
Clinical Applications and Mechanical Properties of CAD-CAM Materials in Restorative and Prosthetic Dentistry: A Systematic Review

 ,
,  ,
,  ,
,  ,
, 

Abstract
:1. Introduction
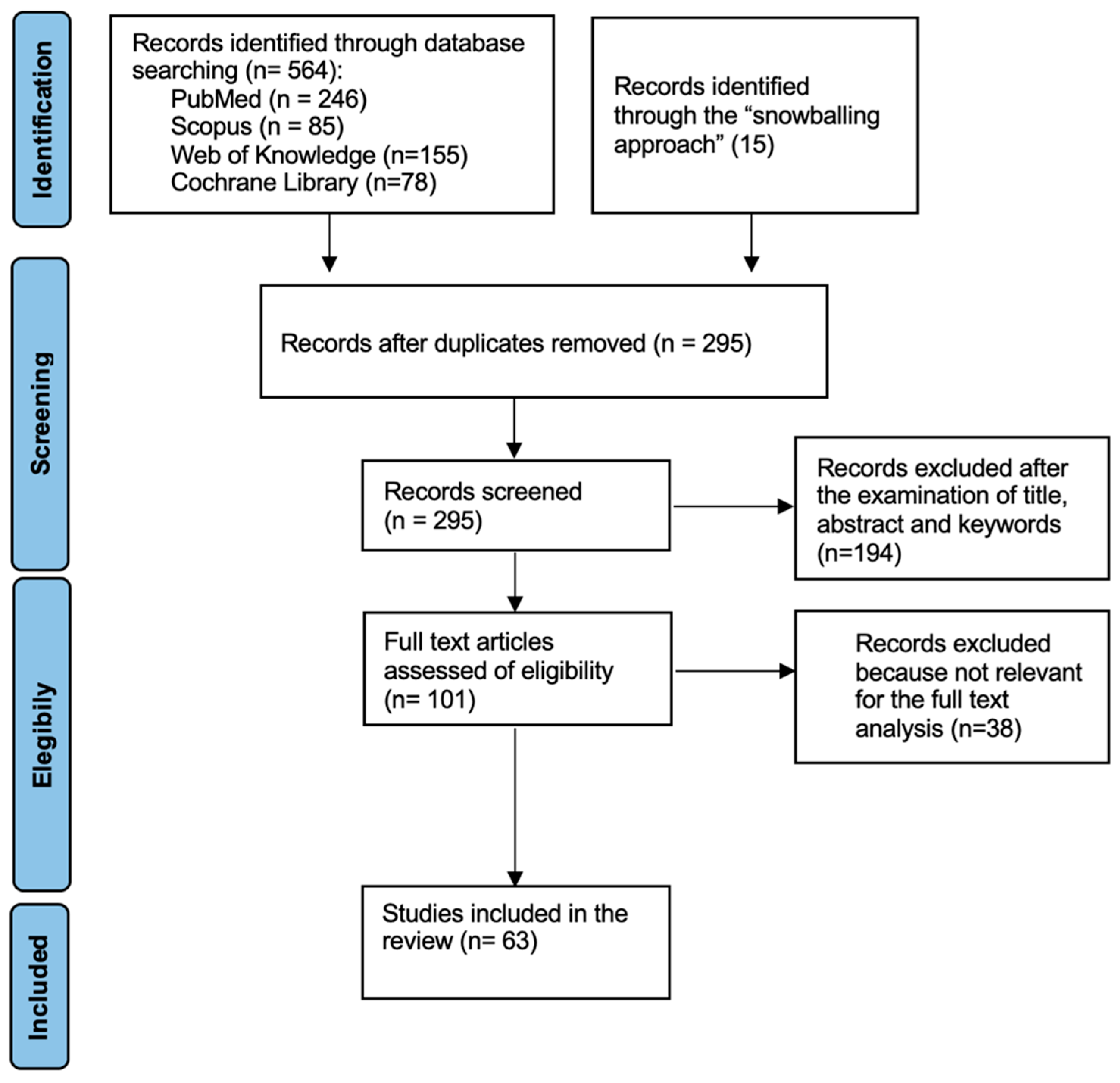
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
- (1)
- Articles addressing at least one of the following topics regarding dental materials for CAD-CAM systems: clinical indications and/or outcomes, manufacturers, mechanical features (flexural strength, hardness, and elastic modulus), and materials’ composition or optical properties;
- (2)
- Studies performed in vitro or in vivo;
- (3)
- Systematic and narrative reviews.
