
Creative Intervention for Acrophobia Sufferers through AIVE Concept

 , , ,
, , ,
Abstract
:1. Introduction
2. Related Work
3. The AIVE Concept
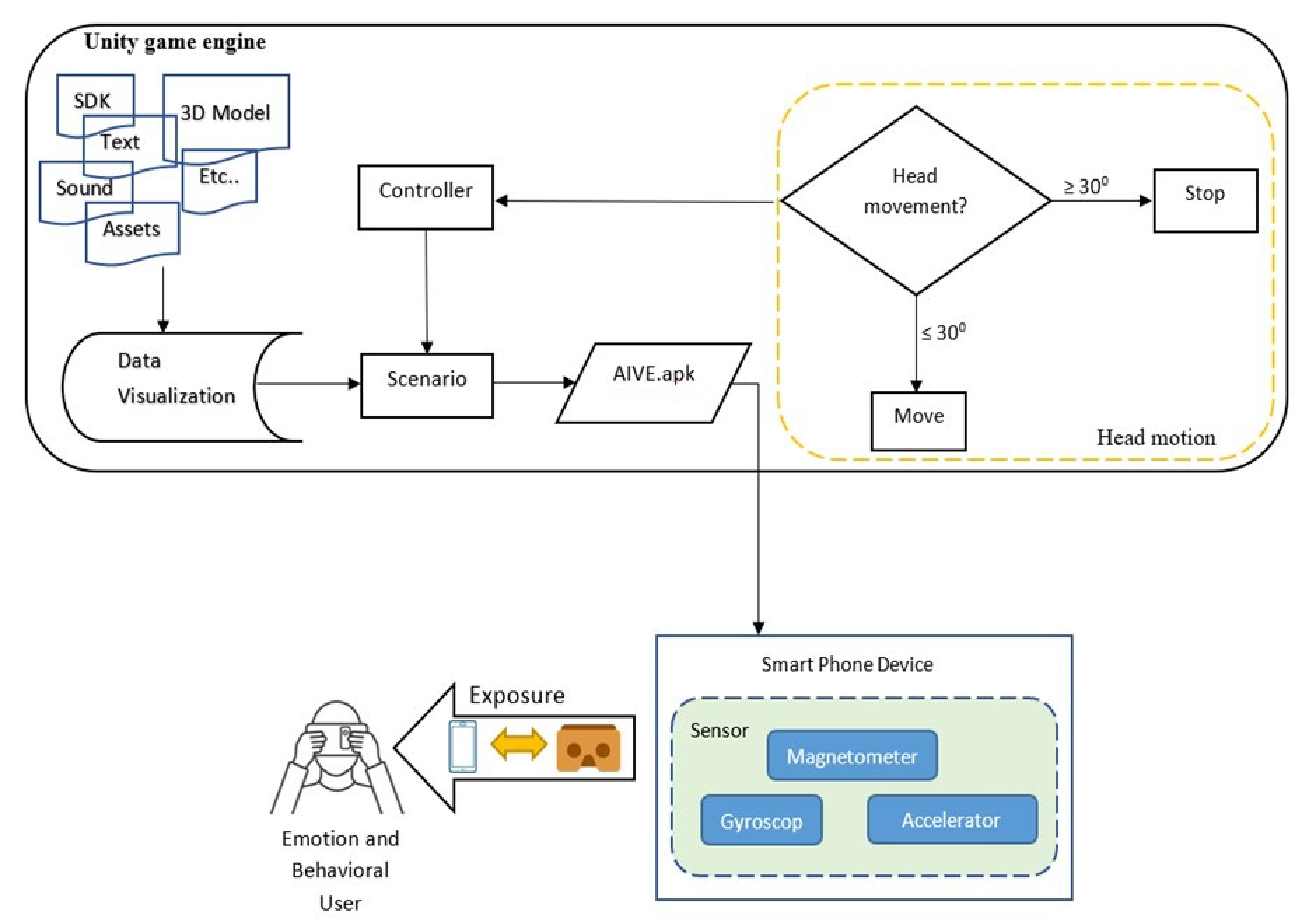
3.1. Acrophobia Immersive Virtual Environment (AIVE)
- Compatibility with standard format;
- Reliability, cross reference, and the need to design features;
- Loose modules are combined (where similar routines, modules, functions, and components are only implemented as needed and are not executed during launch and are being used on software applications);
- The module works cohesively [29].
