
What Does Joy in Living Mean to Elderly Residents of Nursing Homes in Singapore?



S R Nathan School of Human Development, Singapore University of Social Sciences, Singapore 599494, Singapore
*
Author to whom correspondence should be addressed.
Religions 2022, 13(5), 469; https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050469
Submission received: 25 March 2022
/
Revised: 6 May 2022
/
Accepted: 17 May 2022
/
Published: 23 May 2022
(This article belongs to the Special Issue Spirituality and Aging: Finding Meaning in the Context of Personal and Societal Change)
Abstract
:The rapid ageing of Singapore’s population has led to the phenomenon of more elderly spending more total years in nursing homes. This study aimed to explore the meaning of Joy in Living to elderly residents of nursing homes in Singapore, the enabling and disenabling conditions to Joy in Living in nursing homes and how Person-centered Care can support Joy in Living in nursing homes. The concept of Joy in Living is used in this study as it is unique to an individual elderly’s experience; The study employed hermeneutical phenomenological research methodology to allow for the exploration of Joy in Living in lived experiences of elderly residents through in-depth sixteen semi-structured interviews with elderly residents and six participant observations of three nursing homes (pre and post interviews) between July 2021 and November 2021; Seven themes for Joy in Living experiences to flourish were identified, including “supportive nursing home environment and practices”, “connectedness through meaningful relationships”, “meaningful daily living”, “fulfil the need for spiritual care”, “personal control”, “desire to be free from worries”, and “adapting to changes”, each of which explains a facet of Joy in Living experiences of the elderly residing in nursing homes. These themes include the enabling and disenabling conditions to Joy in Living in nursing homes; Focusing efforts and resources on enabling the seven themes, including fulfilling the need for spiritual care will allow Joy in Living experiences of elderly to flourish in nursing homes. This in turn promotes better psychosocial well-being of the elderly and better living environments where nursing home residents may enjoy satisfactory accommodation while spending their remaining years in joy.
1. Introduction
Medical advancement and higher living standards have led to increased average life spans. These, coupled with decreasing fertility rates, have translated into an ageing population worldwide and in Singapore. In 2021, 16.03% of Singapore’s total resident population (citizens and permanent residents) were aged 65 years and above: the elderly population growth increased by 7.23 per cent from 8.80% in 2009 (Department of Statistics Singapore 2021). It is projected that in 2030, 1 in 4 Singaporeans will be aged 65 years and above (Hirschmann 2020).
The expected burden that an ageing population places on public health care expenditure in the Intermediate and Long-Term Care Sector (ILTC) is exacerbated by rising chronic diseases in the elderly (Goh et al. 2015). Several initiatives are in place to mitigate this and enable older people to “age-in-place” and within the community. However, the rush to ramp up capacity might not have placed the elderly resident at the heart of the design and delivery of nursing home services. Basu (2016) stated that the elderly residents are cramped in the living quarters. Singaporeans’ perception of nursing home services is poor. A qualitative study was conducted in 2015 among people aged 50 years and above on perceptions and attitudes regarding ILTC. It entailed one-on-one interviews with care recipients and their primary caregivers using various eldercare services available in Singapore, including nursing home services (Wee et al. 2015). Based on 30% of the interviews, the study found a poor perception of nursing homes existed, namely nursing homes “neglect patients and restrict freedom cut across the responses of both users and nonusers of nursing homes, and their caregivers” (Wee et al. 2015, p. 223). People mostly opted for nursing homes only when caregivers were unavailable for the task.
Since 2016, the quality of care at nursing homes has improved by leaps and bounds due to several initiatives by government agencies, Agency for Integrated Care and the Ministry of Health: for example, the Licensing Terms and Conditions on Enhanced Nursing Home Standards under the Private Hospitals and Medical Clinics Act.
A review of gerontological literature shows a gap in studies that focus on the joy experienced by elderly residents of nursing homes. Notwithstanding this, key findings overwhelmingly point to the positive impact of holistic care models such as Person-centered Care (Rogers 1961), variations of person-centered care like Person-directed Care (White et al. 2008), Eden Alternative Model (Thomas 2003), and the Biopsychosocial Model of Health and Illness (Engel 1977), on the well-being of elderly in nursing homes. The care models are “measured”/assessed on their impact on quality of care, quality of life, well-being, elderly satisfaction with services, staff satisfaction working in nursing homes, with some reference to concepts of happiness and good life, but little attention paid to the joy experienced by care recipients. Wang et al. (2016, p. 1) has defined quality of life as a “multi-dimensional construct with objective and subjective constructs, although the latter is often given greater priority”. An example of an objective construct is a functional status that can be measured using assessment instruments like the Barthel scale. According to Chaturvedi and Muliyala (2016), there is no consensus on a common definition for the subjective construct of quality of life which includes but is not limited to autonomy, enjoyment, employment and income, family relationships, meaningful endeavors, spiritual well-being, and social support. Well-being, compared to the quality of life, looks only at subjective attributes and has been measured by “happiness” i.e., emotional reaction and “satisfaction” i.e., cognitive evaluation of life, in studies on well-being (Gray et al. 2008). According to Rinnan et al. (2018, p. 1469), “Well-being corresponds to processes where people perceive a good life based on their own merits and might be described as comprising joy, enjoyment, fulfilment, pleasure, satisfaction, happiness, involving elements as relationships with family and a sense of community”.
Is a good life possible in old age? Do we have to bid farewell to positive emotions of happiness as we transit to old age? In a Stanford study by Carstensen et al. (2011, p. 21), the researchers used “experience-sampling to examine the developmental course of emotional experience in a representative sample of adults spanning early to very late adulthood” for a one-week period that was carried out again five and then ten years later. During the one-week period, participants were issued pagers and they were required to respond to questions immediately when they were paged. The questions were on how happy, satisfied, and comfortable they were. A key study finding is an improvement in emotional experience from early adulthood into old age, which is congruent with the Selection, Optimization, Compensation (SOC) model of adult development (Baltes and Baltes 1990). The dynamic SOC model is a theory of successful ageing that views ageing through a life course perspective of developmental change from early adulthood to old age. The elderly can be contented and lead good lives by being “selective” in investing time and resources in goals and tapping on their expertise to “optimize” performance in selected areas to “compensate” for losses or limitations brought upon by the ageing process. Studies on ageing invariably touch on life course perspective which allows for analysis of people’s lives within structural, social, cultural, and historical contexts across the four stages of the life course: childhood, adolescence, adulthood, and old age (Giele and Elder 1998).
Two qualitative studies have been conducted in the UK and one in Australia to examine the Good Life concept of seniors residing in care facilities (Bowers et al. 2009; Katz et al. 2011; Minney and Ranzijn 2016). Minney and Ranzijn (2016, p. 919) defined Good Life as it “encompasses both the value of one’s life and well-being in general”.
What about Joy then? Joy comes from things with more intrinsic value (e.g., a belief that one has a purpose in life) and being happy despite losses like loss of physical functioning that results in poor health, loss of income from retirement, and even loss of a loved one. For the elderly, the integrative process is important for inner contentment, harmony, and Joy based on one’s values, purpose, or meaning in life and religious beliefs (Tornstam 1997). As individuals enter old age, they frequently ask existential questions due to the impending reality of death. In this respect, Joy can be interpreted as a step beyond Good Life.
A qualitative study has been conducted on what constitutes the essence of Joy of Life for elderly residents of Norwegian nursing homes (Rinnan et al. 2018). In that study, the researchers used the concept of Joy of Life, a multi-dimensional construct, “which seems more closely related to subjective well-being commonly defined in social science as the absence of negative emotions, the presence of positive emotions and life satisfaction, all of which corresponding to the concept of flourishing” (Rinnan et al. 2018, p. 1469).
Inspired by these studies in other countries and findings of local quantitative studies on nursing homes that psychosocial well-being is not being addressed, the authors have modified and narrowed down on a concept that they think is relevant to Singapore’s context. The concept of Joy in Living is used instead of Joy of Life in the study as the study has a strong applied focus and, in the authors’ perspective, a concept that is “dynamic” and operationalized in concrete terms would be easier for the residents in Singapore nursing homes to understand. Hence, they have coined the concept of Joy in Living which is rooted in the present and has dimensions of physical, psychosocial well-being, and spirituality. By studying this concept, the authors hope that it can be incorporated as an additional dimension into holistic approaches of care in Singapore nursing homes.
There are no hypotheses for this study, instead there are four research questions to guide the study as follows:
- (i)
- What does Joy in Living mean to elderly residents of nursing homes in Singapore?
- (ii)
- What are the enabling conditions that are conducive for Joy in Living in nursing homes?
- (iii)
- What are the disenabling conditions that are not conducive for Joy in Living in nursing homes?
- (iv)
- How does Person-centered Care support Joy in Living in nursing homes?
2. Materials and Methods
2.1. Design
The hermeneutical phenomenological research methodology is used for the study that depends heavily on research participants—the elderly in nursing homes—recalling their lived experiences in those homes and reflecting critically on the meaning they ascribe to Joy in Living (Leedy and Ormrod 2001). The researcher conducting this study is part of the study to interpret and identify the essences of each lived experience, the meaning ascribed to Joy in Living, and find the language to convey the essences of the data collected and analyzed. There are six research activities that provide the methodological structure of phenomenological research studies (van Manen 1990).
This qualitative study was conducted between July 2021 and Nov 2021. This study is a part of an ongoing PhD study involving 25 to 30 elderly participants and observations of five nursing homes.
2.2. Participants
A total of 16 elderly participants were selected from three nursing homes; one home with greater than 300 beds but less than 500 beds and the other two homes with more than 100 beds but less than 300 beds.
Inclusion criteria were participants being 65 years and above of age, residing in the nursing home for at least one year, a Singapore citizen or permanent resident in Singapore, ability to understand and speak in basic English. Bed-bound and residents with dementia, as assessed by the nursing home were excluded.
2.3. Data Collection
The data collection methods in this study are in-depth individual face-to-face interviews with elderly research participants using semi-structured interview guide and running records of onsite observations as a participant observer. The concept of Joy in Living was introduced to the participants at the start of the interview and in the Participant Information Sheet given to all participants. The following topics were covered in the interview:
- (i)
- Participants’ background and why they are in a nursing home;
- (ii)
- Participants’ day-to-day living experience in the nursing home;
- (iii)
- Participants’ religious/spiritual beliefs, their belief system and purpose in life;
- (iv)
- Participants’ understanding of Joy in Living, their views whether Joy in Living is possible in a nursing home and why if their answer is either yes or no;
- (v)
- If participants are living a joyful life in the nursing home, what are the things contributing to it and vice versa.
Six onsite participant observations were conducted at the three nursing homes, two observation sessions pre and post interview at each nursing home. Each observation session was eight hours that was either conducted over one day with an hour’s break in between the am and pm sessions or half days over two days.
There was an interruption to data collection through face-to-face interviews and onsite observations for about two months from mid-September 2021 to mid-November 2021 due to development of COVID-19 clusters in a few nursing homes in Singapore and the national policy response to suspend in-person visits to nursing homes. To allow for operational flexibility given the evolving COVID-19 situation and emergence of “Omicron” new COVID-19 variant detected in December 21, interviews were conducted over “Zoom” online platform with video function from middle of September 2021 onwards.
2.4. Data Analysis
Data analysis was conducted after collection of data from each nursing home, where Joy in Living was used as the analytical concept for the analysis of the data to identify “significant statements” and “clusters of meaning” about Joy in Living from the transcripts of interview and observation audio records. The thematic statements chosen were those phrases that seemed to particularly allude to the Joy in Living experiences (van Manen 1990).
In hermeneutical phenomenological studies, van Manen (1990) offered three methods: (i) wholistic approach; (ii) a selective approach; and (iii) the detailed or line-by-line approach for identifying themes during data analysis. These approaches can be used to discover themes or facets of a pattern of the phenomenon across datasets. As the wholistic and selective methods do not detail out the step-by-step process to conduct data analysis, the first author applied the phases of Reflexive Thematic Analysis (Braun and Clarke 2006, 2021) to guide the process.
Reflexive thematic analysis (RTA) is compatible with hermeneutical phenomenological studies as it is “about the researcher’s reflective and thoughtful engagement with their data and their reflexive and thoughtful engagement with the analytic process”, and the first author has conceptualized themes “as patterns of shared meaning underpinned or united by a core concept (we later conceptualized this as a ‘central organizing concept’…” (Braun and Clarke 2019, pp. 593–94). Before commencement of data analysis, the transcripts were read several times to aid recall and familiarity with the content by immersing in the data. During data analysis, NVivo-Windows January 2022 Release 1.6 (NVivo) software was used. The latest version of NVivo supersedes NVivo 12 and does not have a version number assigned to it. NVivo was used to document the “significant statements” as “codes”, i.e., a short phrase to describe what is said in the elderly interview and the observation transcripts, gather all the quotes that were carefully tagged to the codes, and identify “clusters of meaning” as higher-order conceptual “themes” to answer the research questions (Braun and Clarke 2006; Creswell 2007; van Manen 1990). NVivo was used to handle and analyze the different types of data from the research study, e.g., field notes, transcripts of the interview, and the observation audio recordings and photographs of objects, environment, and activities with faces of people obscured. The hierarchy chart in Figure 1 shows the frequency of reference to the themes, subthemes, and codes in the transcripts of the interview and the observation audio recordings in the NVivo software.
