
Non-Invasive Classification of Blood Glucose Level for Early Detection Diabetes Based on Photoplethysmography Signal




Abstract
:1. Introduction
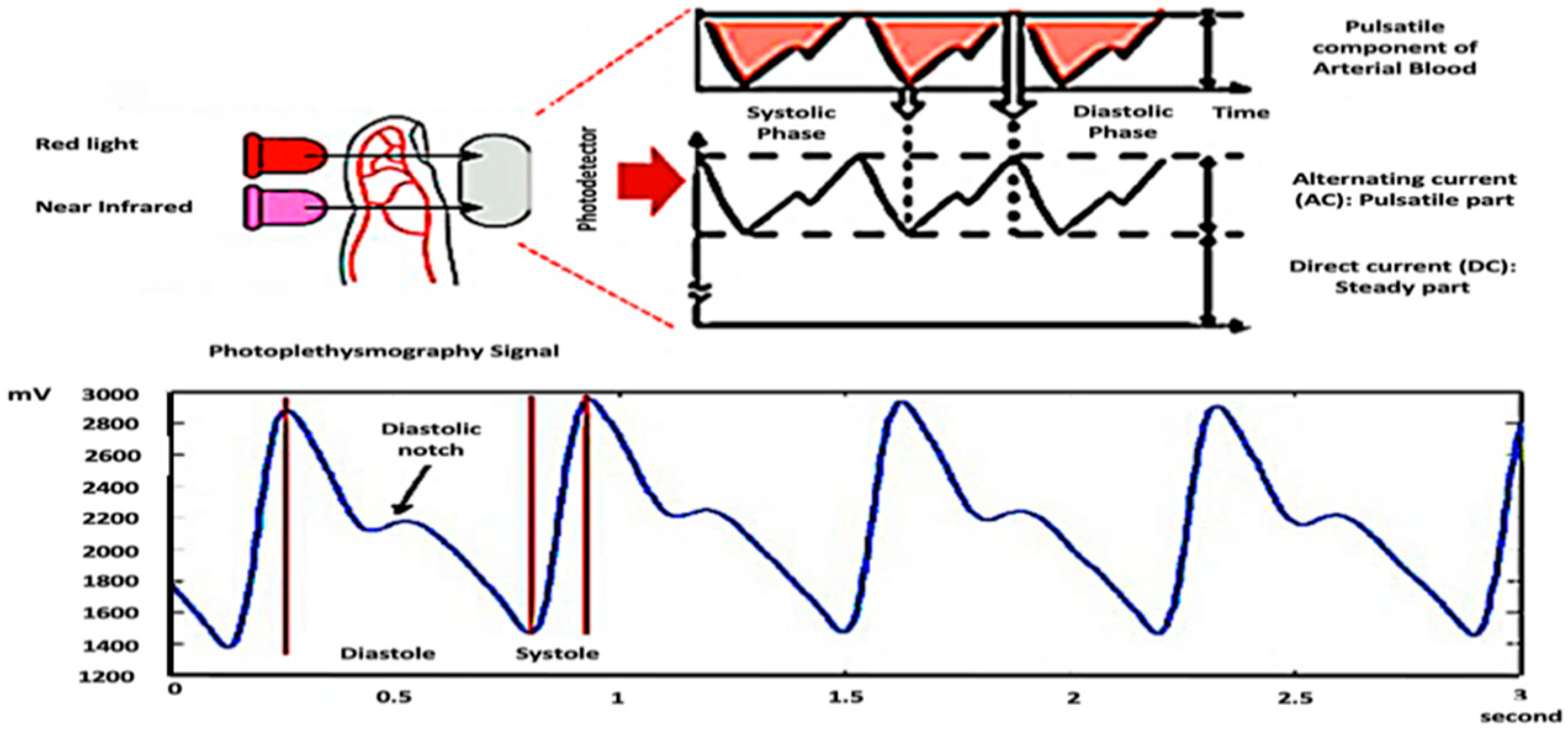
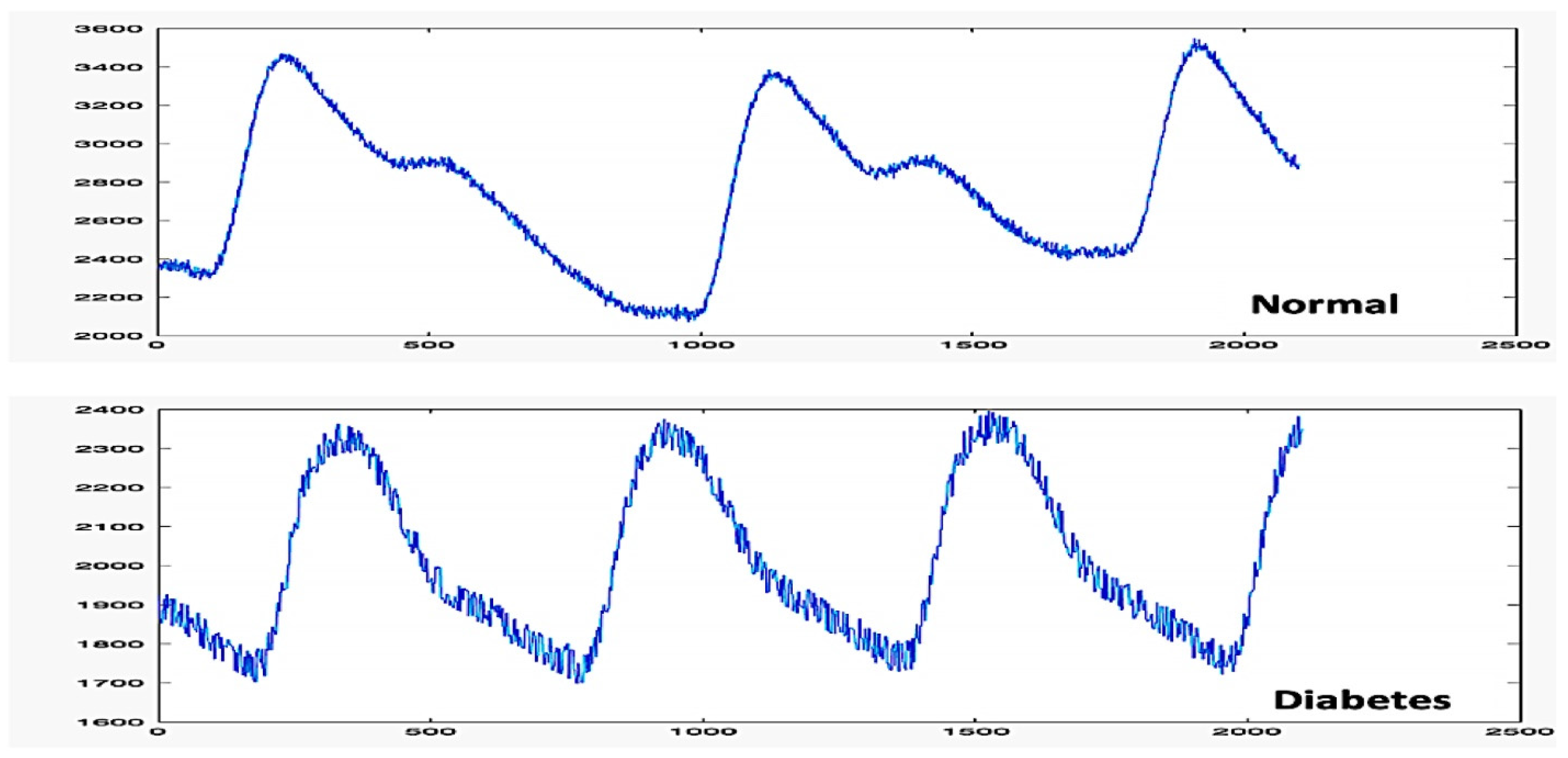
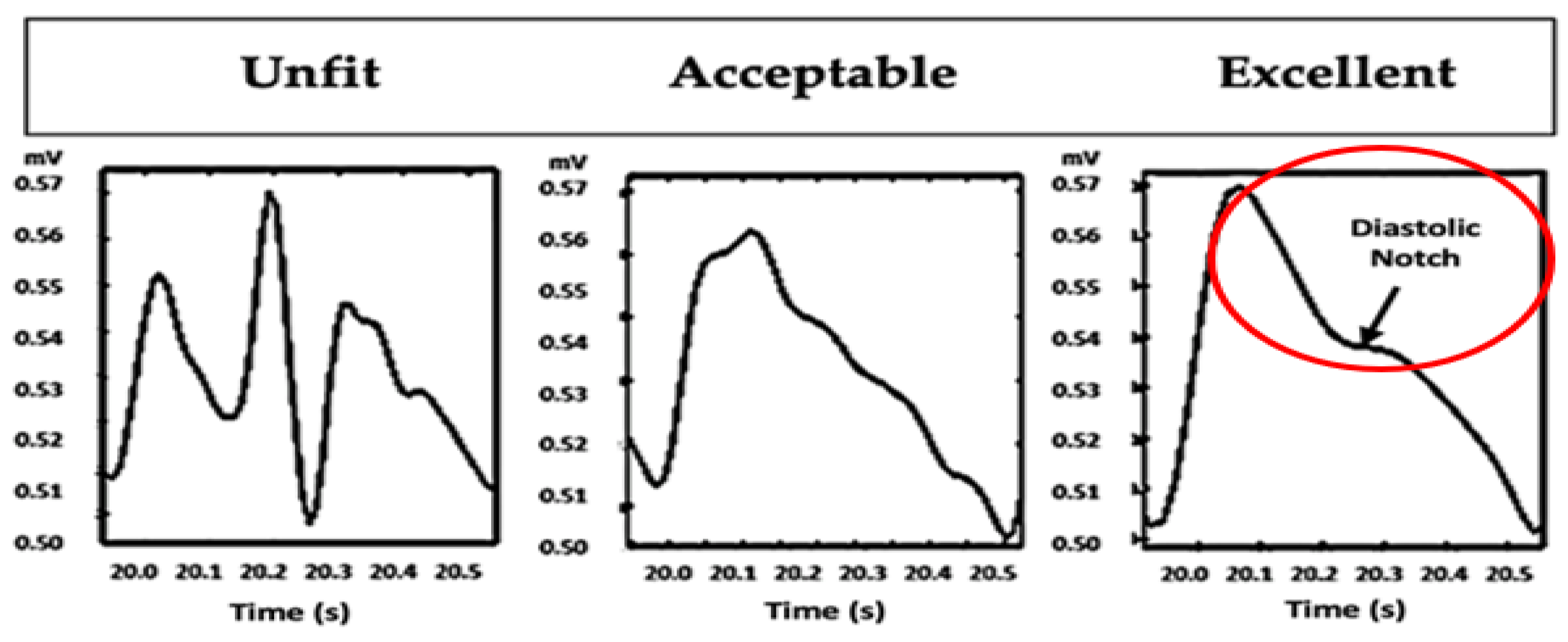
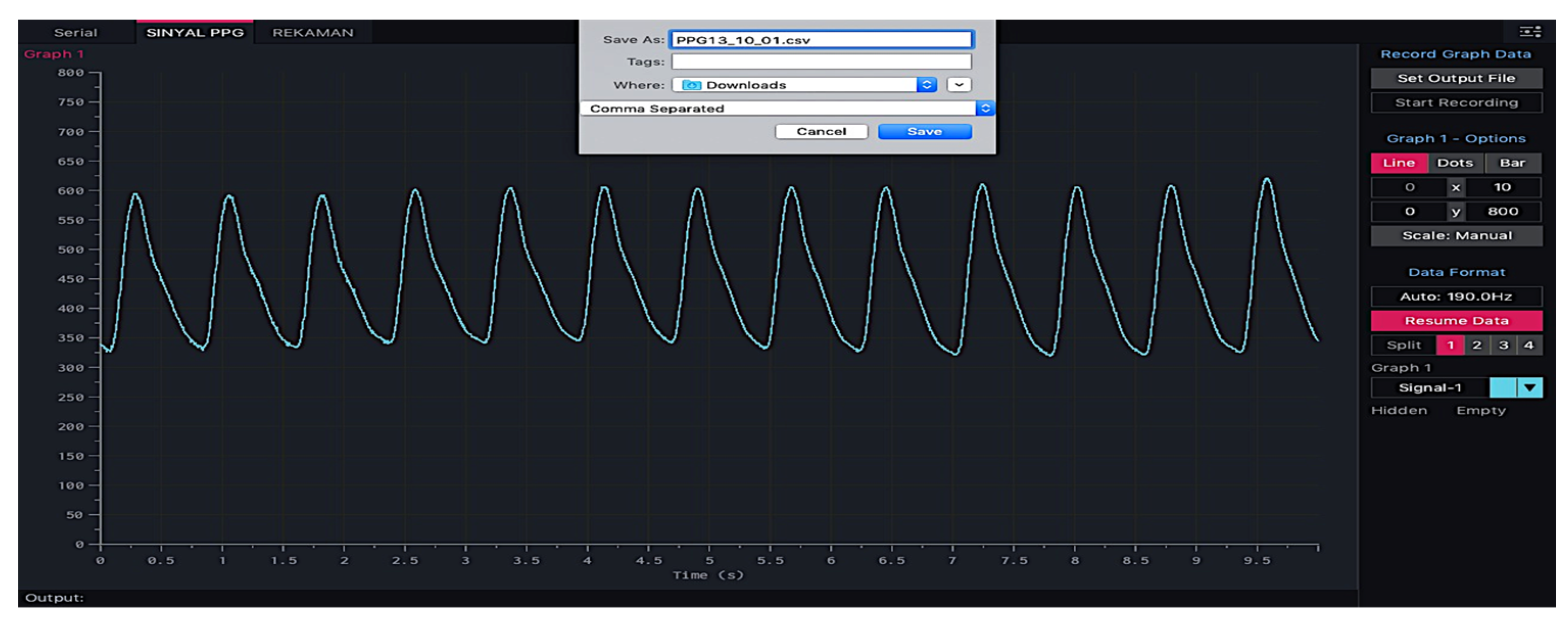
