
The Muslim Gaze and the COVID-19 Syndemic


1
Muslim Doctors Association, London E16 2DQ, UK
2
Allied Health Professionals CIC, Suffolk IP23 7BH, UK
3
Bradford Institute for Health Research, Bradford Teaching Hospitals NHS Foundation Trust, Bradford BD9 6RJ, UK
*
Author to whom correspondence should be addressed.
Religions 2022, 13(9), 780; https://0-doi-org.brum.beds.ac.uk/10.3390/rel13090780
Submission received: 15 January 2022
/
Revised: 3 August 2022
/
Accepted: 8 August 2022
/
Published: 25 August 2022
(This article belongs to the Special Issue Muslims and COVID-19: Everyday Impacts, Experiences and Responses)
Abstract
:COVID-19 has replicated and intensified pre-existing health inequities by creating a vicious syndemic that brings together concurrent biological, psychosocial and structural epidemics with synergistic interactions that reinforce unequal outcomes. In the UK, the Muslim community has been disproportionately impacted by excess morbidity and mortality from COVID-19. This article uses a transdisplinary lens in the context of COVID-19 to analyse the role of Islamophobia as a fundamental driver of health inequities in Britain’s Muslim community. It highlights multilevel policy reforms and recommendations that centre community empowerment, social justice and cultural humility to close the gap and achieve justice and good health for all.
1. Introduction
COVID-19 was declared a pandemic on 11 March 2020. It was first reported in China in December 2019, although evidence suggests it was circulating in Europe before this (Amendola et al. 2021). The virus spread to all continents, except Antarctica, in less than four months. To date, almost 171,396 people have died and over 21 million people have been infected in the UK. COVID-19 has not been a leveller but has been a great revealer, shining a light on pre-existing disparities in society; those who already experienced social and health inequities on the margins of society have been disproportionately impacted, further increasing marginalisation.
After campaigning by community and faith groups on publishing data by faith groups, the government published its report in June 2020, which showed that Muslims had the highest risk of dying from COVID (Office for National Statistics 2020a). There are multiple reasons for the disproportionate numbers of deaths related to COVID-19 among British Muslims, such as living in deprivation, poverty, structural inequalities, racism and Islamophobia. However, after accounting for deprivation and ethnicity, this excess risk disappeared, consistent with structural discrimination, racism and Islamophobia as the main drivers of disparities in the Muslim community as these are exacerbated in a post-9/11 political context in West. These structural disparities are not new; prior to COVID-19 it was well known that Muslims face some of the worst outcomes in domains of social mobility, housing, education, employment and income as well as pre-existing poor health outcomes (Ali 2015).
A more appropriate term for COVID-19 is that it is a syndemic, bringing together concurrent biological, psychosocial and structural epidemics with synergistic interactions that reinforce unequal outcomes. The excess disease burden of COVID-19 experienced by Muslims in the UK necessitates a new framework for health policy and action that predicts, controls and mitigates risks to close an unacceptable, unfair and unjust gap. This paper is a critical analysis; at the time of writing the world is grappling with the Omicron variant of coronavirus. Application of lessons learnt is vital and urgent as we continue to enter cycles of restrictions and normalcy in the face of virus mutation, inequity in global vaccine access, vaccine hesitancy, divisive public policies and social polarities. A syndemic framework and transdisciplinary lens can support more equitable and effective health policy responses.
2. Epidemiology and Clinical Features of COVID
COVID-19 is a disease caused by SARS-CoV-2, a virus belonging to the coronavirus class of viruses. These viruses are named for their appearance; under the microscope, they look like they are covered with pointed structures that surround them like a corona, or crown.
Data from the first wave showed that 81% of infected individuals developed mild to moderate illness, 14% developed severe disease requiring hospital admission, 5% developed critical illness, and 2.3% died (Wu and McGoogan 2020). Most patients experience mild disease as the initial host immune response contains the infection resulting in respiratory symptoms and constitutional upset. However, in patients with severe disease the immune system undergoes excessive activation producing a toxic mix of inflammatory proteins called cytokines, creating a “cytokine storm”. This can further activate an inflammatory cascade resulting in respiratory distress syndrome, bacterial infection and sepsis, multi-organ failure and death (Bhaskar et al. 2020). The presence of this inflammatory “cytokine signature” predicts severity and survival (Del Valle et al. 2020).
Risk factors on clinical assessment found to be associated with the development of severe disease and mortality in the first wave can broadly be categorised into three groups: underlying condition, clinical presentation and laboratory markers (Williamson et al. 2020). Underlying factors associated with increased severity included older age and male sex, ethnic minority background, hypertension, pulmonary and kidney disease, diabetes, obesity, dementia and malignancy. In later waves, being unvaccinated has been observed to be an added risk factor for severe disease (Singanayagam et al. 2022).
In the first wave, death rates for COVID-19 were found to be higher for Black African and Caribbean and Bangladeshi and Pakistani Asian ethnic groups (Office for National Statistics 2020b). In the second wave, there was a decrease in excess mortality risk for Black African and Caribbean groups but an increase for Bangladeshi and Pakistani ethnic groups. However, this datum underestimates the impact on ethnic minority groups (Office for National Statistics 2021a). For example, anecdotal reports indicate that the Somali community has been significantly impacted, as have other Muslim-majority ethnic groups, but the lack of disaggregated data which invisiblises these groups precludes an accurate assessment of impact. In general, British Muslims have experienced a greater risk of COVID-19 and serious consequences of the pandemic (Hassan et al. 2021).
3. Syndemic Theory
The syndemic theory was conceptualised by Singer and colleagues, working in the early 1990s on the AIDS epidemic that was ravaging urban poor communities of colour in North America (Singer 1994, 2000). They observed that these communities already faced multiple other endemic and epidemic health crises such as HIV, TB, sexually transmitted infections, substance misuse, suicide, homicide, chronic liver disease and infant mortality. Singer argued that these health crises did not merely co-occur and cluster among vulnerable communities, but that the synergy among epidemics made each of them worse. Furthermore, situating these co-occurring epidemics in their context was vital as they were created and sustained by broader political, economic and social factors that accumulated over generations resulting in deep-seated inequities.
The framework proposes that co-occurrence of diseases, in particular geographical and temporal contexts due to harmful social conditions, leads to disease concentration in marginalised populations. Additionally, overlapping epidemics exacerbate the health effects of adverse social conditions through disease interactions, either through biological interactions between disease states, or through interactions between biological and social processes at the level of populations and individuals (Singer et al. 2017).
Additional components that we make explicit in this framework in Box 1 are that of intersectionality and mutually causal adverse consequences that contribute to further disparities and create new epidemics. These principles are demonstrated through application of our adapted syndemics framework.
Box 1. Principles of a syndemics framework applied to Britain’s Muslim community.
- Large-scale political-economic forces, accumulate over generations, result in deep-seated social, economic and power inequities grounded in Islamophobia as a fundamental driver of disparities at multiple levels
- Disease concentration: co-occurrence of multiple social and spatial epidemic clusters as a result of inequities shaping distribution of risks and resources for health
- Disease interaction: overlapping epidemics exacerbate the health effects of adverse social conditions, either through biological interactions between disease states or through interactions between biological and social processes
- Intersectionality: overlapping epidemics have differential impact on subgroups that embody unique and multiple axes of discrimination and disadvantage simultaneously along lines of protected characteristics that interact with structural and social forces
- Mutual enhancement and causation: epidemics do not merely co-occur, the synergy and reinforcement between them increases overall burden on communities, contributes to further disparities and creates new epidemics
4. The Muslim Gaze and Islamophobia
According to the 2011 Census, there were 2.8 million Muslims in the UK, comprising almost 5% of the population of United Kingdom. Nearly half were born in the UK and almost half were under 25, representing the youngest age profile of all religious groups. However, Muslims in Britain form a large, heterogeneous group that is demographically, historically, socially and politically diverse with generational differences and internal differentiation around religious sects, political factions, ethnicity, language and cultural practices, among several other characteristics. Despite these differences, a major and near-ubiquitous problem for Muslims in Britain is the way they are perceived as a monolithic “other” through the gaze of the White, non-Muslim British majority (Modood and Thompson 2021).
“The gaze” and the “archaeology of medical perception” was described by Foucault (2012), positioning the medical diagnostic process as an act of looking at patients and objectifying and separating them from their personal identities. The concept of the Foucauldian disciplinary gaze is rooted in psychological relationships of power and privilege of the gazer over the gazed, which produce social oppression. This concept has been adapted and applied to discourses around other marginalised and oppressed communities such as feminism (Ponterotto 2016), racism (Demirtürk 2009) and post-colonial orientalism (Said 1978).