To strengthen research rigor, the interview and observation guides were piloted in a nursing home that was not included in the study, and data were collected and analyzed through methodological triangulation. In the pilot study, where the elderly participant required clarification, prompts were added to the interview questionnaire (e.g., prompts were added to the questions on belief system and purpose of life).
3. Results
The profile of the sixteen participants is as detailed in Table 1.
Seven themes emerged as important for Joy in Living experiences of elderly to flourish in nursing homes: (i) “supportive nursing home environment and practices” that includes adopting person-centered care, (ii) “connectedness through meaningful relationships”, (iii) “meaningful daily living”, (iv) “fulfil the need for spiritual care”, (v) “personal control”, (vi) “desire to be free from worries”, and (vii) “adapting to changes”. These themes include the enabling and disenabling conditions to Joy in Living in nursing homes and, are the common essences of participants lived experience in a nursing home, as narrated by them through reflection of their day-to-day personal experiences (Cohen et al. 2000). These themes, when enabled, promote Joy in Living experiences of the elderly residing in nursing homes as illustrated in Figure 2. The themes and sub-themes are elaborated in Table A1 in Appendix A.
The subthemes within each theme are as illustrated in the concept map in Figure 3.
3.1. Supportive Nursing Home Environment and Practices
Supportive nursing home environment and practices which include adoption of Person-centered Care approaches such as Person-centered Care Model or its variations Person-directed Care or Eden Alternative Model, is the theme that provides the conducive ecosystem for Joy in Living experiences to flourish. There are several sub-themes in this “ecosystem” theme that include: (i) person-centered care; (ii) supportive living environment; (iii) safety and security; (iv) staff competency and capability; (v) food for residents; (vi) continual improvement efforts; (vii) leadership competency; and (viii) clear communications. As this theme has sub-themes that cover distinct aspects of supportive nursing home environment and practices, an elaboration of the sub-themes will be provided for just this theme.
As evident from Figure 1 on the coding references in the hierarchy chart done in NVivo-Windows, this theme has the most coding references. All participants reported the importance of at least one of the sub-themes in providing the conducive “ecosystem” for Joy in Living experiences to flourish. This was also corroborated by observation data.
3.1.1. Person-Centered Care
The psychosocial dimensions of Person-centered Care are covered in subsequent elaboration of themes: “connectedness through meaningful relationships” and “meaningful daily living”. This section covers personalized nursing care for residents. Personalized nursing care for residents was observed at all three nursing homes in areas such as grooming, serving medication and monitoring health, assisted feeding, and providing support at group activities and exercises. Engagement of residents by staff is patchy across the three nursing homes and appears to be dependent on personal qualities of staff involved and ability to communicate in vernacular languages; rather than a consistent practice across all staff interactions.
* xxx is talking to him, cajoling him to finish his meal. He smiles at her and takes a few more spoonful of porridge and the vegetables.(2nd Observation at Nursing Home B)
* To protect the identity of staff, name of staff is replaced with xxx
The Therapy Assistant is sitting next to her and stroking her hair. She speaks to the resident in a Chinese dialect. The Therapy Assistant, who is a local Chinese and a mature staff in either her late forties or fifties, smiles at me and says she is speaking to the resident in Teochew.(1st Observation at Nursing Home A)
A total of 13 out of the 16 participants, i.e., approximately 80% of the participants, reported having received personalized nursing care in the aforementioned areas. One resident mentioned how she felt assured of good care at the nursing home.
“Because I feel that I come here is suit for me. I got the thinking that somebody can look me until old”.(B1, Length of Stay: 3–5 years, Female, Chinese)
The other three residents opined that since they are not wheelchair bound, their nursing care needs are minimal: medication needs and health monitoring.
At an impromptu conversation with a resident during an observation session, a contradictory comment was noted.
“What Joy in Living! Lousy, lousy place. They don’t treat you very well. You want your diaper changed, so hard to get diaper. You lie down, lie down wait for diapers”.(Impromptu Conversation during 1st Observation at Nursing Home C)
3.1.2. Supportive Living Environment
A well-designed physical environment can ensure safety and independent living for the elderly residing in either the community or nursing homes, which in turn has a positive impact on their well-being. In designing living spaces in a nursing home, environmental aspects of supporting person-centered care delivery, conducting social and physical activities, and creating a home-like ambience must be considered. Lawton and Nahemow (1973) in their pioneering work on ecological model of ageing, emphasized the importance of having physical spaces that fit the needs of the occupants for optimal functioning. Several studies in the last two decades have also stressed the importance of accessibility of physical environment on seniors’ functioning (Iwarsson and Ståhl 2003; McCormack et al. 2011; Werngren-Elgström et al. 2009).
Four out of the sixteen participants, i.e., a quarter of the participants, mentioned the living environment as an aspect of the nursing home they liked. One of them decided to choose the nursing home based on her impression of the living environment and amenities when she visited it before deciding.
“…peaceful. I don’t how when I see the picture I know I want. My friend gave me the picture of the building. I went to other homes, but I cannot suit, then I see this I like. My sister also say better, this one also nice…They got proper place. All the sleeping place they have water, put water for drinking at hall”.(B1, Length of Stay: 3–5 years, Female, Chinese)
“I like the garden. Our canteen very, very noisy… in my heart is peaceful. I feel happy in my heart when I hear the water, birds and fish swimming… I also pray there, give me joy”.(C6, Length of Stay: 3–5 years, Male, Malay)
One resident reported his unhappiness with the living environment.
“This building is not properly maintained. It’s dirty. Look at all the fence, never clean. Compared to the old place, every week somebody will come clean all the fence”.(A4, Length of Stay: 1–2 years, Male, Chinese)
At the first author’s second observation session at Nursing Home A, she encountered rodent infestation problem in one of the bedrooms during an impromptu conversation with a resident in his six-bedder ward. She saw a rat trap kept at the foot of the cupboard. The cupboard was not in a good condition. Rat infestation is a safety concern too.
“This is not as bad as the rats… I got a lot of things, so they say you cannot put on the floor and all that, so they gave but they gave one that’s broken <they gave him a cupboard>. And rats used to go in what from the back. Now they say they fix it”.(A5, Length of Stay: >5 years, Male, Chinese; during an Impromptu Conversation at the 2nd Observation Session)
The first author also witnessed a hygiene issue with birds flying in at mealtimes and in the wards at two of the nursing homes. These nursing homes are nestled in open garden compounds that attract birds which could spread diseases through their droppings. Staff are vigilant to shoo the birds away and clean up food waste and spills promptly.
The rest did not have anything negative to report, however, four participants, i.e., a quarter of them, wished for the restricted confinement to their zones as part of temporary COVID-19 safe distancing measures to be over soon. The zoning has cut off their access to the full compound and amenities of the nursing home, as well as group activities with other residents from different zones.
“Yeah. It’s downstairs. There’s a fishpond and everything. Before we used to go down every day. We’ll go down, see the fish, then we all cannot…Now cannot because the COVID-19. We are not supposed to go down, leave our dormitories”.(C6, Length of Stay: 3–5 years, Male, Indian)
3.1.3. Safety and Security
Safety and security practices were mainly gathered at the observation sessions. Staff at all three nursing homes were observed to follow internal safety protocols when giving medication, watching over residents when doing group exercises or at mealtimes, feeding special diets and when transferring residents from bed to wheelchair/geriatric chair and vice versa. The first author observed that falls prevention is a key focus in all three nursing homes and there is an over-reliance on use of restrainers on elderly in beds, wheelchairs and geriatric chairs.
She asks the residents for their names, refers to a medical records ‘IMR’ folder with residents’ names and their laminated photographs, before giving the medicines. The medication trolley is a mobile cabinet with mini drawers. The mini drawers have names and photos of the residents. The medicines are in the mini drawers.(1st Observation at Nursing Home A)
A consistent practice in all my meal observations is having dedicated staff moving around and watching over residents who are eating on their own in both the living and dining rooms. Staff also go around with a pair of scissors to cut the vegetables and meat/fish to smaller pieces for those who ask for assistance or look like they are struggling with their meals.(2nd Observation at Nursing Home B)
Three participants reported having suffered falls at the nursing home which fortunately did not result in any bone fractures. Two participants reported falls of other residents: one resulting in the death of the resident.
“The other day one man died, he fell off the wheelchair and hit his head. This man, I predicted a long time ago. So, nurse ask me why you talk like that. I said if you look, he goes to the toilet 20 times. So, he’s putting himself in danger. You as nurses need to make sure he keeps safe; they don’t lock the wheelchair. I said I fall never mind, but when he falls and there’s nobody around. That’s the danger”.(A4, Length of Stay: 1–2 years, Male, Chinese)
3.1.4. Staff Competency and Capability
Thirteen out of 16 participants, i.e., approximately 80% of the participants reported both positive and negative experiences with different staffs. Negative experiences arose because staffs lacked the necessary knowledge, soft skills, and language barrier (for foreign staff) to carry out their duties effectively. This was further exacerbated by the workload of staff and/or inadequate staffing.
“Some nurses are very observant. Some, not so… I speak frankly, sometimes they are very busy and some of them, they don’t bother”.(A4, Length of Stay: 1–2 years, Male, Chinese)
“A few is very good. They really do the job, they very follow the procedure. Like from bed transfer to this, they really take care of you. Some they just stand down there, like for my case I used to use slide board and slide to my wheelchair. Some stand behind look at you. Anytime I can miss out and I fell down. They just stand down there. Some really good ‘lah’ <simplest and most common Singlish expression like ‘yeah mate’ in Australia> they take my two legs then I slide over very fast. One second. I think less than 20 seconds I go there already. Some they sit down there and slowly do. Some of the nurses they really use their hearts to work, some they just are not really nice”.(A3, Length of Stay: 1–2 years, Male, Chinese)
One of the participants shared his frustration about staff turnover. He misses staff who were good at doing the physiotherapy sessions for him as they are no longer with the nursing home. Another resident reported frequent changes to staff because of attrition.
“They got their problem about the work. How many people go out, already don’t work here”.(B1, Length of Stay: 3–5 years, Female, Chinese)
At observation sessions at two nursing homes, the researcher noticed that there are daily shift handover meetings to share updates with the care team taking over. At all three nursing homes, it was observed that staff follow internal protocols in serving meals, feeding, giving medication, transferring and schedule for changing adult diapers for residents. For e.g., only nursing aides and enrolled nurses feed pureed food to residents at risk of choking and do nasogastric tube feeding for bedbound residents. At one observation session at a nursing home, the first author noticed that staff do not intervene to diffuse tension when sporadic arguments break out among residents. The researcher engaged in an impromptu conversation with another resident who witnessed the incident.
“Some can, some they will leave them. Because ‘aiya’ <Singlish expression of displeasure or frustration>, I don’t want to say anything because it’s not good. Sometimes nurse and all got visitors, special visitors, if no visitors, then you can see shouting”.(Impromptu Conversation during 2nd Observation Session at Nursing Home C)
3.1.5. Food for Residents
There is much literature on nutrition for elderly in hospital and nursing home settings that focus on risks of malnutrition and reasons for reduced appetite in the elderly (Aryana and Kuswardhani 2018; Dorner et al. 2014; Marques et al. 2019; WHO 2022). There is however less literature and studies on association of food with memories in seniors. It is not unusual for an individual to consume food at a party and be transported back to a pleasant or unpleasant memory with that particular dish eaten in the past. An interesting neurological study on laboratory mice by Chinnakkaruppan et al. (2014) established a connection between the regions of the brains in charge of taste memory and remembering the time and location when the taste was experienced.
Coupled with this individualized preference and enjoyment of food, elderly from different ethnic communities have different palate shaped by their cultural heritage and unique dietary restrictions such as consuming only halal or vegetarian meals, or being vegetarian on certain days of the week. A few elderly might need to avoid certain food due to food allergies.
Six out of sixteen participants, i.e., slightly more than one-third of the participants, complained about either the quality of food or food served that does not meet their dietary preference.
“But I like meat, not fish. When I’m outside I always want some meat. When I’m here I got no choice”.(A2, Length of Stay: 1–2 years, Male, Chinese)
Every day the same thing, rice, veggie those type of fish, white colour but not white one then they put those kind of black sauce, ‘wah lao’ <Singlish expression to profess surprise or shock, like the expression ‘Oh my God!’> the taste, horrible.(A3, Length of Stay: 1–2 years, Male, Chinese)
The Chinese one cancelled already. Sometimes got babi <pork>, don’t want. Now, Malay food. Sometimes can, sometimes cannot. I mean, last time one, the Tuesday ah, the Muslim food, they give me chicken. I vegetarian Tuesday and Friday. Eat rice and vegetable only. Last time I like, one staff Indian cook ‘resam’ <a spicy Indian soup dish>, curry in kitchen give me. Missy <nurse> say cannot, my sugar, eat food they give, cannot special.(A1, Length of Stay: 3–5 years, Female, Indian)
Two participants complained about the quantity of food served. When the first author asked if they requested for a second helping, one participant reported being embarrassed to ask “Shame” and the other participant said that staff would be unhappy if she used the call bell unnecessarily to ask for additional serving of breakfast.