3. Results
4. Discussion
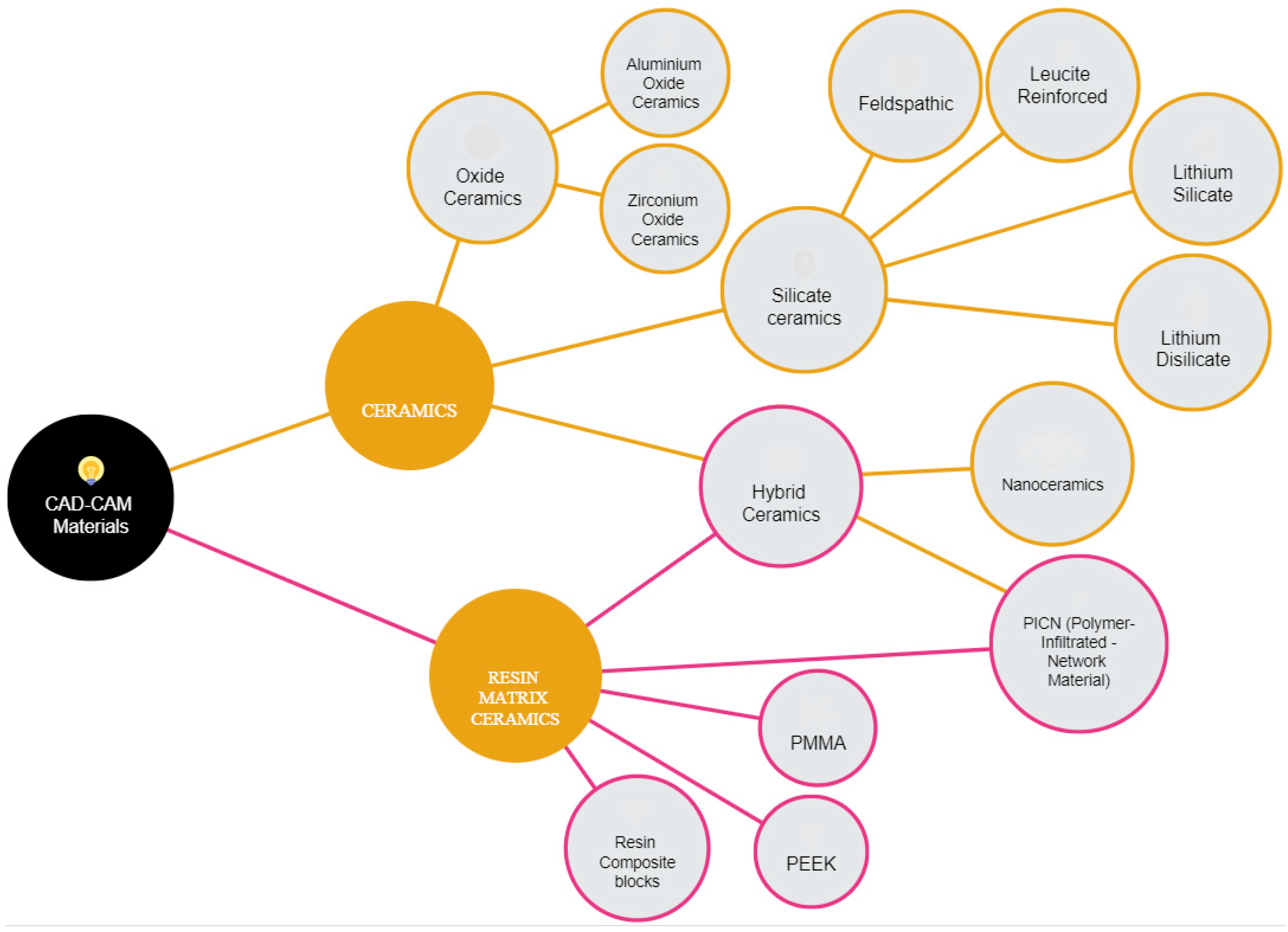
4.1. Silicate Ceramics (Glass Ceramics)
4.1.1. Feldespathic
4.1.2. Leucite-Reinforced
4.1.3. Lithium Silicate
4.1.4. Lithium Disilicate
4.2. Oxide Ceramics
4.2.1. Zirconium Oxide Ceramics
4.2.2. Aluminum Oxide Ceramics
4.3. Hybrid Ceramics
4.3.1. PICN
4.3.2. Nanoceramics
4.4. Resin Matrix Ceramics
4.4.1. PMMA
4.4.2. PEEK
4.4.3. Resin Composite Blocks (RCBs)
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Barenghi, L.; Barenghi, A.; Garagiola, U.; Di Blasio, A.; Giannì, A.B.; Spadari, F. Pros and Cons of CAD/CAM Technology for Infection Prevention in Dental Settings during COVID-19 Outbreak. Sensors 2021, 22, 49. [Google Scholar] [CrossRef]
- Orsini, G.; Tosco, V.; Monterubbianesi, R.; Orilisi, G.; Putignano, A. A New Era in Restorative Dentistry. In The First Out-Standing 50 Years of “Università Politecnica Delle Marche”: Research Achievements in Life Sciences; Longhi, S., Monteriù, A., Freddi, A., Aquilanti, L., Ceravolo, M.G., Carnevali, O., Giordano, M., Moroncini, G., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 319–334. ISBN 978-3-030-33832-9. [Google Scholar]
- Tapie, L.; Lebon, N.; Mawussi, B.; Fron Chabouis, H.; Duret, F.; Attal, J.P. Understanding Dental CAD/CAM for Restorations–the Digital Workflow from a Mechanical Engineering Viewpoint. Int. J. Comput. Dent. 2015, 18, 21–44. [Google Scholar]
- Ahmed, K.E. We’re Going Digital: The Current State of CAD/CAM Dentistry in Prosthodontics. Prim. Dent. J. 2018, 7, 30–35. [Google Scholar] [CrossRef]
- Li, R.W.K.; Chow, T.W.; Matinlinna, J.P. Ceramic Dental Biomaterials and CAD/CAM Technology: State of the Art. J. Prosthodont. Res. 2014, 58, 208–216. [Google Scholar] [CrossRef]
- Papadiochou, S.; Pissiotis, A.L. Marginal Adaptation and CAD-CAM Technology: A Systematic Review of Restorative Material and Fabrication Techniques. J. Prosthet. Dent. 2018, 119, 545–551. [Google Scholar] [CrossRef]
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A Review of Dental CAD/CAM: Current Status and Future Perspectives from 20 Years of Experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef]
- Otto, T.; Dent, M. Case Series Clinical Results from a Long-Term Case Series Using Chairside CEREC CAD-CAM Inlays and Onlays. Int. J. Prosthodont. 2008, 21, 53–59. [Google Scholar]
- Alghazzawi, T.F. Advancements in CAD/CAM Technology: Options for Practical Implementation. J. Prosthodont. Res. 2016, 60, 72–84. [Google Scholar] [CrossRef]
- Saponaro, P.C.; Yilmaz, B.; Heshmati, R.H.; McGlumphy, E.A. Clinical Performance of CAD-CAM-Fabricated Complete Dentures: A Cross-Sectional Study. J. Prosthet. Dent. 2016, 116, 431–435. [Google Scholar] [CrossRef]
- Vecsei, B.; Joós-Kovács, G.; Borbély, J.; Hermann, P. Comparison of the Accuracy of Direct and Indirect Three-Dimensional Digitizing Processes for CAD/CAM Systems—An In Vitro Study. J. Prosthodont. Res. 2017, 61, 177–184. [Google Scholar] [CrossRef]
- Grzebieluch, W.; Mikulewicz, M.; Kaczmarek, U. Resin Composite Materials for Chairside CAD/CAM Restorations: A Comparison of Selected Mechanical Properties. J. Healthc. Eng. 2021, 2021, 8828954. [Google Scholar] [CrossRef]
- Tiu, J.; Belli, R.; Lohbauer, U. Contemporary CAD/CAM Materials in Dentistry. Curr. Oral Health Rep. 2019, 6, 250–256. [Google Scholar] [CrossRef]
- Sulaiman, T.A. Materials in Digital Dentistry—A Review. J. Esthet. Restor. Dent. 2020, 32, 71–181. [Google Scholar] [CrossRef] [PubMed]
- Beuer, F.; Schweiger, J.; Edelhoff, D. Digital Dentistry: An Overview of Recent Developments for CAD/CAM Generated Restorations. Br. Dent. J. 2008, 204, 505–511. [Google Scholar] [CrossRef]
- Lambert, H.; Durand, J.C.; Jacquot, B.; Fages, M. Dental Biomaterials for Chairside CAD/CAM: State of the Art. J. Adv. Prosthodont. 2017, 9, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef]
