
Evaluation of an Injectable Biphasic Calcium Sulfate/Hydroxyapatite Cement for the Augmentation of Fenestrated Pedicle Screws in Osteoporotic Vertebrae: A Biomechanical Cadaver Study

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Methodology
2.2. Specimen Preparation
2.3. Pedicle Screw Implantation
2.4. CaS/HA Cement Preparation and Augmentation Procedure
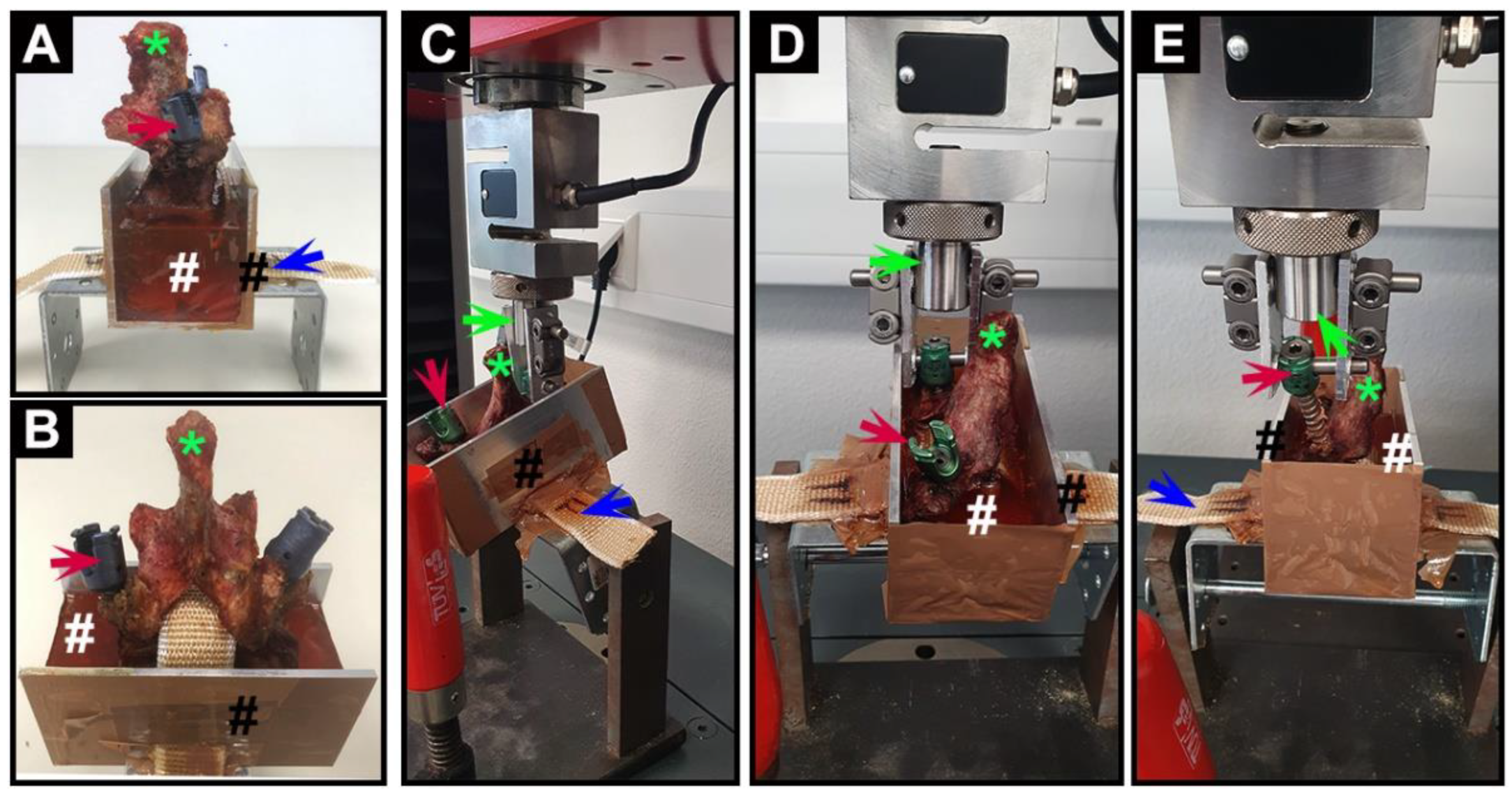
2.5. Mechanical Testing
2.6. Statistics
2.7. Ethical Approval
3. Results
3.1. Specimen Preparation
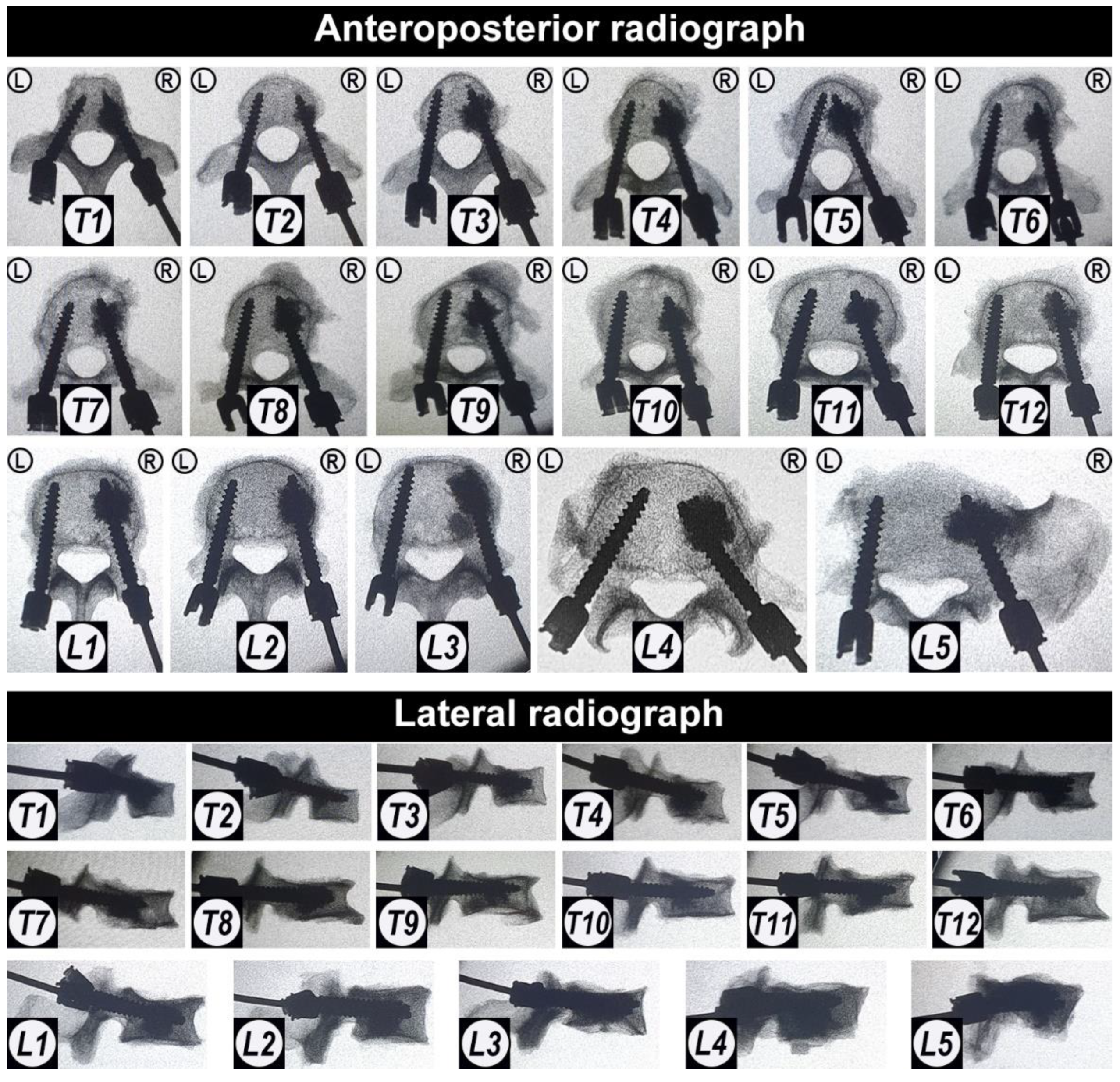
3.2. Pedicle Screw Implantation
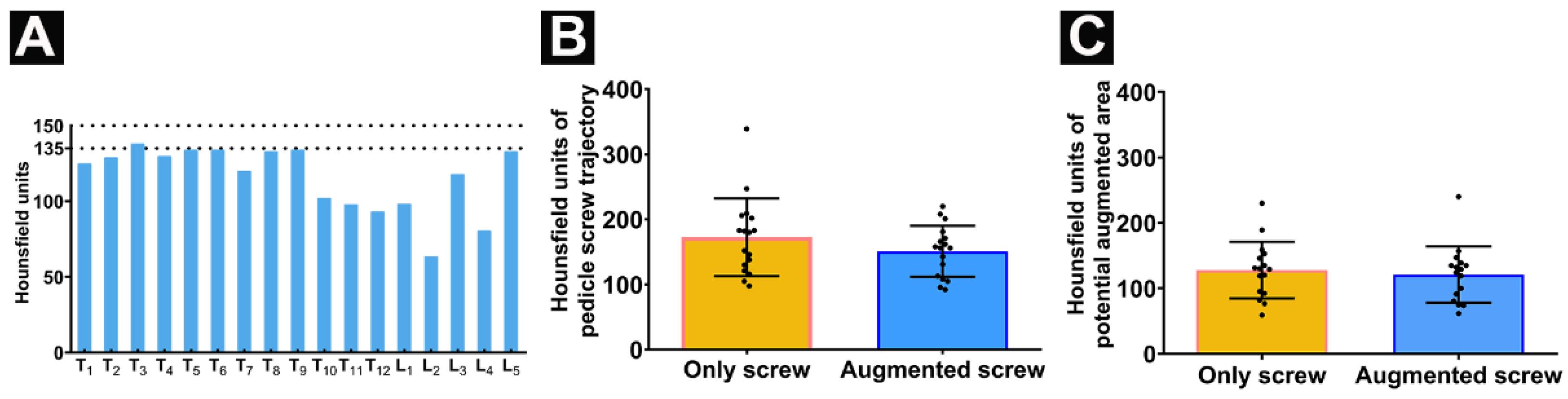
3.3. Trajectories of Augmented and Non-Augmented Pedicle Screws
3.4. CaS/HA Augmentation Leads to an Increased Pull-Out Force
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Krenzlin, H.; Foelger, A.; Mailänder, V.; Blase, C.; Brockmann, M.; Düber, C.; Ringel, F.; Keric, N. Novel Biodegradable Composite of Calcium Phosphate Cement and the Collagen I Mimetic P-15 for Pedicle Screw Augmentation in Osteoporotic Bone. Biomedicines 2021, 9, 1392. [Google Scholar] [CrossRef] [PubMed]
- Reginster, J.Y.; Burlet, N. Osteoporosis: A still increasing prevalence. Bone 2006, 38 (Suppl. 1), 4–9. [Google Scholar] [CrossRef] [PubMed]
- Park, S.B.; Chung, C.K. Strategies of spinal fusion on osteoporotic spine. J. Korean Neurosurg. Soc. 2011, 49, 317–322. [Google Scholar] [CrossRef]
- Xie, F.; Zhou, B.; Wang, J.; Liu, T.; Wu, X.; Fang, R.; Kang, Y.; Dai, R. Microstructural properties of trabecular bone autografts: Comparison of men and women with and without osteoporosis. Arch. Osteoporos. 2018, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Paré, P.E.; Chappuis, J.L.; Rampersaud, R.; Agarwala, A.O.; Perra, J.H.; Erkan, S.; Wu, C. Biomechanical evaluation of a novel fenestrated pedicle screw augmented with bone cement in osteoporotic spines. Spine (Phila Pa 1976) 2011, 36, E1210–E1214. [Google Scholar] [CrossRef] [PubMed]
- Abousayed, M.; Boktor, J.G.; Sultan, A.M.; Koptan, W.; El-Miligui, Y. Augmentation of fenestrated pedicle screws with cement in patients with osteoporotic spine. J. Craniovertebr. Junction Spine 2018, 9, 20–25. [Google Scholar] [CrossRef]