Three participants reported either they are “okay with the food” or “no complaints” with one of the participants sharing that besides being okay with the food, he is grateful to God for the food received. Two participants had no comments about the food served. Three participants reported the food is good and they like it.
3.1.6. Continual Improvement Efforts
All three nursing homes were observed to have adopted centralized services such as central kitchens to cook meals in-house and a central laundry service for all wards. Two nursing homes have adopted technologies such as an automated guided vehicle (i.e., an autonomous robot) for food delivery and the use of an automated steam machine to clean the floors of the dining hall. At an observation session at one of the nursing homes, the researcher observed an innovative programme “Mini Mart” for dementia residents at one of their residential living areas. The programme involves residents accumulating fake money for participation in exercise activities that can be used to deem snacks like potato chips and cup noodles on their “shopping trip” to a “mini mart”. The residents need to count the fake money and coins to pay the exact amount as indicated on the food items on display on the shelves in the “mini mart” room. The “mini mart” room is set up like a supermarket store.
3.1.7. Leadership Competency
Positive role modelling by leadership was observed at Nursing Home B and gathered from an impromptu conversation at an observation session at Nursing Home A.
At the briefing at the female ward, staff nurse informed the Chief Executive (CE) that there was a new resident who was a little unhappy and having adjustment problem. CE walks over to the ward to speak to the new resident. CE returns shortly after her chat with the new resident. Apparently, according to the home protocol, the resident needs to be isolated for 7 days before she can mingle with rest of the residents at the common areas. She is bored. CE asks staff to give her an iPad to let her watch whatever shows she wishes to watch. A staff quickly follows up on this.(1st Observation at Nursing Home B)
“I know about this one <referring to the vacancy at Nursing Home A> because of the certificate course that * xxx <CE> teach. The trainer is xxx <CE> herself…Yeah, she trains us hopefully we’ll join this company but not all will join ‘lah’”.(Impromptu Conversation at 2nd Observation at Nursing Home A)
* To protect the identity of CE, name of CE is replaced with xxx
Two residents expressed strong views that management is not providing the direction and leadership for the organization and staff.
“…the food, all you need to do is to get somebody to do quality control. You’re paying for the food…But if you don’t bother about it, they will just give you the same and this is exactly what is happening”.(A5, Length of Stay: >5 years, Male, Chinese)
“They’re doing this as they’re told to do…By the superior, then they treat all as equal <same treatment for dementia and non-dementia residents> which I don’t like.(C4, Length of Stay: 3–5 years, Male, Indian)
The study did not include interviews or FGDs with staff. However, during an impromptu conversation with a staff at an observation session, the staff alluded to a culture where staff is not encouraged to raise views and provide feedback for improvement.
Observer:
Have you given this feedback to the management?
Staff:
I’m not sure cos I just joined here. But I don’t like to highlight, this is not my portfolio I mean the <*xxx designation> is the lowest level here. Because we cannot understand that, we cannot do.(Impromptu Conversation at 2nd Observation at Nursing Home A)
* To protect the identity of staff and organisation, designation is replaced with xxx
3.1.8. Clear Communications
From the sharing of three participants at interviews and an impromptu conversation at an observation session, there seems to be miscommunication and misunderstanding of COVID-19 restrictions imposed on next of kin visits and certain nursing home policies.
Resident: How long, when can I see family? When allow from MOH side?
Observer: I think soon because it’s been too long already. The government intends to allow visits to hospitals and nursing homes from 21st Nov onwards. This is what is announced in the newspapers and TV news. The resident is relieved to hear this.(Impromptu Conversation during 2nd Observation at Nursing Home C)
“But here only your family can come. Outsider cannot cos they have to take your IC everything. Take your IC and see your name, father’s name, mostly they see your father’s name…we are not supposed to use phone <handphone> here”.(C6, Length of Stay: 3–5 years, Male, Indian)
3.2. Connectedness through Meaningful Relationships
Several studies on the well-being of seniors have stressed the importance of maintaining prior personal relationships and building new relationships for social inclusion (Bowers et al. 2009; Katz et al. 2011; Minney and Ranzijn 2016; Rinnan et al. 2018; Williamson 2010).
All sixteen participants stressed the importance of relationships with family and friends and/or forming new relationships with care staff and other residents to contributing to their Joy in Living experiences. This is in accordance with the Continuity Theory (Atchley 1989), that opportunities to maintain existing relationships for continuity of past roles allow for Joy in Living experiences to flourish.
“My two sons here, I would say they’re very good. This is why I’m blessed. I think among all the residents here, I’m the luckiest… I got a lot of things to talk to them. You know I see a lot of them when the children come, just leave the food and not spend time talking to them. “Okay Pa, then they go out.” So, it’s a very short visit. They just come with some food and all that. The impression I get is as if they come because they are obligated to. My son can sit here for hours… Because there’s so many things, I can talk with them”.(A5, Length of Stay: >5 years, Male, Chinese)
“My birthday. My lawyer <friend> will come. Every year he will buy a big cake for me and for the residents… Good friend in the case that I have my friends who bring me stuff. I give them a call”.(A4, Length of Stay: 1–2 years, Male, Chinese)
On the other hand, lack of opportunities to resolve issues pertaining to bequest and/or to mend broken relationships caused much anxiety and sorrow for the residents.
“Morning, morning I cry already. My house. The last one boy, he say, “I want my father house”, he say… My number 1 daughter, her husband say the house sell and then CPF take the money, they give you. You stay in home here… I mean, the boy he don’t like. He want house. I give house to him. I sell already, the boy where go? I stay ‘sini’ <here in Malay>, where the boy go, where?”.(A1, Length of stay: 3–5 years)
“That is what people say. What people do is different. Well, I don’t know why they think this way. I always look after the family. I’ve never been disloyal. When I go back to my home in Melbourne, I’m afraid I don’t know how to say why are you this way. I’ve done nothing wrong. You’ve done wrong with me… My family never contact me”.(A4, Length of Stay: 1–2 years, Male, Chinese)
There are challenges such as language barriers to developing new relationships with foreign care staff and other residents; especially for residents from ethnic minority groups in forming friendships with other residents.
“Friend, but they never talk. All Chinese. I don’t know Chinese. I speak Malay, English. I Eurasian”.(B5, Length of Stay: 3–5 years, Male, Eurasian)
“Here, you get to meet with them often and get to know them closely… But generally, it probably is a lot of them is from other countries like Myanmar that they can’t talk and understand English well <referring to foreign staff>”.(B4, Length of Stay: 1–2 years, Male, Chinese)
One resident shared her fears of being misunderstood and the fear of being a subject of gossip as a barrier to developing new relationships with care staff and other residents.
“Because sometimes you talk the words can become, cause problems with other resident, even staff, I don’t talk so much”.(B1, Length of Stay: 3–5 years, Female, Chinese)
Another resident shared his misconception that staffs are not supposed to strike conversations with residents. This could in part be colored by his incarceration experience in drug rehabilitation centers from young adulthood to middle age.
“Actually staff, they are not supposed to chit chat with us all. Cos this is a government place”.(C5, Length of Stay: 3–5 years, Male, Indian)
Seven out of 16 participants, i.e., slightly more than 40% of the participants highlighted other challenges to developing relationships with care staff which include staff showing displeasure at having to do tasks such as cleaning soiled diapers of elderly and/or heavy workload of staff to care for all residents.
“Their temperament is bad. Because other things, certain things you cannot complain. You ‘pangsai’ <pass motion> they want to wash you up, is very good. I think most of them are annoyed because of the washing up, they have to wash our backside or shower us, and they’re not happy with that… They talk among themselves and show their face”.(B3, Length of Stay: 3–5 years, Male, Chinese)
“I don’t want to trouble them, all busy. All okay ‘lah’ here. I just watch TV ‘lah’. They put me to sit facing the TV with Chinese shows. Chinese TV also watch”.(C6, Length of Stay: 3–5 years, Male, Malay)
“But most of them are quite busy… More I would say that nobody’s perfect. So, they have to be more relaxed to be able to talk to us, at the same time, it is a balance that they cannot be too relaxed and not get things done”.(B4, Length of Stay: 1–2 years, Male, Chinese)
Six out of 16 participants, i.e., slightly more than one-third of the participants reported being friends with care staff.
“Actually, the staff are quite good the staff. I mean quite good to the residents. They don’t shout around or bully them. They are very gentle to them and always attend to their requests. …Yeah, we get along quite well. I trust them. Nothing very personal…. Just the daily needs and all that. One or two only that are willing to buy for me. Close to me”.(C3, Length of Stay: 1–2 years, Male, Chinese)
At all three nursing homes, the first author observed that most staff were focused on completing tasks effectively and ensuring safety of residents, instead of chatting with them and building a relationship with them. While it was observed that several foreign staff in all three nursing homes can speak a few words of Mandarin and Malay to the residents, it was mainly to convey instructions to the residents and not to engage in conversations with them.
While the staff are courteous and patient, there is no interaction beyond the task of feeding them safely without choking…The interaction is mechanical. Although the staff uses a few words of Malay, it is mainly to ask what colours the resident wants from the colour pencil set.(2nd Observation at Nursing Home A)
3.3. Meaningful Daily Living
Studies on seniors have shown that participation in social and group recreational activities facilitates the development of new relationships, keeps them meaningfully engaged, and promotes physical and mental health (Gabriel and Bowling 2004; Katz et al. 2011; Minney and Ranzijn 2016; Rinnan et al. 2018). An overwhelming majority of the participants, 15 out of 16 participants, reported that there were very few meaningful activities in nursing homes other than the structured physical and occupational therapy exercises for residents. This was also corroborated by observation data.
“I do join the group exercise. It is good for my strength. I like the individual therapy better”.(A4, Length of Stay: 1–2 years, Male, Chinese)
“I go swimming you know. Here in the home”.(A1, Length of Stay: 3–5 years, Female, Indian)
The activities include stacking and rearranging cups, identifying matching items in 3-d game sets, completing jigsaw puzzles and colouring pre-printed drawings. One staff… walks around and supervises the residents…. For selected residents, he works on the range of motion of their upper limbs: the arm, forearm, and hands, while they are working on their assigned tasks.(1st Observation at Nursing Home C)
Many residents spend a lot of time either sleeping or watching TV programmes. Those who are literate in English and Mandarin have access to limited copies of newspapers in these two languages. Residents who are literate in Malay or Tamil do not have access to newspapers in their vernacular languages. One resident whose length of stay is 3–5 years in the nursing home spoke about not having his reading glasses with him as he left it in his home. The lack of meaningful social and recreational activities can cause loneliness and boredom.
“Now, down here, there is not much activity. And then we are sort of restricted living here… My closest thing is a newspaper and the television… Plan all these activities that I can participate, I find that it’s very interesting. Because I don’t like to be bored you see. Anything that I can do I like to do. I’m not particular”.(C3. Length of Stay: 1–2 years, Male, Chinese)
“Down here, cannot, nothing. By 5 o’clock I call it a day. I just lie down”.(A2, Length of Stay: 1–2 years, Male, Chinese)
There are activities organized in Mandarin for the ethnic majority residents who are Chinese. The first author observed a 1.5-h online Zoom singing session in Mandarin organized by church volunteers at Nursing Home A during a weekday afternoon observation session. At the interview with an ethnic minority resident from Nursing Home A, when the first author asked if there were such online volunteer activities on a frequent basis, she replied,
“Tamil don’t have”.(A1, Length of Stay: 3–5 years, Female, Indian)
Loneliness is worsened by the limited interactions between residents and their family members, friends and volunteers due to COVID-19 safety measures in place that restrict and at times disallow visits for extended periods of time when COVID-19 community cases surge.
“<Resident’s wish for volunteer visits to resume> Make me happy. Not lonely”.(C1, Length of Stay: >5 years, Male, Chinese)
Meaningful daily activities organized by nursing homes, that are coupled with time to pursue personal interest contribute to Joy in Living experiences of the elderly residents.
“Then the rest of the time I read, I got a lot of books there, and I play ‘Sudoku’. You will be surprised”.(A5, Length of Stay: >years, Male, Chinese)
“Because I came into this place, I study more and more <the bible>, I pray every day…cos now I stay in this home even if I don’t go out is a heaven to me”.(C5, Length of Stay: 3–5 years, Male, Indian)
Residents who have a sense of belonging to the nursing home and volunteer their services are meaningfully occupied and experience Joy in Living. A total of 2 out of 16 participants, i.e., slightly more than 10% of the participants reported volunteering their services to the nursing homes. At two observation sessions at Nursing Home C, it was observed that a total of six male residents were helping with tasks at the nursing home, such as folding washed laundry, towels, and unused trash bags. During an impromptu conversation at an observation session at Nursing Home B, a staff pointed out a female resident who help them with tasks such as drying medicine cups and encouraging fellow residents to take their medication.
“Fits improved, upgraded by God. I can pour water for the plants.,. So, if you have a sincere heart, pour water for the plant…Because I came into this place; and I thank God”.(C5, Length of Stay: 3–5 years, Male, Indian)
Staff: You notice this lady sitting right in front of me…She always also when we give them medication they refuse to take, she’ll support us by asking them to eat. She’ll help us, do a bit of the chores, dry the medicine cups and all that…
Observer: She offered to help?