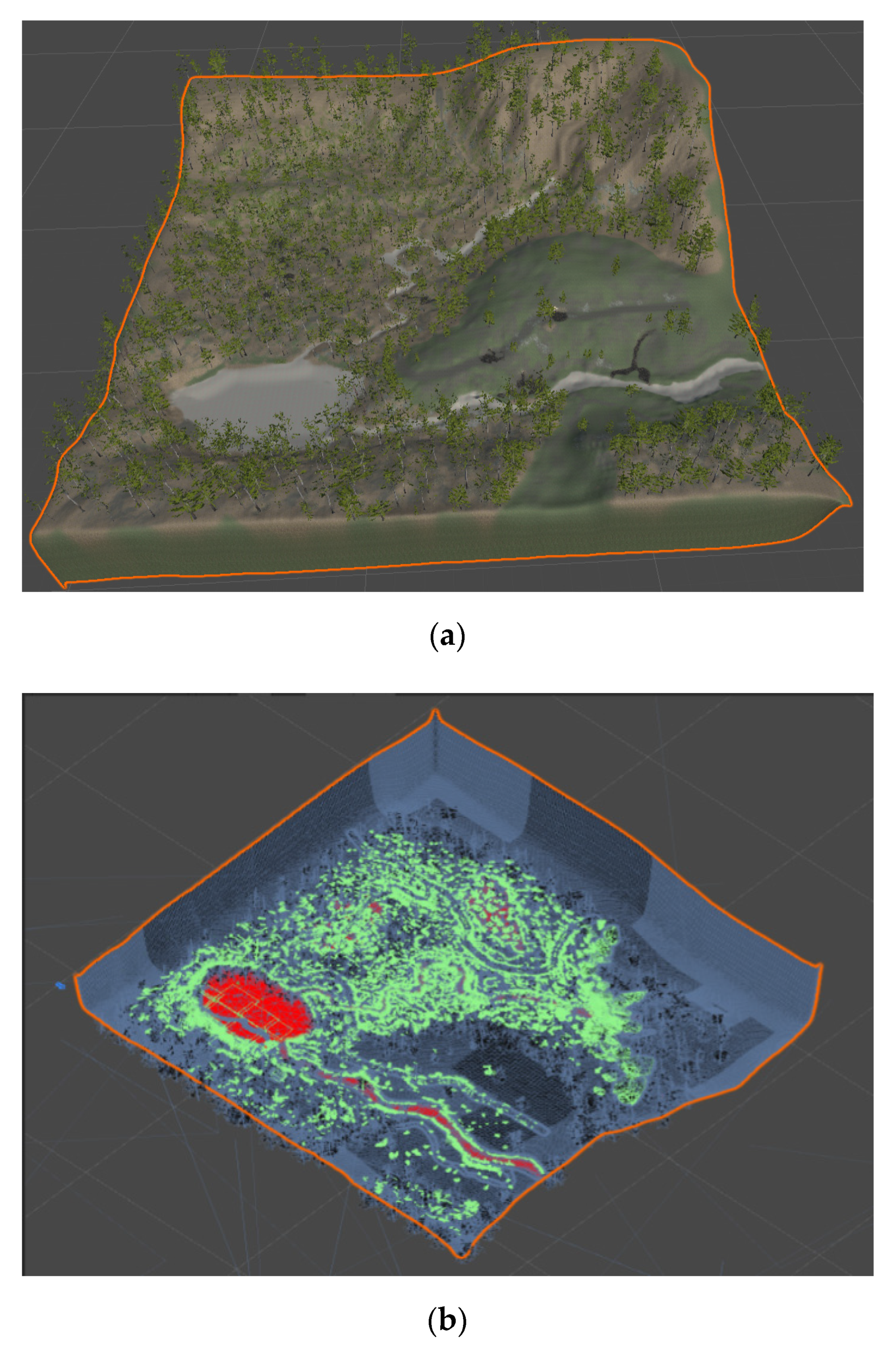
3.2. Design
- Nature Manufacture asset;
- Google VR;
- Digger;
- Toby Fredson.