- El Saman, A.; Meier, S.; Sander, A.; Kelm, A.; Marzi, I.; Laurer, H. Reduced loosening rate and loss of correction following posterior stabilization with or without PMMA augmentation of pedicle screws in vertebral fractures in the elderly. Eur. J. Trauma Emerg. Surg. 2013, 39, 455–460. [Google Scholar] [CrossRef]
- Tomé-Bermejo, F.; Piñera, A.R.; Alvarez-Galovich, L. Osteoporosis and the Management of Spinal Degenerative Disease (I). Arch. Bone Jt. Surg. 2017, 5, 272–282. [Google Scholar]
- Shea, T.M.; Laun, J.; Gonzalez-Blohm, S.A.; Doulgeris, J.J.; Lee, W.E., 3rd; Aghayev, K.; Vrionis, F.D. Designs and techniques that improve the pullout strength of pedicle screws in osteoporotic vertebrae: Current status. Biomed. Res. Int. 2014, 2014, 748393. [Google Scholar] [CrossRef] [Green Version]
- Rometsch, E.; Spruit, M.; Zigler, J.E.; Menon, V.K.; Ouellet, J.A.; Mazel, C.; Härtl, R.; Espinoza, K.; Kandziora, F. Screw-Related Complications after Instrumentation of the Osteoporotic Spine: A Systematic Literature Review with Meta-Analysis. Glob. Spine J. 2020, 10, 69–88. [Google Scholar] [CrossRef] [Green Version]
- Sun, H.; Liu, C.; Liu, H.; Bai, Y.; Zhang, Z.; Li, X.; Li, C.; Yang, H.; Yang, L. A novel injectable calcium phosphate-based nanocomposite for the augmentation of cannulated pedicle-screw fixation. Int. J. Nanomed. 2017, 12, 3395–3406. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.; Liu, C.; Li, X.; Liu, H.; Zhang, W.; Yang, H.; Li, C.; Yang, L. A novel calcium phosphate-based nanocomposite for the augmentation of cement-injectable cannulated pedicle screws fixation: A cadaver and biomechanical study. J. Orthop. Translat. 2020, 20, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Frick, C.; Dietz, A.C.; Merritt, K.; Umbreit, T.H.; Tomazic-Jezic, V.J. Effects of prosthetic materials on the host immune response: Evaluation of polymethyl-methacrylate (PMMA), polyethylene (PE), and polystyrene (PS) particles. J. Long Term Eff. Med. Implant. 2006, 16, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Rohmiller, M.T.; Schwalm, D.; Glattes, R.C.; Elalayli, T.G.; Spengler, D.M. Evaluation of calcium sulfate paste for augmentation of lumbar pedicle screw pullout strength. Spine J. 2002, 2, 255–260. [Google Scholar] [CrossRef]