Staff: She offered to help. The residents they offer to help, you let them do some things.(Impromptu Conversation during 1st Observation at Nursing Home B)
A male resident sitting nearby is busy folding plastic trash bags. He is the only one doing this.
Observer: Why are you folding the trash bags?
Resident: I like to do. I like work, not boring.(Impromptu Conversation during 2nd Observation at Nursing Home C)
One resident reported a life less lonely in the nursing home compared to when he was staying with his wife. Prior to moving to the nursing home, he was cut off from external social networks because of his debilitating illness. At the nursing home, there are a few staffs that he engages in chit chats with.
“I got more people to talk to… More of the staff… They have interesting hobbies and interests that I can talk to them”.(B4, Length of Stay: 1–2 years, Male, Chinese)
The first author observed that staff at all three nursing homes do bring most residents, even several bedbound residents in geriatric chairs, to the common dining hall for lunch and dinner together. There are group exercises or occupational therapy activities in small groups in line with the COVID-19 restrictions on number of persons in group activities.
3.4. Fulfil the Need for Spiritual Care
The “fulfil the need for spiritual care” theme includes the diverse views expressed by participants who ascribe to the main religious faiths of the Singaporean populace (namely Buddhism, Taoism, Christianity, Islam, and Hinduism), one participant of the minority faith Sikhism, two Free-thinkers, and one Atheist. Despite the diversity of religious and spiritual beliefs, common needs emerged: (i) “support for spiritual needs” and (ii) “religious or spiritual beliefs” as anchors when faced with challenges in life. Personal subthemes on “guiding values” and “a life of purpose” also emerged. These findings are consistent with two out of the four domains of the Spiritual Well-being Model (Fisher 2001, 2011); an individual’s intra-relationship with self with regard to values, meaning, and purpose in life and relationship with God or the Cosmos. There are two other domains of the Spiritual Well-being Model, namely, one’s relationship with others (communal) and an environmental domain.
All 16 participants reported the lack of spiritual care to help deal with their health challenges and concerns about meaning, purpose, beliefs, relationship with the cosmos or God and, support for spiritual needs with or without a religious faith.
“You know one thing which is very lacking here, pastoral care, this is totally lacking. They may say they have a pastor and all that… If he does come down because it is to preach. If you go in and look there are a lot of them there waiting to die. They’ve got nothing to do. Pastoral care should be more than just preaching. It should be really getting to know and understand how the elderly feel and communicate with him”.(A5, Length of Stay: >5 years, Male, Chinese)
“… you can pray but must go toilet, use clean water wash face, mouth, nose, ears, hair, arms, feet. Nobody got time take me toilet five times, wash clean before pray <referring to ritual washing called ‘wudu’ by Muslims before praying >”.(C6 Length of Stay: 3–5 years, Male, Malay)
All participants reported that they either did not have, or only had limited opportunities to visit their places of worship, receive prayer group support or spiritual counselling to cope with their deteriorating health conditions or deal with their existential questions.
“That time I stay at my nephew’s house, Neptune court, Holy family. I can walk, go church. <Now>, No. Just stay at home and pray at bed”.(B2, Length of Stay: >5 years, Female, Chinese)
Six participants, i.e., slightly less than 40% of the participants, keep symbols of their religious faith or a copy of their holy book at their bedside cabinets or on walls above their bed and pray by their bedside.
“Got the photo God, I put on top small cabinet near my bed and I pray. All God photo, Vinayagar, Lord Shiva <Hindu dieties>, got ah, pray. I Hindu must pray in the morning after bathing… Before I sleep, I pray”.(A1, Length of Stay: 3–5 years, Female, Indian)
Two out of 16 participants reported praying in the gardens within their nursing homes.
“…more cooling outside, a lot of leaves. I like to look at the leaves, green leaves all these… I just concentrate, close my eyes for one minute. Then I pray ah, just pray. Enjoy praying”.(A3, Length of Stay: 1–2 years, Male, Chinese)
There are positive and negative religious coping methods (Pargament 2001). Positive religious coping is where an individual has a close connection with God, enjoys spiritual connection with family, friends, and the wider community, and is generous. Negative religious coping involves inner turmoil with one’s self and relations with others and God. Research suggests that negative religious coping can promote excessive guilt and have negative health outcomes and even mortality (Pargament 2001).
Three out of the 16 participants, i.e., approximately 20 percent of the participants revealed their struggles with negative religious coping.
“… never go to church after my father die when I young… Yeah, baptised. One day go to church after my father die. When young, If I never go, my father beat us go to church. My mother never beat. My dad beat… I don’t know. I never go to church. I devil. It is written. Written that I do plenty sin. Drink beer…go hell”.(B5, Length of Stay: 3–5 years, Male, Eurasian)
Out of the three participants, one participant is conflicted with his beliefs in two religious faiths in his life; as to which faith will heal him to be able to walk again.
“I believe now got 2 religions inside my body, one Jesus Christ and amulets ‘lah’… See now, when I pray, I want to concentrate more on Jesus. Even the amulet to come and disturb me, I just don’t want to think… For those Thai amulets, they do have this type of amulet to heal. Heal the sickness. … All similar, basically all the same—don’t cheat people, don’t kill people, don’t do bad things, all the same thing but how come for Christian they say all these is not real. This is all demon, but it’s true ‘lah’ those amulets, when I wear that time I feel very happy, I feel very safe.(A3, Length of Stay: 1–2 years, Male, Chinese)
Three participants, an atheist and two others who are either aligned to or practice a religious faith, do not turn to religious coping mechanisms to make meaning of their lives, and find purpose. Ten participants, i.e., approximately 60% of the participants, reported using positive religious coping mechanisms to varying extent that showed in their hopeful attitudes about their lives and a sense of meaning and purpose in their lives.
“I cannot kneel on floor. I sit in the wheelchair and always praying in my heart, always praying in my heart the Quran. Anytime I pray… Give me joy pray Allah… Pray Allah really make me healthy. Bless family with health and money”.(C6, Length of Stay: 3–5 years, Male, Malay)
“I pray every day in the room. My heart I pray, chant. I pray in the morning, before breakfast.
I don’t have a wicked heart. I don’t hurt people. I think nothing wrong. If you do something evil maybe you scared…I believe that if there is no God, we cannot come to this world. There is a God then you come to this world… Whatever the world is given we take. You make good karma, so you can get good things. Good karma is a blessing… I believe that whatever I want, God give me, that one I believe”.(B1, Length of Stay; 3–5 years, Female, Chinese)
3.5. Personal Control
Studies on seniors have revealed the importance of being able to retain some control over their daily lives that nurtures their self-identity and contributes to well-being (Bowers et al. 2009; Katz et al. 2011; Minney and Ranzijn 2016; Potter 2009; Rinnan et al. 2018).
All participants reported a lack of personal control in various facets of their day-to-day life in the nursing home. A common thread is not having a voice to give inputs or feedback in the way their lives are planned and structured for them.
“No. What is there to feedback because when you are given what he called the status of resident. So, in this thing, they are not accepting anything”.(C4, Length of Stay: 3–5 years, Male, Indian)
Eight out of 16 participants, i.e., 50% of the participants feel strongly that there is no independent living as their freedom has been robbed and choices are non-existent.
“This one, they got totally nothing here. They’ll lock you in, lock within the area. Can’t even go out. Can’t even come out here”.(A2, Length of Stay: 1–2 years, Male, Chinese)
“Here they are telling you what to do. You have no freedom to do. So, it bugs me. I make my coffee, I come out and read and drink, and they say why you come here for, so you get very frustrated…”.(C4, Length of Stay: 3–5 years, Male, Indian)
One the other hand, 4 out of 16 participants, i.e., a quarter of them reported having some control over their health conditions by taking actions to improve or maintain their physical health.
“But no matter how, ‘die die’ <Singlish phrase that it is a must have even if you have to die for it> I still need to do. I cannot skip my exercise”.(A3, Length of Stay: 1–2 years, Male, Chinese)
“They will show us the TV <exercise video>, last time my leg cannot carry but after this one I see is very good, I can move my legs. Like this one very good, American exercise. Or Australia, Australia one, not sure”.(B1, Length of Stay: 3–5 years, Female, Chinese)
Five out of 16 residents, i.e., slightly more than a quarter of them either made or accepted the decision to stay in a nursing home to avoid being a burden to family members.
“I am married. I have been here two to three years okay. I come here to relieve my wife. She runs around do the errands, cook, then go see doctor, go to the bank, take me to see doctor because of my Parkinson’s. And she has cancer… Here I can be more relaxed”.(B4, Length of Stay: 1–2 years, Male, Chinese)
Four out of 16 participants, i.e., a quarter of them expressed their desire to acquire new knowledge and skills.
“Want to learn <to go on internet and use the various functions>. But how to learn?”.(C2, Length of Stay: 1–2 years, Male, Chinese)
“I want to learn how to how to do Zoom and I would like to do tuition again and I can give tuition for free”.(A5, Length of Stay: >5 years, Male, Chinese)
“Yeah, I would like to <learn to use a smartphone and surf the internet>. I’m still very alive”.(C3. Length of Stay: 1–2 years, Male, Chinese)
3.6. Desire to Be Free from Worries
There has been an increasing interest on impact of worries on seniors. There are many recent studies that point to poorer quality of life because of anxiety arising from worry (Hohls et al. 2019; Ribeiro et al. 2020; Sousa et al. 2017). Most of the recent studies do fall back on the description of worry by Borkovec (1988), who defined worry as a continuous sequence of negative thoughts while attempting to solve a current problem with unclear solutions and results. According to Granier and Segal (2021), while worry has been established as one of the main symptoms of anxiety disorders, moderate levels of worry, similar to moderate levels of stress, can nudge a person to solve a problem before it becomes unmanageable. However, the study showed that seniors with limited access to resources than younger working adults are less able to solve a problem and very quickly their worry can lead to anxiety and even depression.
Eight out of 16 participants, i.e., 50% of the participants mentioned once in the interview of being free of financial worries as nursing home fees were subsidized by the government and, the remaining portion was either paid by family members or from rental proceeds of their vacant house managed by a family member.
“I think my brother is arranging that… I don’t know. I simply pass my time like that, no problem. I never go and check whether many more money left or what. I never go and check”.(C3. Length of Stay: 1–2 years, Male, Chinese)
Only one participant made reference to being free of financial worries more than once in the interview.
“Young time I was worried…Everything I worry. If have enough money for rent, food, and everything. <Now> Everything is free. Just don’t want to worry”.(C2, Length of Stay: 1–2 years, Male, Chinese)
One female participant reported being free of obligations in managing a household.
“I stay here, no need to do work. I stay here good…Now, I no need to walk, and just lie down. Last time in my home, cook, cook, cook then scold. At my nephew’s house, he got so many things, too many things, the plate too many to wash”.(B2, Length of stay: >5 years, Female, Chinese)
3.7. Adapting to Changes
The ability to change one’s worldview in later life to adapt to changing external environment and circumstances is the start of the change journey in relationship with self, with others, and with the cosmos that happens in old age according to the Theory of Gero-transcendence (Tornstam 19970).
Residents who are able to orientate and accept changes in their new lives in a nursing home are able to experience Joy in Living moments despite diminished health functions and restrictions on their lifestyle from communal living.
Six out of 16 participants, i.e., slightly more than one-third of the participants reported being able to adapt to living in the nursing home and/or accept their diminished health functions in their stride.
“I stay here quite long already. I use to”.(C6, Length of Stay: 3–5 years, Male, Malay)
“I was sick, I fall down. Yeah, so my friends say it’s very difficult, you two stay and no people to look after I and my sister…I see the home is quite good, my friend told me, so they let me think over around three days… I think to make sure my sister also wants to go. My sister says okay, we go in a home better”.(B1, Length of Stay: 3–5 years, Female, Chinese)
Three out of 16 participants, i.e., approximately 20 percent of the participants felt strongly about being forced to live in a nursing home due to their changed circumstances.
“For me, I can take care of myself so many years all along. Why should I need to be in a home? I know the reason simple, they didn’t accept me, but I didn’t expect it to be all the way you know. They took my freedom; they took my freaking life away”.(C4, Length of stay: 3–5 years, Male, Indian)
Two residents reported their frustration and inability to accept their diminished health functions.
“Nothing. Nothing. My hand and legs no good. Nothing can do… My dream is 80 pass away. Now 76. 4 more <years>”.(B5, Length of Stay: 3–5 years, Male, Eurasian)
“Now I cannot walk. I cannot go out. I happen to go out, my eyes will be gone…”.(B3, length of Stay: 3–5 years, Male, Chinese)
4. Discussion
The aim of this study was to uncover the lived experiences of elderly residents in nursing homes and acquire an understanding of what truly and essentially constitutes Joy in Living from their perspective. The study was also meant to shed light on the enabling conditions that nursing home operators can implement that are conducive for Joy in Living, and disenabling conditions to be avoided or eliminated for Joy in Living experiences of residents to flourish.