3.3. Participants
- Firstly, the researcher gave instructions on the safety and health of the prospective participants before using the VR device. The instructions given were, users should be in good health and appropriate physical fitness to avoid unwanted side effects (headaches, dizziness, nausea, etc.);
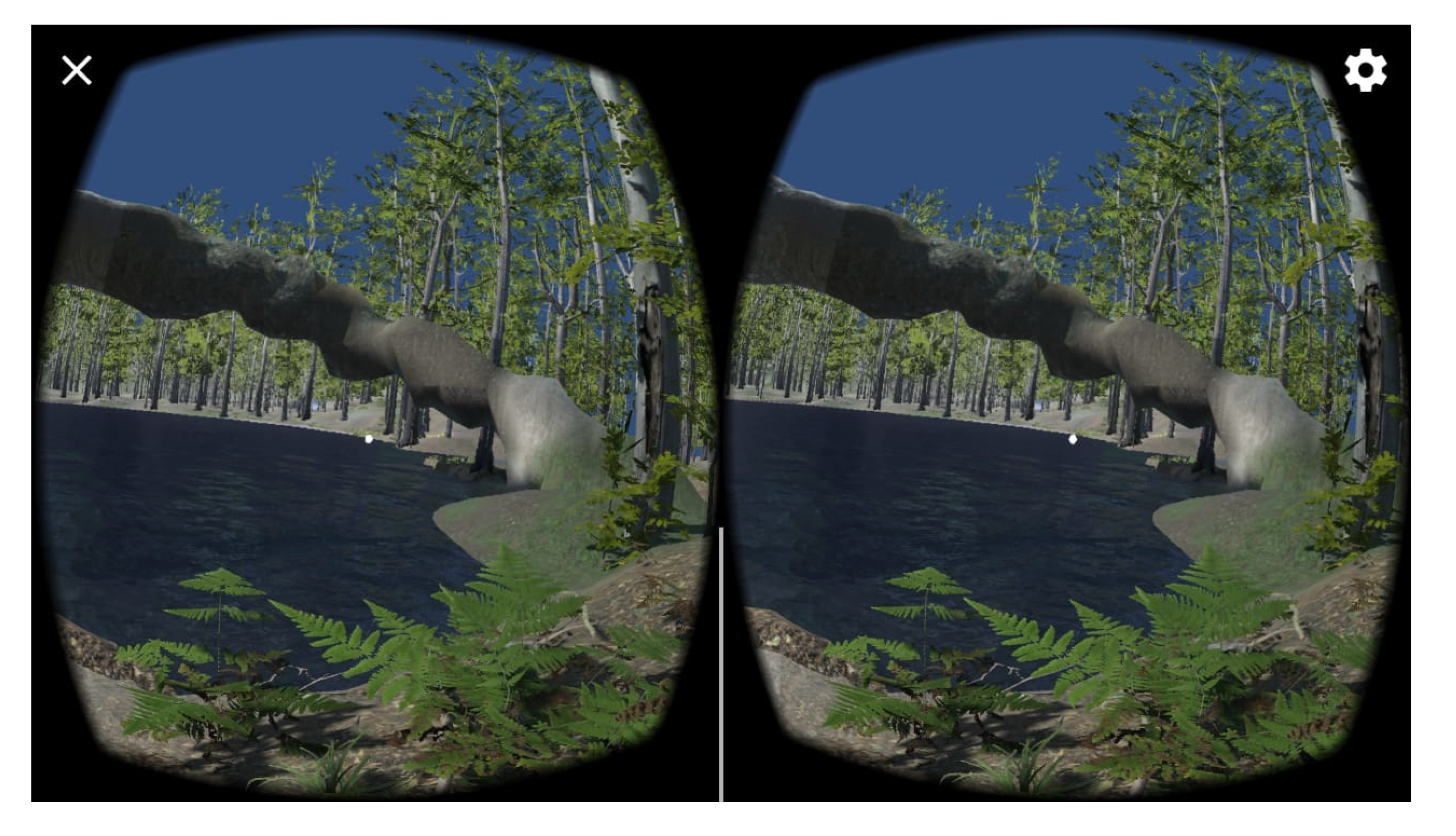
