
Changes in Gloss Alteration, Surface Roughness, and Color of Direct Dental Restorative Materials after Professional Dental Prophylaxis
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
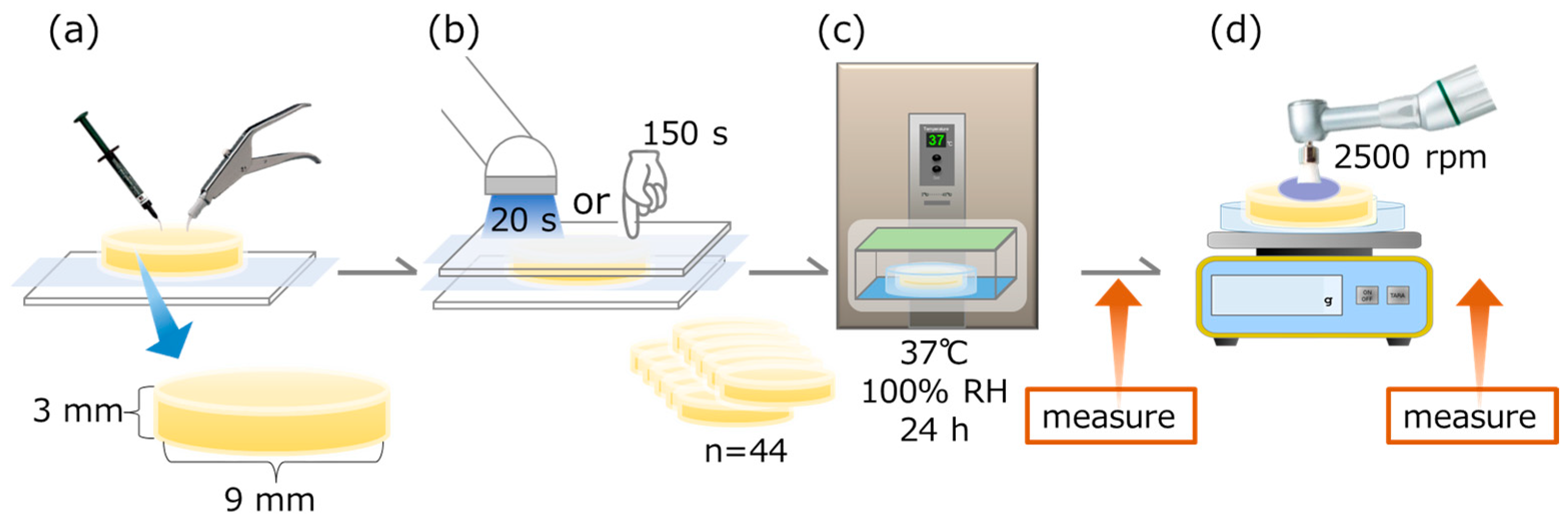
2.2. Specimen Preparation and Group Setting
- Group 1: Load of 100 gf, 10 s, 4×
- Group 2: Load of 100 gf, 30 s, 4×
- Group 3: Load of 300 gf, 10 s, 4×
- Group 4: Load of 300 gf, 30 s, 4×
2.3. Surface Gloss (Gs)
2.4. Surface Roughness
2.5. Initial Color
2.6. Professional Dental Prophylaxis
2.7. Color Change
Δa* = a*After − a*Before
Δb* = b*After − b*Before.
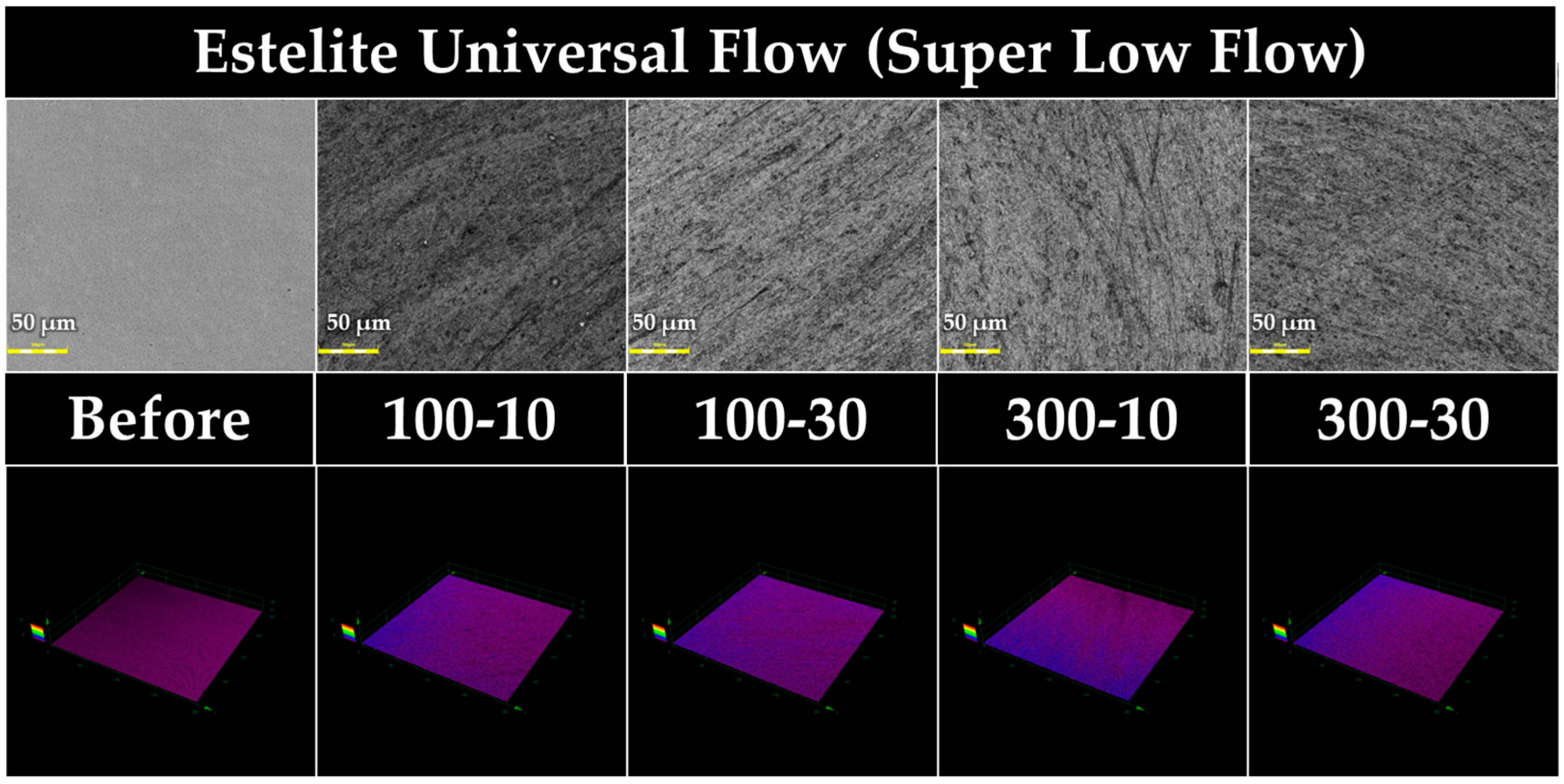
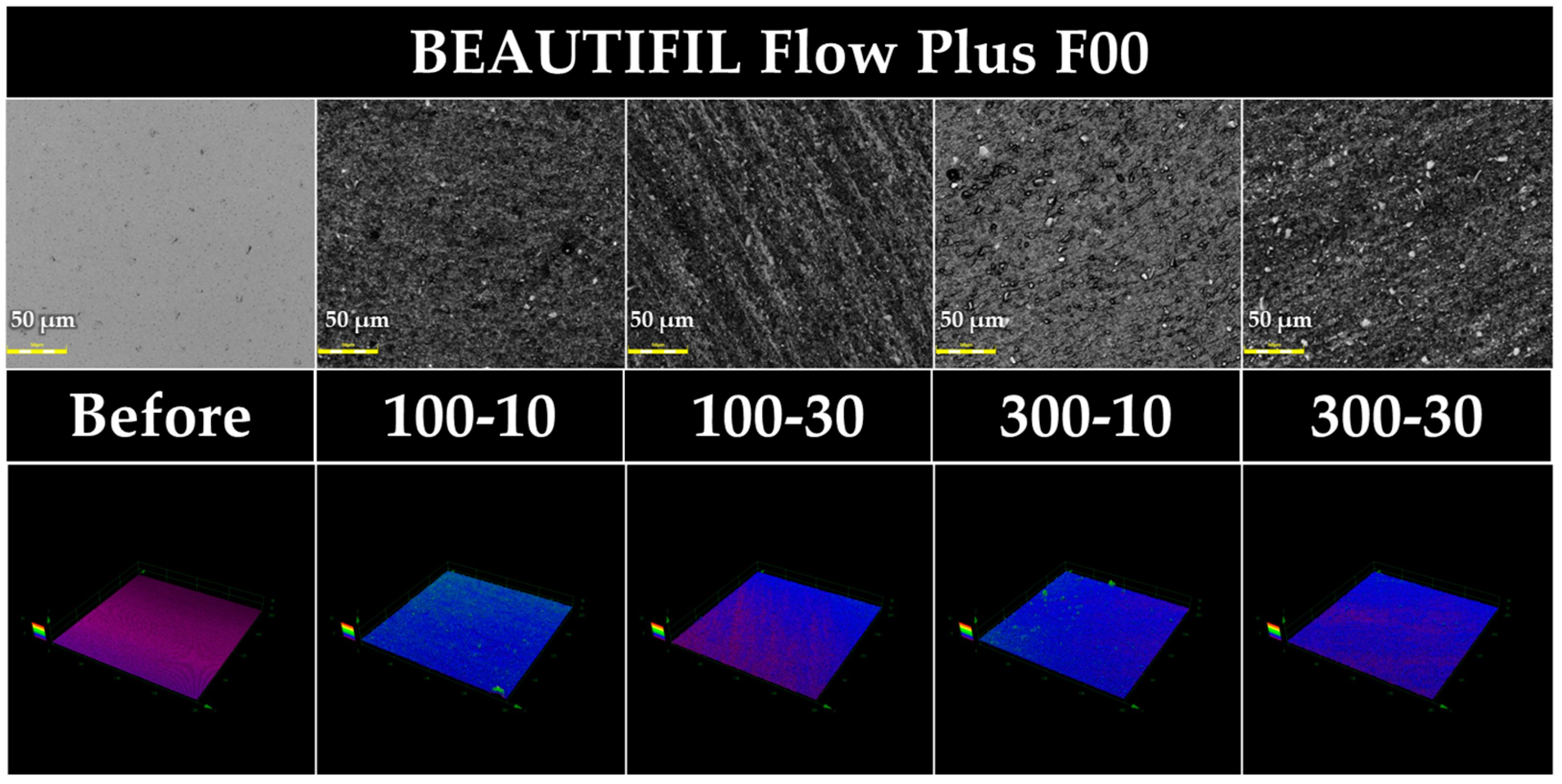