- Choong, M.K.; Galgani, F.; Dunn, A.G.; Tsafnat, G. Automatic Evidence Retrieval for Systematic Reviews. J. Med. Internet Res. 2014, 16, e223. [Google Scholar] [CrossRef]
- Skorulska, A.; Piszko, P.; Rybak, Z.; Szymonowicz, M.; Dobrzyński, M. Review on Polymer, Ceramic and Composite Materials for CAD/CAM Indirect Restorations in Dentistry—Application, Mechanical Characteristics and Comparison. Materials 2021, 14, 1592. [Google Scholar] [CrossRef]
- Zhang, Y.; Lawn, B.R. Novel Zirconia Materials in Dentistry. J. Dent. Res. 2018, 97, 140–147. [Google Scholar] [CrossRef]
- Gracis, S.; Thompson, V.P.; Ferencz, J.L.; Silva, N.R.; Bonfante, E.A. A New Classification System for All-Ceramic and Ceramic-Like Restorative Materials. Int. J. Prosthodont. 2015, 28, 227–235. [Google Scholar] [CrossRef]
- Ahmed, H. Craig’s Restorative Dental Materials, 14th ed.; Elsevier: Amsterdam, The Netherlands, 2019; p. 226. [Google Scholar]
- Avram, L.T.; Galațanu, S.V.; Opriș, C.; Pop, C.; Jivănescu, A. Effect of Different Etching Times with Hydrofluoric Acid on the Bond Strength of CAD/CAM Ceramic Material. Materials 2022, 15, 7071. [Google Scholar] [CrossRef]
- Veríssimo, A.H.; Moura, D.M.D.; Tribst, J.P.M.; Araújo, A.M.M.; Leite, F.P.P.; Souza, R.O.A.E. Effect of Hydrofluoric Acid Concentration and Etching Time on Resin-Bond Strength to Different Glass Ceramics. Braz. Oral Res. 2019, 33, e041. [Google Scholar] [CrossRef] [PubMed]
- Hinz, S.; Bensel, T.; Bömicke, W.; Henningsen, A.; Rudolph, J.; Boeckler, A.F. Impact of the Veneering Technique and Framework Material on the Failure Loads of All-Ceramic Computer-Aided Design/Computer-Aided Manufacturing Fixed Partial Dentures. Materials 2022, 15, 756. [Google Scholar] [CrossRef]
- D’Addazio, G.; Santilli, M.; Rollo, M.L.; Cardelli, P.; Rexhepi, I.; Murmura, G.; Al-Haj Husain, N.; Sinjari, B.; Traini, T.; Özcan, M.; et al. Fracture Resistance of Zirconia-Reinforced Lithium Silicate Ceramic Crowns Cemented with Conventional or Adhesive Systems: An In Vitro Study. Materials 2020, 13, 2012. [Google Scholar] [CrossRef] [PubMed]
- Mavriqi, L.; Valente, F.; Murmura, G.; Sinjari, B.; Macrì, M.; Trubiani, O.; Caputi, S.; Traini, T. Lithium Disilicate and Zirconia Reinforced Lithium Silicate Glass-Ceramics for CAD/CAM Dental Restorations: Biocompatibility, Mechanical and Microstructural Properties after Crystallization. J. Dent. 2022, 119, 104054. [Google Scholar] [CrossRef]
- Fabian Fonzar, R.; Carrabba, M.; Sedda, M.; Ferrari, M.; Goracci, C.; Vichi, A. Flexural Resistance of Heat-Pressed and CAD-CAM Lithium Disilicate with Different Translucencies. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2017, 33, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Gardell, E.; Larsson, C.; von Steyern, P.V. Translucent Zirconium Dioxide and Lithium Disilicate: A 3-Year Follow-up of a Prospective, Practice-Based Randomized Controlled Trial on Posterior Monolithic Crowns. Int. J. Prosthodont. 2021, 34, 163–172. [Google Scholar] [CrossRef] [PubMed]
- Traini, T.; Gherlone, E.; Parabita, S.F.; Caputi, S.; Piattelli, A. Fracture Toughness and Hardness of a Y-TZP Dental Ceramic after Mechanical Surface Treatments. Clin. Oral Investig. 2014, 18, 707–714. [Google Scholar] [CrossRef]
- Mirdamadi, E.S.; Nazarpak, M.H.; Solati-Hashjin, M. Metal oxide-based ceramics. In Woodhead Publishing Series in Biomaterials, Structural Biomaterials; Wen, C., Ed.; Woodhead Publishing: Sawston, UK, 2021; pp. 301–331. ISBN 9780128188316. [Google Scholar] [CrossRef]
- Li, J.; Hastings, G.W. Oxide bioceramics: Inert ceramic materials in medicine and dentistry. In Handbook of Biomaterial Properties; Black, J., Hastings, G., Eds.; Springer: Boston, MA, USA, 1998. [Google Scholar] [CrossRef]
- Guazzato, M.; Albakry, M.; Ringer, S.P.; Swain, M.V. Strength, Fracture Toughness, and Microstructure of a Selection of All-Ceramic Materials. Part II. Zirconia-Based Dental Ceram-Ics. Dent. Mater. 2004, 20, 449–456. [Google Scholar] [CrossRef]