“The Muslim gaze” places Muslims as the observed other in the UK, identifying them through the prism of normative values defined by the privileged observer (White, non-Muslim British). In times of crises such as COVID-19, the Muslim gaze is intensified and operationalised through necropolitics (Mbembe 2008) and structural violence, with the government using social and political power to dictate who must live and who must die.
The Muslim gaze is at the root of Islamophobia. The term “Islamophobia” was first formally coined in the late 1990s (Runnymede Trust 1997) to conceptualise growing anti-Muslim sentiments. Though hostile sentiments towards Muslims have existed even before they settled in Britain, those sentiments have intensified in recent times due to the Iranian Revolution, the Salman Rushdie affair, the Gulf War, 9/11 and ISIS fuelling negative stereotypes and creating a stigmatised and socially devalued identity in all aspects of the lives of Britain’s Muslims through narratives fixated on integration, multiculturalism, civilisation, British values and security.
The All Party Parliamentary Group on British Muslims report Islamophobia Defined (All Party Parliamentary Group 2017) identifies Islamophobia as a form of cultural racism that “targets Muslimness and expressions of Muslimness” based on the racialisation of Islam and Muslims. This legally non-binding definition has been adopted by several major parties and includes the Mayor of London, but it was rejected by the Conservative government as “unworkable”. The Equality Act (2010) recognises race and religion as protected characteristics. However, focusing on race or religion alone may underestimate the oppression and disadvantage that Muslims in the UK face because of the synergistic interaction between both of these marginalised identities. The multiple and alternative conceptualisations of Islamophobia are beyond the scope of this article and have been covered elsewhere (Sealy 2021). The gendered nature of Islamophobia and the disproportionate impact on women through hate crimes (Tell Mama 2018) and workplace exclusions referred to as “The Triple Penalty” (Miller 2016) point to the need for an intersectional approach. An intersectional Muslim gaze operating in a multilevel overlapping syndemics framework from the structural to the individual can be useful for understanding the potent effect of Islamophobia on shaping risks and outcomes from COVID-19 in Britain’s Muslim community.
5. The Perfect Biosocial Storm
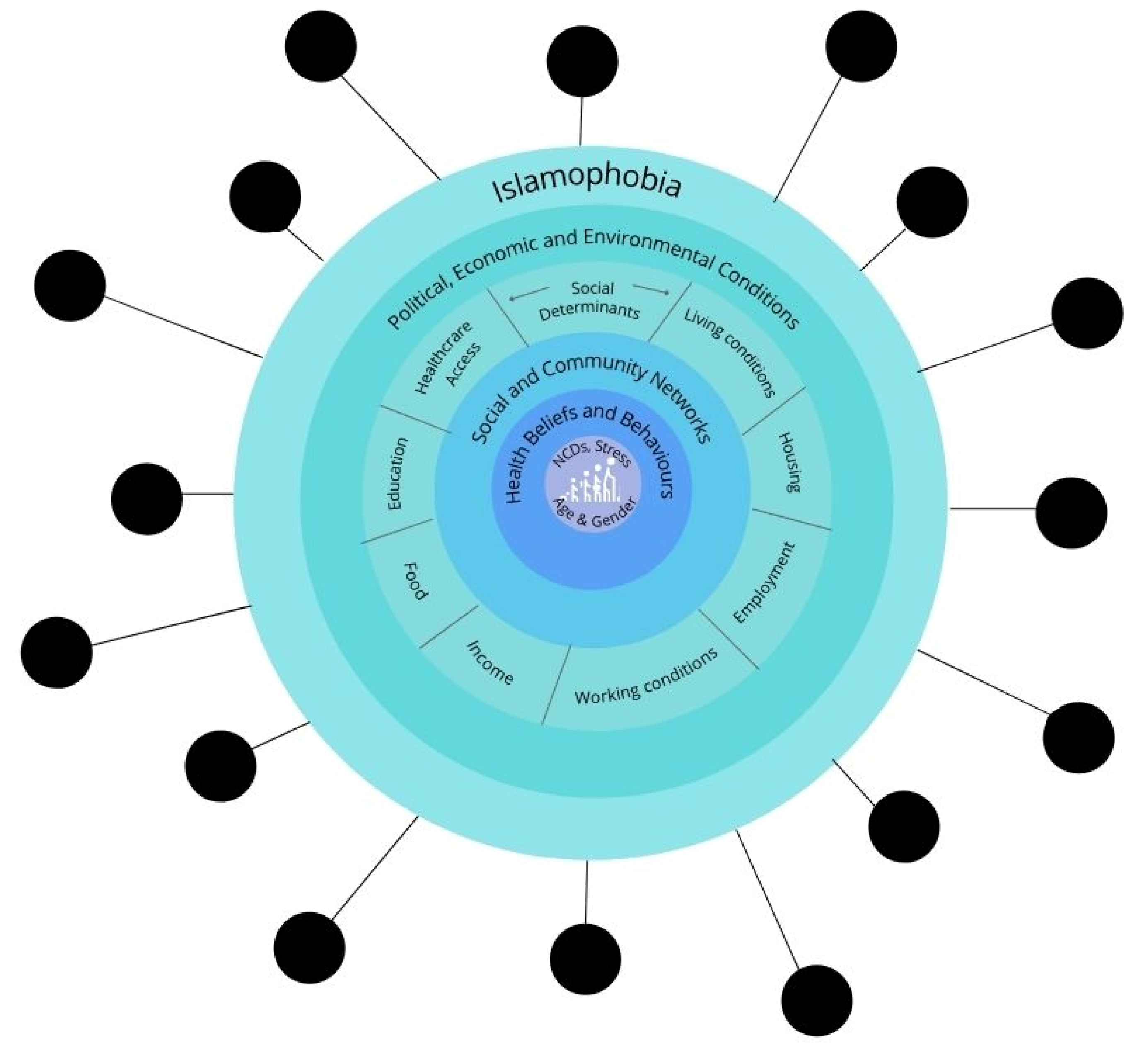
Co-occurring biological, psychosocial and structural epidemics create a perfectly toxic biosocial storm in which disease concentration and interaction take place, driven by Islamophobia as the fundamental driver and re-enforcer as shown in Figure 1.
5.1. Structural Epidemics
The Muslim gaze creates a hostile policy environment through legalisation, media and engagement practices, resulting in deep-seated social, economic and power injustices against Muslims with downstream effects. They undermine confidence and compliance with public health interventions, create barriers and reduce trust in healthcare professionals and services and contribute to community transmission, delay in accessing treatment and increased risk of severe illness and death.
5.1.1. Historical Mistrust
Historical mistrust of government through legacies of colonialism and slavery has been accentuated through recent dehumanising events exemplified by the Grenfell tragedy, the Windrush scandal and the current Nationality and Borders Bill (UK Parliament 2021), which highlight necropolitics and the conditional nature of belonging of ethnic minorities and Muslims in the UK. Policies and legislations on areas such as austerity, immigration, security and civil society engagement are key structural tools of the government’s biopolitical machinery and are subject to the Muslim gaze. Policies of selective engagement with Muslim civil society organisations (Elahi and Khan 2017) by the government resulted in the exclusion of critical grassroots Muslim voices from early policy decisions during COVID-19. Early community engagement is essential to trust building and knowledge exchange to ensure that policies and programmes are inclusive, participatory and sensitive to the needs of marginalised groups. It is well reported in the literature predating COVID-19 that certain groups within the Muslim community have lower confidence in vaccination programmes (Larson et al. 2018). Yet there was still a lack of early consultation with faith and community groups on the COVID-19 vaccine roll out, and this was reflected in the low uptake of COVID-19 vaccination in the Muslim community. The concept of medical mistrust is seen in communities of colour (Thorburn et al. 2012) with implications on health service utilisation and disparities (LaVeist et al. 2009). The structural factors above may similarly lead to public health and medical mistrust in the Muslim community. In the context of COVID-19, they may have reduced compliance with public health messaging around isolation and testing as well as contributed to misinformation, fake news and alternative sources of health information and services, such as alternative practitioners and faith healers whose methods lack robust evidence base in mainstream science and may be harmful and further delay necessary medical treatment.