- The quality of the PPG waveform depends on the quality of the blood circulation.
- Characteristics of the PPG waveforms vary according to blood viscosity, vascular elasticity, and fluctuations in peripheral vascular resistance [37].
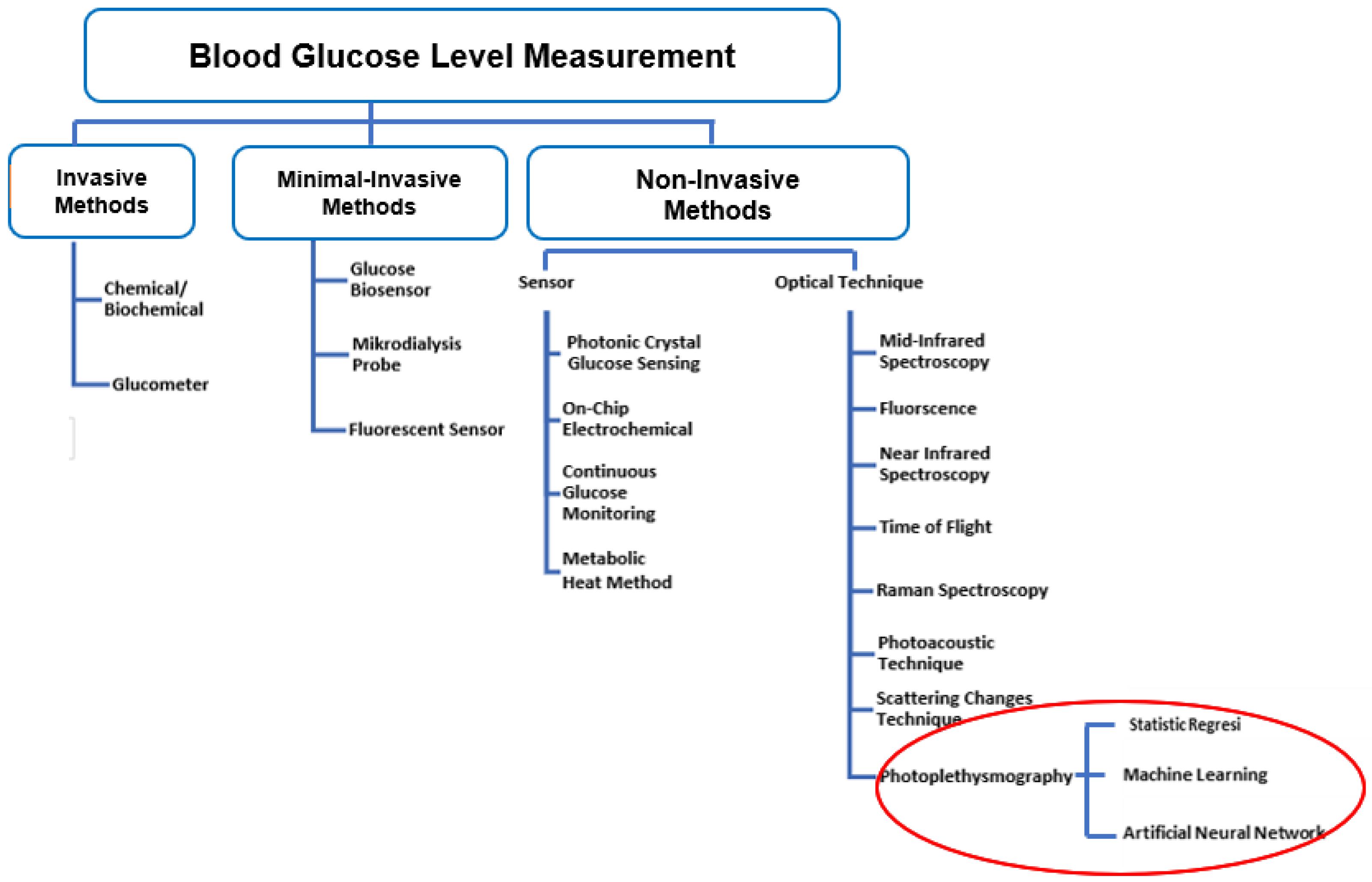