- Monaco, C.; Caldari, M.; Scotti, R. Clinical Evaluation of Tooth-Supported Zirconia-Based Fixed Dental Prostheses: A Retrospective Cohort Study from the AIOP Clinical Research Group. Int. J. Prosthodont. 2015, 28, 236–238. [Google Scholar] [CrossRef]
- Pihlaja, J.; Näpänkangas, R.; Raustia, A. Outcome of Zirconia Partial Fixed Dental Prostheses Made by Predoctoral Dental Students: A Clinical Retrospective Study after 3 to 7 Years of Clinical Service. J. Prosthet. Dent. 2016, 116, 40–46. [Google Scholar] [CrossRef]
- Joda, T.; Gintaute, A.; Brägger, U.; Ferrari, M.; Weber, K.; Zitzmann, N.U. Time-Efficiency and Cost-Analysis Comparing Three Digital Workflows for Treatment with Monolithic Zirconia Implant Fixed Dental Prostheses: A Double-Blinded RCT. J. Dent. 2021, 113, 103779. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M.A.; Skroch, M.; Schmidt, A..; Rehmann, P.; Wöstmann, B. Monitoring Fatigue Damage in Different CAD/CAM Materials: A New Approach with Optical Coherence Tomography. J. Prosthodont. Res. 2021, 65, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Ozer, F.; Mante, F.K.; Chiche, G.; Saleh, N.; Takeichi, T.; Blatz, M.B. A Retrospective Survey on Long-Term Survival of Posterior Zirconia and Porcelain-Fused-to-Metal Crowns in Private Practice. Quintessence Int. 2014, 45, 31–38. [Google Scholar]
- Selz, C.F.; Strub, J.R.; Vach, K.; Guess, P.C. Long-Term Performance of Posterior InCeram Alumina Crowns Cemented with Different Luting Agents: A Prospective, Random-Ized Clinical Split-Mouth Study over 5 Years. Clin. Oral Investig. 2014, 18, 1695–1703. [Google Scholar] [CrossRef]
- Kawajiri, Y.; Ikeda, H.; Nagamatsu, Y.; Masaki, C.; Hosokawa, R.; Shimizu, H. PICN Nanocomposite as Dental CAD/CAM Block Comparable to Human Tooth in Terms of Hardness and Flexural Modu-Lus. Materials 2021, 14, 1182. [Google Scholar] [CrossRef] [PubMed]
- Kang, L.; Zhou, Y.; Lan, J.; Yu, Y.; Cai, Q.; Yang, X. Effect of Resin Composition on Performance of Polymer-Infiltrated Feldsparnetwork Composites for Dental Restoration. Dent. Mater. J. 2020, 39, 900–908. [Google Scholar] [CrossRef]
- Steinbrenner, H. Multichromatic and Highly Translucent Hybrid Ceramic Vita Enamic. Int. J. Comput. Dent. 2018, 21, 239–250. [Google Scholar]
- Yano, H.T.; Ikeda, H.; Nagamatsu, Y.; Masaki, C.; Hosokawa, R.; Shimizu, H. Correlation between Microstructure of CAD/CAM Composites and the Silanization Effect on Adhesive Bonding. J. Mech. Behav. Biomed. Mater. 2020, 101, 103441. [Google Scholar] [CrossRef]
- Li, K.; Kou, H.; Rao, J.; Liu, C.; Ning, C. Fabrication of Enamel-Like Structure on Polymer-Infiltrated Zirconia Ceramics. Dent. Mater. 2021, 37, e245–e255. [Google Scholar] [CrossRef]
- Demirel, A.; Bezgin, T.; Akaltan, F.; Sarı, Ş. Resin Nanoceramic CAD/CAM Restoration of the Primary Molar: 3-Year Follow-Up Study. Case Rep. Dent. 2017, 2017, 3517187. [Google Scholar] [CrossRef] [PubMed]
- Heck, K.; Paterno, H.; Lederer, A.; Litzenburger, F.; Hickel, R.; Kunzelmann, K.H. Fatigue Resistance of Ultrathin CAD/CAM Ceramic and Nanoceramic Composite Occlusal Veneers. Dent. Mater. 2019, 35, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Al Amri, M.D.; Labban, N.; Alhijji, S.; Alamri, H.; Iskandar, M.; Platt, J.A. In Vitro Evaluation of Translucency and Color Stability of CAD/CAM Polymer-Infiltrated Ceramic Materials after Accelerated Aging. J. Prosthodont. 2021, 30, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Al-Harbi, F.A.; Ayad, N.M.; ArRejaie, A.S.; Bahgat, H.A.; Baba, N.Z. Effect of Aging Regimens on Resin Nanoceramic Chairside CAD/CAM Material. J. Prosthodont. 2017, 26, 432–439. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.; Kim, Y.K.; Jang, Y.S.; Lee, J.J.; Lee, M.H.; Bae, T.S. Comparative Evaluation of the Mechanical Properties of CAD/CAM Dental Blocks. Odontology 2019, 107, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Ludovichetti, F.S.; Trindade, F.Z.; Werner, A.; Kleverlaan, C.J.; Fonseca, R.G. Wear Resistance and Abrasiveness of CAD-CAM Monolithic Materials. J. Prosthet. Dent. 2018, 120, 318.e1–318.e8. [Google Scholar] [CrossRef]