- Users tested the application using a mobile device that had been placed in cardboard;
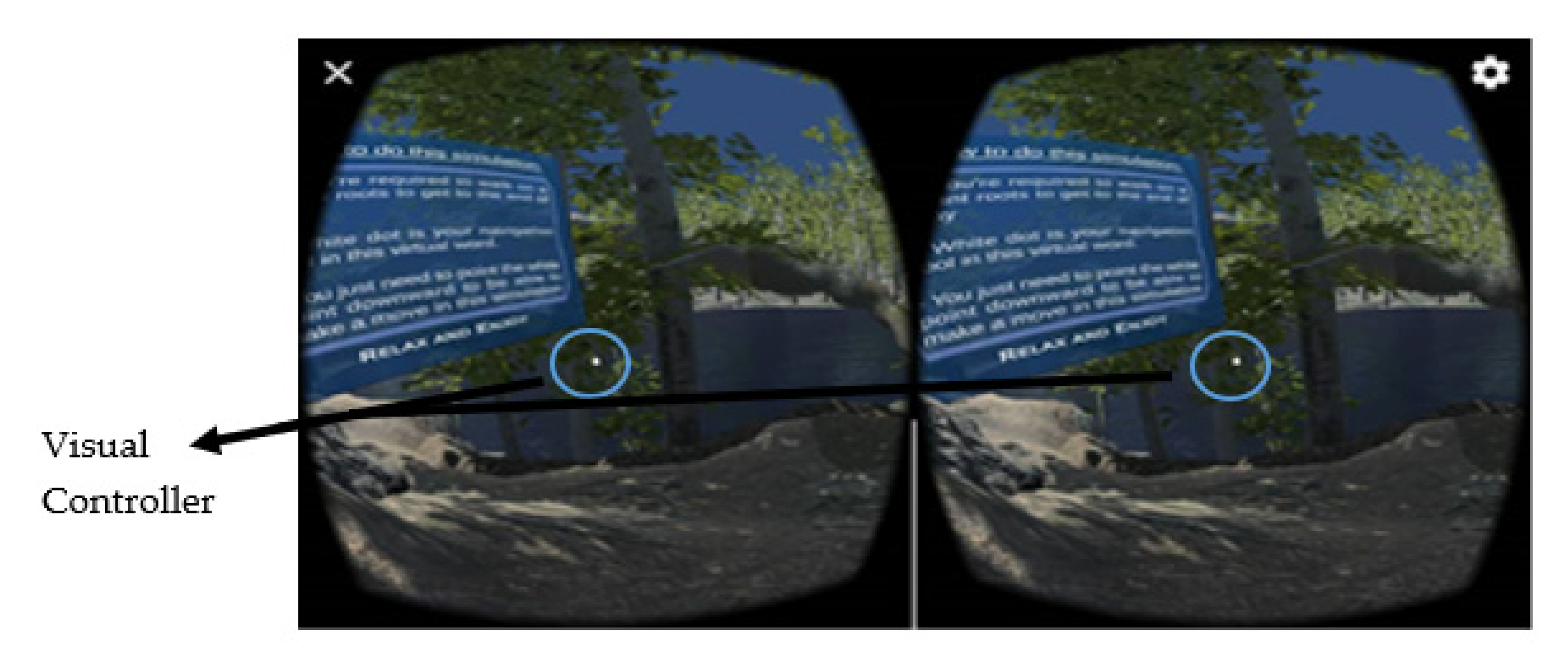
- While using it, the respondent should have read the instructions in the virtual environment created and executed the instructions comfortably and thoroughly;
- After using it, participants were asked to answer the questionnaire.