5.1.2. Media Stereotypes
The media is a powerful tool that shapes public perception. The Muslim gaze created divisive media and political narratives that scapegoated Muslims, created a climate of fear and fueled further mistrust of public health messages from official sources. The negative representation and stereotypes of Muslims in mainstream media are well documented (Allen 2012). During COVID-19, Islamophobic bias, prejudice and group stigma were further amplified in negative media stories about Muslims constructed around narratives of non-compliance with public health measures, such as frontpage images of hijab-wearing women not wearing masks, spreading COVID due to attending mosques and social gatherings, panic buying and travelling abroad (Centre for Media Monitoring 2021). Last-minute travel restrictions left thousands of British Muslims stranded, and inconsistent travel policies created anger and further alienation, such as among the Pakistani community who were placed on the red list due to the rapid transmission of the Delta variant in their neighbouring country that was not under the same restrictions. A similar inconsistency was seen with penalties on African countries during early days of the Omicron variant. The effect of this was to intensify the Muslim gaze, increase alienation and reduce the social cohesion essential to managing a public health emergency that depends on cooperation and collaboration.
Hijab-wearing women were hypervisibilised in the Muslim gaze of the media and projected as symbols of the ongoing threat that the Muslim community poses to wider society. On social media, an “Islamophobic infodemic” (Awan et al. 2021) was widespread with anti-Muslim hatred and hostility, and misinformation about Muslims being poisonous and spreading COVID-19 through religious festivals, conspiring a “Muslim plot” to rule the world through vaccines, the origin for COVID-19 being in the Quran, as well as open expressions of joy at Muslim suffering, death and inequalities and pride and enjoyment in the act of spreading misinformation and being Islamophobic (Poole and Williamson 2021). Once again, these contribute to public health and medical mistrust.
5.1.3. Immigration Policies
As a significant proportion of Muslims are born outside the UK, immigration policies disproportionately impact them, creating financial and psychological barriers, such as the immigration health surcharge and the fear of deportation of undocumented migrants presenting to health services. These can create a barrier to accessing healthcare, resulting in delayed presentation with more advanced disease. Border closure policies, suspensions of search and rescue operations in the Mediterranean and UN resettlement programmes and lack of preparedness plans during COVID-19 also significantly impacted refugees and migrants (Kluge et al. 2020), a significant proportion of them from Muslim-majority countries. Where migrants do enter the UK, they need to deal with unfamiliar language and multiple complex processes to navigate the healthcare system, which further layers barriers to healthcare access. COVID-19 restrictions of self-isolation and quarantine also resulted in reduced help from volunteers, reducing support to vulnerable populations in the UK and increasing health and social risks.
5.1.4. Security Policies
Security policies such as Countering Violent Extremism (CVE) have alienated Muslims (Cohen and Tufail 2017) and have been shown to create a barrier to accessing healthcare through mistrust of the government through a mandatory prevent policy in the NHS (Aked 2020). Marginalisation and alienation also create an information vacuum that is easily filled with alternative information sources, including fake news and conspiracy theories that can be harmful and increase community transmission by downplaying or dismissing the legitimacy and credibility of health advice. Additionally, young ethnic minority people were more likely to be fined for allegedly breaching COVID-19 restrictions (Currenti and Flatley 2020), feeding into fears around state hyper-surveillance and the Muslim gaze among the Muslim community, which may have impacted compliance with the track and test programme as well as generated concerns around COVID-19 vaccines containing microchips for state surveillance.
5.1.5. Poverty
Poverty is endemic within the UK’s Muslim community, with almost half of Muslim households living in poverty (Ali 2015). Deprivation was one of the strongest risk factors for worse outcomes during the first wave of COVID-19. The earliest data showed that more patients from ethnic minority backgrounds were admitted to critical care with a clear social deprivation gradient and doubling of risk in those from the most deprived areas (Intensive Care National Audit and Research Centre 2020). In particular, Muslim-predominant Pakistani and Bangladeshi patients along with Black patients occupied a third of intensive care beds despite making up 14% of the population.
5.1.6. Neighbourhood Characteristics and Residential Segregation
Data also showed that urban areas, increased population density (Office for National Statistics 2020c) and high levels of air pollution (Rashid et al. 2021) were associated with higher COVID-19 mortality. The majority of Muslims live in the population-dense cities of Bradford, Birmingham, Manchester and London and other major cities in Wales and Scotland, although these trends are gradually changing with increased dispersion now being observed (Gale 2013). It is worth noting that conscious self-segregation and separatism are common negative stereotypes that Muslims face, but segregation can be a protective response to living in a hostile society where Islamophobic hate crimes and violent attacks continue to increase year after year (Home Office 2021).
Lack of affordable housing also limits residential options and choice, with Muslims being the most likely to live in poor quality social housing. Additionally, urban and deprived neighborhoods in which Muslims find themselves are associated with increased levels of air pollution (Fecht et al. 2015) and may be also associated with obesogenic environments lacking green spaces and food deserts with poor quality energy-dense nutrition (Burgoine et al. 2011). This can contribute to obesity, cardiometabolic and nutritional disorders, conditions associated with a higher risk from COVID-19 infection, as described previously (Thorburn et al. 2012; LaVeist et al. 2009).
5.2. Psychosocial Epidemics
The Muslim gaze creates multiple social epidemics that are not only inert by-products of structural violence and injustices but also positively interact with and reinforce them.
5.2.1. Living Conditions
Adverse living conditions are not just limited to the neighbourhood level; Muslims are more likely to live in multigenerational and multifamily households in social housing, thus experiencing overcrowding (Ali 2015). This makes self-isolation and shielding difficult and increases transmission risk to clinically vulnerable older relatives living in the same household. Additionally, social housing is more likely to suffer from damp and poor ventilation, which increases the risk of underlying chronic respiratory conditions and therefore severe COVID-19.
5.2.2. Employment and Financial Hardship
Muslims have been hit harder by financial hardship in multiple ways. During COVID-19, Muslims were six times more likely to lose their job (Muslim Census 2020). They are also more likely to work in shut-down sectors, be self-employed, work in the lowest skilled occupations in front-facing key worker roles, are more likely to be in single-income households and less likely to have savings (Bunglawala 2004). In addition to increased exposure, Muslims had reduced protection due to discrimination at work and insufficient access to PPE reported during community engagement and outreach work (MDA 2021). Due to the language and citizenship barriers explained above, they also experienced difficulty with signing up to government support schemes due to fear of being deported, which negatively impacted their health and well-being. This created a moral dilemma during illness, necessitating a choice between life and livelihood.
5.2.3. Workplace Discrimination
In highly skilled jobs such as medicine, over 90% of doctors who died were from an ethnic minority background, and an analysis by the Muslim Doctors Association revealed that over 50% of the doctors who died in the first wave were Muslim (MDA 2020). A number of factors were thought to contribute to this; challenges cited included lack of access to PPE, testing and appropriate risk assessment, stress, discrimination and reports of being bullied and harassed to work in high-risk frontline conditions compared to their White counterparts. Lack of belonging and psychological safety, outsider status and the inability to show up authentically at work (Shahid and Ali 2021) contributed to internalised Islamophobia, low self-esteem and an inability to raise concerns at work. High exposure risk and lack of adequate protection contributed to an increased infection rate as well as transmission to extended family members.
5.2.4. Trauma-Based Barriers to Healthcare
The Muslim gaze others the cultural practices of Muslims, which influences community and social networks as well as health beliefs and access to healthcare. The media stereotypes of “Muslim ghettos”, male terrorists and oppressed women are replicated in the attitudes of healthcare professionals treating Muslim patients, especially women (Laird et al. 2007). These lead to a breakdown in trust and therapeutic relationship and can create suspicion, fear, mistrust, stigma, stereotype threat and internalised Islamophobia, resulting in avoidance of mainstream health services. Other trauma-based barriers to accessing healthcare include the legacy of unethical medical experimentation and practices on racialised bodies, such as the use of the Simms speculum on enslaved women (Ojanuga 1993), the Tuskegee Syphilis Study (Gamble 1997), forced sterilisation of marginalised women (Patel 2017) and the CIA-led fake hepatitis B campaign in Pakistan to obtain DNA samples in the search for Osama Bin Laden (Kakalia and Karrar 2016). These create transgenerational trauma imprints and may drive the widely reported under-representation of minorities in health research and clinical trials for vaccines and therapeutic agents (UK Government Scientific Advisory Group for Emergencies 2020) and give rise to specific fears around vaccines altering DNA and being used for surveillance, experimentation or depopulation of minoritised populations.
