway. Cell. Physiol. 2011, 226, 2181–2188. [Google Scholar] [CrossRef]
- Tripathi, D.; Kant, S.; Pandey, S.; Ehtesham, N.Z. Resistin in metabolism, inflammation, and disease. FEBS J. 2020. [Google Scholar] [CrossRef]
- Machura, E.; Szczepanska, M.; Ziora, K.; Ziora, D.; Swietochowska, E.; Barc-Czarnecka, M.; Kasperska-Zajac, A. Evaluation of adipokines: Apelin, visfatin, and resistin in children with atopic dermatitis. Mediat. Inflamm. 2013. [Google Scholar] [CrossRef] [PubMed]
- Banihani, S.A.; Abu-Alia, K.F.; Khabour, O.F.; Alzoubi, K.H. Association between resistin gene polymorphisms and atopic dermatitis. Biomolecules 2018, 8, 17. [Google Scholar] [CrossRef] [Green Version]
- Farag, A.G.A.; Hammam, M.A.; Khaled, H.N.; Soliman, S.; Tayel, N.R.; El-Shamendy, A.A.; Shehata, W.A. Resistin adipokine in atopic dermatitis patients: A clinical, biochemical, and genetic study. J. Cosmet. Dermatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Proenca, R.; Maffei, M.; Barone, M.; Leopold, L.; Friedman, J.M. Positional cloning of the mouse obese gene and its human homologue. Nature 1994, 372, 425–432. [Google Scholar] [CrossRef]
- Hu, Y.; Zhu, Y.; Lian, N.; Chen, M.; Bartke, A.; Yuan, R. Metabolic syndrome and skin diseases. Front. Endocrinol. 2019, 10, 788. [Google Scholar] [CrossRef]
- Poeggeler, B.; Schulz, C.; Pappolla, M.A.; Bodo, E.; Tiede, S.; Lehnert, H.; Paus, R. Leptin and the skin: A new frontier. Exp. Dermatol. 2010, 19, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Martin-Romero, C.; Santos-Alvarez, J.; Goberna, R.; Sanchez-Margalet, V. Human leptin enhances activation and proliferation of human circulating T lymphocytes. Cell. Immunol. 2000, 199, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Lord, G.M.; Matarese, G.; Howard, J.K.; Baker, R.J.; Bloom, S.R.; Lechler, R.I. Leptin modulates the T-cell immune response and reverses starvation-induced immunosuppression. Nature 1998, 394, 897–901. [Google Scholar] [CrossRef]
- Zheng, H.; Wu, D.; Wu, X.; Zhang, X.; Zhou, Q.; Luo, Y.; Yang, X.; Chock, C.J.; Liu, M.; Yang, X.O. Leptin promotes allergic airway inflammation through targeting the unfolded protein response pathway. Sci. Rep. 2018, 8, 8905. [Google Scholar] [CrossRef] [PubMed]
- Balato, N.; Nino, M.; Patruno, C.; Matarese, G.; Ayalam, F. ‘Eczemas’ and leptin. Dermatitis 2011, 22, 320–323. [Google Scholar] [PubMed]
- Bostanci, I.; Atli, O.; Celebi, N.; Tasar, A.; Alpkarakoc, E.; Dallar, Y. Serum leptin level in children with atopic dermatitis-treated topical steroids. Pediatr. Allergy Immunol. 2004, 15, 267–269. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Yan Sun, W.; Fu, B.; Xu, A.; Wang, Y. Lipocalin-2-the myth of its expression and function. Basic Clin. Pharmacol. Toxicol. 2020. [Google Scholar] [CrossRef] [Green Version]
- Schroll, A.; Eller, K.; Feistritzer, C.; Nairz, M.; Sonnweber, T.; Moser, P.A.; Rosenkranz, A.R.; Theurl, I.; Weiss, G. Lipocalin-2 ameliorates granulocyte functionality. Eur. J. Immunol. 2012, 42, 3346–3357. [Google Scholar] [CrossRef] [PubMed]
- Kamata, M.; Tada, Y.; Tatsuta, A.; Kawashima, T.; Shibata, S.; Mitsui, H.; Asano, Y.; Sugaya, M.; Kadono, T.; Kanda, N.; et al. Serum lipocalin-2 levels are increased in patients with psoriasis. Clin. Exp. Dermatol. 2012, 37, 296–299. [Google Scholar] [CrossRef] [PubMed]