3.4. Instrument
4. Method
- −
- Natural conditions around which has been in the fox with the use of the Unity Asset;
- −
- Color, blur level, level of the graphic which is very different from the pre-test application.
- The magnetometer works to find out the direction of the user’s gaze;
- The accelerometer is used to determine the direction of the force of gravity;
- The gyroscope is used as a detector of the acceleration of the rotation of the user’s head angle.
5. Discussion
6. Conclusions
Author Contributions
Funding
Ethical Approval
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
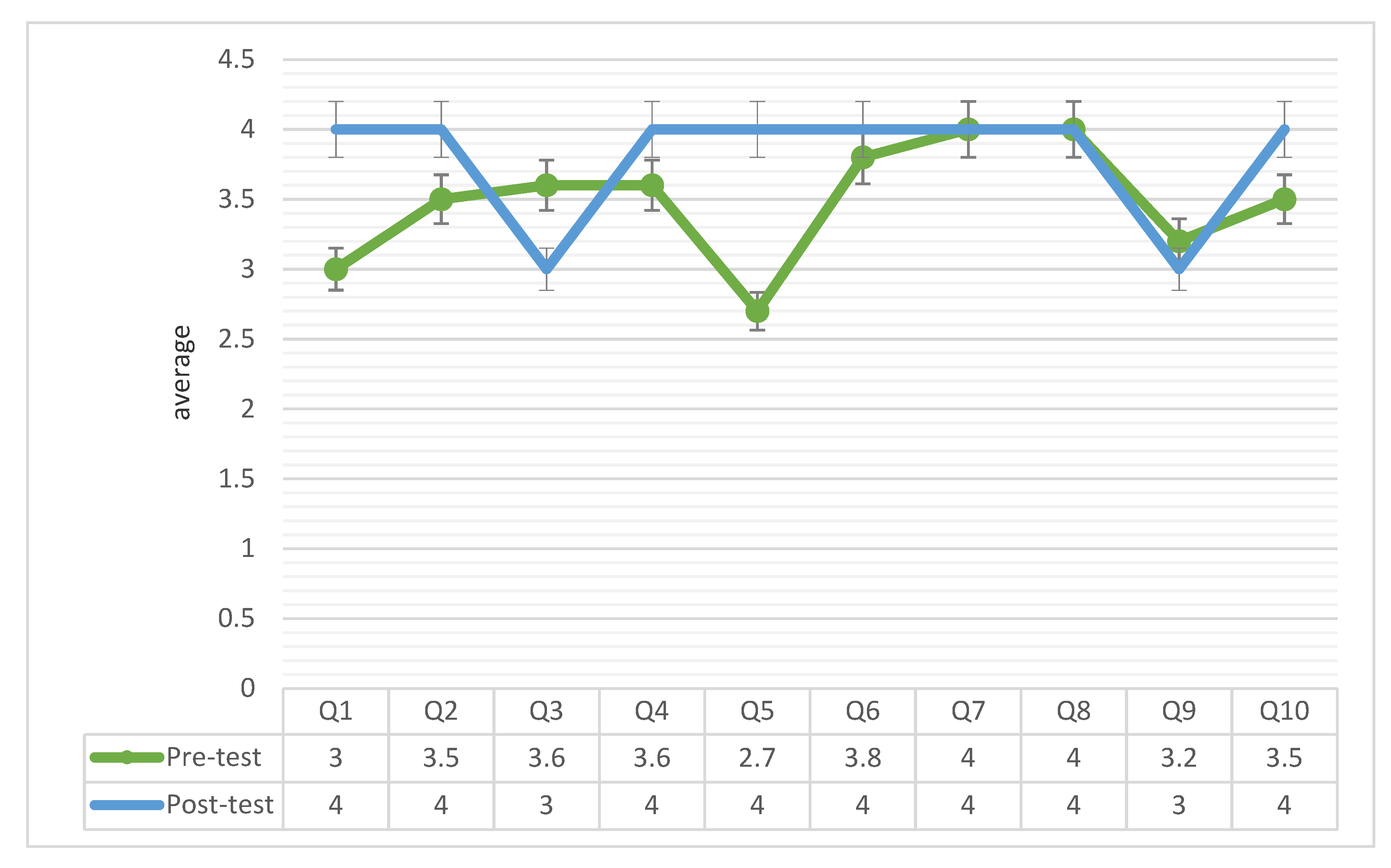
| Questions | Extremely Disagree (1) | Disagree (2) | Neutral (3) | Agree (4) | Extremely Agree (5) |
|---|---|---|---|---|---|
| I can navigate the application easily | |||||
| I can explore the environment more effectively. | |||||
| I feel comfortable while using the application. | |||||
| The use of virtual reality media is beneficial in therapy | |||||
| I am quite satisfied with the speed of the application displays while processing. | |||||
| The environment and objects are consistent. | |||||
| I am satisfied because the application can be used offline mode. | |||||
| Presenting material in the application does not make me confused. | |||||
| I will always use this application. | |||||
| The visualization result is comfortable. |
References
- Mahalil, I.; Rusli, M.E.; Yusof, A.M.; Yusof, M.Z.M.; Zainudin, A.R.R. Virtual reality-based technique for stress therapy. In Proceedings of the Engineering Technology and Technopreneuship (ICE2T), 2014 4th International Conference, Kuala Lumpur, Malaysia, 27–29 August 2014; pp. 295–300. [Google Scholar]
- Aboalsamh, H.; Hashim, H.A.; Alrashed, F.; Alkhamis, N. Virtual Reality System Specifications for Pain Management Therapy. In Proceedings of the Bioinformatics and Bioengineering (BIBE), 2011 IEEE 11th International Conference, Los Alamitos, CA, USA, 24–26 October 2011; pp. 143–147. [Google Scholar]
- Riva, G.; Baños, R.M.; Botella, C.; Mantovani, F.; Gaggioli, A. Transforming Experience: The Potential of Augmented Reality and Virtual Reality for Enhancing Personal and Clinical Change. Front. Psychiatry 2016, 7, 164. [Google Scholar] [CrossRef]
- Hagen, K.; Solem, S.; Opstad, H.B.; Vogel, P.A.; Kennair, L.E.O.; Kvale, G.; Hansen, B. Therapist variability in the task/goal dimension of the early working alliance predicts outcome in exposure and response prevention treatment for obsessive-compulsive disorder. Clin. Neuropsychiatry J. Treat. Eval. 2016, 13, 94–99. [Google Scholar]