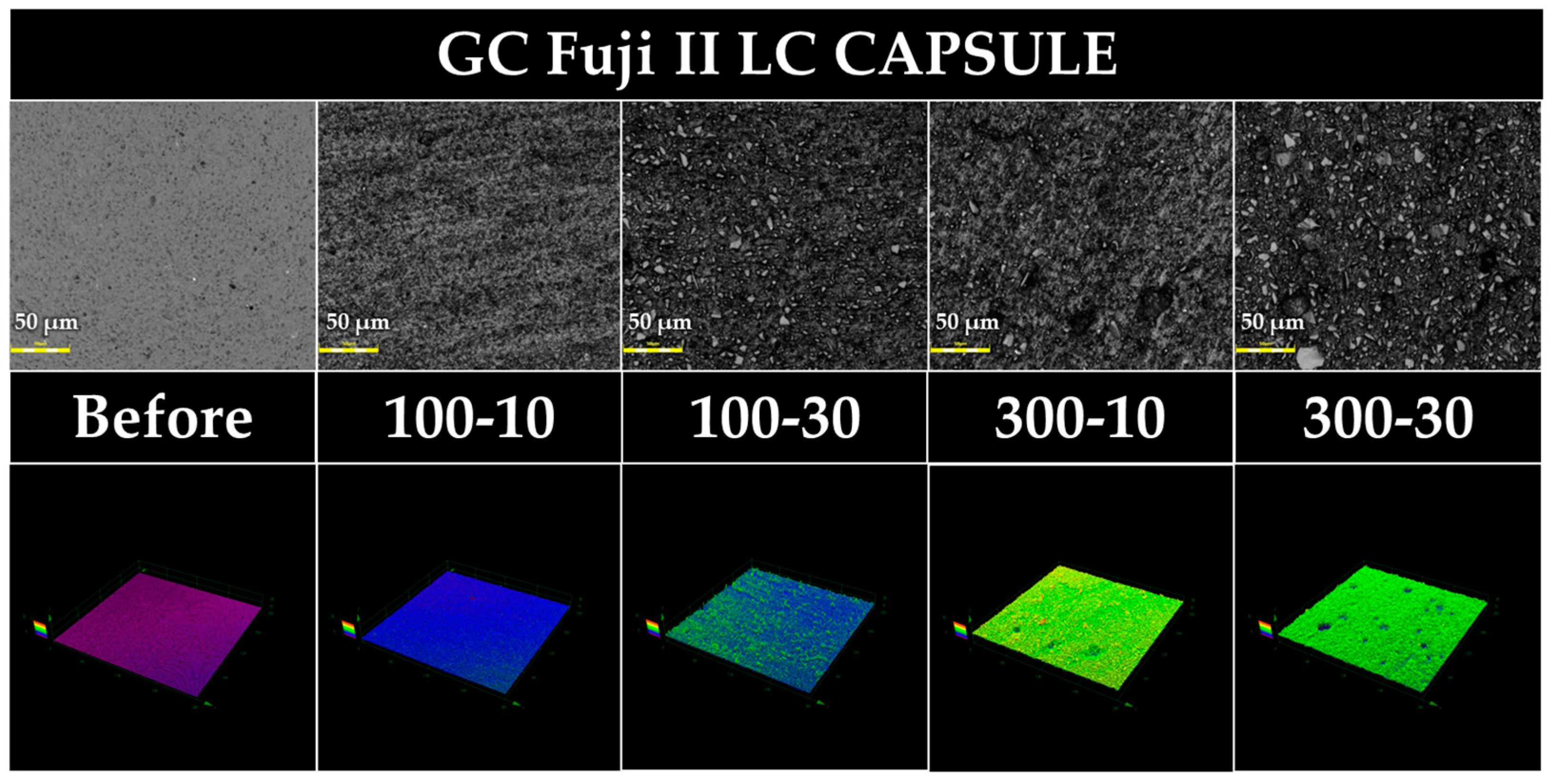
2.8. Surface Observation with a 3D Measuring Laser Microscope
2.9. Scanning Electron Microscopy Observations of the Prophylaxis Paste Particles
3. Results
3.1. Surface Gloss and Roughness of Baseline
3.2. Differences in Surface Gloss (Gs) Measured before and after Prophylaxis
3.3. Differences in Ra Values Measured before and after Prophylaxis
3.4. Differences in Rz Values Measured before and after Prophylaxis
3.5. Differences in Ry Values Measured before and after Prophylaxis
3.6. Color Change
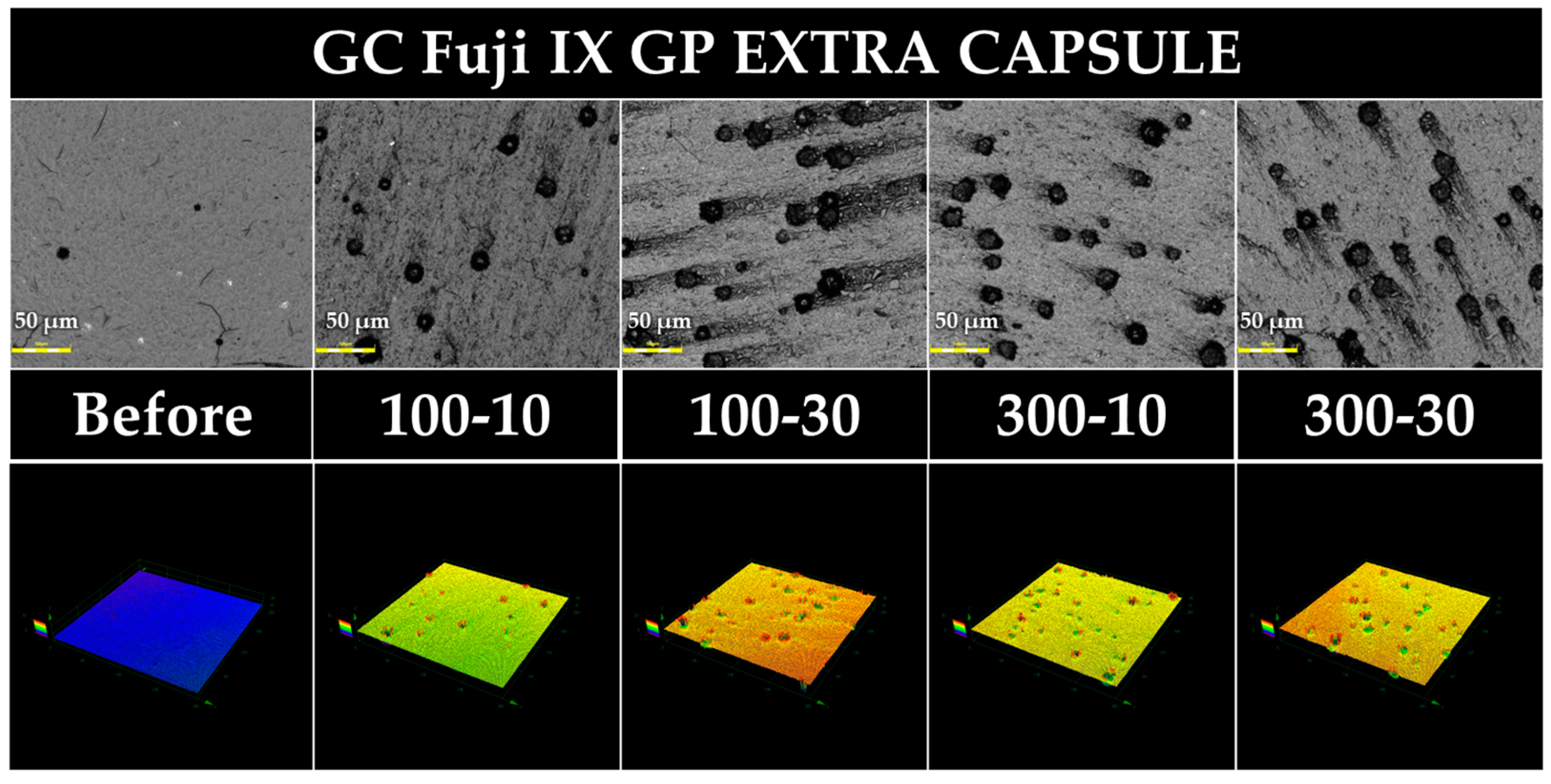
3.7. Three-Dimensional Measuring Laser Microscopy