- Shiratori-Hayashi, M.; Koga, K.; Tozaki-Saitoh, H.; Kohro, Y.; Toyonaga, H.; Yamaguchi, C.; Hasegawa, A.; Nakahara, T.; Hachisuka, J.; Akira, S.; et al. STAT3-dependent reactive astrogliosis in the spinal dorsal horn underlies chronic itch. Nat. Med. 2015, 21, 927–931. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, N.; Ishiuji, Y.; Tominaga, M.; Sakata, S.; Takahashi, N.; Yanaba, K.; Umezawa, Y.; Asahina, A.; Kimura, U.; Suga, Y.; et al. Relationship between the degrees of itch and serum lipocalin-2 levels in patients with psoriasis. J. Immunol. Res. 2019. [Google Scholar] [CrossRef] [PubMed]
- Dai, R.; Dong, Z.; Qian, Y.; Han, Y. Obese type 2 diabetes mellitus patients have higher serum vaspin concentrations. Diabetes 2016, 8, 445–447. [Google Scholar] [CrossRef]
- Ziegler, K.; Weiner, J.; Krause, K.; Schwarz, M.; Kohn, M.; Stumvoll, M.; Bluher, M.; Heiker, J.T. Vaspin suppressed cytokine-induce inflammation in 3T3-L1 adipocytes via inhibition of NF-ĸB pathway. Mol. Cell. Endocrinol. 2018, 460, 181–188. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Dong, Y.; Wang, T.; Zhao, S.; Yang, K.; Chen, X.; Zheng, C. Vaspin inhibited pro-inflammatory cytokine-induced activation of nuclear factor-kappa B and its downstream molecules in human endothelial E.A.hy926 cells. Diabetes Res. Clin. Pract. 2014, 103, 482–488. [Google Scholar] [CrossRef]
- Yin, C.; Hu, W.; Wang, M.; Xiao, Y. The role of the adipocytokines vaspin and visfatin in vascular endothelial function and insulin resistance in obese children. BMC Endocr. Disord. 2019, 19, 127. [Google Scholar] [CrossRef]
- Saalbach, A.; Tremel, J.; Herbert, D.; Schwede, K.; Wandel, E.; Schirmer, C.; Anderegg, U.; Beck-Sickinger, A.G.; Heiker, J.T.; Schultz, S.; et al. Antiinflammatory action of keratinocyte-derived vaspin: Relevance for the pathogenesis of psoriasis. Am. J. Pathol. 2016, 186, 639–651. [Google Scholar] [CrossRef] [Green Version]
- Weiner, J.; Zieger, K.; Pippel, J.; Heiker, J.T. Molecular mechanisms of vaspin action—From adipose tissue to skin and bone, from blood vessels to the brain. Adv. Exp. Med. Biol. 2018, 1111, 159–188. [Google Scholar]
- Saalbach, A.; Vester, K.; Rall, K.; Tremel, J.; Anderegg, U.; Beck-Sickinger, A.G.; Blüher, M.; Simon, J.C. Vaspin—A link of obesity and psoriasis? Exp. Dermatol. 2012, 21, 309–312. [Google Scholar] [CrossRef] [PubMed]
- Carpaij, O.A.; van den Berge, M. The asthma-obesity relationship: Underlying mechanisms and treatment implications. Curr. Opin. Pulm. Med. 2018, 24, 42–49. [Google Scholar] [CrossRef]
- Ali, Z.; Ulrik, S.C.; Agner, T.; Thomsen, S.F. Association between atopic dermatitis and the metabolic syndrome: A systemic review. Dermatology 2018, 234, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Greenland, P. Eczema and cardiovascular risk factors in 2 US adult population studies. J. Allergy Clin. Immunol. 2015, 135, 721–728. [Google Scholar] [CrossRef]
- Sybilski, A.J.; Raciborski, F.; Lipiec, A.; Tomaszewska, A.; Lusawa, A.; Furmańczyk, K.; Fałta-Krzych, E.; Komorowski, J.; Samoliński, B. Obesity—A risk factor for asthma, but not for atopic dermatitis, allergic rhinitis and sensitization. Public Health Nutr. 2015, 18, 530–536. [Google Scholar] [CrossRef]