- Hoffart, A.; Øktedalen, T.; Langkaas, T.F.; Wampold, B.E. Alliance and outcome in varying imagery procedures for PTSD: A study of within-person processes. J. Couns. Psychol. 2013, 60, 471–482. [Google Scholar] [CrossRef] [PubMed]
- Wheaton, M.G.; Huppert, J.D.; Foa, E.B.; Simpson, H.B. how important is the therapeutic alliance in treating obsessive-compulsive disorder with exposure and response prevention? An empirical report. Clin. Neuropsychiatry J. Treat. Eval. 2016, 13, 88–93. [Google Scholar]
- Gaggioli, A.; Ferscha, A.; Riva, G.; Dunne, S.; Viaud-Delmon, I. Human Computer Confluence: Transforming Human Experience Through Symbiotic Technologies; De Gruyter: Berlin, Germany, 2016. [Google Scholar]
- Müller, H.J.; Krummenacher, J. Visual search and selective attention. Vis. Cogn. 2006, 14, 389–410. [Google Scholar] [CrossRef]
- Sanchez-Vives, M.; Slater, M. From presence to consciousness through virtual reality. Nat. Rev. Neurosci. 2005, 6, 332–339. [Google Scholar] [CrossRef]
- Slater, M. Place illusion and plausibility can lead to realistic behaviour in immersive virtual environments. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 3549–3557. [Google Scholar] [CrossRef] [Green Version]
- Depla, M.F.I.A.; Have, M.L.T.; Van Balkom, A.J.L.M.; De Graaf, R. Specific fears and phobias in the general population: Results from the Netherlands Mental Health Survey and Incidence Study (NEMESIS). Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Milosevic., I.; McCabe., R.E. Phobias: The Psychology of Irrational Fear: The Psychology of Irrational Fear; ABC-CLIO: Santa Barbara, CA, USA, 2015; p. 444. [Google Scholar]
- Park, S.-C.; Kim, Y.-K. Anxiety Disorders in the DSM-5: Changes, Controversies, and Future Directions. In Anxiety Disorders: Rethinking and Understanding Recent Discoveries; Kim, Y.-K., Ed.; Springer: Singapore, 2020; pp. 187–196. [Google Scholar]
- Choy, Y.; Fyer, A.J.; Lipsitz, J.D. Treatment of specific phobia in adults. Clin. Psychol. Rev. 2007, 27, 266–286. [Google Scholar] [CrossRef] [PubMed]
- Teo, A.R. Phobias. In Encyclopedia of the Neurological Sciences, 2nd ed.; Aminoff, M.J., Daroff, R.B., Eds.; Academic Press: Oxford, Amsterdam, The Netherlands, 2014; pp. 890–891. [Google Scholar]
- Riddle-Walker, L.; Veale, D.; Chapman, C.; Ogle, F.; Rosko, D.; Najmi, S.; Walker, L.M.; MacEachern, P.; Hicks, T. Cognitive behaviour therapy for specific phobia of vomiting (Emetophobia): A pilot randomized controlled trial. J. Anxiety Disord. 2016, 43, 14–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joseph, A.; Chapman, M. Visual CBT: Using Pictures to Help You Apply Cognitive Behaviour Therapy to Change Your Life; Capstone: Mankato, MN, USA, 2013. [Google Scholar]