5.2.5. Health Literacy
A combination of these factors may be implicated in the persistent dissatisfaction in health services (Department of Health 2009) reported by Muslim patients as well as a reduced utilisation of healthcare services and an uptake of preventative services such as vaccination and screening (Szczepura et al. 2008). In addition, poorer educational attainment in older Muslims can intersect with socioeconomic deprivation and influence health literacy, beliefs and behaviours. It is also well known that individuals from ethnic minority backgrounds, especially older generations that are at increased health risks, prefer media sources that are culturally, linguistically and contextually appropriate. The lack of messaging through these channels early in the first wave may have marginalised Muslims and further contributed to an information vacuum by reducing the reach and impact of life-saving protective public health messaging. This vacuum may have been filled by complimentary or alternative health services creating delays in accessing appropriate care. In addition, fatalistic health beliefs and myths can further delay presentation to healthcare services when unwell. These factors may contribute to increased transmission and risk of serious complications and deaths due to delayed and advanced presentations of COVID-19.
5.2.6. Disruption of Communal Cultural Practices
Communal cultural practices such as burials, funerals, congregational prayers and large weddings were a significant aspect of cultural practices that were not given timely attention. These may have increased risk of exposure and transmission and required tailored health messaging co-produced and delivered by trusted community leaders, which was lacking early in the COVID-19 pandemic. Eid, on the contrary, was singled out for requiring a last-minute Northern lockdown and Muslims were blamed for disease transmission. This created a stigma, fed in to stereotypes and generated anger among the Muslim community aimed at what was seen as a divisive government response to the pandemic (Mahase 2020).
5.2.7. Adverse Mental Health Impacts
Restrictions from COVID-19 had a negative impact on the mental health of Muslims. These were particularly linked to the disruption of cultural and religious practices, resulting in psychological distress and reduced feelings of belonging and connectedness (Hassan et al. 2021). Minority stress, acculturative stress and complex trauma amplified by Islamophobia and hate crimes experienced by Muslims accumulate over the life course and are associated with poorer mental health, including depression, anxiety and psychosis, in addition to producing physiological dysregulation and interacting with the physical health risks and the pathological processes described below. A recent report demonstrated that over 70% of Muslims who disclosed mental health problems had been victims of Islamophobia (Bunglawala et al. 2021). These intersect with the increased prevalence of mental health disorders seen during COVID-19 among Muslims, increasing the overall burden of poor mental health (Hassan et al. 2021).
5.3. Biological Epidemics
5.3.1. Chronic Disease Burden and Nutritiona Deficiencies
Chronic diseases such as diabetes and cardiovascular disease are higher among Muslims as are multi-morbidity, vitamin D deficiency and other nutritional deficiencies (Shahid 2022; Shahid et al. forthcoming). These were associated with a higher risk of severe disease and death form COVID-19 as previously described. These conditions are also known to be predominantly socially patterned, i.e., shaped by the distribution of socially determined risk and access to resources. However, even at interpersonal levels, “everyday discrimination” is associated with an increased risk of cardiovascular disease, diabetes and obesity (Lewis et al. 2010). Therefore, Islamophobia at multiple levels creates poor baseline health.
5.3.2. Epigenetic Modulation
Attributing ethnic health disparities largely to genetic factors is misplaced; it is well known that there is more genetic variation within than between ethnic groups, and there is widespread consensus amongst genetics experts and epidemiologists that genetic factors contribute only little to ethnic inequalities in health. However, an increased interest in the role of adverse childhood events (ACE), also known as early life stress (ELS), in modulating genotypic and phenotypic expression and developmental and physiological processes is creating a new understanding of how social discrimination can have a cumulative life course and transgenerational impact that are embodied biologically and transmitted through genetic modifications such as DNA methylation (Lang et al. 2020). Raised cortisol levels (Lapp et al. 2019), cardiovascular health (Kuzawa and Sweet 2009), chronic pain (Aroke et al. 2019), and epigenetic contributions to nutrition, psychosocial stress and environmental toxicant exposure have been described in the literature, which are all relevant to the Muslim population (Thayer and Kuzawa 2011).
5.3.3. Intersectionality and Multiply Marginalised Groups
Risks and vulnerabilities are not distributed evenly across the Muslim population and there are important subgroup differences; the lack of disaggregated data makes it difficult to understand this in more depth. Intersectionality (Crenshaw 2018) is a highly relevant concept to Britain’s Muslims because it recognises that individuals from marginalised groups experience multiple axes of discrimination and oppression with a synergistic effect. Muslim men were most likely to die from COVID-19, with the risk increasing with age. Among women, more than half of pregnant women admitted to hospital with COVID-19 were from an ethnic minority background. Asian pregnant women were four times more likely to be admitted with COVID-19 and Black pregnant women eight times. The barriers faced by Muslim women in accessing healthcare are multiple (Shahid et al. forthcoming). Additionally, 4 in 10 ethnic minority women reported facing struggles making ends meet, and 45% struggled to cope with different demands on their time due to domestic, care work and home schooling. Over half of disabled or retired ethnic minority women did not know where to turn to for help, and life satisfaction and happiness were lowest for this group. Almost two thirds of people who died due to COVID-19 had a disability; the rates of disability are higher among Muslims (Ali 2015).
Though ethnic minorities have historically made up only 3% of the care home population, with lower levels among Muslims, over half of the deaths in care homes were among Black people, and COVID-19 accounted for almost half of the deaths among Asian care home residents. It is not possible to disaggregate this data for faith.
Among children, 70–80% of children who were treated for a rare COVID-19 syndrome were from an ethnic minority background. Children from lower socioeconomic backgrounds and those living in overcrowded households faced difficulties with access to online learning and there was the added psychological burden among ethnic minority children of losing family members through excess mortality observed in these communities. Although disaggregated data for faith are not available, we have described above how socioeconomic disadvantaged and COVID-19 mortality is concentrated in the Muslim community.
6. Disease Interactions
The biosocial storm of the syndemics framework (Singer et al. 2017) shows how diseases that are known to cluster in Muslims, such as cardiovascular disease, diabetes and nutritional deficiencies, as well as poorer outcomes in maternal and child health, mental health, elderly care and patients with disability, intersected with and were amplified by COVID-19 and the social disparities that shape them, which are driven by Islamophobia as a determinant of “risk of risk” through multiple, interacting and interchangeable pathways. Some of these pathways increase the risk of specific chronic diseases, some to mental health disorders, some to COVID-19, and some to combinations of these and beyond.
Psychological risks and vulnerabilities generated by structural injustice, social disparities and multiple disadvantages simultaneously invisiblise and hypervisiblise Muslims through marginalisation/exclusion and blaming/scapegoating. These create individual and group stigma and a socially devalued identity. These factors in turn shape health beliefs and behaviours through access to healthcare and compliance with public health measures, as well as disrupt the social cohesion that is essential in a public health crisis, where the interdependence of individual and social actions require solidarity and a collective response.
The embodiment of Islamophobia is an area that has not been directly researched. At the biological level, the convergence of the pathophysiological processes of SARS-CoV-2 and embodiment of Islamophobia produces excess morbidity and mortality. Drawing on research on trauma, stress, racism and discrimination (removed for peer review), key mechanisms through which the pathophysiological processes produced by Islamophobia may interact with the pathophysiological processes of SARS-nCoV-2 to increase severe disease outcomes, deaths and therefore widen health disparities include:
- (a)
- Stress and trauma that alter key regulatory physiological systems (Ong et al. 2017): cardiovascular, neuroendocrine and immune function which can lead to acute inflammation and elevated stress hormone levels such as adrenaline and cortisol, elevated inflammatory markers such as C-reactive protein, raise blood pressure and cardiovascular risk, suppress or hyperactivate the immune system, stimulate the expression of several pro-inflammatory cytokine, increase oxidative stress and generate a systemic inflammatory response. These pro-inflammatory cytokines overlap with the components of the cytokine storm, and thus may amplify the cytokine storm produced by SARS-nCoV-2 associated with severe disease.
- (b)
- Allostatic load and biological weathering: chronic inflammation and physiological activation weather the body, contributing to the development of long-term conditions such as hypertension, obesity, diabetes and malignancy. All of these are known risk factors for severe COVID-19 and raise the possibility of interaction between allostatic load and biological weathering and disease states that increase risks from COVID-19.
- (c)
- Appraisal and affective reactions that evoke changes in the function of organs in key physiological systems such as dilatation of blood vessels, modulation of the neuroendocrine and immune system resulting in the release of pro-inflammatory cytokines and changes in cardiac, hepatobiliary and mental function (Liu et al. 2017). These processes overlap with the cytokine storm seen with COVID-19 and may also amplify multi-organ damage observed with severe COVID-19. Negative appraisal and affective responses and chronic inflammation can also alter neural circuitry and increase social stereotypes that negatively impact mental health and generate a vicious cycle (Eisenberger et al. 2017).