- Rönmark, E.P.; Ekerljung, L.; Mincheva, R.; Sjölander, S.; Hagstad, S.; Wennergren, G.; Rönmark, E.; Lötvall, J.; Lundbäck, B. Different risk factor patterns for adult asthma, rhinitis and eczema: Results from West Sweden Asthma Study. Clin. Transl. Allergy 2016, 6, 28. [Google Scholar] [CrossRef] [Green Version]
- Fujii, M. Current understanding of pathophysiological mechanisms of atopic dermatitis: Interactions among skin barrier dysfunction, immune abnormalities and pruritus. Biol. Pharm. Bull. 2020, 43, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Bieber, T.; D’Emme, A.M.; Akdis, C.A.; Traidl-Hoffmann, C.; Lauener, R.; Schappi, G.; Schmid-Grendelmeier, P. Clinical phenotypes and endotypes of atopic dermatitis: Where are we, and where should we go. J. Allergy Clin. Immunol. 2017, 139, S58–S64. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Atopic Dermatitis | Healthy Controls | ||
|---|---|---|---|
| Mild Eczema (n = 19) | Severe Eczema (n = 30) | No Eczema (n = 30) | |
| Sex: M/F, n (%) | 3 (15.7)/16 (84.3) | 14 (46.6)/16 (53.4) | 15 (50)/15 (50) |
| Age: median (min–max) (years) | 28 (22–60) | 41 (20–75) | 42 (22–78) |
| SCORAD: median (min–max) (points) | 16.7 (10.6–20.7) | 62.2 (50.2–80.4) | 0.0 |
| VAS: median (min–max) (points) | 5 (3–8) | 9 (8–10) | 0.0 |
| BMI: median (min–max) (kg/m2) | 21.3 (18.5–23.4) | 21.7 (18.3–28.6) | 21.0 (18.9–28.7) |
| tIgE: median (min–max) (IU/mL) | 403 (105–2300) | 7670 (813–58,300) | 0.0 |
| Atopic Dermatitis (n = 49) | Controls (n = 30) | p | |
|---|---|---|---|
| Median (Min–Max) | Median (Min–Max) | ||
| Adiponectin (µg/mL) | 8.94 (2.3–17.1) | 11.2 (4.0–17.4) | 0.020 |
| Resistin (ng/mL) | 10.9 (9.7–18.4) | 16.4 (11.7–23.9) | <0.001 |
| Lipocalin-2 (ng/mL) | 83.0 (55.6–147.6) | 96.7 (52.6–178.3) | 0.540 |
| Leptin (ng/mL) | 9.6 (1.9–76.3) | 5.19 (0.9–188.8) | 0.020 |
| Vaspin (pg/mL) | 224.3 (93.5–891.7) | 267.1 (108.2–708.7) | 0.540 |
| Resistin | Lipocalin-2 | Leptin | Vaspin | |
|---|---|---|---|---|
| Adiponectin | −0.21 | −0.18 | −0.06 | −0.02 |
| Resistin | 1.00 | 0.37 * | −0.05 | 0.02 |
| Lipocalin-2 | 1.00 | 0.02 | 0.28 | |
| Leptin | 1.00 | −0.01 | ||
| Vaspin | 1.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaworek, A.K.; Szepietowski, J.C.; Szafraniec, K.; Jaworek, M.; Hałubiec, P.; Wojas-Pelc, A.; Pokorski, M. Adipokines as Biomarkers of Atopic Dermatitis in Adults. J. Clin. Med. 2020, 9, 2858. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092858
Jaworek AK, Szepietowski JC, Szafraniec K, Jaworek M, Hałubiec P, Wojas-Pelc A, Pokorski M. Adipokines as Biomarkers of Atopic Dermatitis in Adults. Journal of Clinical Medicine. 2020; 9(9):2858. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092858
Chicago/Turabian StyleJaworek, Andrzej Kazimierz, Jacek C. Szepietowski, Krystyna Szafraniec, Magdalena Jaworek, Przemysław Hałubiec, Anna Wojas-Pelc, and Mieczysław Pokorski. 2020. "Adipokines as Biomarkers of Atopic Dermatitis in Adults" Journal of Clinical Medicine 9, no. 9: 2858. https://0-doi-org.brum.beds.ac.uk/10.3390/jcm9092858