- Lauvahutanon, S.; Shiozawa, M.; Takahashi, H.; Iwasaki, N.; Oki, M.; Finger, W.J.; Arksornnukit, M. Discoloration of Various CAD/CAM Blocks after Immersion in Coffee. Restor. Dent. Endod. 2017, 42, 9–18. [Google Scholar] [CrossRef]
- Kurtulmus-Yilmaz, S.; Cengiz, E.; Ongun, S.; Karakaya, I. The Effect of Surface Treatments on the Mechanical and Optical Behaviors of CAD/CAM Restorative Materials. J. Prosthodont. 2019, 28, e496–e503. [Google Scholar] [CrossRef] [PubMed]
- Zafar, M.S. Prosthodontic Applications of Polymethyl Methacrylate (PMMA): An Update. Polymers 2020, 12, 2299. [Google Scholar] [CrossRef]
- Hassan, M.; Asghar, M.; Din, S.U.; Zafar, M.S. Chapter 8. In Thermoset Polymethacrylate-Based Materials for Dental Applications; Elsevier: Amsterdam, The Netherlands, 2019; pp. 273–308. [Google Scholar]
- Arslan, M.; Alp, G.; Zaimoglu, A.; Murat, S. Evaluation of Flexural Strength and Surface Properties of Pre-polymerized CAD/CAM PMMA-Based Polymers Used for Digital 3D Complete Dentures. Int. J. Comput. Dent. 2018, 21, 31–40. [Google Scholar]
- Al-Dwairi, Z.N.; Tahboub, K.Y.; Baba, N.Z.; Goodacre, C.J. A comparison of the flexural and impact strengths and flexural modulus of CAD/CAM and conventional heat-cured polymethyl methacrylate (PMMA). J. Prosthodont. 2018, 29, 341–349. [Google Scholar] [CrossRef] [PubMed]
- Al-Dwairi, Z.N.; Tahboub, K.Y.; Baba, N.Z.; Goodacre, C.J.; Ozcan, M. A Comparison of the Surface Properties of CAD/CAM and Conventional Polymethylmethacrylate (PMMA). J. Prosthodont. 2019, 28, 452–457. [Google Scholar] [CrossRef]
- Bidra, A.S.; Taylor, T.D.; Agar, J.R. Computer-Aided Technology for Fabricating Complete Dentures: Systematic Review of Historical Background, Current Status, and Future Perspectives. J. Prosthet. Dent. 2013, 109, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.J.E.; Uy, C.E.; Plaksina, P.; Ramani, R.S.; Ganjigatti, R.; Waddell, J.N. Bond Strength of Denture Teeth to Heat-Cured, CAD/CAM and 3D Printed Denture Acrylics. J. Prosthodont. 2020, 29, 415–421. [Google Scholar] [CrossRef]
- Kalberer, N.; Mehl, A.; Schimmel, M.; Müller, F.; Srinivasan, M. CAD-CAM Milled versus Rapidly Prototyped (3D-Printed) Complete Dentures: An In Vitro Evaluation of Trueness. J. Prosthet. Dent. 2019, 121, 637–643. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira Limírio, J.; Gomes, J.; Alves Rezende, M.; Lemos, C.; Rosa, C.; Pellizzer, E.P. Mechanical Properties of Polymethyl Methacrylate as a Denture Base: Conventional versus CAD-CAM Resin—A Systematic Review and Meta-Analysis of In Vitro Studies. J. Prosthet. Dent. 2021, 128, 1221–1229. [Google Scholar] [CrossRef]
- Murat, S.; Alp, G.; Alatalı, C.; Uzun, M. In Vitro Evaluation of Adhesion of Candida Albicans on CAD/CAM PMMA-Based Polymers. J. Prosthodont. 2019, 28, 873–879. [Google Scholar] [CrossRef]
- Papathanasiou, I.; Kamposiora, P.; Papavasiliou, G.; Ferrari, M. The Use of PEEK in Digital Prosthodontics: A Narrative Review. BMC Oral Health 2020, 20, 217. [Google Scholar] [CrossRef]
- Alexakou, E.; Damanaki, M.; Zoidis, P.; Bakiri, E.; Mouzis, N.; Smidt, G.; Kourtis, S. PEEK High Performance Polymers: A Review of Properties and Clinical Applications in Prosthodontics and Restorative Dentis-Try. Eur. J. Prosthodont. Restor. Dent. 2019, 27, 113–121. [Google Scholar]
- Muhsin, S.A.; Wood, D.J.; Johnson, A.; Hatton, V.P. Effects of Novel Polyetheretherketone (PEEK) Clasp Design on Retentive Force at Different Tooth Undercuts. J. Oral Dent. Res. 2018, 5, 13–25. [Google Scholar]