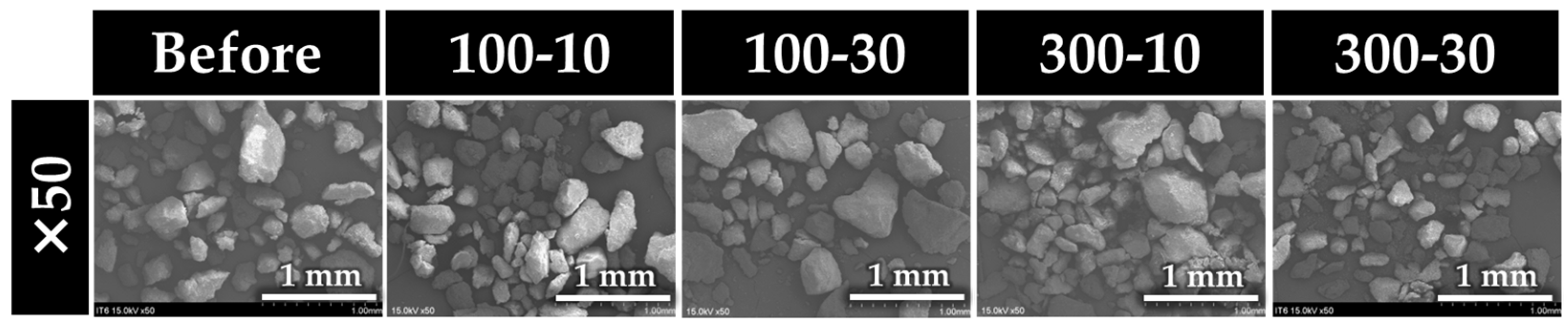
3.8. Scanning Electron Microscopy of Prophylaxis Paste Particles
4. Discussion
5. Conclusions
- Dental prophylaxis to direct dental restorative materials significantly reduces their surface gloss, except for FGP.
- Dental prophylaxis to direct dental restorative materials significantly increases their surface roughness for EUF, BFP, and FLC. However, the surface roughness parameters of FGP are substantially decreased after dental prophylaxis.
- Dental prophylaxis to direct dental restorative materials does not affect their color change.
- The higher loadings and longer durations of dental prophylaxis might affect the surface gloss and roughness, depending on the material.
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shinsyo, F. New strategy for better geriatric oral health in Japan: 80/20 movement and Healthy Japan 21. Int. Dent. J. 2001, 51 (Suppl. 3), 200–206. [Google Scholar] [CrossRef]
- Uchikawa, R.; Sadaoka, S.; Kawahara, I.; Oki, E.; Otogoto, J.; Yamamoto, A.; Tomida, M. Oral health and lifestyle to keep many teeth in elderly people. Oral Health Dent. Sci. 2020, 4, 1–5. [Google Scholar] [CrossRef]
- The 8020 Promotion Foundation. Outline of Its Objectives and Operations. Available online: https://www.8020zaidan.or.jp/english/ (accessed on 1 July 2023).