The results showed that there are seven themes that are important for Joy in Living experiences of elderly to flourish in nursing homes: (i) “supportive nursing home environment and practices” that includes adopting person-centered care, (ii) “connectedness through meaningful relationships”, (iii) “meaningful daily living”, (iv) “fulfil the need for spiritual care”, (v) “personal control”, (vi) “desire to be free from worries”, and (vii) “adapting to changes”. These themes include the enabling and disenabling conditions to Joy in Living in nursing homes and when enabled, promote different facets of Joy in Living experiences of the elderly residing in nursing homes. For example, if a nursing home allocates resources and works through external partnerships to provide spiritual care for residents, then this constitutes an enabling condition to Joy in Living in nursing homes, while neglecting spiritual care is a disenabling condition to Joy in Living in nursing homes.
Person-centered Care (Rogers 1961) and variations of person-centered care such as Person-directed Care (White et al. 2008), Eden Alternative model (Thomas 2003) have been shown in studies to have a positive impact on the well-being of elderly in nursing homes. A review of the literature on Person-centered Care shows that the approach has at its core empathy and a partnership mindset in providing care. There are clearly more studies on positive than negative impact of Person-centered Care on care outcomes for beneficiaries, staff, and the organization. Person-centered Care aims to provide holistic care by considering the recipient as a whole human being with needs beyond the disability or illness presented. Its primary focus is to maintain one’s identity, by recognizing and respecting the individual’s values, preferences, experiences, and relationships formed over their lifetime, with an aim to provide them with a positive psychosocial environment to thrive and enjoy a high quality of life (Leplege et al. 2007). Refer to Table A2 at Appendix A for the summary of studies on Person-centered Care and the findings.
In the study by Moore et al. (2017) that explored the barriers and facilitators to the delivery of Person-centered Care services, a key barrier identified is traditional structures that prioritize quick medical decisions by healthcare professionals in place of conversations with the care recipients to jointly discuss and agree on care plans. Another impediment is the time investment required to learn the new approach and correct language for conversations with care recipients.
The biggest hurdle is overcoming the existing mindsets of management and staff who tend to equate good care with an over-emphasis on medical care (Brownie and Nancarrow 2013). Consequently, the elderly residents are generally still viewed through the medical lens and the service design philosophy is based on the notion of frail elderly being dependent on care providers who will endeavor to deliver services with dignity and compassion. The elderly are regarded as passive recipients of services that focus on their medical needs rather than their broader aspirations for psychosocial and mental well-being and quality of life.
This study revealed the importance of a new dimension not addressed in Person-centered Care models: “fulfil the need for spiritual care” for Joy in Living experiences to flourish. The emergence of this condition in the study is not surprising since according to the Theory of Gero-transcendence (Tornstam 1997), change in relationship within self, with others, and with the cosmos happen in old age.
There are many definitions of spirituality in the literature. Notwithstanding the variety in the definition, there are some common themes such as personal to the individual, inner connection, self in harmony with the external world, the quest for answers to existential questions, relationship with the cosmos or God, and being spiritual with or without religious faith. For example, Puchalski (2008, p. 36) explained that “some measures have included religious attendance or frequency of prayer… while others have looked at more existential or philosophical constructs such as meaning in one’s life or satisfaction with achieving life’s goals”. On the other hand, religion is described as a prescribed set of beliefs, customs, and practices that identifies an individual with a particular religious faith (Baker 2003). Puchalski (2008) associated spirituality with the very essence of being human and the source of our existence and for this very reason, there were studies in the last two decades advocating that spirituality be considered and offered in clinical care settings (Koenig 2012; Puchalski et al. 2009; Saguil and Phelps 2012).
Waaijman (2007) claimed that spirituality involves a relationship to a God or a higher power and can be expressed in many art forms and the interaction with nature, community, and family. Pattison et al. (2010) stated that many individuals associate their religious beliefs with spirituality, yet an individual can be spiritual without being religious. On religiosity, Pargament (2001) put forth the view that one of the key objectives of religion is to find meaning in life. According to Frankl (1962), the search for meaning in life is a life-long pursuit that persists in suffering, old age, and even when faced with inevitable death.
The study revealed four sub-themes of the “fulfil the need for spiritual care” theme for Joy in Living experiences to flourish: (i) “religious or spiritual beliefs”; (ii) “guiding values”; (iii) “support for spiritual needs”; (iv) “a life of purpose”. These are consistent with the literature on spirituality and religion.
Another theme for Joy in Living experiences to flourish is “connectedness through meaningful relationships”. According to MacKinlay (2021), spirituality is closely associated with deep relationship and connectedness with other people, especially those who matter in an individual’s life. She further expounded that individuals with a spiritual connection throughout their lives have a more balanced outlook in life and as they age, they continue to live a life of purpose and are open to new ideas and ways. One of the four domains of the Spiritual Well-being Model is the “communal” domain on an individual’s relationship with others (Fisher 2001, 2011). These studies further strengthen the premise that fulfilling the need for spiritual care is important for Joy in Living experiences to flourish and is a new dimension to be considered in Person-centered Care Model (Rogers 1961) and its variations Person-directed Care Model (White et al. 2008) and Eden Alternative Model (Thomas 2003) in the delivery of services to nursing home residents.
The two separate studies by Bowers et al. (2009) and Katz et al. (2011) revealed common themes of personal identity and self-esteem contributing to quality of life. Even with the loss of independent living and sacrifice of control over many aspects of their lives, the elderly in nursing homes want to maintain as much control as they can over their daily lives, with their opinions sought and heard by healthcare service providers (Bowers et al. 2009; Potter 2009). Other themes that emerged from the two studies are: Elderly with high care needs value having meaningful personal relationships (ongoing or new relationships); being engaged in activities for fulfilment and joy; to contribute to the nursing home and other residents; and, to improve or maintain their physical health. The findings from the study by Minney and Ranzijn (2016) stated that participants’ ability to come to terms with the loss of certain aspects of their lives pre-retirement, willingness to modify their current lifestyles due to health impediments, and be free from responsibilities and worries also influenced their perception of a Good Life.
The findings on “connectedness through meaningful relationships”, “meaningful daily living”, “desire to be free from worries”, “personal control”, and “adapting to changes” are consistent with the findings of the aforementioned three studies. The new themes that emerged from this study are the themes on “supportive nursing home environment and practices” and “fulfil the need for spiritual care”. Even the study by Rinnan et al. (2018) on Joy of Life of the elderly residing in Norwegian nursing homes did not reveal a spirituality component amongst the five dimensions identified. The study by Rinnan et al. (2018) reported one dimension on “sources of meaning” that is aligned with one of the sub-themes: “a life of purpose” of “fulfil the need for spiritual care” theme as revealed by this study.
The importance of the sub-themes of “supportive nursing home environment and practices” theme in this study were identified in several quantitative studies conducted in Singapore. A study by Wang et al. (2016, p. 1) to identify “predictors of self-reported quality of life (QOL) of NH <nursing home> residents in Singapore” revealed that “depression and difficulty in communication with staff are the two main modifiable risk factors of poor QOL of local NH residents”. The results of the quantitative study indicated that higher scores in food enjoyment were negatively associated with major depression and poorer cognitive function. Higher scores in autonomy were negatively associated with major depression, greater dependence, and difficulty in communication with staff.
One key finding in a most recent local study by Tew et al. (2021, p. 1) on “QOL, person-centred care and lived experiences of nursing home residents in a developed urban Asian country” is that “beyond their basic care needs, the residents’ psychosocial needs can be better fulfilled”. The cross-sectional study involved 696 residents from seven Singapore nursing homes. The satisfaction survey covered five dimensions of care: “environment, interaction with people, activities, food, and impact on lifestyle and overall” (Tew et al. 2021, p. 3). Less than half were satisfied in “areas of psycho-emotional needs and autonomy (interaction with the community, maintain a home routine, awareness of happenings outside NH, staff informing residents about what is happening and considering their preferences)” (Tew et al. 2021, p. 6). The survey findings in the five dimensions of care emphasize the need to enhance psychosocial care and empowerment of elderly residents.
The fewer coding references for “desire to be free from worries” and “adapting to changes” themes will be tested against new data to be collected from two other nursing homes for the ongoing study. These themes may be dropped from the final theoretical framework if no new codes emerge from the new data. At the same time, the authors will confirm data saturation that is starting to appear in the current dataset from the three nursing homes and look out for emergence of any new theme(s).
The frequency of coding reference is not the only basis that will be used to assign weightage to the themes and sub-themes when finalizing the theoretical framework upon completion of the study. Weightage will be assigned based on emphasis of particular themes and sub-themes by gender, ethnicity, and length of stay. Literature review and the first author’s experience serving on a Board of a nursing home in Singapore will also be used to interpret the data. For example, the sub-theme “leadership competency” is ranked seven out of the eight sub-themes of “supportive nursing home environment and practices” theme based on frequency of mention in the interviews with residents and observations. Residents in general do not have a full 360-degree view of how a nursing home is run as they are likely to have more interaction with frontline care staff than the leadership team. “Leadership competency” is not easily observable either. “Leadership competency” could have been gleaned from staff interviews which is not one of the data collection methods of the study. From literature review on leadership impact on organizations, “leadership competency” could be ranked as most impactful as management sets the tone of the culture and practices in a nursing home.
5. Conclusions and Recommendations
The study sheds light on the seven themes that have emerged as important for Joy in Living experiences of elderly to flourish in nursing homes that include the enabling and disenabling conditions.
The following recommendations address the key findings of the study discussed earlier under results and discussion sections:
5.1. Supportive Nursing Home Environment and Practices
In the area of supportive nursing home environment and practices, management as the leadership team of the nursing homes can do more to role model desired behaviors and be more “hands on” in soft skills training programmes to bring to life the values of their organizations through story-telling to inspire staff. Staffing and duty rostering need to be reviewed to ensure sufficient staff bandwidth and rest to prevent burnout especially in the current COVID-19 pandemic. Management can also set up systems and adopt practices that encourage feedback from staff and resident for improvement efforts. Management can have regular communication sessions with them to update on evolving COVID-19 measures and other policies impacting the ILTC sector.
Nursing homes need to strengthen their staff development training programmes to include soft skills training programmes, as well as basic English and vernacular languages courses for foreign staff. Current training tend to focus more on nursing skills-based training, which the first author observed at the daily shift hand-over meetings and educational posters in the nursing homes. Certain soft skills training programmes can even be extended to residents, e.g., resilience training to equip residents with the knowledge and skills to bounce back from setbacks in their health functions or loss of a friend or a loved one.
Food, living environment, and safety are basic needs that must be addressed. While it is important to prepare nutritious meals for the elderly, management must realize that boredom can set in with repeated menu options. Having varied menu options featuring local delights and catering to residents with dietary restrictions such as vegetarians, vegans, those requiring halal meals (for Muslims) are important considerations. Management can do quality control of meals catered or prepared in-house by having the same meals as the residents on certain days. Nursing homes may consider having meals ordered from hawker stalls for at least one meal every week where residents get to choose their meal order from a pre-set menu.
When rejuvenating existing nursing home premises or designing new nursing home facilities, management can work with consultants experienced in designing elderly communal living spaces to build homely, conducive, and accessible physical spaces for the elderly to encourage social interaction, participation in activities, and promote independence.
Physical safety and security are important. However, management needs to balance residents’ desire for autonomy versus falls prevention and explore pharmacological and non-pharmacological therapy interventions to treat agitation in residents rather than using restrainers excessively. Regarding the bird nuisance problem, for a longer-term solution, management can work with the National Parks Board of Singapore for innovative and ethical methods to contain the bird population in the vicinity of the nursing homes.
5.2. Meaningful Daily Living
To foster a sense of belonging, social workers of the nursing homes can work with the nursing staff to identify talents, skills and interests of the residents within three to six months on admission. Opportunities can be created for residents to volunteer their services according to their talent and skill. For example, a resident who can play a musical instrument or sing can lead a music interest group. Further, management can build their volunteer base to tap on external expertise to train residents who have an interest to pick up a new skill or organize activities for residents with the involvement of the community. There is room to increase the breadth and depth of social and recreational activities for the residents to prevent boredom from setting in.
5.3. Fulfil the Need for Spiritual Care
Nursing homes in Singapore can do more to provide spiritual care for their residents. Nursing homes could consider hiring counsellors who are trained to provide spiritual counselling for residents and connect with community resources to provide residents with the right faith, spiritual, and cultural support. Within each region in Singapore, there could be a pool of nursing home chaplains of various faiths who could be roped in to support the spiritual needs of residents. Although the “fulfil the need for spiritual care” theme is only one of the seven themes, it is an area when compared to the other themes, the least developed in nursing homes in Singapore. The study findings and recommendations on this theme when adopted in nursing homes in Singapore will greatly enhance Joy in Living experiences in nursing homes.
The strength of the study is the understanding of what truly and essentially constitutes Joy in Living from the perspective of Asian elderly residents of multicultural Singapore and identification of a new dimension on fulfilling the need for spiritual care of residents in person-centered care approaches to allow Joy in Living experiences to flourish. While the small sample size does not permit the generalizability of findings to all nursing homes in Singapore, future quantitative or mixed methods studies with larger samples can verify the findings.
A limitation of the study is that the interviews were conducted in English and excluded elderly who can only speak vernacular languages. To overcome this limitation to some extent, participants who could at least understand and speak basic English were included in the study.