- Londero, A.; Viaud-Delmon, I.; Baskind, A.; Delerue, O.; Bertet, S.; Bonfils, P.; Warusfel, O. Auditory and visual 3D virtual reality therapy for chronic subjective tinnitus: Theoretical framework. Virtual Real. 2010, 14, 143–151. [Google Scholar] [CrossRef] [Green Version]
- Rosa, P.J.; Esteves, F.; Arriaga, P. Beyond Traditional Clinical Measurements for Screening Fears and Phobias. IEEE Trans. Instrum. Meas. 2015, 64, 3396–3404. [Google Scholar] [CrossRef]
- Lindner, P.; Miloff, A.; Bergman, C.; Andersson, G.; Hamilton, W.; Carlbring, P. Gamified, Automated Virtual Reality Exposure Therapy for Fear of Spiders: A Single-Subject Trial Under Simulated Real-World Conditions. Front. Psychiatry 2020, 11, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langhoff, C.; Baer, T.; Zubraegel, D.; Linden, M. Therapist–Patient Alliance, Patient–Therapist Alliance, Mutual Therapeutic Alliance, Therapist–Patient Concordance, and Outcome of CBT in GAD. J. Cogn. Psychother. 2008, 22, 68–79. [Google Scholar] [CrossRef]
- Miloff, A.; Lindner, P.; Dafgård, P.; Deak, S.; Garke, M.; Hamilton, W.; Heinsoo, J.; Kristoffersson, G.; Rafi, J.; Sindemark, K.; et al. Automated virtual reality exposure therapy for spider phobia vs. in-vivo one-session treatment: A randomized non-inferiority trial. Behav. Res. Ther. 2019, 118, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Botella, C.; Pérez-Ara, M.Á.; Bretón-López, J.; Quero, S.; García-Palacios, A.; Baños, R.M. In Vivo versus Augmented Reality Exposure in the Treatment of Small Animal Phobia: A Randomized Controlled Trial. PLoS ONE 2016, 11, e0148237. [Google Scholar] [CrossRef] [Green Version]
- Bentz, D.; Wang, N.; Ibach, M.K.; Schicktanz, N.S.; Zimmer, A.; Papassotiropoulos, A.; de Quervain, D.J.F. Effectiveness of a stand-alone, smartphone-based virtual reality exposure app to reduce fear of heights in real-life: A randomized trial. Npj Digit. Med. 2021, 4, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Boeldt, D.; McMahon, E.; Mcfaul, M.; Greenleaf, W. Using Virtual Reality Exposure Therapy to Enhance Treatment of Anxiety Disorders: Identifying Areas of Clinical Adoption and Potential Obstacles. Front. Psychiatry 2019, 10, 773. [Google Scholar] [CrossRef] [Green Version]
- Hubona, G.S.; Shirah, G.W. Spatial Cues in 3D Visualization. In Ambient Intelligence for Scientific Discovery: Foundations, Theories, and Systems; Cai, Y., Ed.; Springer Berlin Heidelberg: Berlin, Heidelberg, 2005; pp. 104–128. [Google Scholar]