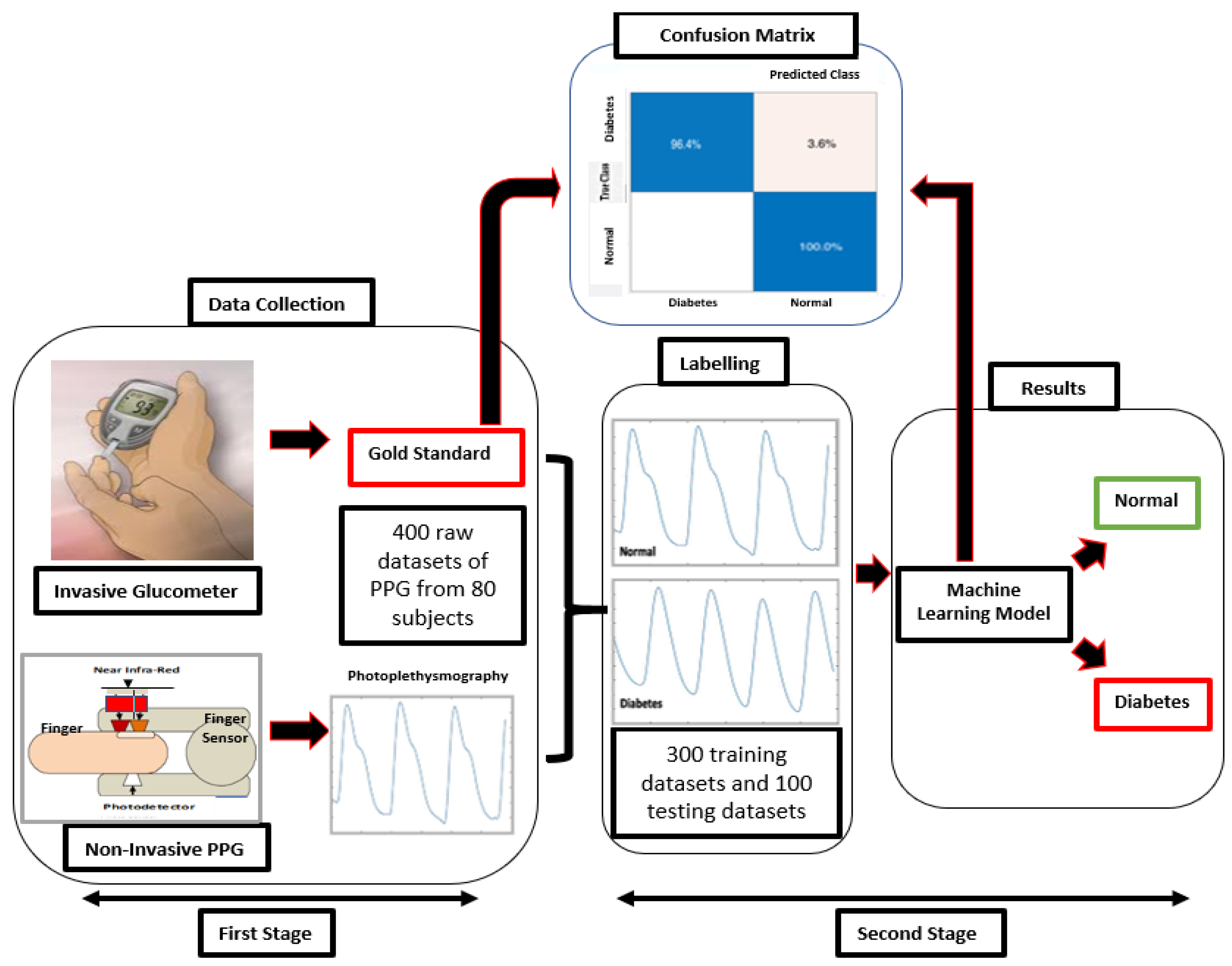
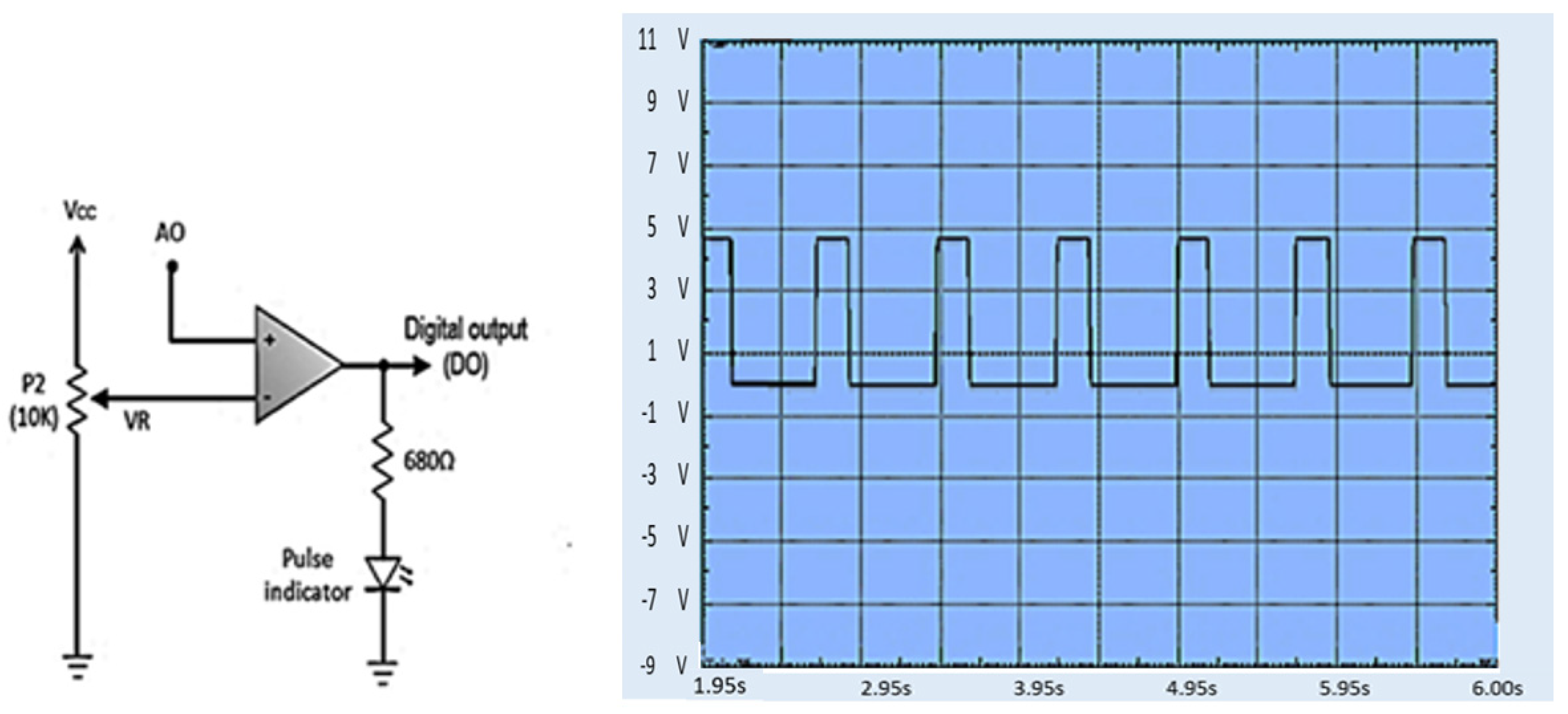
- With our proposed method, users can immediately know the condition of their blood BGL. We focus on a BGL classification based on the PPG signal. Therefore, in this study, two BGL levels were established: “normal” and “diabetes”.