- Peng, T.Y.; Ogawa, Y.; Akebono, H.; Iwaguro, S.; Sugeta, A.; Shimoe, S. Finite Element Analysis and Optimization of the Mechanical Properties of Polyetheretherketone (PEEK) Clasps for Removable Partial Dentures. J. Prosthodont. Res. 2020, 64, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Negm, E.E.; Aboutaleb, F.A.; Alam-Eldein, A.M. Virtual Evaluation of the Accuracy of Fit and Trueness in Maxillary Poly (Etheretherketone) Removable Partial Denture Frame-Works Fabricated by Direct and Indirect CAD/CAM Techniques. J. Prosthodont. 2019, 28, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Siddiqui, F. Applications of Polyetheretherketone (PEEK) in Oral Implantology and Prosthodontics. J. Prosthodont. Res. 2016, 60, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wu, P.; Liu, H.L.; Zhang, L.; Liu, L.P.; Ma, C.F.; Chen, J.H. Polyetheretherketone versus Titanium CAD-CAM Framework for Implant-Supported Fixed Complete Dentures: A Retrospective Study with Up to 5-Year Follow-Up. J. Prosthodont. Res. 2021, 66, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.; Hey, J.; Schweyen, R.; Setz, J.M. Accuracy of CAD-CAM-Fabricated Removable Partial Dentures. J. Prosthet. Dent. 2018, 119, 586–592. [Google Scholar] [CrossRef]
- Alamoush, R.A.; Silikas, N.; Salim, N.A.; Al-Nasrawi, S.; Satterthwaite, J.D. Effect of the Composition of CAD/CAM Composite Blocks on Mechanical Properties. BioMed Res. Int. 2018, 2018, 4893143. [Google Scholar] [CrossRef]
- Alamoush, R.A.; Salim, N.A.; Silikas, N.; Satterthwaite, J.D. Long-Term Hydrolytic Stability of CAD/CAM Composite Blocks. Eur. J. Oral Sci. 2022, 130, e12834. [Google Scholar] [CrossRef]
- Fonseca, A.S.Q.S.; Labruna Moreira, A.D.; de Albuquerque, P.P.A.C.; de Menezes, L.R.; Pfeifer, C.S.; Schneider, L.F.J. Effect of Monomer Type on the CC Degree of Conversion, Water Sorption and Solubility, and Color Stability of Model Dental Composites. Dent. Mater. 2017, 33, 394–401. [Google Scholar] [CrossRef]
- Marchesi, G.; Camurri Piloni, A.; Nicolin, V.; Turco, G.; Di Lenarda, R. Chairside CAD/CAM Materials: Current Trends of Clinical Uses. Biology 2021, 10, 1170. [Google Scholar] [CrossRef]
- Liebermann, A.; Wimmer, T.; Schmidlin, P.R.; Scherer, H.; Löffler, P.; Roos, M.; Stawarczyk, B. Physico Mechanical Characterization of Polyetheretherketone and Current Esthetic Dental CAD/CAM Polymers after Aging in Different Storage Media. J. Prosthet. Dent. 2016, 115, 321–328. [Google Scholar] [CrossRef]
- Monterubbianesi, R.; Tosco, V.; Sabbatini, S.; Orilisi, G.; Conti, C.; Özcan, M.; Orsini, G.; Putignano, A. How Can Different Polishing Timing Influence Methacrylate and Dimethacrylate Bulk Fill Composites? Evaluation of Chemical and Physical Properties. Biomed Res. Int. 2020, 2020, 1965818. [Google Scholar] [CrossRef]
- Alharbi, A.; Ardu, S.; Bortolotto, T.; Krejci, I. Stain Susceptibility of Composite and Ceramic CAD/CAM Blocks versus Direct Resin Composites with Different Resinous Matrices. Odontology 2017, 105, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M.A.; Skroch, M.; Schmidt, A.; Rehmann, P.; Wöstmann, B. Influence of Different Luting Systems on Microleakage of CAD/CAM Composite Crowns: A Pilot Study. Int. J. Prosthodont. 2019, 32, 530–532. [Google Scholar] [CrossRef] [PubMed]
- Vichi, A.; Goracci, C.; Carrabba, M.; Tozzi, G.; Louca, C. Flexural Resistance of CAD-CAM Blocks. Part 3: Polymer-Based Restorative Materials for Permanent Restorations. Am. J. Dent. 2020, 33, 243–247. [Google Scholar] [PubMed]
- Wendler, M.; Stenger, A.; Ripper, J.; Priewich, E.; Belli, R.; Lohbauer, U. Mechanical Degradation of Contemporary CAD/CAM Resin Composite Materials after Water Ageing. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2021, 37, 1156–1167. [Google Scholar] [CrossRef]
- Paolone, G.; Mandurino, M.; De Palma, F.; Mazzitelli, C.; Scotti, N.; Breschi, L.; Gherlone, E.; Cantatore, G.; Vichi, A. Color Stability of Polymer-Based Composite CAD/CAM Blocks: A Systematic Review. Polymers 2023, 15, 464. [Google Scholar] [CrossRef]