- (d)
- Stress/discrimination and epigenetics: research on epigenetics has shown that differences in host tissue and subgroup patterns of SARS-nCoV-2 infection may be driven by DNA methylation modifications (Chlamydas et al. 2021). A similar process of DNA methylation modification can occur as a response to stress-induced epigenetic processes seen in socially marginalised groups, as described previously, which could potentially alter susceptibility to COVID-19 infection.
7. Worsening Inequities and New Epidemics
There is evidence from previous outbreaks that SARS may impact susceptibility to lipid and glucose disorders, inflammation and tumours (Wu et al. 2017). Additionally, the increased risk of severe disease carries with it increased risk of long-term organ damage; the impact of this is still not fully understood. Evidence of long COVID among ethnic groups is mixed; prevalence determined through self-reporting (Office for National Statistics 2021b) was found to be higher among White people compared with Asian, but clinically diagnosed post COVID-19 syndrome was found to be highest in South Asian and Black groups (Walker et al. 2021). Again, data examining the impact on different faith groups are not available.
However, infection mortality and morbidity rates do not capture the full burden of COVID-19 due to excess mortality from delayed care and access to healthcare, social determinants and socioeconomic consequences, and overburdened health care systems. The indirect impact of COVID-19 through lockdown restrictions creating a barrier to accessing healthcare and the backlog of care in the NHS may be driving worsened control of conditions such as diabetes, hypertension, weight gain, lipid disorders and delayed cancer diagnosis being observed in the NHS. As these conditions are concentrated in the Muslim community, health disparities are likely to intensify post COVID-19. The collateral casualties associated with COVID-19 and public health interventions, such as restrictions and stigmatising narratives around vaccination uptake, may widen mistrust between the Muslim community, the government and health services. Using the terminology such as “vaccine hesitancy” while combating the pandemic to describe the low uptake of COVID-19 vaccination that was generic in the UK (Lockyer et al. 2021) and associating it with British Muslim populations without any evidence, will only further the counterproductive Muslim gaze in health policy and among health practitioners, and it will deprive British Muslims from active participation in health promotion programmes.
COVID-19 is associated with an increased risk of psychiatric and neurological morbidity, which increases with severity of infection (Taquet et al. 2021). This intersects with the high mental health burden present in the Muslim community before and during the pandemic, made worse by excess deaths in the Muslim community and associated with bereavement disorders, post-traumatic stress disorders, financial strain, disruption of communal rituals through lockdown restrictions, and experiences of Islamophobia.
This evidence points to the intensification of health and social inequalities due to COVID-19 among Muslims in Britain. Increased Islamophobia, socioeconomic adversity, the increased burden of chronic and mental health disorders and the high COVID-19 burden with long-term sequelae may interact to worsen long-term health outcomes after COVID-19. This can lead to individuals being less likely to be fit for work, impacting employment prospects, income, housing, access to material resources and other social assets that are determinants of health, generating a vicious cycle that also poses a risk to the economic objectives of the government’s “levelling up” agenda.
Racialised health and social disparities will not only further widen, but also Islamophobia is likely to amplify and intensify the Muslim gaze by feeding into stereotypes of welfare-dependent minorities, and by increasing the othering and vulnerability that is capitalised on by extremist groups. This will undermine the government’s community cohesion plan by increasing discord and conflict, negatively impacting community relations and solidarity, and further increasing Islamophobia, all of which will create another vicious cycle. Trauma due to the layering and overlapping of these multiple and intensified epidemics is in itself an invisible epidemic with long-term and transgenerational impacts that need further attention and intervention.
8. Implication for UK Policy, Practice and Future Directions
This analysis highlights the utility of a syndemics framework in systematically mapping risks and vulnerabilities in Britain’s Muslim population and highlights the role of Islamophobia as a fundamental cause and driver of disparities from COVID-19. Co-occurring structural, psychosocial and biological epidemics have increased the risks of COVID-19 in four inter-related and interdependent ways in Britain’s Muslim community: (a) increased exposure through living in deprived, dense and polluted neighbourhoods, overcrowded housing and working in frontline key worker roles; (b) reduced protection due to lack of trust in public health messages and barriers to accessing and utilising health care and information, and working conditions without adequate risk assessments and PPE; (c) increased transmission due to living in multigenerational, ovecrowded, poorly ventilated housing, inability to self-isolate due to lack of sickness pay and financial protection, communal cultural practices, misplaced health beliefs and behaviours and associated conspiracy theories and misinformation; and (d) increased complications due to delays in accessing and utilising healthcare, increased risk of underlying health conditions and embodiment of Islamophobia altering physiological and genetic processes that increase disease severity. Application of the framework predicts widened health disparities through mutual causation and enhancement, increasing disease concentration and interaction in the Muslim community. Epigenetic modifications create a “biological memory” of stress and trauma (Thayer and Kuzawa 2011) with predicted long-term impacts; therefore, minimizing future health disparities among Britain’s Muslim population requires addressing Islamophobia and structural inequities in the current environment.
An effective policy response requires an explicit focus on health inequity, social justice and well-being. It must involve a whole system life course approach built on an asset and strengths-based model centred on community empowerment with transparent, inclusive and participatory governance structures. This begins by recognising the urgent need to address Islamophobia in order to mitigate potent downstream risks and vulnerabilities demonstrated by the syndemics framework. An approach to multilevel responses to mitigate risks is shown in Table 1.
Important lessons have been learnt during COVID-19 that have implications for ongoing and future public health interventions. Evidence shows the significant positive role that faith-based organisations have played during the pandemic, especially in increasing the uptake of COVID-19 vaccinations in the Muslim community and delivering innovative and inclusive campaigns to reach underserved populations (Race Disparities Unit 2021). Religion is an overlooked determinant of health and faith-based interventions that can save lives; a community empowerment approach embedded in public health policy can maximise the reach, impact and sustainability of health interventions. Acknowledging religion as a strength and an asset can shift the Muslim gaze and dismantle the Islamophobia that is a fundamental driver of health and social inequities. Using Islamic faith settings in the UK, such as mosques, madrassas and women circles, to study Islam and Muslim community organisations can help increase the uptake of marginalised populations in public health interventions and ensure their involvement in the implementation and delivery of health promotion programmes (Rai et al. 2019; Dogra et al. 2021). Once the active involvement of those Islamic faith settings in health promotion programmes becomes a norm, the behavior change among authorities and health promotion bodies can facilitate shifting the Muslim gaze in mainstream media from projecting British Muslims as “others” or “suspects”. Popular imagination about British Muslims shaped by the Muslim gaze might turn from “others” into active contributors and partners for reducing health inequalities among high-risk groups and ethnic minorities. (Figure 2)
The strong family, neighbourhood, community and religious ties that are found in Britain’s Muslim community have been shown to increase the social capital (Helliwell and Putnam 2004) associated with improvement in both physical health and subjective well-being. Creating agency for ownership of health interventions and asset mapping are important mechanisms to give voice to the marginalised, focus on the strengths of communities that are stereotyped and stigmatised, and provide ownership and control of decisions impacting communities to support self-determination and self-management.
Social justice foundation and cultural humility must be at the core of all interventions. A commitment to eliminating inequities and marginalisation requires trust building, strengthening capabilities and capacities and recognising communities as self-determined experts in the health issues affecting them. This involves centring lived experiences, listening to concerns with empathy and responding with validation and compassion to ensure that communities feel heard and that interventions are culturally and contextually relevant and responsive to their needs and priorities. By way of example, understanding the contextual validity of the concerns around the ingredients and the religious acceptability and the history of medical experimentation and unethical practices, how these play out in shaping specific fears around COVID-19 vaccination, and using trusted people, places and spaces to address these concerns, have been helpful in increasing vaccine uptake.
Subgroup differences in risks and outcomes in the Muslim community indicate the need for holistic, multidimensional and tailored interventions rather than a one-size-fits- all approach. Joined up care and working with a focus on personalised care are vital to address the social and wider determinants of health impacting Muslim communities. New systems of care, such as Integrated Care Systems being legislated in the UK from April 2022, provide a unique opportunity to embed joined up care as a routine way of working in the National Health Service, where community organisations have a vital role, such as working with Primary Care Networks to deliver funded social prescribing and referral schemes.