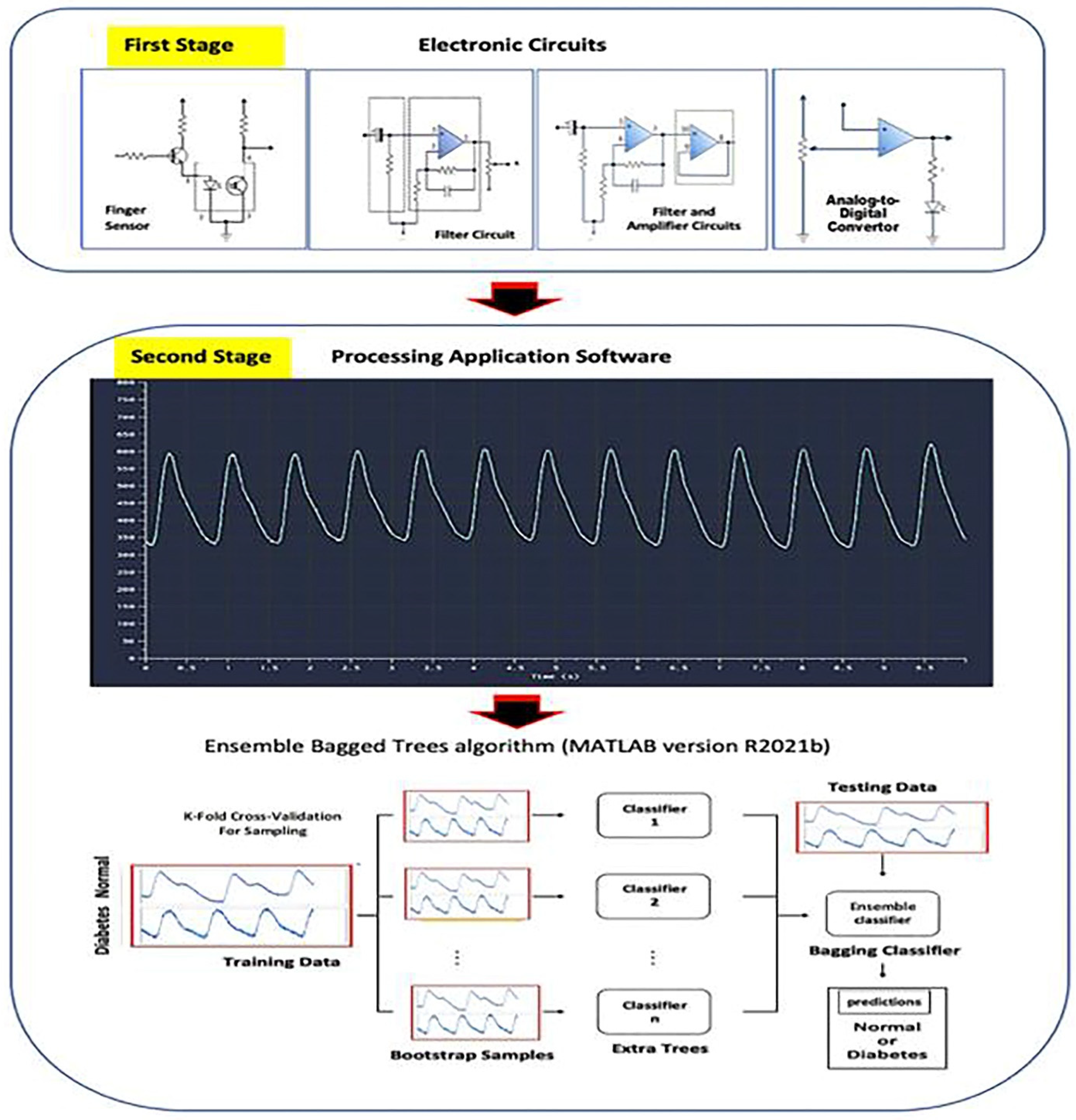
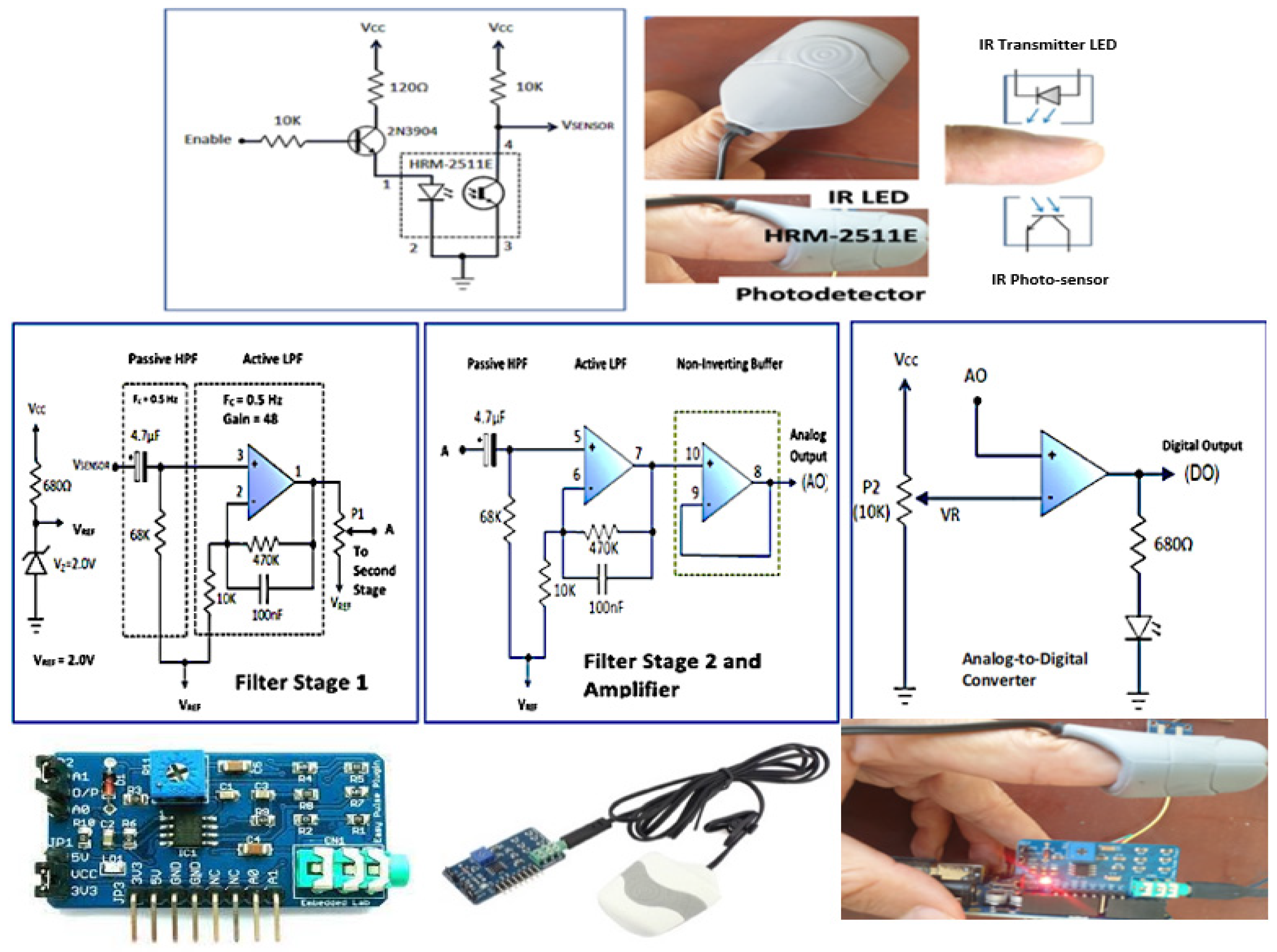
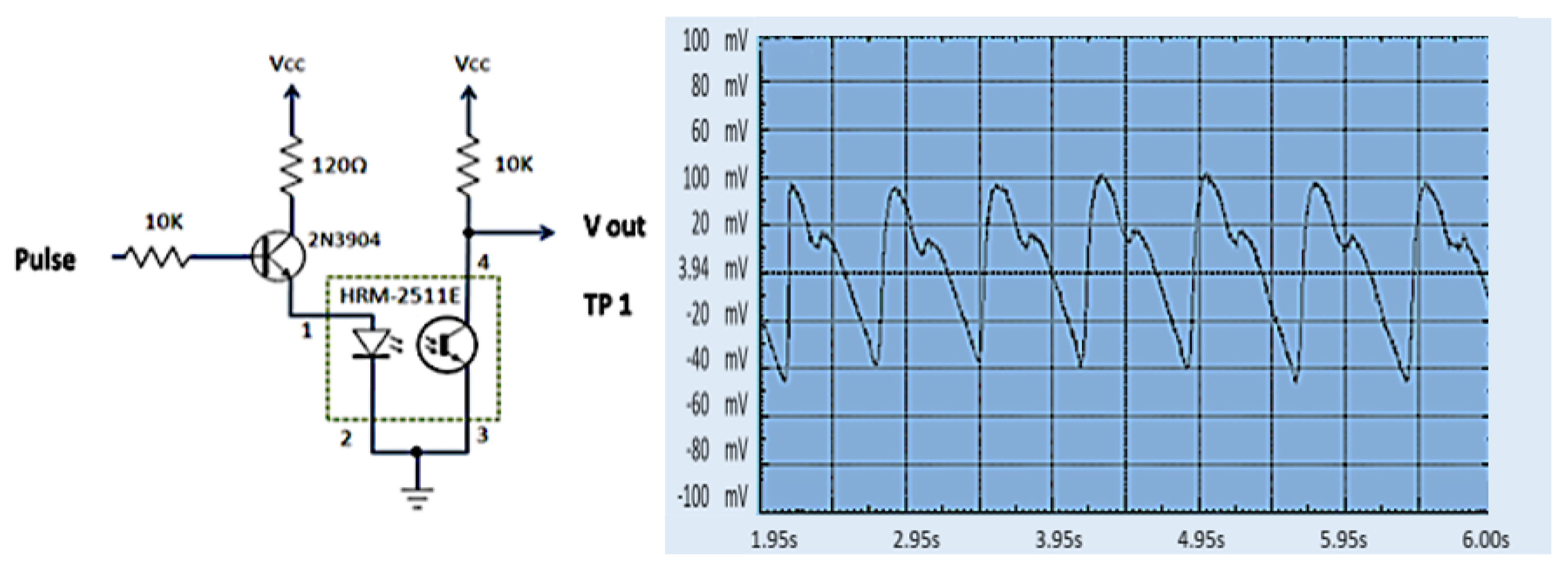
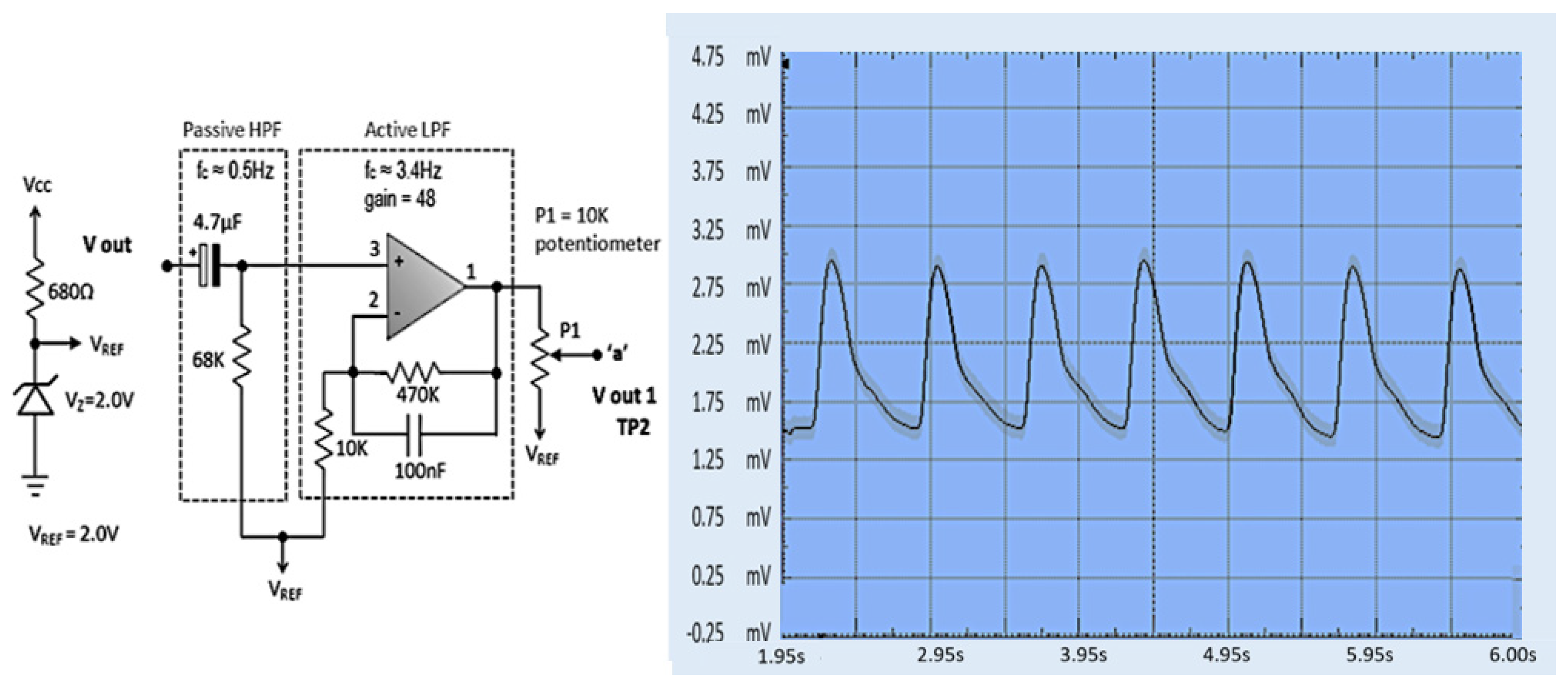
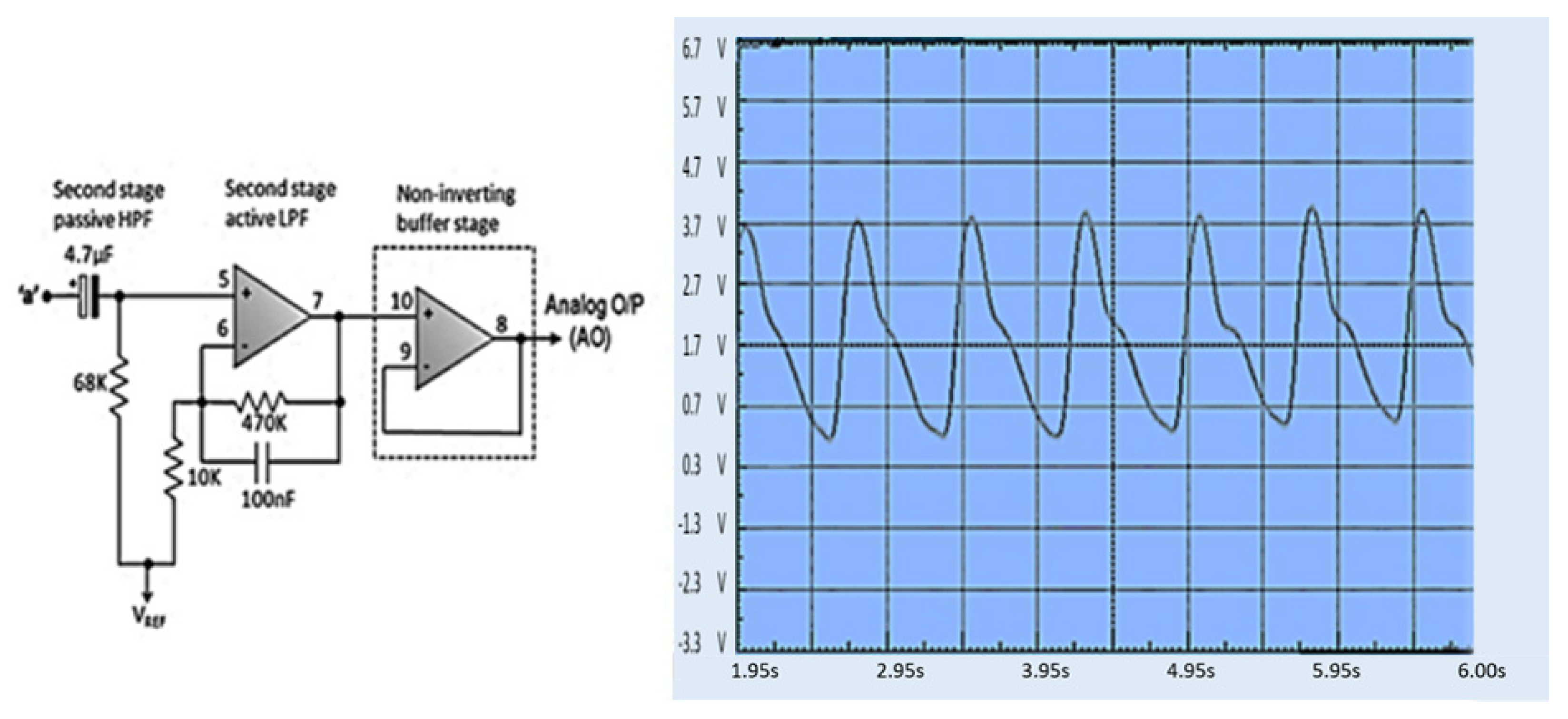