- Vichi, A.; Balestra, D.; Scotti, N.; Louca, C.; Paolone, G. Translucency of CAD/CAM, and 3D Printable Composite Materials for Permanent Dental Restorations. Polymers 2023, 15, 1443. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Focused Question (PICO) | Is There a Greater Range of Clinical Applications of CAD/CAM Materials than Traditional Ones Due to the Improvement of Their Mechanical Properties? | |
|---|---|---|
| Search strategy | Population | Teeth to be partially or totally rehabilitated |
| Intervention | CAD/CAM restorations teeth to be partially or totally rehabilitated | |
| Comparison | CAD/CAM restorations teeth to be partially or totally rehabilitated compared to Conventionally manufactured restorations due to their mechanical properties | |
| Outcome | Clinical Application of these materials in accordance with their mechanical properties | |
| Inclusion Criteria |
|---|
| Articles addressing at least one of the following topics regarding dental materials for CAD-CAM systems |
| clinical indications and/or outcomes; manufacturers; mechanical features (flexural strength, hardness, and elastic modulus); materials’ composition; optical properties. |
| In Vivo Studies |
| In Vitro Studies |
| Systematic Reviews |
| Narrative Reviews |
| Materials | Clinical Application | References |
|---|---|---|
| Silicate Ceramics | ||
| Feldespathic | inlay, onlay, anterior and posterior restorations and for veneers | Skorulska, A. et al. (2021) [19], Zhang Y. et al. (2018) [20], Gracis, Stefano et al. (2015) [21] |
| Leucite-reinforced | veneers, inlays, onlays, and single crowns | Gracis, Stefano et al. (2015) [21], H Ahmed et al. (2019) [22], Avram et al. (2022) [23], Veríssimo et al. 2019 [24] |
| Lithium silicate | single crowns (better in anterior regions), veneers and inlays/onlays | Hinz, Sebastian et al. (2022) [25] D’Addazio, Gianmaria et al. (2020) [26] |
| Lithium disilicate | veneers, inlays/onlays, single crowns or small bridges (up to 3 units) | Hinz, Sebastian et al. (2022) [25] D’Addazio, Gianmaria et al. (2020) [26] Mavriqi, Luan et al. (2021) [27] Fabian Fonzar et al. (2017) [28] Gardell E. et al., (2021) [29] Traini, Tonino et al. (2014) [30] |
| Oxide Ceramics | ||
| Zirconium | bridges in anterior or posterior region, up to entire full-arch rehabilitations on implants or natural teeth | Mirdamadi E.S. et al. (2021) [31] Li J. et al. (1998) [32] Guazzato, Massimiliano et al. (2004) [33] Monaco, Carlo et al. (2015) [34] Pihlaja, Juha et al. (2016) [35] Joda, Tim et al. (2021) [36] |
| Aluminum | anterior three-unit fixed dental prosthesis, crowns and for posterior rehabilitation | llenz, Maximiliane Amelie et al. (2021) [37] Ozer, Fusun et al. (2014) [38] Selz, Christian F et al. (2014) [39] |
| Hybrid Ceramics | ||
| Polymer infiltrated ceramic network (PICN) | veneers, inlays/onlays, anterior and posterior single crowns and for implant prostheses | Kawajiri, Yohei et al. (2021) [40] Kang, Longzhao et al. (2020) [41] Steinbrenner, Harald (2018) [42] Yano, Haruka Takesue et al. (2020) [43] Li, Ke et al. (2021) [44] |
| Nanoceramics | veneers, inlay/onlay, anterior and posterior single crowns, anterior and posterior bridges | Demirel, Akif et al. (2017) [45] Heck, Katrin et al. (2019) [46] Al Amri, Mohammad D et al. (2021) [47] Al-Harbi, Fahad A et al. (2017) [48] Yin, Ruizhi et al. (2019) [49] Ludovichetti, Francesco Saverio et al. (2018) [50] Lauvahutanon, Sasipin et al. (2017) [51] Kurtulmus-Yilmaz, Sevcan et al. (2019) [52] |
| Resin Matrix Ceramics | ||
| Polymethyl methacrylate (PMMA) | long term (up to one year) provisional restoration | Zafar, Muhammad Sohail (2020) [53] Hassan, M et al. (2019) [54] Arslan, Mustafa et al. (2018) [55] Al-Dwairi, Ziad N et al. (2018) [56] Al-Dwairi, Ziad N et al. (2019) [57] Bidra, Avinash S et al. (2013) [58] Choi, Joanne Jung Eun et al. (2020) [59] Kalberer, Nicole et al. (2019) [60] de Oliveira Limírio, João Pedro Justino et al. (2021) [61] Murat, Sema et al. (2019) [62] |