It is envisaged that these changes if implemented by operators/management of nursing homes will promote better psychosocial well-being of the elderly and better living environments where nursing home residents may enjoy satisfactory accommodation while spending their remaining years in joy.
Author Contributions
Data collection, analysis and interpretation of results, S.D.; Organisation, editing and polishing of the paper, K.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board of the Singapore University of Social Sciences. Approval number is APR-0124-V1.0-03062021 and date of approval is 1 June 2021.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A

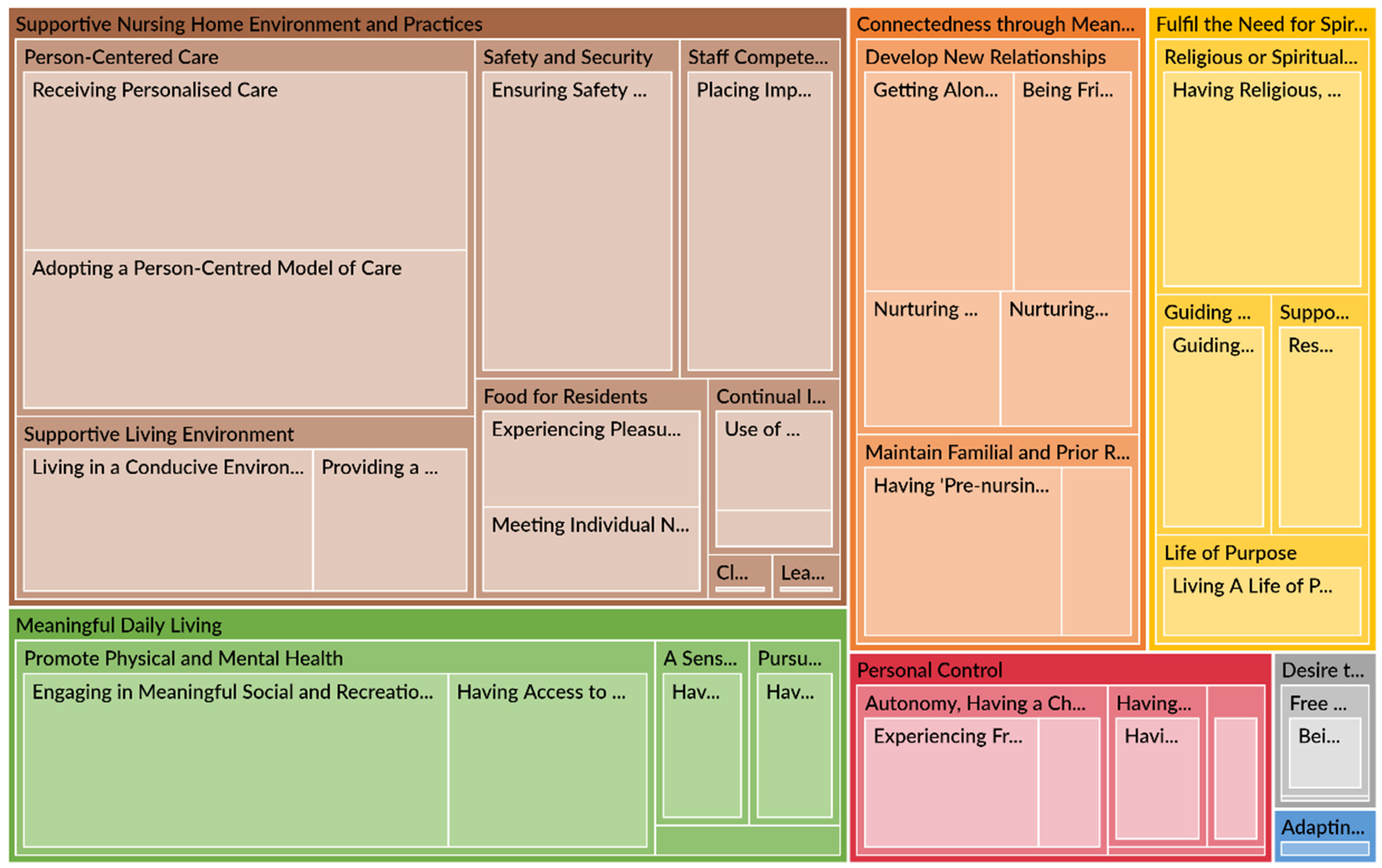{kind=link}
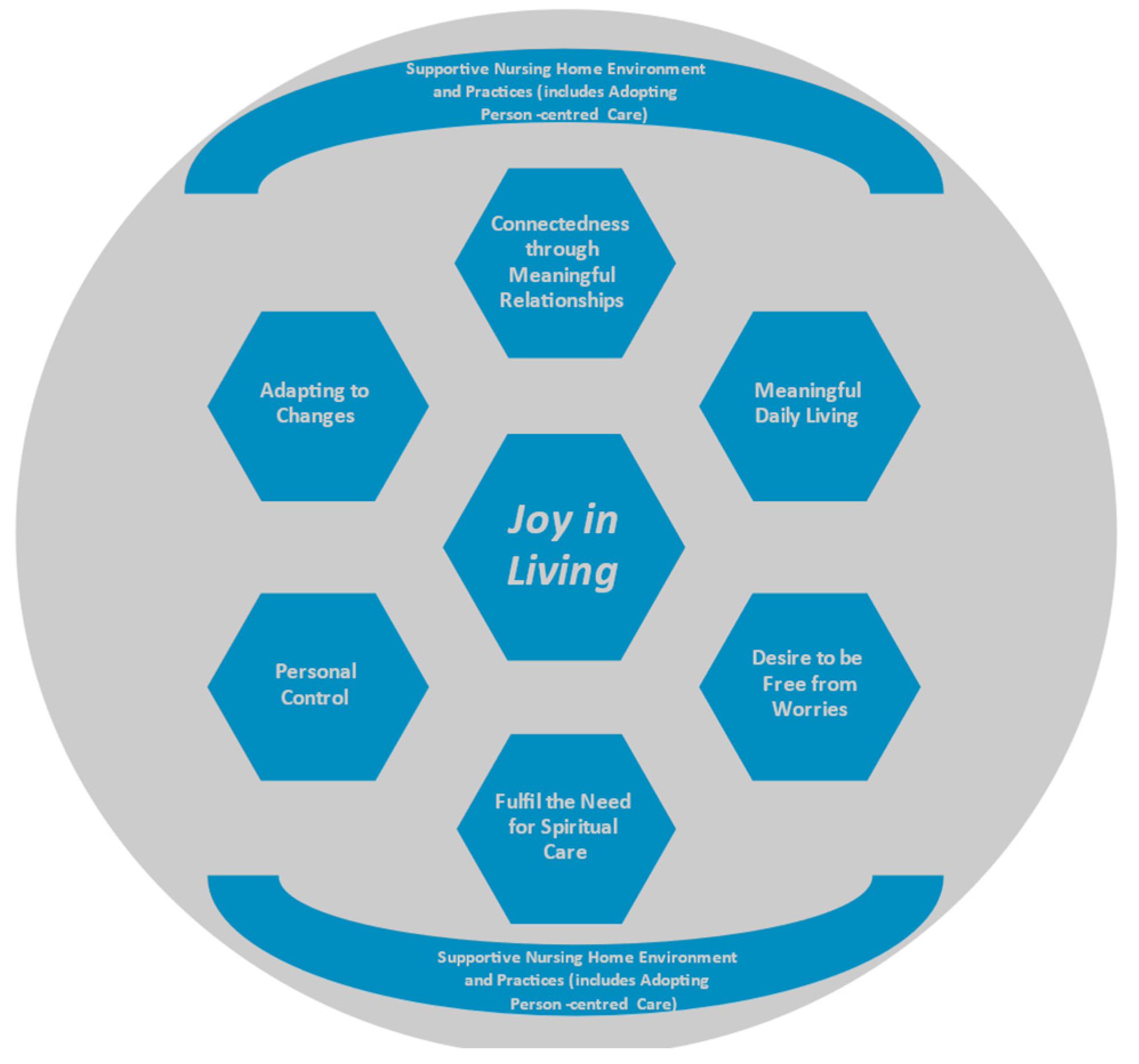{kind=link}
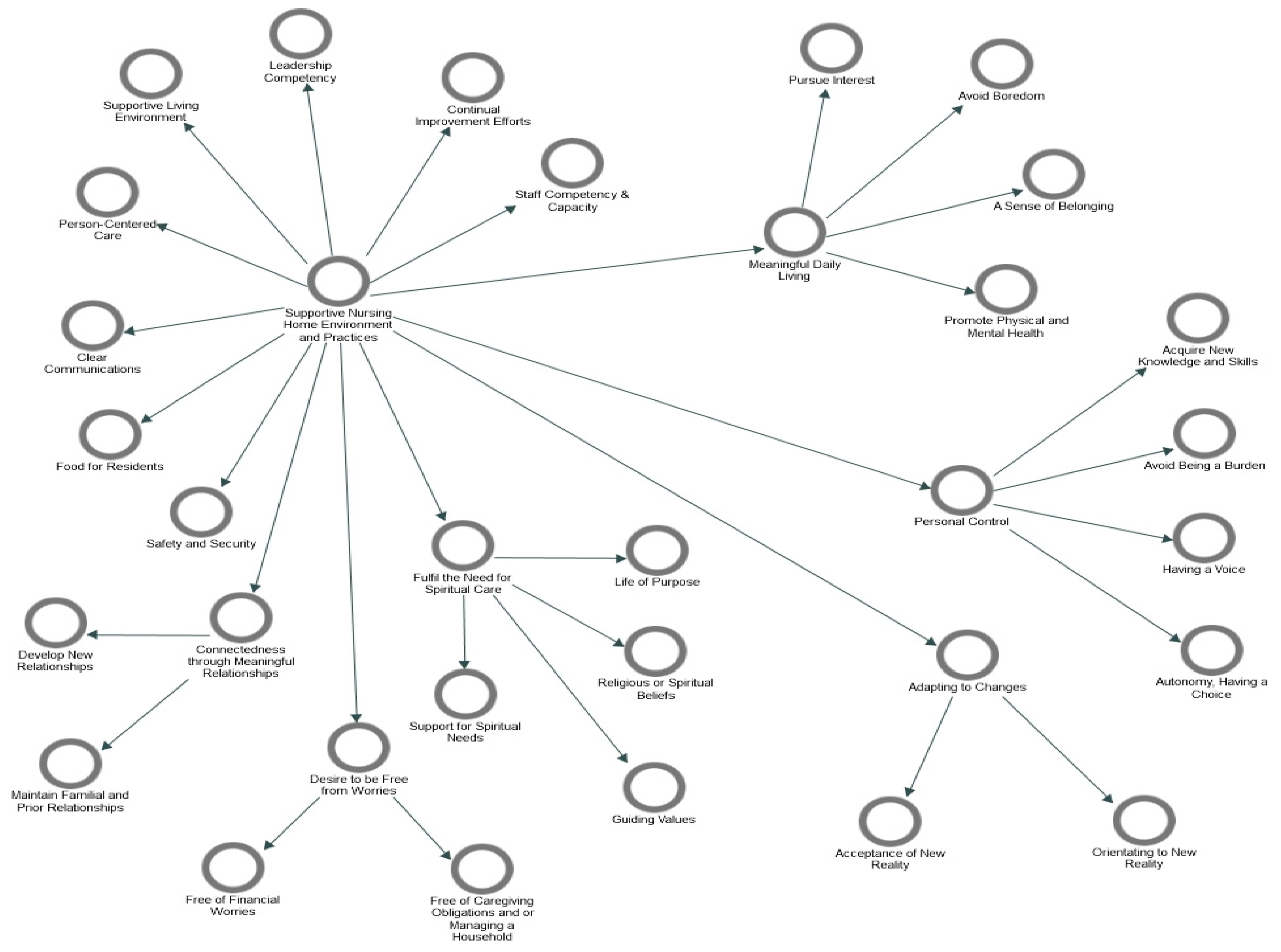{kind=link}
Table A1.