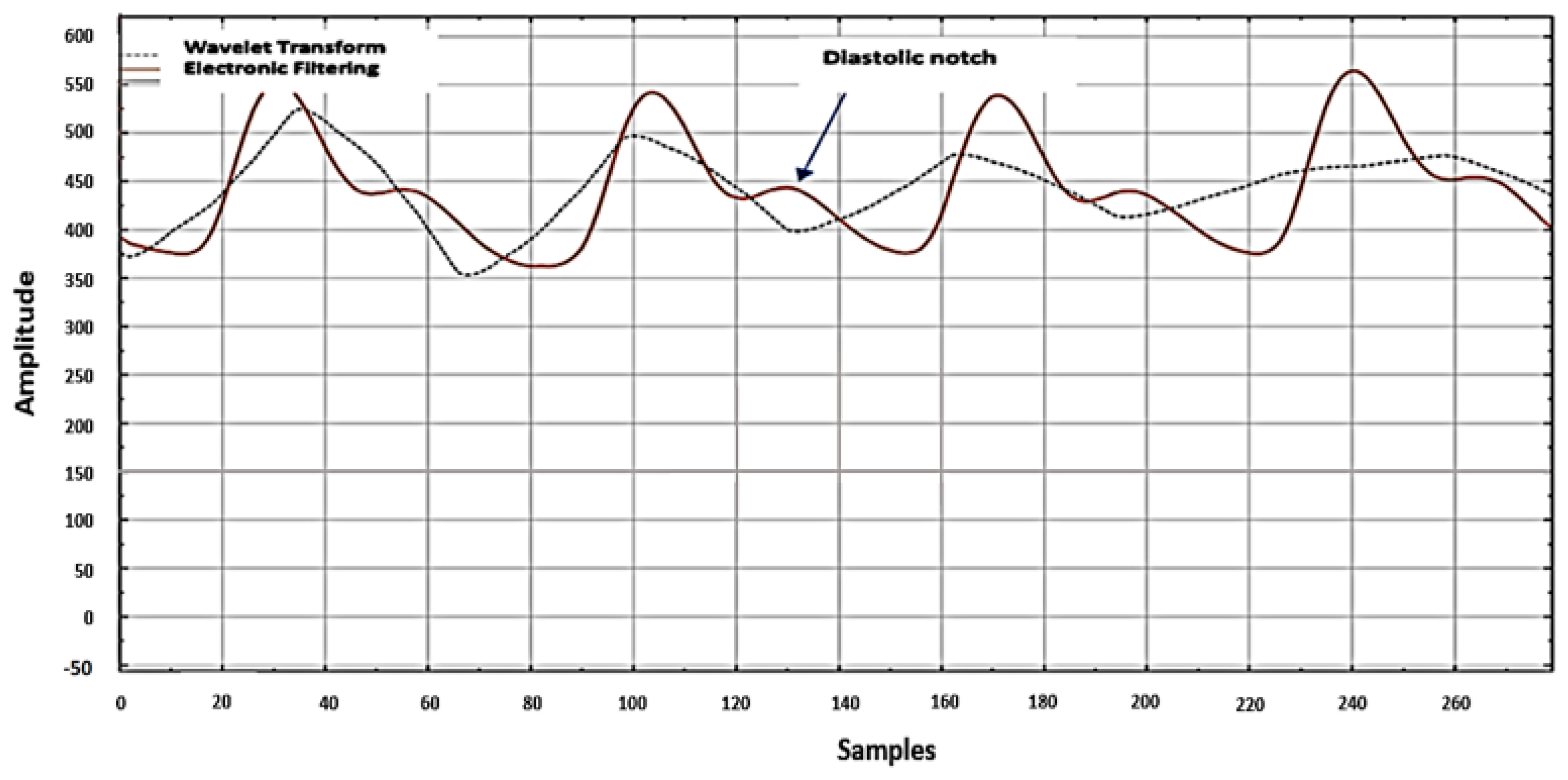
- A particular process is not needed to establish the PPG signal’s quality with our proposed method. We have used electronic filter circuits instead of filter algorithms such as wavelets.