- Motegi, E.; Nomura, M.; Tachiki, C.; Miyazaki, H.; Takeuchi, F.; Takaku, S.; Abe, Y.; Miyatani, M.; Ogai, T.; Fuma, A.; et al. Occlusal force in people in their sixties attending college for elderly. Bull. Tokyo Dent. Coll. 2009, 50, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.; Pearson, A. Oral hygiene care for residents with dementia: A literature review. J. Adv. Nurs. 2005, 52, 410–419. [Google Scholar] [CrossRef] [PubMed]
- Dermont, M.A.; Sadaghiani, S.S. Integrating oral health into a dementia care pathway. Community Dent. Health 2014, 31, 196–199. [Google Scholar] [PubMed]
- Hashimoto, M.; Yamanaka, K.; Shimosato, T.; Ozawa, A.; Takigawa, T.; Hidaka, S.; Sakai, T.; Noguchi, T. Oral condition and health status of elderly 8020 achievers in Aichi Prefecture. Bull. Tokyo Dent. Coll. 2006, 47, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Ishimaru, M.; Ono, S.; Morita, K.; Matsui, H.; Yasunaga, H. Domiciliary dental care among homebound older adults: A nested case-control study in Japan. Geriatr. Gerontol. Int. 2019, 19, 679–683. [Google Scholar] [CrossRef]
- Webb, B.C.; Whittle, T.; Schwarz, E. Oral health and dental care in aged care facilities in New South Wales, Australia. Part 3 concordance between residents’ perceptions and a professional dental examination. Gerodontology 2016, 33, 363–372. [Google Scholar] [CrossRef]
- Yamaga, T.; Yoshihara, A.; Ando, Y.; Yoshitake, Y.; Kimura, Y.; Shimada, M.; Nishimuta, M.; Miyazaki, H. Relationship between dental occlusion and physical fitness in an elderly population. J. Gerontol. A Biol. Sci. Med. Sci. 2002, 57, M616–M620. [Google Scholar] [CrossRef]
- Sjogren, P.; Wardh, I.; Zimmerman, M.; Almstahl, A.; Wikstrom, M. Oral care and mortality in older adults with pneumonia in hospitals or nursing homes: Systematic review and meta-analysis. J. Am. Geriatr. Soc. 2016, 64, 2109–2115. [Google Scholar] [CrossRef]
- O’Donnell, L.E.; Smith, K.; Williams, C.; Nile, C.J.; Lappin, D.F.; Bradshaw, D.; Lambert, M.; Robertson, D.P.; Bagg, J.; Hannah, V.; et al. Dentures are a reservoir for respiratory pathogens. J. Prosthodont. 2016, 25, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Hariyani, N.; Spencer, A.J.; Luzzi, L.; Do, L.G. Root surface caries among older Australians. Community Dent. Oral Epidemiol. 2018, 46, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Griffin, S.O.; Regnier, E.; Griffin, P.M.; Huntley, V. Effectiveness of fluoride in preventing caries in adults. J. Dent. Res. 2007, 86, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Sardana, D.; Li, K.Y.; Leung, K.C.M.; Lo, E.C.M. Topical fluoride to prevent root caries: Systematic review with network meta-analysis. J. Dent. Res. 2020, 99, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.K.Y.; Tamrakar, M.; Jiang, C.M.; Tsang, Y.C.; Leung, K.C.M.; Chu, C.H. Clinical evidence for professionally applied fluoride therapy to prevent and arrest dental caries in older adults: A systematic review. J. Dent. 2022, 125, 104273. [Google Scholar] [CrossRef] [PubMed]
- Crystal, Y.O.; Niederman, R. Evidence-based dentistry update on silver diamine fluoride. Dent. Clin. N. Am. 2019, 63, 45–68. [Google Scholar] [CrossRef] [PubMed]
- Meyer-Lueckel, H.; Machiulskiene, V.; Giacaman, R.A. How to intervene in the root caries process? Systematic review and meta-analyses. Caries Res. 2019, 53, 599–608. [Google Scholar] [CrossRef]
- Islam, M.S.; Aal-Fatlah, A.A.; Alkhan, N.S.; Aryal Ac, S.; Sadr, A.; Rehman, M.M. The effect of different finishing polishing protocols on stain absorption and color stability of resin composite restorations. Am. J. Dent. 2022, 35, 141–145. [Google Scholar]
- Carlén, A.; Nikdel, K.; Wennerberg, A.; Holmberg, K.; Olsson, J. Surface characteristics and in vitro biofilm formation on glass ionomer and composite resin. Biomaterials 2001, 22, 481–487. [Google Scholar] [CrossRef]
- Lima, F.G.; Romano, A.R.; Correa, M.B.; Demarco, F.F. Influence of microleakage, surface roughness and biofilm control on secondary caries formation around composite resin restorations: An in situ evaluation. J. Appl. Oral Sci. 2009, 17, 61–65. [Google Scholar] [CrossRef]
- Kameyama, A.; Nakazawa, T.; Haruyama, A.; Haruyama, C.; Hosaka, M.; Hirai, Y. Influence of finishing/polishing procedures on the surface texture of two resin composites. Open Dent. J. 2008, 2, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Kocaagaoglu, H.; Aslan, T.; Gürbulak, A.; Albayrak, H.; Taşdemir, Z.; Gumus, H. Efficacy of polishing kits on the surface roughness and color stability of different composite resins. Niger. J. Clin. Pract. 2017, 20, 557–565. [Google Scholar] [CrossRef] [PubMed]