Themes and sub-themes.
| Theme | Sub-Theme | Description |
|---|---|---|
| 1. Supportive Nursing Home Environment and Practices | Person-centered Care | Implementing a holistic care approach that emphasizes the well-being of the elderly as a whole person beyond just nursing and medical care. This includes residents receiving care that is tailored to their needs. Nursing homes use various person-centred care approaches such as Person-centred Care Model or its variations Person-directed Care or Eden Alternative Model to guide the delivery of care for elderly residents. |
| Supportive Living Environment | Creating a good living space in the nursing home for residents’ comfort and an experience of living in their own homes. | |
| Safety and Security | Systems, processes, and practices that protect residents from harm or injury. | |
| Staff Competency & Capacity | Building staff professional competencies, personal leadership, inter-personal and soft skills and knowledge. At the same time, ensuring that staff have sufficient bandwidth by hiring adequate headcount and rostering of duties. | |
| Food for Residents | Meals in nursing homes fulfil each resident’s dietary needs (e.g., vegetarian diet on certain days, diabetic calorie control, “Halal” meals etc.,) and ethnic dietary preference of what they enjoy most and find satisfying. And/or Giving residents opportunities to eat food that has nostalgia associated with it based on the social and celebratory deep memories that can include caring and love. | |
| Continual Improvement Efforts | Innovative or improved resident care policies, systems, processes, products, or services and care delivery approaches that improve nursing home residents’ lives. And/or reaping cost savings by bringing activities together in one place (e.g., a central kitchen, centralized laundry services) or outsourcing and using technology to simplify time-consuming tasks of staff. | |
| Leadership Competency | Management of the nursing home shows by example and/or implements systems, processes and practices that place the needs of the residents at the heart of design and delivery of services. | |
| Clear Communications | Residents receiving up-to-date and clear information on COVID-19 situation, national policies and programmes, and rules of the nursing home. | |
| 2. Connectedness through Meaningful Relationships | Develop New Relationships | Systems (i.e., the structure of how an organization is set up), processes (i.e., activities and tasks that need to be carried out to achieve the outcomes), and practices (i.e., the behaviors and actions of staff) that encourage bonding between residents and care staff (including volunteers). As a result of the bonding, residents feel that staff/volunteers genuinely care and support them throughout their stay in the nursing home. And/or Systems, processes and practices that encourage bonding and friendship among residents. |
| Maintain Familial and Prior Relationships | Proactively exploring opportunities (e.g., counselling by social workers from the nursing home) to mend and/or improve relations with residents’ families. Also, residents can communicate and see their family members and friends as easily as when they were living in the community. | |
| 3. Meaningful Daily Living | Pursue Interest | Setting aside time for residents to take up leisure activities of their choice and have sufficient rest. |
| Avoid Boredom | Boredom is a state of being weary and restless when there is too much time and limited or no opportunities to be engaged in social and recreational activities or pursue interests. | |
| A Sense of Belonging | Having a feeling of acceptance, inclusion and identity as a valued member of the nursing home. | |
| Promote Physical and Mental Health | Residents participating in leisure activities and activities that involve communication and interaction with others that are tailored to the needs and preferences of individual residents. And Residents participating in exercises and activities with movement (either solo or group activities) that have benefits for health, both physical and mental health; including occupational therapy activities that help to maintain health and promote independence of the elderly residents. | |
| 4. Fulfil the Need for Spiritual Care | Support for Spiritual Needs | Meeting residents’ need for inner awakening beyond everyday existence or * Gerotranscendence. * Gerotranscendence is a theory that older people transcend the limited opinions and views of life they once held, and develop new understanding of the self, relationships to others and fundamental existential questions. Support for spiritual growth includes tapping on the resources of the nursing home in the pursuit of God-consciousness and the gerotranscendence theory on self-awareness, relationship with others, and the cosmos. |
| Guiding Values | Moral standards, an ideology or religious views that dictate behaviors and attitudes in the lives of residents. | |
| Religious or Spiritual Beliefs | Relating to a particular religion and its ways or relating to matters of the human spirit or soul. | |
| A Life of Purpose | A central motivation in a resident’s life that gives him/her a reason to carry on living to achieve personal aspirations. | |
| 5. Personal Control | Having a Voice | Giving residents an active and participatory role in either deciding or influencing a decision on their care plans and daily activities. |
| Autonomy, Having a Choice | Residents having opportunities and autonomy to perform actions and move around without being constrained by staff or other parties. And/or Residents having a feeling of autonomy (i.e., freedom from external control or influence; independence) in taking actions to improve their health. | |
| Avoid Being a Burden | Residents not wanting to cause others (especially their loved ones and caregivers) a lot of difficulty, worry or hard work in their care. | |
| Acquire New Knowledge and Skills | Growth opportunities provided or supported by the nursing home for residents to acquire new knowledge and skills. | |
| 6. Desire to be Free from Worries | Free of Financial Worries | Residents not wanting to feel troubled or being required to do something about their finances. |
| Free of Caregiving Obligations and/or Managing a Household | Residents not wanting to feel troubled of caregiving obligations to children, grandchildren or spouses, and/or managing a household. | |
| 7. Adapting to Changes | Orientating to New Reality | Residents adjusting their lives toward the established norms of communal living in a nursing home. |
| Acceptance of New Reality | Residents can accept their diminished health functions. |
Table A2.
Summary of studies on Person-centered Care and the findings.
| Summary of Studies on Person-Centred Care and the Findings | |||
|---|---|---|---|
| Item Number | Theme | Summary of the Study Findings | References |
| 1 | Improved health outcomes in clinical settings | Patient-centred care is associated with better care process with positive outcomes, such as clinical effectiveness, satisfaction ratings, and improved QOL. | (Doyle et al. 2013; Fors et al. 2015; Lowther et al. 2018) |
| 2 | Effectiveness of Person-centred Care of people with dementia | Person-centred care is associated with positive impact on well-being, QOL, improvements to degree of depression severity, and reduced behavioral symptom of agitation in persons with dementia. | (Kitwood 1997; Edvardsson et al. 2014; Barbosa et al. 2015; Kim and Park 2017) |
| 3 | Reduction in cost to healthcare organisations | Patient-centred care interventions in intensive care units and hospital treatments that resulted in cost savings from reduced length of hospital stay and improvements to discharge process. | (Ulin et al. 2016; Goldfarb et al. 2017) |
| 4 | Effectiveness of Person-centred Care of elderly in nursing homes and home care services | Person-centred Care associated with positive impact on well-being, mental and physical health, and QOL. | (Byrne et al. 2012; Edvardsson et al. 2017; Wilberforce et al. 2017) |
| 5 | Barriers and facilitators for the implementation of Person-centred Care | Organisational conditions such as culture, structures, processes, leadership, and HR practices that facilitate or hinder implementation of Person-centred Care | (Braithwaite et al. 2017; Cho et al. 2016; Moore et al. 2017; Ree 2020) |
References
- Aryana, I. G. P. Suka, and R. A. Tuty Kuswardhani. 2018. Sarcopenia in elderly. International Journal of Geriatrics and Gerontology 1: 1–4. [Google Scholar] [CrossRef]
- Atchley, Robert C. 1989. A continuity theory of normal aging. The Gerontologist 29: 183–90. [Google Scholar] [CrossRef] [PubMed]
- Baker, David C. 2003. Studies of the inner life: The impact of spirituality on quality of life. Quality of Life Research 12: 51–57. [Google Scholar] [CrossRef] [PubMed]
- Baltes, Paul B, and Margret M. Baltes. 1990. Successful Ageing: Perspectives from the Behavioural Sciences. Cambrideg: Cambrideg University Press. [Google Scholar] [CrossRef]
- Barbosa, Ana, Liliana Sousa, Mike Nolan, and Daniela Figueiredo. 2015. Effects of person-centered care approaches to dementia care on staff: A systematic review. American Journal of Alzheimer’s Disease & Other Dementias® 30: 713–22. [Google Scholar] [CrossRef] [Green Version]
- Basu, Radha. 2016. Safe but soulless. Lien Foundation. Available online: https://www.lienfoundation.org (accessed on 15 December 2020).
- Borkovec, Thomas D. 1988. Comments on “Worry as a phenomenon relevant to the elderly”. Behavior Therapy 19: 381–83. [Google Scholar] [CrossRef]
- Bowers, Helen, Angela Clark, Gilly Crosby, Lorna Easterbrook, Alison Macadam, Rosemary MacDonald, Ann Macfarlane, Mairi Maclean, Meena Patel, Dorothy Runnicles, and et al. 2009. Older People’s Vision for Long-Term Care. York: Joseph Rowntree Foundation. [Google Scholar]
- Braithwaite, Jeffrey, Jessica Herkes, Kristiana Ludlow, Luke Testa, and Gina Lamprell. 2017. Association Between Organisational and Workplace Cultures, and Patient Outcomes: Systematic Review. BMJ Open 7: e017708. [Google Scholar] [CrossRef] [Green Version]
- Braun, Virginia, and Victoria Clarke. 2006. Using thematic analysis in psychology. Qualitative Research in Psychology 3: 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, Virginia, and Victoria Clarke. 2019. Reflecting on reflexive thematic analysis. Qualitative Research in Sport, Exercise and Health 11: 589–97. [Google Scholar] [CrossRef]
- Braun, Virginia, and Victoria Clarke. 2021. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qualitative Research in Psychology 18: 328–52. [Google Scholar] [CrossRef]
- Brownie, Sonya, and Susan Nancarrow. 2013. Effects of person-centered care on residents and staff in aged-care facilities: A systematic review. Clinical Interventions in Aging 8: 1. [Google Scholar] [CrossRef] [Green Version]
- Byrne, Kerry, Krista Frazee, Joanie Sims-Gould, and Anne Martin-Matthews. 2012. Valuing the older person in the context of delivery and receipt of home support: Client perspectives. Journal of Applied Gerontology 31: 377–401. [Google Scholar] [CrossRef]
- Carstensen, Laura L., Susanne Scheibe, Hal Ersner-Hershfield, Kathryn P. Brooks, Bulent Turan, Nilam Ram, Gregory R. Samanez-Larkin, and John R. Nesselroade. 2011. Emotional Experience Improves With Age: Evidence Based on Over 10 Years of Experience Sampling. Psychology and Aging 26: 21–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, Santosh K., and Krishna Prasad Muliyala. 2016. The Meaning in Quality of Life. Journal of Psycho Social Rehabilitation and Mental Health 3: 47–49. [Google Scholar] [CrossRef] [Green Version]
- Chinnakkaruppan, Adaikkan, Marie E. Wintzer, Thomas J. McHugh, and Kobi Rosenblum. 2014. Differential Contribution of Hippocampal Subfields to Components of Associative Taste Learning. The Journal of Neuroscience 34: 11007–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, Eunhee, Nam-Ju Lee, Eun-Young Kim, Sinhye Kim, Kyongeun Lee, Kwang-Ok Park, and Young Hee Sung. 2016. Nurse staffing level and overtime associated with patient safety, quality of care, and care left undone in hospitals: A cross-sectional study. International Journal of Nursing Studies 60: 263–71. [Google Scholar] [CrossRef] [PubMed]
- Cohen, Marlene Zichi, David L. Kahn, and Richard H. Steeves. 2000. Hermeneutic Phenomenological Research: A Practical Guide for Nurse Researchers. Thousand Oaks: Sage Publications, Inc. [Google Scholar] [CrossRef]
- Creswell, John W. 2007. Qualitative Inquiry and resEarch Design: Choosing among Five Approaches, 2nd ed. Thousand Oaks: Sage Publications, Inc. [Google Scholar]
- Department of Statistics Singapore. 2021. Population Trends. SingStat Website. Available online: https://www.singstat.gov.sg/publications/population-trends (accessed on 18 March 2022).
- Dorner, T. E., Eva Luger, J. Tschinderle, K. V. Stein, S. Haider, A. Kapan, C. Lackinger, and K. E. Schindler. 2014. Association between nutritional status (MNA®-SF) and frailty (SHARE-FI) in acute hospitalised elderly patients. The Journal of Nutrition, Health & Aging 18: 264–69. [Google Scholar] [CrossRef]
- Doyle, Cathal, Laura Lennox, and Derek Bell. 2013. A systematic review of evidence on the links between patient experience and clinical safety and effectiveness. BMJ Open 3: e001570. [Google Scholar] [CrossRef]
- Edvardsson, David, Karin Sjögren, Qarin Lood, Ådel Bergland, Marit Kirkevold, and Per-Olof Sandman. 2017. A person-centred and thriving-promoting intervention in nursing homes-study protocol for the U-Age nursing home multi-centre, non-equivalent controlled group before-after trial. BMC Geriatrics 17: 1–9. [Google Scholar] [CrossRef] [Green Version]
- Edvardsson, David, P. O. Sandman, and Lena Borell. 2014. Implementing national guidelines for person-centered care of people with dementia in residential aged care: Effects on perceived person-centeredness, staff strain, and stress of conscience. International Psychogeriatrics 26: 1171–79. [Google Scholar] [CrossRef] [Green Version]
- Engel, George L. 1977. The need for a new medical model: A challenge for biomedicine. Science 196: 129–36. [Google Scholar] [CrossRef]
- Fisher, John W. 2001. Comparing Levels of Spiritual Well-Being in State, Catholic and Independent Schools in Victoria, Australia. Journal of Beliefs and Values 22: 99–105. [Google Scholar] [CrossRef]
- Fisher, John W. 2011. The Four Domains Model: Connecting Spirituality, Health and Well-Being. Religions 2: 17–28. [Google Scholar] [CrossRef]
- Fors, Andreas, Inger Ekman, Charles Taft, Cecilia Björkelund, Kerstin Frid, Maria E. H. Larsson, Jörgen Thorn, Kerstin Ulin, Axel Wolf, and Karl Swedberg. 2015. Person-centred care after acute coronary syndrome, from hospital to primary care—a randomised controlled trial. International Journal of Cardiology 187: 693–99. [Google Scholar] [CrossRef] [PubMed]
- Frankl, Viktor. 1962. Man’s Search for Meaning, trans. Ilse Lasch, rev. ed. New York: Simon and Schuster, vol. 65, p. 22. [Google Scholar]
- Gabriel, Zahava, and A. N. N. Bowling. 2004. Quality of life from the perspectives of older people. Ageing & Society 24: 675–91. [Google Scholar] [CrossRef] [Green Version]
- Giele, Janet Z., and Glen H. Elder Jr., eds. 1998. Methods of Life Course Research: Qualitative and Quantitative Approaches. Thousand Oaks: Sage Publications, Inc., ISBN 0 761914374. [Google Scholar]
- Goh, Lee Gan, Ee Heok Kua, and Hai Ding Chiang. 2015. Ageing in Singapore: The Next 50 Years. Singapore: Spring Publishing Pte Ltd. [Google Scholar]
- Goldfarb, Michael J., Lior Bibas, Virginia Bartlett, Heather Jones, and Naureen Khan. 2017. Outcomes of patient-and family-centered care interventions in the ICU: A systematic review and meta-analysis. Critical Care Medicine 45: 1751–61. [Google Scholar] [CrossRef] [PubMed]
- Granier, Katie L., and Daniel L. Segal. 2021. Diverse Aspects of Worry among Younger and Older Adults: A Multifaceted Approach. Psychology 12: 441. [Google Scholar] [CrossRef]
- Gray, Rossarin Soottipong, Pungpond Rukumnuaykit, Sirinan Kittisuksathit, and Varachai Thongthai. 2008. Inner Happiness Among Thai Elderly. Journal of Cross-Cultural Gerontology 23: 211–24. [Google Scholar] [CrossRef]
- Hirschmann, Raudhah. 2020. Forecasted Share of the Population Aged 65 Years and above in Singapore in 2019, 2030 and 2050. Statista. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/713663/singapore-forecast-ageing-population/ (accessed on 18 March 2022).