- Cho, W.; Wu, C.; Erkan, S.; Kang, M.M.; Mehbod, A.A.; Transfeldt, E.E. The effect on the pullout strength by the timing of pedicle screw insertion after calcium phosphate cement injection. J. Spinal Disord. Tech. 2011, 24, 116–120. [Google Scholar] [CrossRef]
- Hoppe, S.; Keel, M.J. Pedicle screw augmentation in osteoporotic spine: Indications, limitations and technical aspects. Eur. J. Trauma Emerg. Surg. 2017, 43, 3–8. [Google Scholar] [CrossRef]
- Raina, D.B.; Matuszewski, L.M.; Vater, C.; Bolte, J.; Isaksson, H.; Lidgren, L.; Tägil, M.; Zwingenberger, S. A facile one-stage treatment of critical bone defects using a calcium sulfate/hydroxyapatite biomaterial providing spatiotemporal delivery of bone morphogenic protein-2 and zoledronic acid. Sci. Adv. 2020, 6, eabc1779. [Google Scholar] [CrossRef]
- Alfotawi, R.; Naudi, K.; Dalby, M.J.; Tanner, K.E.; McMahon, J.D.; Ayoub, A. Assessment of cellular viability on calcium sulphate/hydroxyapatite injectable scaffolds. J. Tissue Eng. 2013, 4, 2041731413509645. [Google Scholar] [CrossRef] [Green Version]
- Abramo, A.; Geijer, M.; Kopylov, P.; Tägil, M. Osteotomy of distal radius fracture malunion using a fast remodeling bone substitute consisting of calcium sulphate and calcium phosphate. J. Biomed. Mater. Res. B Appl. Biomater. 2010, 92, 281–286. [Google Scholar] [CrossRef]
- Nilsson, M.; Wielanek, L.; Wang, J.S.; Tanner, K.E.; Lidgren, L. Factors influencing the compressive strength of an injectable calcium sulfate-hydroxyapatite cement. J. Mater. Sci. Mater. Med. 2003, 14, 399–404. [Google Scholar] [CrossRef]
- Masala, S.; Nano, G.; Marcia, S.; Muto, M.; Fucci, F.P.; Simonetti, G. Osteoporotic vertebral compression fractures augmentation by injectable partly resorbable ceramic bone substitute (Cerament™|SPINE SUPPORT): A prospective nonrandomized study. Neuroradiology 2012, 54, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Marcia, S.; Boi, C.; Dragani, M.; Marini, S.; Marras, M.; Piras, E.; Anselmetti, G.C.; Masala, S. Effectiveness of a bone substitute (CERAMENT™) as an alternative to PMMA in percutaneous vertebroplasty: 1-year follow-up on clinical outcome. Eur. Spine J. 2012, 21 (Suppl. 