- da Costa, J.B.; Ferracane, J.L.; Amaya-Pajares, S.; Pfefferkorn, F. Visually acceptable gloss threshold for resin composite and polishing systems. J. Am. Dent. Assoc. 2021, 152, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, G.D.; Sandalli, N.; Selvi-Kuvvetli, S.; Topcuoglu, N.; Kulekci, G. Effect of two different polishing systems on fluoride release, surface roughness and bacterial adhesion of newly developed restorative materials. J. Esthet. Restor. Dent. 2017, 29, 424–434. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Yu, P.; Wang, X.-Y. Surface roughness and gloss of polished nanofilled and nanohybrid resin composites. J. Dent. Sci. 2021, 16, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Amaya-Pajares, S.P.; Koi, K.; Watanabe, H.; da Costa, J.B.; Ferracane, J.L. Development and maintenance of surface gloss of dental composites after polishing and brushing: Review of the literature. J. Esthet. Restor. Dent. 2022, 34, 15–41. [Google Scholar] [CrossRef] [PubMed]
- Ismail, H.S.; Ali, A.I.; Abo El-Ella, M.A.; Mahmoud, S.H. Effect of different polishing techniques on surface roughness and bacterial adhesion of three glass ionomer-based restorative materials: In vitro study. J. Clin. Exp. Dent. 2020, 12, e620–e625. [Google Scholar] [CrossRef]
- Warren, D.P.; Colescott, T.D.; Henson, H.A.; Powers, J.M. Effects of four prophylaxis pastes on surface roughness of a composite, a hybrid ionomer, and a compomer restorative material. J. Esthet. Restor. Dent. 2002, 14, 245–251. [Google Scholar] [CrossRef]
- Wu, S.S.; Yap, A.U.; Chelvan, S.; Tan, E.S. Effect of prophylaxis regimens on surface roughness of glass ionomer cements. Oper. Dent. 2005, 30, 180–184. [Google Scholar]
- Gomes, I.A.; Mendes, H.G.; Filho, E.M.M.; de C Rizzi, C.; Nina, M.G.; Turssi, C.P.; Vasconcelos, A.J.; Bandeca, M.C.; de Jesus Tavarez, R.R. Effect of dental prophylaxis techniques on the surface roughness of resin composites. J. Contemp. Dent. Pract. 2018, 19, 37–41. [Google Scholar] [CrossRef]
- Sugiyama, T.; Kameyama, A.; Enokuchi, T.; Haruyama, A.; Chiba, A.; Sugiyama, S.; Hosaka, M.; Takahashi, T. Effect of professional dental prophylaxis on the surface gloss and roughness of CAD/CAM restorative materials. J. Clin. Exp. Dent. 2017, 9, e772–e778. [Google Scholar] [CrossRef] [PubMed]
- Uchikawa, R.; Oki, A.; Haruyama, A.; Sugiyama, T.; Komachiya, M.; Komatsu, S.; Kohda, K.; Okuse, T.; Mori, H.; Yoshinari, N.; et al. Professional mechanical tooth cleaning using one-step prophylaxis paste: Effect of load and polishing time on the surface gloss and roughness of CAD/CAM restorative materials. Jpn. J. Conserv. Dent. 2020, 63, 166–172. [Google Scholar] [CrossRef]
- Kameyama, A.; Haruyama, A.; Asami, M.; Takahashi, T. Effect of emitted wavelength and light guide type on irradiance discrepancies in hand-held dental curing radiometers. Sci. World J. 2013, 2013, 647941. [Google Scholar] [CrossRef] [PubMed]
- Abu-Bakr, N.; Han, L.; Okamoto, A.; Iwaku, M. Color stability of compomer after immersion in various media. J. Esthet. Dent. 2000, 12, 258–263. [Google Scholar] [CrossRef]
- Fay, R.M.; Servos, T.; Powers, J.M. Color of restorative materials after staining and bleaching. Oper. Dent. 1999, 24, 292–296. [Google Scholar]
- Christensen, R.P.; Bangerter, V.W. Determination of rpm, time, and load used in oral prophylaxis polishing in vivo. J. Dent. Res. 1984, 63, 1376–1382. [Google Scholar] [CrossRef]
- Hodges, K. (Ed.) Concepts in Nonsurgical Periodontal Therapy, 1st ed.; Delmar: New York, NY, USA, 1998; pp. 345–366. [Google Scholar]
- Onoue, A.; Inukai, J.; Nakagaki, H.; Mukai, M. Changes in surface roughness of human enamel due to mechanical tooth polishing. J. Dent. Health. 2013, 63, 35–42. [Google Scholar] [CrossRef]
- Fleming, G.J.; Marquis, P.M.; Shortall, A.C. The influence of clinically induced variability on the distribution of compressive fracture strengths of a hand-mixed zinc phosphate dental cement. Dent. Mater. 1999, 15, 87–97. [Google Scholar] [CrossRef]
- Dowling, A.H.; Fleming, G.J. Are encapsulated anterior glass-ionomer restoratives better than their hand-mixed equivalents? J. Dent. 2009, 37, 133–140. [Google Scholar] [CrossRef]
- Pameijer, C.H.; Garcia-Godoy, F.; Morrow, B.R.; Jefferies, S.R. Flexural strength and flexural fatigue properties of resin-modified glass ionomers. J. Clin. Dent. 2015, 26, 23–27. [Google Scholar]
- Al-Taee, L.; Deb, S.; Banerjee, A. An in vitro assessment of the physical properties of the physical properties of manually- mixed and encapsulated glass-ionomer cements. BDJ Open. 2020, 6, 12. [Google Scholar] [CrossRef]