- Our proposed method uses ML instead of DL to achieve a faster training time. Deep learning uses extensive computing power and takes a long time to train, making it difficult to validate and repeat extensively to improve results [47].
2. Materials and Methods
2.1. Data Collection
2.2. Electronic Circuits
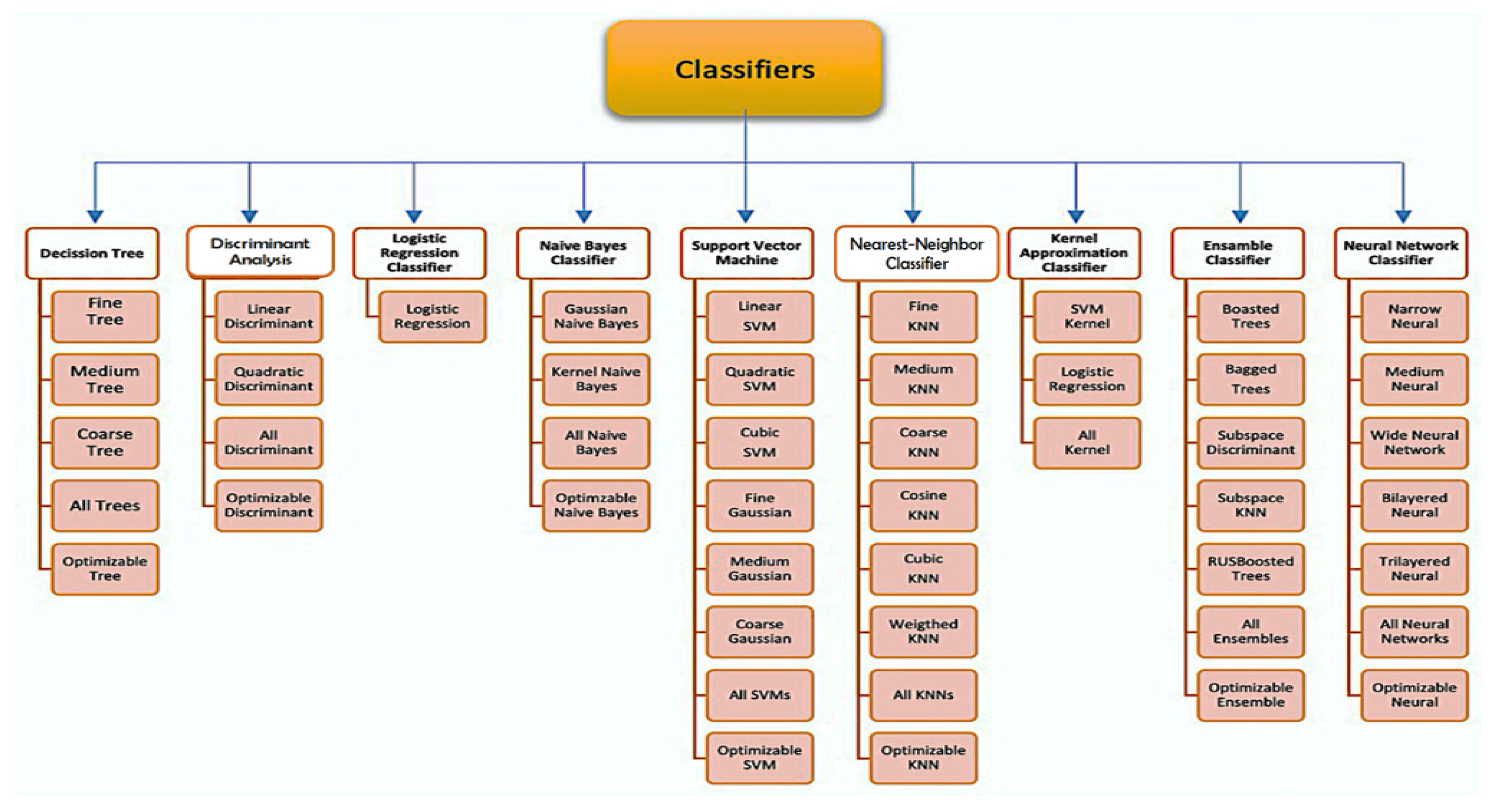
2.3. Classifier
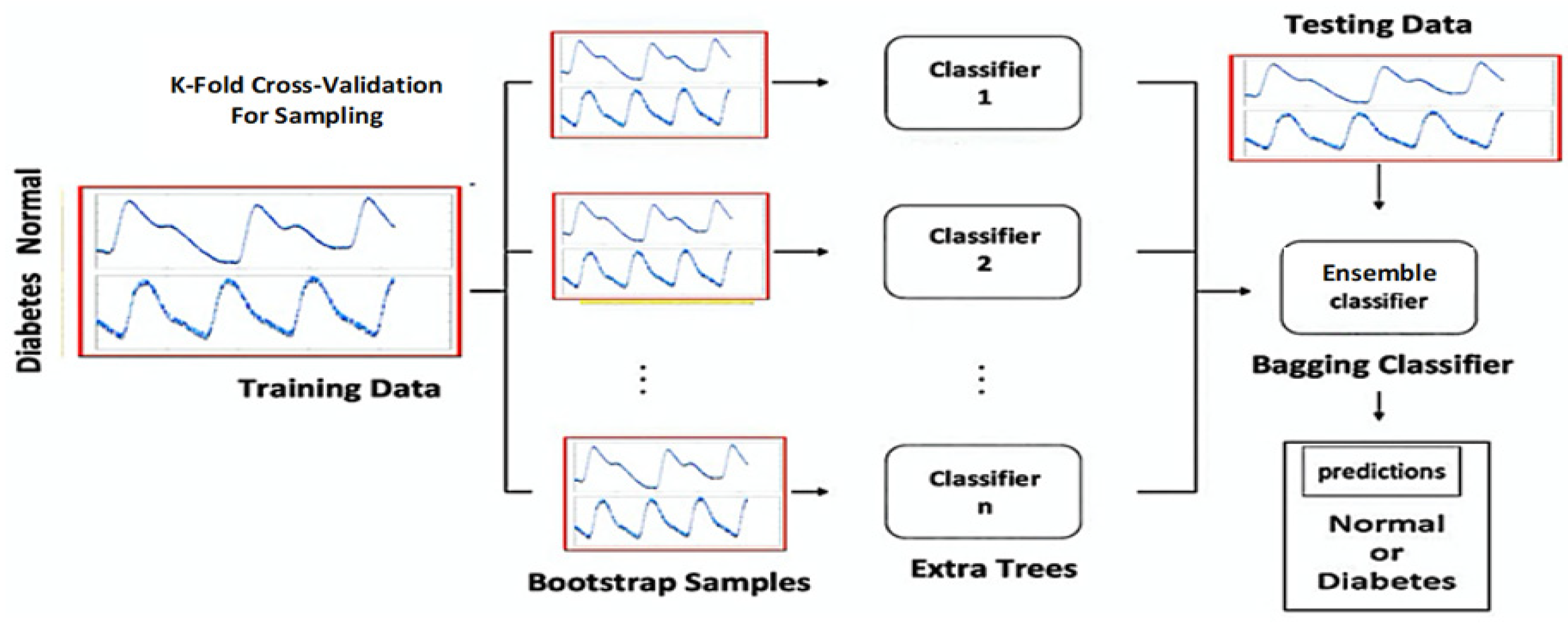
Ensemble Classification
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Clarke, S.; Foster, J. A history of blood glucose meters and their role in self-monitoring of diabetes mellitus. Br. J. Biomed. Sci. 2012, 69, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Galaviz, K.I.; Narayan, K.V.; Lobelo, F.; Weber, M.B. Lifestyle and the Prevention of Type 2 Diabetes: A Status Report. Am. J. Lifestyle Med. 2018, 12, 4–20. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. IDF Diabetes Atlas, 8th ed.; International Diabetes Federation: Brussel, Belgium, 2017; Available online: www.diabetesatlas.org (accessed on 24 November 2020).