1), S112–S118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kok, J.; Širka, A.; Liu, Y.; Tarasevičius, Š.; Belickas, J.; Tägil, M.; Lidgren, L.; Isaksson, H.; Raina, D.B. Augmenting a dynamic hip screw with a calcium sulfate/hydroxyapatite biomaterial. Med. Eng. Phys. 2021, 92, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Zampelis, V.; Tägil, M.; Lidgren, L.; Isaksson, H.; Atroshi, I.; Wang, J.S. The effect of a biphasic injectable bone substitute on the interface strength in a rabbit knee prosthesis model. J. Orthop. Surg. Res. 2013, 8, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raina, D.B.; Markevičiūtė, V.; Stravinskas, M.; Kok, J.; Jacobson, I.; Liu, Y.; Sezgin, E.A.; Isaksson, H.; Zwingenberger, S.; Tägil, M.; et al. A New Augmentation Method for Improved Screw Fixation in Fragile Bone. Front. Bioeng. Biotechnol. 2022, 10, 816250. [Google Scholar] [CrossRef]
- Li, D.; Sun, C.; Jiang, J.; Lu, F.; Xia, X.; Wang, H.; Zou, F.; Ma, X. A study of screw placement to obtain the optimal pull-out resistance of lumbar pedicle screws-analysis of Hounsfield units measurements based on computed tomography. BMC Musculoskelet. Disord. 2022, 23, 124. [Google Scholar] [CrossRef]
- Zhang, R.J.; Li, H.M.; Gao, H.; Jia, C.Y.; Xing, T.; Shen, C.L. Associations between the hounsfield unit values of different trajectories and bone mineral density of vertebrae: Cortical bone and traditional trajectories. Am. J. Transl. Res. 2020, 12, 3906–3916. [Google Scholar]
- Kuhns, C.A.; Reiter, M.; Pfeiffer, F.; Choma, T.J. Surgical strategies to improve fixation in the osteoporotic spine: The effects of tapping, cement augmentation, and screw trajectory. Global Spine J. 2014, 4, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Ahern, D.P.; McDonnell, J.M.; Riffault, M.; Evans, S.; Wagner, S.C.; Vaccaro, A.R.; Hoey, D.A.; Butler, J.S. A meta-analysis of the diagnostic accuracy of Hounsfield units on computed topography relative to dual-energy X-ray absorptiometry for the diagnosis of osteoporosis in the spine surgery population. Spine J. 2021, 21, 1738–1749. [Google Scholar] [CrossRef]
- Chevalier, Y.; Matsuura, M.; Krüger, S.; Traxler, H.; Fleege, C.; Rauschmann, M.; Schilling, C. The effect of cement augmentation on pedicle screw fixation under various load cases: Results from a combined experimental, micro-CT, and micro-finite element analysis. Bone Jt. Res. 2021, 10, 797–806. [Google Scholar] [CrossRef]