Representation and accountability are essential to strengthen trust and relationships. Community insights and intelligence are important tools for early planning and preparedness. Rapid policy briefings in a project between the Muslim Doctors Association and the School of Oriental and African Studies London (SOAS) provided early insights, predictors and recommendations (MDA 2020), but the lack of early consultation and representation of community leaders and organisations on policy decisions by the government cost lives, with subsequent government reports and documents showing the lessons learnt that communities had already forewarned about. It is also concerning that there is no reference to Islamophobia in the Commission on Race and Ethnic Disparities (2021) report commissioned by the government on ethnic disparities in COVID-19 outcomes, despite clear evidence of Muslims being disproportionately impacted. Dislocating the penetrating Muslim gaze from the mental scrutiny of policy makers, where visible Islamophobia in Britain remains invisible (Foucault 2012), is necessary to ensure that the recommendations by public health authorities transform health care practices for everyone, including British Muslims. As an independent public inquiry is under way, this must be well-resourced and wide-ranging in its consultation and include recommendations to address Islamophobia as a fundamental cause of health disparities in the Muslim community.
It is highly likely that there will be another pandemic; the lessons learnt from three waves of COVID-19 must not go to waste and the same mistakes should not be repeated. The COVID-19 syndemic sharply highlights our global interconnectedness and thus requires moving away from nationalist and populist policies to values-based policies driven by justice, compassion and solidarity to protect lives, livelihoods and human respect and dignity. It necessitates equitable and ethical distribution and access to vaccines, therapeutic agents and health system strengthening, mitigating co-occurring structural, social, psychological and biological epidemics and centring community empowerment of marginalised groups and addressing fundamental structural drivers. This is essential to not only contain the emergence of new variants and epidemics, but to affirm that good health is a fundamental human right for all that sees no borders, colour or religion.
Author Contributions
Conceptualization, H.J.S.; methodology, H.J.S. and S.A.D.; formal analysis, H.J.S. and S.A.D.; investigation, H.J.S. and S.A.D.; writing—original draft preparation, H.J.S. and S.A.D.; writing—review and editing, H.J.S. and S.A.D.; visualization, H.J.S.; project administration, H.J.S. and S.A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Aked, Hil. 2020. False Positives: The Prevent Counter-Extremism Policy in Healthcare. London: Medact, pp. 80–83, Paperback, Free. ISBN 978-1-8381205-0-4. Available online: https://www.medact.org/wp-content/uploads/2020/07/MEDACT-False-Positives-WEB.pdf (accessed on 14 January 2021).
- Ali, S. 2015. British Muslims in Numbers: A Demographic Socioeconomic and Health Profile of Muslims in Britain Drawing on the 2011 Census. London: Muslim Council of Britain. [Google Scholar]
- All Party Parliamentary Group. 2017. Islamophobia Defined. Available online: https://static1.squarespace.com/static/599c3d2febbd1a90cffdd8a9/t/5bfd1ea3352f531a6170ceee/1543315109493/Islamophobia+Defined.pdf (accessed on 14 January 2021).
- Allen, Chris. 2012. A Review of the Evidence Relating to the Representation of Muslims and Islam in the British Media. Birmingham: Institute of Applied Social Studies. [Google Scholar]
- Amendola, Antonella, Silvia Bianchi, Maria Gori, Daniela Colzani, Marta Canuti, Elisa Borghi, Mario C. Raviglione, Gian Vincenzo Zuccotti, and Elisabetta Tanzi. 2021. Evidence of SARS-CoV-2 RNA in an oropharyngeal swab specimen, Milan, Italy, early December. 2019. Emerging Infectious Diseases 27: 648. [Google Scholar] [CrossRef] [PubMed]
- Aroke, Edwin N., Paule V. Joseph, Abhrarup Roy, Demario S. Overstreet, Trygve O. Tollefsbol, David E. Vance, and Burel R. Goodin. 2019. Could epigenetics help explain racial disparities in chronic pain? Journal of Pain Research 12: 701. [Google Scholar] [CrossRef] [PubMed]
- Awan, Imran, Pelham Carter, Hollie Sutch, and Harkeeret Lally. 2021. COVID-19: What Are the Drivers of the Islamophobic Infodemic Communications on Social Media? Available online: http://www.open-access.bcu.ac.uk/12536/ (accessed on 14 January 2022).
- Bhaskar, Sonu, Akansha Sinha, Maciej Banach, Shikha Mittoo, Robert Weissert, Joseph S. Kass, Santhosh Rajagopal, Anupama R. Pai, and Shelby Kutty. 2020. Cytokine storm in COVID-19—Immunopathological mechanisms, clinical considerations, and therapeutic approaches: The REPROGRAM consortium position paper. Frontiers in Immunology 11: 1648. [Google Scholar] [CrossRef] [PubMed]
- Bunglawala, Shenaz, Adriana Meha, and Aneta D Tunariu. 2021. Hidden Survivors: Uncovering the Mental Health Struggles of Young British Muslims. London: The Better Communities Business Network. [Google Scholar]
- Bunglawala, Zamila. 2004. Aspirations and Reality: British Muslims and the Labour Market. Budapest: Open Society Institute. [Google Scholar]
- Burgoine, Thomas, Seraphim Alvanides, and Amelia A. Lake. 2011. Assessing the obesogenic environment of North East England. Health & Place 17: 738–47. [Google Scholar]
- Centre for Media Monitoring. 2021. British Media’s Coverage of Muslims and Islam 2018–2020. Available online: https://cfmm.org.uk/wp-content/uploads/2021/11/CfMM-Annual-Report-2018-2020-digital.pdf (accessed on 14 January 2022).
- Chlamydas, Sarantis, Athanasios G. Papavassiliou, and Christina Piperi. 2021. Epigenetic mechanisms regulating COVID-19 infection. Epigenetics 16: 263–70. [Google Scholar] [CrossRef]
- Cohen, Barbara, and Waqas Tufail. 2017. Prevent and the Normalization of Islamophobia. Available online: https://eprints.leedsbeckett.ac.uk/id/eprint/5462/1/PreventandtheNormalizationofIslamophobiaPV-TUFAILpdf.pdf (accessed on 14 January 2022).
- Commission on Race and Ethnic Disparities. 2021. Commission on Race and Ethnic Disparities: The Report. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/974507/20210331_-_CRED_Report_-_FINAL_-_Web_Accessible.pdf (accessed on 7 August 2022).
- Crenshaw, Kimberle. 2018. Demarginalizing the intersection of race and sex: A Black feminist critique of antidiscrimination doctrine, feminist theory, and antiracist politics [1989]. In Feminist Legal Theory. London: Routledge, pp. 57–80. [Google Scholar]
- Currenti, Rosanna, and John Flatley. 2020. Policing the Pandemic: Detailed Analysis on Public Enforcement of the Public Health Regulations and an assessment on Disproportionality across Ethnic Groups; London: National Police Chiefs’ Council. Available online: https://www.northyorkshire-pfcc.gov.uk/content/uploads/2020/07/Policing-the-Pandemic-NPCC.pdf (accessed on 14 January 2022).
- Del Valle, Diane Marie, Seunghee Kim-Schulze, Hsin-Hui Huang, Noam D. Beckmann, Sharon Nirenberg, Bo Wang, Yonit Lavin, Talia H. Swartz, Deepu Madduri, Aryeh Stock, and et al. 2020. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nature Medicine 26: 1636–43. [Google Scholar] [CrossRef]
- Demirtürk, E. Lâle. 2009. Black Bodies, White Gazes: The Continuing Significance of Race. MELUS: Multi-Ethnic Literature of the US 34: 221–22. [Google Scholar] [CrossRef]
- Department of Health. 2009. Report on the Self-Reported Experience of Patients from Black and Minority Ethnic Groups. June. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/213375/BME-report-June-09-FINAL3.pdf (accessed on 14 January 2022).
- Dogra, Sufyan Abid, Kiran Rai, Sally Barber, Rosemary R. C. McEachan, Peymane Adab, and Laura Sheard. 2021. Delivering a childhood obesity prevention intervention using Islamic religious settings in the UK: What is most important to the stakeholders? Preventive Medicine Reports 22: 101387. [Google Scholar] [CrossRef]
- Eisenberger, Naomi. I., Mona Moieni, Tristen K. Inagaki, Keely. A. Muscatell, and Michael R. Irwin. 2017. In sickness and in health: The co-regulation of inflammation and social behavior. Neuropsychopharmacology 42: 242–53. [Google Scholar] [CrossRef]
- Elahi, Farah, and Omar Khan. 2017. Islamophobia: Still a Challenge for Us All. London: Runnymede Trust. [Google Scholar]
- Equality Act. 2010. Available online: https://www.gov.uk/guidance/equality-act-2010-guidance (accessed on 14 January 2022).