- American Diabetes Association. (2) Classification and diagnosis of diabetes. Diabetes Care 2015, 38 (Suppl. 1), S8–S16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Big Picture: Checking Your Blood Sugar. Available online: https://www.diabetes.org/healthy-living/medication-treatments/blood-glucose-testing (accessed on 20 November 2020).
- Kirk, J.K.; Stegner, J. Self-monitoring of blood glucose: Practical aspects. J. Diabetes Sci. Technol. 2010, 4, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, E.M. Self-Monitoring of Blood Glucose: The Basics. Clin. Diabetes 2002, 20, 45–47. Available online: https://clinical.diabetesjournals.org/content/20/1/45.full-text.pdf (accessed on 10 November 2020). [CrossRef] [Green Version]
- Villena Gonzales, W.; Mobashsher, A.T.; Abbosh, A. The Progress of Glucose Monitoring-A Review of Invasive to Minimally and Non-Invasive Techniques, Devices and Sensors. Sensors 2019, 19, 800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, T. Non-Invasive Glucose Monitoring: A Review of Challenges and Recent Advances. Curr. Trends Biomed. Eng. Biosci. 2017, 6, 555696. [Google Scholar] [CrossRef]
- Tang, L.; Chang, S.J.; Chen, C.J.; Liu, J.T. Non-Invasive Blood Glucose Monitoring Technology: A Review. Sensors 2020, 20, 6925. [Google Scholar] [CrossRef]
- Poddar, R.; Andrews, J.T.; Shukla, P.; Sen, P. Non-Invasive Glucose Monitoring Techniques: A review and current trends. arXiv 2008, arXiv:0810.5755. Available online: https://www.researchgate.net/publication/210255819 (accessed on 24 November 2020).
- Khalil, O.S. Non-invasive glucose measurement technologies: An update from 1999 to the dawn of the new millennium. Diabetes Technol. Ther. 2004, 6, 660–697. [Google Scholar] [CrossRef]
- Tura, A.; Maran, A.; Pacini, G. Non-invasive glucose monitoring: Assessment of technologies and devices according to quantitative criteria. Diabetes Res. Clin. Pract. 2007, 77, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Moreno, E.M.; Lujan, M.J.; Rusinol, M.T.; Fernandez, P.J.; Manrique, P.N.; Trivino, C.A.; Miquel, M.P.; Rodriguez, M.A.; Burguillos, M.J. Type 2 Diabetes Screening Test by Means of a Pulse Oximeter. IEEE Trans. Biomed. Eng. 2017, 64, 341–351. [Google Scholar] [CrossRef]
- Shokrekhodaei, M.; Quinones, S. Review of Non-invasive Glucose Sensing Techniques: Optical, Electrical and Breath Acetone. Sensors 2020, 20, 1251. [Google Scholar] [CrossRef] [Green Version]
- Waynant, R.W.; Chenault, V.M. Overview of Non-Invasive Fluid Glucose Measurement Using Optical Techniques to Maintain Glucose Control in Diabetes Mellitus. IEEE LEOS Newsl. 1998, 12, 3–6. [Google Scholar]
- Moraes, J.L.; Rocha, M.X.; Vasconcelos, G.G.; Vasconcelos Filho, J.E.; de Albuquerque, V.H.C.; Alexandria, A.R. Advances in Photopletysmography Signal Analysis for Biomedical Applications. Sensors 2018, 18, 1894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hina, A.; Saadeh, W. A Noninvasive Glucose Monitoring SoC Based on Single Wavelength Photoplethysmography. IEEE Trans. Biomed. Circuits Syst. 2020, 14, 504–515. [Google Scholar] [CrossRef]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [Green Version]
- Alian, A.A.; Shelley, K.H. Photoplethysmography. Best Pract. Res. Clin. Anaesthesiol. 2014, 28, 395–406. [Google Scholar] [CrossRef]
- Sviridova, N.; Sakai, K. Human photoplethysmogram: New insight into chaotic characteristics. Chaos Solitons Fractals 2015, 77, 53–63. [Google Scholar] [CrossRef] [Green Version]
- Aimie-Salleh, N.; Ghani, N.A.A.; Hasanudin, N.; Shafie, S.N.S. Heart Rate Variability Recording System Using Photoplethysmography Sensor. In Autonomic Nervous System Monitoring-Heart Rate Variability; IntechOpen: London, UK, 2019. [Google Scholar]
- Nguyen, L.; Su, S.; Nguyen, H.T. Effects of Hyperglycemia on Variability of RR, QT and corrected QT intervals in Type 1 Diabetic Patients. In Proceedings of the 35th Annual International Conference of the IEEE EMBS, Osaka, Japan, 3–7 July 2013. [Google Scholar]
- Akhter, N.; Tharewal, S.; Gite, H.; Kale, K.V. Microcontroller based RR-Interval measurement using PPG signals for Heart Rate Variability based biometric application. In Proceedings of the 2015 International Conference on Advances in Computing, Communications and Informatics (ICACCI), Kochi, India, 10–13 August 2015; pp. 588–593. [Google Scholar]
- Vinik, A.I.; Erbas, T.; Casellini, C.M. Diabetic cardiac autonomic neuropathy, inflammation and cardiovascular disease. J. Diabetes Investig. 2013, 4, 4–18. [Google Scholar] [CrossRef]
- Rothberg, L.J.; Lees, T.; Clifton-Bligh, R.; Lal, S. Association Between Heart Rate Variability Measures and Blood Glucose Levels: Implications for Noninvasive Glucose Monitoring for Diabetes. Diabetes Technol. Ther. 2016, 18, 366–376. [Google Scholar] [CrossRef] [PubMed]
- Benichou, T.; Pereira, B.; Mermillod, M.; Tauveron, I.; Pfabigan, D.; Maqdasy, S.; Dutheil, F. Heart rate variability in type 2 diabetes mellitus: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0195166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chellappan, K.; Sahathevan, R. Accelerated Aging and Non-invasive Cardiovascular Risk Monitoring. Cerebrovasc. Dis. 2015, 40, 25–27. [Google Scholar]
- Nirala, N.; Periyasamy, R.; Kumar, A. Noninvasive Diagnostic Methods for Better Screening of Peripheral Arterial Disease. Ann. Vasc. Surg. 2018, 52, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Pilt, K.; Ferenets, R.; Meigas, K.; Lindberg, L.G.; Temitski, K.; Viigimaa, M. New photoplethysmographic signal analysis algorithm for arterial stiffness estimation. Sci. World J. 2013, 2013, 169035. [Google Scholar] [CrossRef] [PubMed]
- Yousef, Q.; Reaz, M.B.I.; Ali, M.A.M. The Analysis of PPG Morphology: Investigating the Effects of Aging on Arterial Compliance. Meas. Sci. Rev. 2012, 12, 266. [Google Scholar] [CrossRef] [Green Version]
- Md Lazin Md Lazim, M.R.; Aminuddin, A.; Chellappan, K.; Ugusman, A.; Hamid, A.A.; Wan Ahmad, W.A.N.; Mohamad, M.S.F. Is Heart Rate a Confounding Factor for Photoplethysmography Markers? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2591. [Google Scholar] [CrossRef] [Green Version]
- Hiramine, K.; Miwa, T.; Horashima, K. A study of the Arterial Stiffness Index in Diabetes Patient: Trial of a New Non-Invasive Arterial Hardness Estimation Procedure That Uses an Oscillometric Method; Japan Diabetes Society: Tokyo, Japan, 2002. [Google Scholar]
- Tjahjadi, H.; Ramli, K. Non-invasive Blood Pressure Classification Based on Photoplethysmography Using K-Nearest Neighbors Algorithm: A Feasibility Study. Information 2020, 11, 93. [Google Scholar] [CrossRef] [Green Version]
- Banik, S.K.; Fenley, A.T.; Kulkarni, R.V. A model for signal transduction during quorum sensing in Vibrio harveyi. Phys. Biol 2009, 6, 046008. [Google Scholar] [CrossRef]
- Lim, P.K.; Ng, S.C.; Lovell, N.H.; Yu, Y.P.; Tan, M.P.; McCombie, D.; Lim, E.; Redmond, S.J. Adaptive template matching of photoplethysmogram pulses to detect motion artefact. Physiol. Meas. 2018, 39, 105005. [Google Scholar] [CrossRef]