- Aung, S.Z.; Takagaki, T.; Ikeda, M.; Nozaki, K.; Burrow, M.F.; Abdou, A.; Nikaido, T.; Tagami, J. The effect of different light curing units on Vickers microhardness and degree of conversion of flowable resin composites. Dent. Mater. J. 2021, 40, 44–51. [Google Scholar] [CrossRef]
- Jassé, F.F.; de Campos, E.A.; Lefever, D.; Di Bella, E.; Salomon, J.P.; Krejci, I.; Ardu, S. Influence of filler charge on gloss of composite materials before and after in vitro toothbrushing. J. Dent. 2013, 41 (Suppl. 5), 41–44. [Google Scholar] [CrossRef]
- Campbell, P.M.; Johnston, W.M.; O’Brien, W.J. Light scattering and gloss of an experimental quartz-filled composite. J. Dent. Res. 1986, 65, 892–894. [Google Scholar] [CrossRef]
- Lee, Y.K.; Lu, H.; Oguri, M.; Powers, J.M. Changes in gloss after simulated generalized wear of composite resins. J. Prosthet. Dent. 2005, 94, 370–376. [Google Scholar] [CrossRef]
- Hondrum, S.O.; Fernández, R., Jr. Contouring, finishing, and polishing Class 5 restorative materials. Oper. Dent. 1997, 22, 30–36. [Google Scholar]
- Komalsingsakul, A.; Srisatjaluk, R.L.; Senawongse, P. Effect of brushing on surface roughness, fluoride release, and biofilm formation with different tooth-colored materials. J. Dent. Sci. 2022, 17, 389–398. [Google Scholar] [CrossRef]
- Miyano, Y.; Suzuki, M.; Shinkai, K. Toothbrush abrasion of restorations fabricated with flowable resin composites with different viscosities in vitro. Materials 2021, 14, 6436. [Google Scholar] [CrossRef]
- Hosoya, Y.; Shiraishi, T.; Odatsu, T.; Ogata, T.; Miyazaki, M.; Powers, J.M. Effects of specular component and polishing on color of resin composites. J. Oral Sci. 2010, 52, 599–607. [Google Scholar] [CrossRef]
- Shinkai, K.; Taira, Y.; Suzuki, S.; Suzuki, M. In vitro wear of flowable resin composite for posterior restorations. Dent. Mater. J. 2016, 35, 37–44. [Google Scholar] [CrossRef]
- Hosoya, Y.; Shiraishi, T.; Ando, S.; Miyazaki, M.; Garcia-Godoy, F. Effects of polishing on surface roughness and gloss of S-PRG filled flowable resin composite. Am. J. Dent. 2012, 25, 227–230. [Google Scholar] [PubMed]
- Bala, O.; Arisu, H.D.; Yikilgan, I.; Arslan, S.; Gullu, A. Evaluation of surface roughness and hardness of different glass ionomer cements. Eur. J. Dent. 2012, 6, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Bennett, H.E.; Porteus, J.O. Relation between surface roughness and specular reflectance at normal incidence. J. Opt. Soc. Am. 1961, 51, 123–129. [Google Scholar] [CrossRef]
- Bollen, C.M.; Papaioanno, W.; Van Eldere, J.; Schepers, E.; Quirynen, M.; van Steenberghe, D. The influence of abutment surface roughness on plaque accumulation and peri-implant mucositis. Clin. Oral Implant. Res. 1996, 7, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Ghinea, R.; Ugarte-Alvan, L.; Yebra, A.; Pecho, O.E.; Paravina, R.D.; Perez, M.; Perez, M.D.M. Influence of surface roughness on the color of dental-resin composites. J. Zhejiang Univ. Sci. B 2011, 12, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Kameyama, A.; Tsukamoto, R.; Haruyama, C.; Nakazawa, Y.; Hirai, Y.; Koga, H.; Tomori, T.; Ishihara, H.; Matsukubo, T.; Takaesu, Y. A study on fluoride release and uptake from various restorative materials in vitro. Shikwa Gakuho 1999, 99, 383–392. [Google Scholar]
- Torii, Y.; Itota, T.; Okamoto, M.; Nakabo, S.; Nagamine, M.; Inoue, K. Inhibition of artificial secondary caries in root by fluoride-releasing restorative materials. Oper. Dent. 2001, 26, 36–43. [Google Scholar]
- Smales, R.J.; Gao, W. In vitro caries inhibition at the enamel margins of glass ionomer restoratives developed for the ART approach. J. Dent. 2000, 28, 249–256. [Google Scholar] [CrossRef]
- Yoshihara, K.; Nagaoka, N.; Maruo, Y.; Sano, H.; Yoshida, Y.; Van Meerbeek, B. Bacterial adhesion not inhibited by ion-releasing bioactive glass filler. Dent. Mater. 2017, 33, 723–734. [Google Scholar] [CrossRef]
- Ruyter, I.E.; Nilner, K.; Moller, B. Color stability of dental composite resin materials for crown and bridge veneers. Dent. Mater. 1987, 3, 246–251. [Google Scholar] [CrossRef]
- Vichi, A.; Ferrari, M.; Davidson, C.L. Color and opacity variations in three different resin-based composite products after water aging. Dent. Mater. 2004, 20, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Paolone, G.; Formiga, S.; De Palma, F.; Abbruzzese, L.; Chirico, L.; Scolavino, S.; Goracci, C.; Cantatore, G.; Vichi, A. Color stability of resin-based composites: Staining procedures with liquids—A narrative review. J. Esthet. Restor. Dent. 2022, 34, 865–887. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Lee, M.J.; Oh, S.H.; Kim, K.M. Changes in the physical properties and color stability of aesthetic restorative materials caused by various beverages. Dent. Mater. J. 2019, 38, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Aydın, N.; Topçu, F.T.; Karaoğlanoğlu, S.; Oktay, E.A.; Erdemir, U. Effect of finishing and polishing systems on the surface roughness and color change of composite resins. J. Clin. Exp. Dent. 2021, 13, 446–454. [Google Scholar] [CrossRef]