- Fecht, Daniela, Paul Fischer, Léa Fortunato, Gerard Hoek, Kees de Hoogh, Marten Marra, Hanneke Kruize, Danielle Vienneau, Rob Beelen, and Anna Hansell. 2015. Associations between air pollution and socioeconomic characteristics, ethnicity and age profile of neighbourhoods in England and the Netherlands. Environmental Pollution 198: 201–10. [Google Scholar] [CrossRef]
- Foucault, Michel. 2012. The Birth of the Clinic. London: Routledge. [Google Scholar]
- Gale, Richard. 2013. Religious residential segregation and internal migration: The British Muslim case. Environment and Planning A 45: 872–91. [Google Scholar] [CrossRef]
- Gamble, Vanessa Northington. 1997. Under the shadow of Tuskegee: African Americans and health care. American Journal of Public Health 87: 1773–78. [Google Scholar] [CrossRef] [PubMed]
- Hassan, Shaima M., Adele Ring, Naheed Tahir, and Mark Gabbay. 2021. The impact of COVID-19 social distancing and isolation recommendations for Muslim communities in North West England. BMC Public Health 21: 812. [Google Scholar] [CrossRef] [PubMed]
- Helliwell, John F., and Robert D. Putnam. 2004. The social context of well–being. Philosophical Transactions of the Royal Society of London. Series B: Biological Sciences 359: 1435–46. [Google Scholar]
- Home Office. 2021. Hate Crime, England and Wales 2020 to. 2021. Available online: https://www.gov.uk/government/statistics/hate-crime-england-and-wales-2020-to-2021/hate-crime-england-and-wales-2020-to-2021 (accessed on 14 January 2022).
- Intensive Care National Audit and Research Centre. 2020. ICNARC Report on COVID-19 in Critical Care. May 15. Available online: https://www.icnarc.org/DataServices/Attachments/Download/cbcb6217-f698-ea11-9125-00505601089b12 (accessed on 14 January 2022).
- Kakalia, Spenta, and Hasan H. Karrar. 2016. Polio, public health, and the new pathologies of militancy in Pakistan. Critical Public Health 26: 446–54. [Google Scholar] [CrossRef]
- Kluge, Hans Henri P., Zsuzsanna Jakab, Jozef Bartovic, Veronika d’Anna, and Santino Severoni. 2020. Refugee and migrant health in the COVID-19 response. The Lancet 395: 1237–39. [Google Scholar] [CrossRef]
- Kuzawa, Christopher W., and Elizabeth Sweet. 2009. Epigenetics and the embodiment of race: Developmental origins of US racial disparities in cardiovascular health. American Journal of Human Biology: The Official Journal of the Human Biology Association 21: 2–15. [Google Scholar]
- Laird, Lance D., Mona M. Amer, Elizabeth D. Barnett, and Linda L. Barnes. 2007. Muslim patients and health disparities in the UK and the US. Archives of Disease in Childhood 92: 922–26. [Google Scholar] [CrossRef]
- Lang, Jason, Judith McKie, Helen Smith, Angela McLaughlin, Christopher Gillberg, Paul G. Shiels, and Helen Minnis. 2020. Adverse childhood experiences, epigenetics and telomere length variation in childhood and beyond: A systematic review of the literature. European Child & Adolescent Psychiatry 29: 1329–38. [Google Scholar]
- Lapp, Hannah E., Sarah Ahmed, Celia L. Moore, and Richard G. Hunter. 2019. Toxic stress history and hypothalamic-pituitary-adrenal axis function in a social stress task: Genetic and epigenetic factors. Neurotoxicology and Teratology 71: 41–49. [Google Scholar] [CrossRef]
- Larson, Heidi, Alexandre de Figueiredo, Emilie Karafillakis, and Mahesh Rawal. 2018. State of vaccine confidence in the EU. Luxembourg: Publications Office of the European Union 10: 241099. [Google Scholar]
- LaVeist, Thomas A., Lydia A. Isaac, and Karen Patricia Williams. 2009. Mistrust of health care organizations is associated with underutilization of health services. Health Services Research 44: 2093–105. [Google Scholar] [CrossRef]
- Lewis, Tené T., Allison E. Aiello, Sue Leurgans, Jeremiah Kelly, and Lisa L. Barnes. 2010. Self-reported experiences of everyday discrimination are associated with elevated C-reactive protein levels in older African-American adults. Brain, Behavior, and Immunity 24: 438–43. [Google Scholar] [CrossRef] [PubMed]
- Liu, Yun-Zi, Yun-Xia Wang, and Chun-Lei Jiang. 2017. Inflammation: The common pathway of stress-related diseases. Frontiers in Human Neuroscience 11: 316. [Google Scholar] [CrossRef] [PubMed]
- Lockyer, Bridget, Shahid Islam, Aamnah Rahman, Josie Dickerson, Kate Pickett, Trevor Sheldon, and Bradford Institute for Health Research Covid-19 Scientific Advisory Group. 2021. Understanding COVID-19 misinformation and vaccine hesitancy in context: Findings from a qualitative study involving citizens in Bradford, UK. Health Expectations 24: 1158–67. [Google Scholar] [CrossRef]
- Mahase, Elisabeth. 2020. COVID-19: Tighter restrictions imposed in the north of England as cases spike. BMJ, 370. [Google Scholar] [CrossRef]
- Mbembe, Achille. 2008. Necropolitics. In Foucault in an Age of Terror. London: Palgrave Macmillan, pp. 152–82. [Google Scholar]
- Miller, Maria. 2016. Employment Opportunities for Muslims in the UK. Report of The Parliamentary Women’s and Equalities Committee. London: House of Commons. [Google Scholar]
- Modood, Tariq, and Simon Thompson. 2021. Othering, Alienation and Establishment. Political Studies 70: 780–96. [Google Scholar] [CrossRef]
- Muslim Census. 2020. Financial Impact of COVID-19 on the Muslim Community. Available online: https:/muslimcensus.co.uk/financial-impact-of-covid-19-on-the-muslim-community (accessed on 18 November 2020).
- Muslim Doctors Association (MDA). 2020. Muslim NHS Heroes Gallery. Available online: https://muslimdoctors.org/muslim-nhs-heroes/ (accessed on 14 January 2022).
- Muslim Doctors Association (MDA). 2021. Policy and reports. London. Available online: https://muslimdoctors.org/wp-content/uploads/2021/02/Impact-of-COVID-19-on-the-Muslim-Community.pdf (accessed on 14 January 2022).
- Office for National Statistics. 2020a. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/coronaviruscovid19relateddeathsbyreligiousgroupenglandandwales/2marchto15may2020 (accessed on 14 January 2022).
- Office for National Statistics. 2020b. Available online: https://www.gov.uk/government/publications/covid-19-reported-sars-cov-2-deaths-in-england/covid-19-confirmed-deaths-in-england-to-31-july-2021-report#ethnicity (accessed on 14 January 2022).
- Office for National Statistics. 2020c. Deaths Involving COVID-19 by Local Area and Socioeconomic Deprivation: Deaths Occurring between 1 March and 31 July. 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19bylocalareasanddeprivation/deathsoccurringbetween1marchand31july2020 (accessed on 14 January 2022).
- Office for National Statistics. 2021a. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/articles/updatingethniccontrastsindeathsinvolvingthecoronaviruscovid19englandandwales/24january2020to31march2021 (accessed on 14 January 2022).
- Office for National Statistics. 2021b. Prevalene of Ongoing Symptoms Following Coronavirus (COVID-19) Infection in the UK. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/alldatarelatingtoprevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk (accessed on 14 January 2022).
- Ojanuga, Durrenda. 1993. The medical ethics of the ‘father of gynaecology’, Dr J Marion Sims. Journal of Medical Ethics 19: 28–31. [Google Scholar] [CrossRef]
- Ong, Anthony D., Saarang Deshpande, and David R. Williams. 2017. Biological Consequences of Unfair Treatment: A Theoretical and Empirical Review. New York: Wiley-Blackwell. [Google Scholar]
- Osuafor, Christopher N., Catriona Davidson, Alistair J. Mackett, Marie Goujon, Lelane Van Der Poel, Vince Taylor, Jacobus Preller, Robert J. B. Goudie, and Victoria L. Keevil. 2021. Clinical Features, Inpatient Trajectories and Frailty in Older Inpatients with COVID-19: A Retrospective Observational Study. Geriatrics 6: 11. [Google Scholar] [CrossRef]
- Patel, Priti. 2017. Forced sterilization of women as discrimination. Public Health Reviews 38: 1–12. [Google Scholar] [CrossRef]
- Ponterotto, Diane. 2016. Resisting the male gaze: Feminist responses to the” normatization” of the female body in Western culture. Journal of International Women’s Studies 17: 133–51. [Google Scholar]
- Poole, Elizebeth, and Milly Williamson. 2021. Disrupting or reconfiguring racist narratives about Muslims? The representation of British Muslims during the Covid crisis. Journalism. [Google Scholar] [CrossRef]
- Race Disparities Unit. 2021. UK Government. Available online: https://www.gov.uk/government/publications/final-report-on-progress-to-address-covid-19-health-inequalities/final-report-on-progress-to-address-covid-19-health-inequalities#fn:5 (accessed on 14 January 2022).