- Maeda, Y.; Sekine, M.; Tamura, T. Relationship between measurement site and motion artifacts in wearable reflected photoplethysmography. J. Med. Syst. 2011, 35, 969–976. [Google Scholar] [CrossRef] [PubMed]
- Hettiarachchi, C.; Chitraranjan, C. A Machine Learning Approach to Predict Diabetes Using Short Recorded Photoplethysmography and Physiological Characteristics. In Artificial Intelligence in Medicine; Springer: Cham, Switzerland, 2019; Chapter 41; pp. 322–327. [Google Scholar]
- Zou, Q.; Qu, K.; Luo, Y.; Yin, D.; Ju, Y.; Tang, H. Predicting Diabetes Mellitus With Machine Learning Techniques. Front. Genet. 2018, 9, 515. [Google Scholar] [CrossRef] [PubMed]
- Karimipour, H.; Shandiz, H.T.; Zahedi, E. Diabetic diagnose test based on PPG signal and identification system. J. Biomed. Sci. Eng. 2009, 02, 465–469. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Zhang, Y.; Siddiqui, S.A.; Kos, A. Non-invasive blood-glucose estimation using smartphone PPG signals and subspace kNN classifier. Elektrotehniski Vestn. 2019, 86, 68–74. [Google Scholar]
- Nirala, N.; Periyasamy, R.; Singh, B.K.; Kumar, A. Detection of type-2 diabetes using characteristics of toe photoplethysmogram by applying support vector machine. Biocybern. Biomed. Eng. 2019, 39, 38–51. [Google Scholar] [CrossRef]
- Qawqzeh, Y.K.; Bajahzar, A.S.; Jemmali, M.; Otoom, M.M.; Thaljaoui, A. Classification of Diabetes Using Photoplethysmogram (PPG) Waveform Analysis: Logistic Regression Modeling. Biomed. Res. Int. 2020, 2020, 3764653. [Google Scholar] [CrossRef]
- Zhang, G.; Mei, Z.; Zhang, Y.; Ma, X.; Lo, B.; Chen, D.; Zhang, Y. A Non-invasive Blood Glucose Monitoring System Based on Smartphone PPG Signal Processing and Machine Learning. IEEE Trans. Ind. Inform. 2020, 16, 7209–7218. [Google Scholar] [CrossRef]
- Hossain, S.; Debnath, B.; Biswas, S.; Al-Hossain, M.J.; Anika, A.; Zaman Navid, S.K. Estimation of Blood Glucose from PPG Signal Using Convolutional Neural Network. In Proceedings of the 2019 IEEE International Conference on Biomedical Engineering, Computer and Information Technology for Health (BECITHCON), Dhaka, Bangladesh, 28–30 November 2019; pp. 53–58. [Google Scholar]
- Sen Gupta, S.; Kwon, T.-H.; Hossain, S.; Kim, K.-D. Towards non-invasive blood glucose measurement using machine learning: An all-purpose PPG system design. Biomed. Signal Process. Control 2021, 68, 102706. [Google Scholar] [CrossRef]
- Majumder, S.; Balaji, N.; Brey, K.; Fu, W.; Menzies, T. 500+ Times Faster Than Deep Learning (A Case Study Exploring Faster Methods for Text Mining StackOverflow). In Proceedings of the 2018 IEEE/ACM 15th International Conference on Mining Software Repositories (MSR), Gothenburg, Sweden, 28–29 May 2018. [Google Scholar] [CrossRef]
- Bolandraftar, M. Application of K-Nearest Neighbor (KNN) Approach for Predicting Economic Events: Theoretical Background. J. Eng. Res. Appl. 2013, 3, 605–610. [Google Scholar]
- Easy Pulse Sensor (Version 1.1). Available online: http://www.embedded-lab.com (accessed on 20 October 2021).
- Jukic, S.; Saracevic, M.; Subasi, A.; Kevric, J. Comparison of Ensemble Machine Learning Methods for Automated Classification of Focal and Non-Focal Epileptic EEG Signals. Mathematics 2020, 8, 1481. [Google Scholar] [CrossRef]
- Lu, H.; Xu, Y.; Ye, M.; Yan, K.; Gao, Z.; Jin, Q. Learning misclassification costs for imbalanced classification on gene expression data. BMC Bioinform. 2019, 20, 681. [Google Scholar] [CrossRef] [PubMed]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Subject ID | Sex F/M | Age (Years) | Systolic (mmHg) | Diastolic (mmHg) | HR (bpm) | Random Glucose Test (mg/dL) | Status |
|---|---|---|---|---|---|---|---|---|
| 1 | 4 | F | 19 | 125 | 80 | 80 | 92 | Normal |
| 2 | 5 | M | 18 | 100 | 70 | 80 | 80 | Normal |
| 4 | 12 | M | 40 | 111 | 67 | 101 | 211 | Diabetes |
| 5 | 13 | M | 48 | 112 | 57 | 83 | 230 | Diabetes |
| Plasma Glucose Test | Normal | Prediabetes | Diabetes |
|---|---|---|---|
| Random | <200 mg/dL or <11.1 mmol/L | N/A | >200 mg/dL or >11.1 mmol/L |
| Fasting | <100 mg/dL or <5.5 mmol/L | 100–125 mg/dL or 5.5–6.9 mmol/L | >126 mg/dL or >7 mmol/L |
| Classifier | Accuracy (%) | Prediction Speed (Observation/s) | Training Time (s) | Total Cost |
|---|---|---|---|---|
| Ensemble Bagged Trees | 98.00 | 8.02 | 2 | |
| Weighted KNN | 93.00 | 8.87 | 7 | |
| Ensemble Subspace KNN | 93.00 | 15.00 | 7 | |
| Fine Trees | 93.00 | 24.00 | 7 | |
| Medium Trees | 93.00 | 24.00 | 7 | |
| Fine KNN | 92.00 | 8.00 | 8 | |
| Three-layered Neural Network | 92.00 | 16.18 | NA | |
| Narrow Neural Network | 91.00 | 7.09 | NA | |
| Coarse Gaussian SVM | 90.00 | 5.17 | 9 | |
| Ensemble Boosted Trees | 91.00 | 27.00 | 10 | |
| Ensemble RUS Boosted Trees | 87.00 | 48.08 | 13 | |
| Logistic Regression | 76.00 | 19.03 | NA |
| Year | PPG Signal | Invasive Methods | Classifier | Features Extraction | Evaluation Metric | Characteristic |
|---|---|---|---|---|---|---|
| 2009 | Finger sensor [40] | Not mentioned | Auto-Regressive Moving Average (ARMA) | Not Mentioned | Specificity = 0.9 Sensitivity = 1 | Classification |
| 2017 | Pulse Oximeter [14] | HbA1c Test | Random Forest | 9 | ROC = 0.7 | Classification |
| Gradient Boosting | 9 | ROC = 0.7 | Classification | |||
| Linear Discriminant Analysis | 9 | ROC = 0.6 | Classification | |||
| 2019 | Smartphone Camera [41] | Glucose meter | Subspace KNN | 67 | Accuracy = 86.2%. | Classification |
| RUS Boosted Trees | 67 | Accuracy = 85.0% | Classification | |||
| Bagged Trees | 67 | Accuracy = 86.0% | Classification | |||
| Decision Trees | 67 | Accuracy = 80.1% | Classification | |||
| 2019 | Finger sensor [42] | Blood Glucose Lab Test | Support Vector Machine | 37 | Accuracy = 97.9% | Classification |
| 2020 | Finger sensor [43] | HbA1c Test | Logistic Regression | Not Mentioned | Accuracy = 92.3% | Classification |
| 2020 | Smartphone [44] | Glucose meter | Gaussian Support Vector Machine (GSVM) | 28 | Accuracy = 81.5% | Classification |
| Bagged Trees | 28 | Accuracy = 74.0% | Classification | |||
| K-Nearest Neighbor | 28 | Accuracy = 71.0% | Classification | |||
| 2021 | Finger sensor | Glucose meter | Ensemble bagged trees (Proposed method in this study) | 2100 | Accuracy: 98.0% | Classification |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Susana, E.; Ramli, K.; Murfi, H.; Apriantoro, N.H. Non-Invasive Classification of Blood Glucose Level for Early Detection Diabetes Based on Photoplethysmography Signal. Information 2022, 13, 59. https://0-doi-org.brum.beds.ac.uk/10.3390/info13020059
Susana E, Ramli K, Murfi H, Apriantoro NH. Non-Invasive Classification of Blood Glucose Level for Early Detection Diabetes Based on Photoplethysmography Signal. Information. 2022; 13(2):59. https://0-doi-org.brum.beds.ac.uk/10.3390/info13020059
Chicago/Turabian StyleSusana, Ernia, Kalamullah Ramli, Hendri Murfi, and Nursama Heru Apriantoro. 2022. "Non-Invasive Classification of Blood Glucose Level for Early Detection Diabetes Based on Photoplethysmography Signal" Information 13, no. 2: 59. https://0-doi-org.brum.beds.ac.uk/10.3390/info13020059