| Polyether Ether Ketone (PEEK) | mill frameworks for dentures or FDPs, three to four-unit FDPs, telescopic restorations, implant abutments, and secondary structures associated with bar-supported prostheses | Papathanasiou, Ioannis et al. (2020) [63] Alexakou, E et al. (2019) [64] Muhsin, S.A et al. (2018) [65] Peng, Tzu-Yu et al. (2020) [66] Negm, Enas Elhamy et al. (2019) [67] Najeeb, S et al. (2016) [68] Wang, Jing et al. (2021) [69] Arnold, Christin et al. (2018) [70] |
| Resin Block Composites | inlays, onlays, veneers, partial crowns, crowns, and multi-unit, up to three bridge units | Alamoush, Rasha A et al. (2018) [71] Alamoush, Rasha A et al. (2022) [72] Fonseca, Andrea Soares Q S et al. (2017) [73] Marchesi, Giulio et al. (2021) [74] Liebermann, Anja et al. (2016) [75] Monterubbianesi, Riccardo et al. (2020) [76] Alharbi, Amal et al. (2017) [77] Schlenz, Maximiliane Amelie et al. (2019) [78] Vichi, Alessandro et al. (2020) [79] Wendler, Michael et al. (2021) [80] Paolone G. et al. (2023) [81] Vichi Alessandro et al. (2023) [82] |
| Mechanical Properties: | Flexural Strength (MPa) | Vickers Hardness (VH) | Elastic Modulus (GPa) | References | Manufacturers |
|---|---|---|---|---|---|
| Silicate Ceramics | |||||
| Feldespathic | 97–133 | 640 ± 20 | 45 | [19,20,21] | CEREC Blocs (VITABLOC, Bad Säckingen, Germany) |
| Leucite-reinforced | 106–160 | 525–565 | 62–70 | [21,22,23,24] | IPS Empress CAD, (Ivoclar Vivadent, Liechtenstein) |
| Lithium silicate | 400 | up to 7000 | 70 | [25,26] | Suprinity PC (Vita Zahnfabrik, Bad Säckingen, Germany), Celtra Duo (Densply Sirona, Verona, Italy) |
| Lithium disilicate | 130 | 452–731 | 58–110 | [25,26,27,28,29,30] | IPS E. max CAD (Ivoclar Vivadent, Liechtenstein) |
| Oxide Ceramics | |||||
| Zirconium | 500–1200 | 12 | 210 | [31,32,33,34,35,36] | Nobelprocera Zirconia (Nobel Biocare, Kloten, Switzerland) Lava Plus, (3M ESPE, Milano, Italy) |
| Aluminum | 500 | 18.3 | 206 | [37,38,39] | InCeram Alumina (Vita Zahnfabrik, Bad Säckingen, Germany) |
| Hybrid Ceramics | |||||
| Polymer-infiltrated ceramic network (PICN) | 107.8–153.7 | 204.8–299.2 | 13.0–2.2 | [40,41,42,43,44] | VITA ENAMIC (Vita Zahnfabrik, Bad Säckingen, Germany), |
| Nanoceramics | 200 | 91.5 | 15 | [45,46,47,48,49,50,51,52] | Lava Ultimate (3M ESPE, Milano, Italy) |
| Resin Matrix Ceramics | |||||
| Polymethyl Methacrylate (PMMA) | 80–135 | 27.7411 | 2.68–3.43 | [53,54,55,56,57,58,59,60,61,62] | Telio CAD, Ivoclar Vivadent, VITA CAD-Temp MultiColor Blocks, (Vita Zahnfabrik, Bad Säckingen, Germany), |
| Polyether Ether Ketone (PEEK) | 165–185 | 26.1–28.5 | 4 | [63,64,65,66,67,68,69,70] | Juvora dental PEEK CAD/CAM-Rohling, Straumann, Bio High Performance Polymer, (Bredent, Senden, Germany) |
| Resin Block Composites | 80 | 65–98 | 2.8 | [71,72,73,74,75,76,77,78,79,80,81,82] | Grandio Blocks (VOCO GmbH, Cuxhaven, Germany), LuxaCam Composite (LUXA, DMG, Cheshire, UK) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rexhepi, I.; Santilli, M.; D’Addazio, G.; Tafuri, G.; Manciocchi, E.; Caputi, S.; Sinjari, B. Clinical Applications and Mechanical Properties of CAD-CAM Materials in Restorative and Prosthetic Dentistry: A Systematic Review. J. Funct. Biomater. 2023, 14, 431. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14080431
Rexhepi I, Santilli M, D’Addazio G, Tafuri G, Manciocchi E, Caputi S, Sinjari B. Clinical Applications and Mechanical Properties of CAD-CAM Materials in Restorative and Prosthetic Dentistry: A Systematic Review. Journal of Functional Biomaterials. 2023; 14(8):431. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14080431
Chicago/Turabian StyleRexhepi, Imena, Manlio Santilli, Gianmaria D’Addazio, Giuseppe Tafuri, Eugenio Manciocchi, Sergio Caputi, and Bruna Sinjari. 2023. "Clinical Applications and Mechanical Properties of CAD-CAM Materials in Restorative and Prosthetic Dentistry: A Systematic Review" Journal of Functional Biomaterials 14, no. 8: 431. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb14080431