- Rai, Kiran K., Sufyan Abid Dogra, Sally Barber, Peymane Adab, Carolyn Summerbell, and Childhood Obesity Prevention in Islamic Religious Settings’ Programme Management Group. 2019. A scoping review and systematic mapping of health promotion interventions associated with obesity in Islamic religious settings in the UK. Obesity Reviews 20: 1231–61. [Google Scholar] [CrossRef]
- Rashid, Rukhsana, Felisha Chong, Shahid Islam, Maria Bryant, and Rosemary R. C. McEachan. 2021. Taking a deep breath: A qualitative study exploring acceptability and perceived unintended consequences of charging clean air zones and air quality improvement initiatives amongst low-income, multi-ethnic communities in Bradford, UK. BMC Public Health 21: 1305. [Google Scholar] [CrossRef]
- Runnymede Trust. 1997. Islamophobia A Challenge for Us All. London: Runnymede Trust. [Google Scholar]
- Said, Edward. 1978. Orientalism: Western Concepts of the Orient. New York: Pantheon. [Google Scholar]
- Sealy, Thomas. 2021. Islamophobia: With or without Islam? Religions 12: 369. [Google Scholar] [CrossRef]
- Shahid, Hina. 2022. Islamophobia makes me sick! British muslim and health inequalities. In British Muslims, Ethnicity, Health Inequalities. Edited by Sufyan Dogra. Edinburgh: Edinburgh University Press. Available online: https://edinburghuniversitypress.com/book-british-muslims-ethnicity-and-health-inequalities.html (accessed on 14 January 2022).
- Shahid, Hina, Asma Khan, Jennifer Hall, Melanie Haith-Cooper, Anya Ahmed, and Sufyan Abid Dogra. Forthcoming. Gendered health inequalities and British Muslim women: An intersectional approach and analysis. In British Muslims, Ethnicity, Health Inequalities. Edited by Sufyan Dogra. Edinburgh: Edinburgh University Press.
- Shahid, Hina, and Hira Ali. 2021. Excluded on the Frontline: Discrimination, Racism and Islamophobia in the NHS. London: The Muslim Doctors Association. [Google Scholar]
- Singanayagam, Anika, Seran Hakki, Jake Dunning, Kieran J. Madon, Michael A. Crone, Aleksandra Koycheva, Nieves Derqui-Fernandez, Jack L. Barnett, Michael G. Whitfield, Robert Varro, and et al. 2022. Community transmission and viral load kinetics of the SARS-CoV-2 delta (B. 1.617. 2) variant in vaccinated and unvaccinated individuals in the UK: A prospective, longitudinal, cohort study. The Lancet Infectious Diseases 22: 183–95. [Google Scholar] [CrossRef]
- Singer, Merrill. 1994. AIDS and the health crisis of the US urban poor; the perspective of critical medical anthropology. Social Science & Medicine 39: 931–48. [Google Scholar]
- Singer, Merrill. 2000. A dose of drugs, a touch of violence, a case of AIDS: Conceptualizing the SAVA syndemic. Free Inquiry in Creative Sociology 28: 13–24. [Google Scholar]
- Singer, Merill, Nicola Bulled, Bayla Ostrach, and Emily Mendenhall. 2017. Syndemics and the biosocial conception of health. The Lancet 389: 941–50. [Google Scholar] [CrossRef]
- Szczepura, Ala, Charlotte Price, and Anil Gumber. 2008. Breast and bowel cancer screening uptake patterns over 15 years for UK south Asian ethnic minority populations, corrected for differences in socio-demographic characteristics. BMC Public Health 8: 346. [Google Scholar] [CrossRef]
- Taquet, Maxime, John R. Geddes, Masud Husain, Sierra Luciano, and Paul J. Harrison. 2021. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: A retrospective cohort study using electronic health records. The Lancet Psychiatry 8: 416–27. [Google Scholar] [CrossRef]
- Tell Mama. 2018. Gendered Anti-Muslim Hatred and Islamophobia. London: Faith Matters. Available online: https://tellmamauk.org/gendered-anti-muslim-hatred-and-islamophobia-street-based-aggression-in-cases-reported-to-tell-mama-is-alarming/ (accessed on 14 January 2022).
- Thayer, Zaneta M., and Christopher W. Kuzawa. 2011. Biological memories of past environments: Epigenetic pathways to health disparities. Epigenetics 6: 798–803. [Google Scholar] [CrossRef] [PubMed]
- Thorburn, Sheryl, Jenifer Kue, Karen Levy Keon, and Patela Lo. 2012. Medical mistrust and discrimination in health care: A qualitative study of Hmong women and men. Journal of Community Health 37: 822–29. [Google Scholar] [CrossRef] [PubMed]
- UK Government Scientific Advisory Group for Emergencies. 2020. Factors Influencing COVID-19 Vaccine Uptake among Minority Ethnic Groups. December 17. Available online: https://www.gov.uk/government/publications/factors-influencing-covid-19-vaccine-uptake-among-minority-ethnic-groups-17-december-2020 (accessed on 14 January 2022).
- UK Parliament. 2021. Nationality and Borders Bill. Available online: https://bills.parliament.uk/bills/3023 (accessed on 14 January 2022).
- Walker, Alex J., Brian MacKenna, Peter Inglesby, Laurie Tomlinson, Christopher T. Rentsch, Helen J. Curtis, Caroline E. Morton, Jessica Morley, Amir Mehrkar, Seb Bacon, and et al. 2021. Clinical coding of long COVID in English primary care: A federated analysis of 58 million patient records in situ using OpenSAFELY. medRxiv 71: e806-14. [Google Scholar]
- Williamson, Elizabeth J., Alex J. Walker, Krishnan Bhaskaran, Seb Bacon, Chris Bates, Caroline E. Morton, Helen J. Curtis, Amir Mehrkar, David Evans, Peter Inglesby, and et al. 2020. Factors associated with COVID-19-related death using OpenSAFELY. Nature 584: 430–36. [Google Scholar] [CrossRef]
- Wu, Qi, Lina Zhou, Xin Sun, Zhongfang Yan, Chunxiu Hu, Junping Wu, Long Xu, Xue Li, Huiling Li, Peiyuan Yin, and et al. 2017. Altered lipid metabolism in recovered SARS patients twelve years after infection. Scientific Reports 7: 9110. [Google Scholar] [CrossRef]
- Wu, Zunyou, and Jennifer M. McGoogan. 2020. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. Jama 323: 1239–42. [Google Scholar] [CrossRef]
Figure 1.
The syndemic of Islamophobia, social determinants of health and health inequities in the Muslim community in Britain.
Figure 1.
The syndemic of Islamophobia, social determinants of health and health inequities in the Muslim community in Britain.

Figure 2.
Moving beyond community engagement to community empowerment, adapted from (Osuafor et al. 2021).
Figure 2.
Moving beyond community engagement to community empowerment, adapted from (Osuafor et al. 2021).


{kind=link}
{kind=link}
Table 1.
Multilevel policy responses to mitigate risks and eliminate health inequities in the Muslim community in Britain.
Table 1.
Multilevel policy responses to mitigate risks and eliminate health inequities in the Muslim community in Britain.
| Level | Intervention |
|---|---|
| Governance, legislation and media |
|
| Social policies |
|
| Neighbourhood |
|
| Institutional (workplace) |
|
| Healthcare services |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Shahid, H.J.; Dogra, S.A. The Muslim Gaze and the COVID-19 Syndemic. Religions 2022, 13, 780. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13090780
AMA Style
Shahid HJ, Dogra SA. The Muslim Gaze and the COVID-19 Syndemic. Religions. 2022; 13(9):780. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13090780
Chicago/Turabian StyleShahid, Hina Javaid, and Sufyan Abid Dogra. 2022. "The Muslim Gaze and the COVID-19 Syndemic" Religions 13, no. 9: 780. https://0-doi-org.brum.beds.ac.uk/10.3390/rel13090780
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.