- Weiser, L.; Huber, G.; Sellenschloh, K.; Viezens, L.; Püschel, K.; Morlock, M.M.; Lehmann, W. Insufficient stability of pedicle screws in osteoporotic vertebrae: Biomechanical correlation of bone mineral density and pedicle screw fixation strength. Eur Spine J. 2017, 26, 2891–2897. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, Q.; Danisa, O.A.; Cheng, W. Measurement Techniques and Utility of Hounsfield Unit Values for Assessment of Bone Quality Prior to Spinal Instrumentation: A Review of Current Literature. Spine (Phila Pa 1976) 2019, 44, E239–E244. [Google Scholar] [CrossRef] [PubMed]
- Leichtle, C.I.; Lorenz, A.; Rothstock, S.; Happel, J.; Walter, F.; Shiozawa, T.; Leichtle, U.G. Pull-out strength of cemented solid versus fenestrated pedicle screws in osteoporotic vertebrae. Bone Jt. Res. 2016, 5, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Elder, B.D.; Lo, S.F.; Holmes, C.; Goodwin, C.R.; Kosztowski, T.A.; Lina, I.A.; Locke, J.E.; Witham, T.F. The biomechanics of pedicle screw augmentation with cement. Spine J. 2015, 15, 1432–1445. [Google Scholar] [CrossRef] [PubMed]
- Son, H.J.; Choi, S.H.; Heo, D.R.; Kook, I.; Lee, M.K.; Ahn, H.S.; Kang, C.N. Outcomes of the use of cement-augmented cannulated pedicle screws in lumbar spinal fusion. Spine J. 2021, 21, 1857–1865. [Google Scholar] [CrossRef]
- Wang, J.S.; Tägil, M.; Isaksson, H.; Boström, M.; Lidgren, L. Tissue reaction and material biodegradation of a calcium sulfate/apatite biphasic bone substitute in rat muscle. J. Orthop. Translat. 2016, 6, 10–17. [Google Scholar] [CrossRef] [Green Version]
- Raina, D.B.; Širka, A.; Qayoom, I.; Teotia, A.K.; Liu, Y.; Tarasevicius, S.; Tanner, K.E.; Isaksson, H.; Kumar, A.; Tägil, M.; et al. Long-Term Response to a Bioactive Biphasic Biomaterial in the Femoral Neck of Osteoporotic Rats. Tissue Eng. Part A 2020, 26, 1042–1051. [Google Scholar] [CrossRef]
- Širka, A.; Raina, D.B.; Isaksson, H.; Tanner, K.E.; Smailys, A.; Kumar, A.; Tarasevičius, Š.; Tägil, M.; Lidgren, L. Calcium Sulphate/Hydroxyapatite Carrier for Bone Formation in the Femoral Neck of Osteoporotic Rats. Tissue Eng. Part A 2018, 24, 1753–1764. [Google Scholar] [CrossRef]
- Raina, D.B.; Isaksson, H.; Hettwer, W.; Kumar, A.; Lidgren, L.; Tägil, M. A Biphasic Calcium Sulphate/Hydroxyapatite Carrier Containing Bone Morphogenic Protein-2 and Zoledronic Acid Generates Bone. Sci. Rep. 2016, 6, 26033. [Google Scholar] [CrossRef] [Green Version]