- Hohls, Johanna Katharina, Hans-Helmut König, Eleanor Quirke, and André Hajek. 2019. Association between anxiety, depression and quality of life: Study protocol for a systematic review of evidence from longitudinal studies. BMJ Open 9: e027218. [Google Scholar] [CrossRef]
- Iwarsson, Susanne, and Agneta Ståhl. 2003. Accessibility, usability and universal design—positioning and definition of concepts describing person-environment relationships. Disability and Rehabilitation 25: 57–66. [Google Scholar] [CrossRef]
- Katz, Jeanne, Caroline Holland, Sheila Peace, and Emily Taylor. 2011. A Better Life-What Older People with High Support Needs Value. York: Joseph Rowntree Foundation, Available online: www.jrf.org.uk/publications/older-people-high-suppport-needs.full.pdf (accessed on 15 December 2020).
- Kim, Sun Kyung, and Myonghwa Park. 2017. Effectiveness of person-centered care on people with dementia: A systematic review and meta-analysis. Clinical Interventions in Aging 12: 381. [Google Scholar] [CrossRef] [Green Version]
- Kitwood, Thomas Marris. 1997. Dementia Reconsidered: The Person Comes First. Buckingham: Open University Press, vol. 20. [Google Scholar]
- Koenig, Harold G. 2012. Religion, Spirituality, and Health: The Research and Clinical Implications. ISRN Psychiatry 2012: 278730–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, M. Powell, and Lucille Nahemow. 1973. Ecology and the aging process. In The Psychology of Adult Development and Aging. Washington, DC: American Psychological Association, pp. 619–74. [Google Scholar] [CrossRef]
- Leedy, Paul D., and Jeanne Ellis Ormrod. 2001. Practical Research: Planning and Design, 7th ed. Hoboken: Merrill Prentice Hall. [Google Scholar]
- Leplege, Alain, Fabrice Gzil, Michele Cammelli, Celine Lefeve, Bernard Pachoud, and Isabelle Ville. 2007. Person-centredness: Conceptual and historical perspectives. Disability and Rehabilitation 29: 1555–65. [Google Scholar] [CrossRef] [PubMed]
- Lowther, Keira, Richard Harding, Victoria Simms, Aabid Ahmed, Zipporah Ali, Nancy Gikaara, Lorraine Sherr, Hellen Kariuki, Irene J. Higginson, and Lucy Ellen Selman. 2018. Active ingredients of a person-centred intervention for people on HIV treatment: Analysis of mixed methods trial data. BMC Infectious Diseases 18: 1–9. [Google Scholar] [CrossRef] [Green Version]
- MacKinlay, Elizabeth. 2021. Ageing and frailty: A spiritual perspective of the lived experience. Journal of Religion, Spirituality & Aging 33: 236–49. [Google Scholar] [CrossRef]
- Marques, M., Ana Faria, and Marisa Cebola. 2019. Body mass index and body composition in institutionalized older adults with malnutrition, sarcopenia and frailty. European Journal of Public Health 29: ckz034-070. [Google Scholar] [CrossRef]
- McCormack, Brendan, Jan Dewing, and Tanya Mccance. 2011. Developing person-centred care: Addressing contextual challenges through practice development. Online Journal of Issues in Nursing 16: 1–12. [Google Scholar] [CrossRef]
- Minney, Melissa J., and Rob Ranzijn. 2016. “We Had a Beautiful Home… But I Think I’m Happier Here”: A Good or Better Life in Residential Aged Care. The Gerontologist 56: 919–27. [Google Scholar] [CrossRef] [Green Version]
- Moore, Lucy, Nicky Britten, Doris Lydahl, Öncel Naldemirci, Mark Elam, and Axel Wolf. 2017. Barriers and facilitators to the implementation of person-centred care in different healthcare contexts. Scandinavian Journal of Caring Sciences 31: 662–73. [Google Scholar] [CrossRef]
- Pargament, Kenneth I. 2001. The Psychology of Religion and Coping: Theory, Research, Practice. New York: The Guilford Press. [Google Scholar]
- Pattison, Stephen, Ben Hannigan, and Roisin Pill. 2010. Emerging Values in Health Care: The Challenge for Professionals. Philadelphia: Jessica Kingsley Publishers. [Google Scholar]
- Potter, Charlotte. 2009. What quality healthcare means to older people: Exploring and meeting their needs. Nursing Times 105: 14–18. [Google Scholar]
- Puchalski, Christina M. 2008. Spirituality and the Care of Patients at the End-of-Life: An Essential Component of Care. OMEGA Journal of Death and Dying 56: 33–46. [Google Scholar] [CrossRef] [Green Version]
- Puchalski, Christina, Betty Ferrell, Rose Virani, Shirley Otis-Green, Pamela Baird, Janet Bull, Harvey Chochinov, George Handzo, Holly Nelson-Becker, Maryjo Prince-Paul, and et al. 2009. Improving the Quality of Spiritual Care as a Dimension of Palliative Care: The Report of the Consensus Conference. Journal of Palliative Medicine 12: 885–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ree, Eline. 2020. What is the role of transformational leadership, work environment and patient safety culture for person-centred care? A cross-sectional study in Norwegian nursing homes and home care services. Nursing Open 7: 1988–96. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, Oscar, Laetitia Teixeira, Lia Araújo, Carmen Rodríguez-Blázquez, Amaia Calderón-Larrañaga, and Maria João Forjaz. 2020. Anxiety, depression and quality of life in older adults: Trajectories of influence across age. International Journal of Environmental Research and Public Health 17: 9039. [Google Scholar] [CrossRef] [PubMed]
- Rinnan, Eva, Beate André, Jorunn Drageset, Helge Garåsen, Geir Arild Espnes, and Gørill Haugan. 2018. Joy of life in nursing homes: A qualitative study of what constitutes the essence of joy of life in elderly individuals living in Norwegian nursing homes. Scandinavian Journal of Caring Sciences 32: 1468–76. [Google Scholar] [CrossRef] [Green Version]
- Rogers, Carl Ransom. 1961. On Becoming a Person: A Therapist’s View of Psychotherapy. Boston: Houghton Mifflin Harcourt. [Google Scholar]
- Saguil, Aaron, and Karen Phelps. 2012. The spiritual assessment. American Family Physician 86: 546–50. [Google Scholar]
- Sousa, Rute Dinis de, Ana Maria Rodrigues, Maria João Gregório, Jaime Da Cunha Branco, Maria João Gouveia, Helena Canhão, and Sara Simões Dias. 2017. Anxiety and depression in the Portuguese older adults: Prevalence and associated factors. Frontiers in Medicine 4: 196. [Google Scholar] [CrossRef]
- Tew, Chee-Wee, Siew Pei Ong, Philip Lin Kiat Yap, Amber Yew Chen Lim, Nan Luo, Gerald C. H. Koh, Tze Pin Ng, and Shiou Liang Wee. 2021. Quality of Life, Person-Centred Care and Lived Experiences of Nursing Home Residents in A Developed Asian Urban Country: A Cross-Sectional Study. The Journal of Nursing Home Research 7: 1–8. [Google Scholar] [CrossRef]
- Thomas, William H. 2003. Evolution of Eden. Journal of Social Work in Long-Term Care 2: 141–57. [Google Scholar] [CrossRef]
- Tornstam, Lars. 1997. Gerotranscendence: The contemplative dimension of aging. Journal of Aging Studies 11: 143–54. [Google Scholar] [CrossRef]
- Ulin, Kerstin, Lars-Eric Olsson, Axel Wolf, and Inger Ekman. 2016. Person-centred care–An approach that improves the discharge process. European Journal of Cardiovascular Nursing 15: e19–e26. [Google Scholar] [CrossRef]
- van Manen, Max. 1990. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy. Albany: University New York Press. [Google Scholar]
- Waaijman, Kees. 2007. Spirituality-A multifaceted phenomenon: Interdisciplinary explorations. Studies in Spirituality 17: 1–113. [Google Scholar] [CrossRef] [Green Version]
- Wang, Pei, Philip Yap, Gerald Koh, Jia An Chong, Lucy Jennifer Davies, Mayank Dalakoti, Ngan Phoon Fong, Wei Wei Tiong, and Nan Luo. 2016. Quality of life and related factors of nursing home residents in Singapore. Health and Quality of Life Outcomes 14: 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wee, Shiou-Liang, Athel J. Hu, Joel Yong, Wayne F. Chong, Prassanna Raman, and Angelique Chan. 2015. Singaporeans’ perceptions of and attitudes toward long-term care services. Qualitative Health Research 25: 218–27. [Google Scholar] [CrossRef] [PubMed]
- Werngren-Elgström, Monica, Gunilla Carlsson, and Susanne Iwarsson. 2009. A 10-year follow-up study on subjective well-being and relationships to person–environment (P–E) fit and activity of daily living (ADL) dependence of older Swedish adults. Archives of Gerontology and Geriatrics 49: e16–e22. [Google Scholar] [CrossRef] [Green Version]
- White, Diana L., Linda Newton-Curtis, and Karen S. Lyons. 2008. Development and initial testing of a measure of person-directed care. The Gerontologist 48: 114–23. [Google Scholar] [CrossRef] [Green Version]
- Wilberforce, Mark, David Challis, Linda Davies, Michael P. Kelly, Chris Roberts, and Paul Clarkson. 2017. Person-centredness in the community care of older people: A literature-based concept synthesis. International Journal of Social Welfare 26: 86–98. [Google Scholar] [CrossRef] [Green Version]
- Williamson, Toby. 2010. My Name Is Not Dementia: People with Dementia Discuss Quality of Life Indicators. London: Alzheimer’s Society. [Google Scholar]
- World Health Organisation (WHO). 2022. “Malnutrition”. WHO Website. Available online: https://www.who.int/news-room/questions-and-answers/item/malnutrition (accessed on 18 March 2022).
Figure 1.
The hierarchy chart shows the frequency of reference to the themes, subthemes, and codes in the transcripts of the interview and the observation audio recordings.
Figure 1.
The hierarchy chart shows the frequency of reference to the themes, subthemes, and codes in the transcripts of the interview and the observation audio recordings.

Figure 2.
Themes for Joy in Living experiences in nursing homes.

Figure 3.
Concept map of the themes and sub-themes for Joy in Living experiences in nursing homes.

Table 1.
Profile of the sixteen participants.
| Name of Resident | Gender | Ethnicity | Length of Stay |
|---|---|---|---|
| Nursing Home A | |||
| A1 | Female | Indian | 3–5 years |
| A2 | Male | Chinese | 1–2 years |
| A3 | Male | Chinese | 1–2 years |
| A4 | Male | Chinese | 1–2 years |
| A5 | Male | Chinese | >5 years |
| Nursing Home B | |||
| B1 | Female | Chinese | 3–5 years |
| B2 | Female | Chinese | >5 years |
| B3 | Male | Chinese | 3–5 years |
| B4 | Male | Chinese | 1–2 years |
| B5 | Male | Eurasian | 3–5 years |
| Nursing Home C | |||
| C1 | Male | Chinese | >5 years |
| C2 | Male | Chinese | 1–2 years |
| C3 | Male | Chinese | 1–2 years |
| C4 | Male | Indian | 3–5 years |
| C5 | Male | Indian | 3–5 years |
| C6 | Male | Malay | 3–5 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Dayanandan, S.; Mehta, K. What Does Joy in Living Mean to Elderly Residents of Nursing Homes in Singapore? Religions 2022, 13, 469. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050469
AMA Style
Dayanandan S, Mehta K. What Does Joy in Living Mean to Elderly Residents of Nursing Homes in Singapore? Religions. 2022; 13(5):469. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050469
Chicago/Turabian StyleDayanandan, Swapna, and Kalyani Mehta. 2022. "What Does Joy in Living Mean to Elderly Residents of Nursing Homes in Singapore?" Religions 13, no. 5: 469. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13050469
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.