- Streicher, A.; Hoffmann, J.; Roller, W. VIEW: A Concept for an Immersive Virtual Reality Image Interpretation Workbench. In Proceedings of the International Conference on Theory and Practice in Modern Computing, MCCSIS 2019, Porto, Portugal, 16–18 July 2019. [Google Scholar]
- Tang, Y.M.; Ng, G.W.Y.; Chia, N.H.; So, E.H.K.; Wu, C.H.; Ip, W.H. Application of virtual reality (VR) technology for medical practitioners in type and screen (T&S) training. J. Comput. Assist. Learn. 2021, 37, 359–369. [Google Scholar] [CrossRef]
- Fleming, I. Chapter 3—Defining software quality characteristics to facilitate software quality control and software process improvement. In Software Quality Assurance; Mistrik, I., Soley, R., Ali, N., Grundy, J., Tekinerdogan, B., Eds.; Morgan Kaufmann: Boston, MA, USA, 2016; pp. 47–61. [Google Scholar]
- Riva, G. Virtual Reality in Clinical Psychology. Ref. Modul. Neurosci. Biobehav. Psychol. 2020, 978. [Google Scholar] [CrossRef]





| Questions | Respond | Frequency | Percentage |
|---|---|---|---|
| R1. Can this application assist your phobia treatment? | Agree | 13 | 65 |
| Disagree | 7 | 35 | |
| R2. Can this application motivate you to relax while in high condition? | Agree | 14 | 70 |
| Disagree | 6 | 30 | |
| R3. Is this application more effective for treatment than by conventional method? | Agree | 14 | 70 |
| Disagree | 6 | 30 | |
| R4. Is the application helpful for you? | Agree | 16 | 80 |
| Disagree | 4 | 20 | |
| R5. I prefer treatment with the Acrophobia Immersive Virtual Exposure (AIVE) application compared to medicine? | Agree | 12 | 60 |
| Disagree | 8 | 40 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hazidar, A.H.; Sulaiman, R.; Sharip, S.; Ganie, M.W.; Baharudin, A.; Abdul Hamid, H.; Mat Nayan, N. Creative Intervention for Acrophobia Sufferers through AIVE Concept. Information 2021, 12, 261. https://0-doi-org.brum.beds.ac.uk/10.3390/info12070261
Hazidar AH, Sulaiman R, Sharip S, Ganie MW, Baharudin A, Abdul Hamid H, Mat Nayan N. Creative Intervention for Acrophobia Sufferers through AIVE Concept. Information. 2021; 12(7):261. https://0-doi-org.brum.beds.ac.uk/10.3390/info12070261
Chicago/Turabian StyleHazidar, Al Hamidy, Riza Sulaiman, Shalisah Sharip, Meutia Wardhanie Ganie, Azlin Baharudin, Hamzaini Abdul Hamid, and Norshita Mat Nayan. 2021. "Creative Intervention for Acrophobia Sufferers through AIVE Concept" Information 12, no. 7: 261. https://0-doi-org.brum.beds.ac.uk/10.3390/info12070261