- Raina, D.B.; Larsson, D.; Sezgin, E.A.; Isaksson, H.; Tägil, M.; Lidgren, L. Biomodulation of an implant for enhanced bone-implant anchorage. Acta Biomater. 2019, 96, 619–630. [Google Scholar] [CrossRef]
- Kueny, R.A.; Kolb, J.P.; Lehmann, W.; Püschel, K.; Morlock, M.M.; Huber, G. Influence of the screw augmentation technique and a diameter increase on pedicle screw fixation in the osteoporotic spine: Pullout versus fatigue testing. Eur. Spine J. 2014, 23, 2196–2202. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Location | Size (d/l) in mm | Location | Size (d/l) in mm | Location | Size (d/l) in mm |
|---|---|---|---|---|---|
| T1 | 6/30 | T7 | 6/45 | L1 | 7/50 |
| T2 | 5/35 | T8 | 6/50 | L2 | 7/50 |
| T3 | 5/40 | T9 | 6/50 | L3 | 7/50 |
| T4 | 5/40 | T10 | 7/45 | L4 | 7/45 |
| T5 | 5/45 | T11 | 7/45 | L5 | 7/40 |
| T6 | 6/45 | T12 | 7/50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, X.; Raina, D.B.; Vater, C.; Kilian, D.; Ahlfeld, T.; Platzek, I.; Nimtschke, U.; Tägil, M.; Lidgren, L.; Thomas, A.; et al. Evaluation of an Injectable Biphasic Calcium Sulfate/Hydroxyapatite Cement for the Augmentation of Fenestrated Pedicle Screws in Osteoporotic Vertebrae: A Biomechanical Cadaver Study. J. Funct. Biomater. 2022, 13, 269. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb13040269
Tian X, Raina DB, Vater C, Kilian D, Ahlfeld T, Platzek I, Nimtschke U, Tägil M, Lidgren L, Thomas A, et al. Evaluation of an Injectable Biphasic Calcium Sulfate/Hydroxyapatite Cement for the Augmentation of Fenestrated Pedicle Screws in Osteoporotic Vertebrae: A Biomechanical Cadaver Study. Journal of Functional Biomaterials. 2022; 13(4):269. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb13040269
Chicago/Turabian StyleTian, Xinggui, Deepak B. Raina, Corina Vater, David Kilian, Tilman Ahlfeld, Ivan Platzek, Ute Nimtschke, Magnus Tägil, Lars Lidgren, Alexander Thomas, and et al. 2022. "Evaluation of an Injectable Biphasic Calcium Sulfate/Hydroxyapatite Cement for the Augmentation of Fenestrated Pedicle Screws in Osteoporotic Vertebrae: A Biomechanical Cadaver Study" Journal of Functional Biomaterials 13, no. 4: 269. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb13040269