- Padilla, K.; Savage, K.; Kim, H.J.; Poon, E.; Diaz, D.; Garcia-Godoy, F.; Oyoyo, U.; Kwon, S.R. Effect of toothpaste tablets on gloss and surface roughness of resin-based composite materials. Am. J. Dent. 2023, 36, 156–160. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product Name (Manufacturer) | Shade | Principal Ingredient | Lot No. | Code |
|---|---|---|---|---|
| (Resin-based composite restorative material) | ||||
| Estelite Universal Flow (Super Low Flow) (Tokuyama Dental, Tokyo, Japan) | A3 | Silica–zirconia filler, Bis-GMA, Bis-MPEPP, TEGDMA, UDMA, CQ, other | 070021 | EUF |
| BEAUTIFIL Flow Plus F00 (Shofu, Kyoto, Japan) | A3 | Bis-GMA, TEGDMA, glass powder, other | 042169 | BFP |
| (Glass–ionomer-based restorative material) | ||||
| GC Fuji II LC CAPSULE (GC, Tokyo, Japan) | A3 | Powder: fluoroaluminosilicate glass Liquids: methacrylic acid ester, polyacrylic acid, distilled water | 2101121 2106122 | FLC |
| GC Fuji IX GP EXTRA CAPSULE (GC, Tokyo, Japan) | A3 | Powder: fluoroaluminosilicate glass, polyacrylic acid Liquids: polyacrylic acid, distilled water, polybasic carboxylic acid | 2101252 2109201 | FGP |
| (Prophylactic paste) | ||||
| Prophy Paste PRO (Directa AB, Upplands Väsby, Sweden) | Glycerin, sodium dihydrogen phosphate, water, other | 33248 |
| Gs (%) | Ra (µm) | Rz (µm) | Ry (µm) | |
|---|---|---|---|---|
| Estelite Universal Flow | 85.5 (5.8) a | 0.063 (0.013) a | 0.357 (0.108) a | 0.436 (0.128) b |
| BEAUTIFIL Flow Plus | 89.4 (2.9) a | 0.059 (0.013) a | 0.251 (0.088) a | 0.284 (0.102) a |
| GC Fuji II LC CAPSULE | 72.4 (6.3) b | 0.145 (0.023) b | 0.624 (0.130) b | 0.911 (0.177) c |
| GC Fuji IX GP EXTRA CAPSULE | 63.5 (9.9) c | 0.287 (0.061) c | 1.439 (0.354) c | 2.014 (0.441) d |
| Baseline | After Prophylaxis | ΔGs | |
|---|---|---|---|
| Estelite Universal Flow | |||
| 100 gf–10 s | 88.2 (4.4) a | 63.7 (5.1) def | 24.51 |
| 100 gf–30 s | 82.4 (5.7) abc | 52.1 (4.7) ghi | 30.36 |
| 300 gf–10 s | 84.2 (6.6) ab | 60.7 (6.8) efg | 23.52 |
| 300 gf–30 s | 87.1 (5.4) a | 43.1 (3.3) ij | 43.96 |
| BEAUTIFIL Flow Plus | |||
| 100 gf–10 s | 88.1 (3.7) a | 56.6 (6.2) fgh | 31.48 |
| 100 gf–30 s | 90.1 (2.7) a | 43.0 (11.4) ij | 47.09 |
| 300 gf–10 s | 90.6 (2.1) a | 23.6 (5.3) kl | 67.00 |
| 300 gf–30 s | 88.7 (2.4) a | 23.7 (11.6) kl | 64.95 |
| GC Fuji II LC CAPSULE | |||
| 100 gf–10 s | 71.5 (6.0) cde | 50.6 (6.0) ghi | 20.95 |
| 100 gf–30 s | 72.0 (6.9) cde | 34.0 (4.0) jk | 38.00 |
| 300 gf–10 s | 74.9 (5.4) bcd | 26.2 (6.1) kl | 48.72 |
| 300 gf–30 s | 71.2 (7.0) cde | 15.1 (2.9) l | 56.13 |
| GC Fuji IX GP EXTRA CAPSULE | |||
| 100 gf–10 s | 61.6 (7.5) efg | 61.6 (4.3) efg | −0.07 |
| 100 gf–30 s | 61.3 (13.4) efg | 48.8 (7.9) hi | 12.51 |
| 300 gf–10 s | 61.9 (10.0) efg | 55.8 (4.3) fgh | 6.19 |
| 300 gf–30 s | 69.1 (6.4) de | 46.7 (9.5) hi | 22.39 |
| Baseline | After Prophylaxis | ΔRa | |
|---|---|---|---|
| Estelite Universal Flow | |||
| 100 gf–10 s | 0.064 (0.007) i | 0.058 (0.019) i | −0.006 |
| 100 gf–30 s | 0.068 (0.014) i | 0.070 (0.015) i | 0.002 |
| 300 gf–10 s | 0.064 (0.017) i | 0.063 (0.014) i | 0.000 |
| 300 gf–30 s | 0.057 (0.013) i | 0.069 (0.022) i | 0.012 |
| BEAUTIFIL Flow Plus | |||
| 100 gf–10 s | 0.050 (0.010) i | 0.059 (0.008) i | 0.009 |
| 100 gf–30 s | 0.056 (0.010) i | 0.095 (0.026) hi | 0.039 |
| 300 gf–10 s | 0.063 (0.013) i | 0.111 (0.020) ghi | 0.048 |
| 300 gf–30 s | 0.066 (0.014) i | 0.135 (0.019) fgh | 0.069 |
| GC Fuji II LC CAPSULE | |||
| 100 gf–10 s | 0.151 (0.027) fgh | 0.157 (0.032) efgh | 0.006 |
| 100 gf–30 s | 0.150 (0.024) fgh | 0.160 (0.060) efg | 0.010 |
| 300 gf–10 s | 0.137 (0.021) fgh | 0.165 (0.040) defg | 0.029 |
| 300 gf–30 s | 0.144 (0.021) fgh | 0.171 (0.029) defg | 0.028 |
| GC Fuji IX GP EXTRA CAPSULE | |||
| 100 gf–10 s | 0.271 (0.053) abc | 0.222 (0.045) bcd | −0.049 |
| 100 gf–30 s | 0.280 (0.080) ab | 0.217 (0.083) cde | −0.063 |
| 300 gf–10 s | 0.295 (0.056) a | 0.182 (0.054) def | −0.114 |
| 300 gf–30 s | 0.300 (0.056) a | 0.167 (0.037) defg | −0.133 |
| Baseline | After Prophylaxis | ΔRz | |
|---|---|---|---|
| Estelite Universal Flow | |||
| 100 gf–10 s | 0.445 (0.099) fgh | 0.347 (0.143) gh | −0.098 |
| 100 gf–30 s | 0.329 (0.085) gh | 0.305 (0.087) gh | −0.024 |
| 300 gf–10 s | 0.354 (0.106) gh | 0.339 (0.163) gh | −0.015 |
| 300 gf–30 s | 0.301 (0.098) gh | 0.316 (0.099) gh | 0.014 |
| BEAUTIFIL Flow Plus | |||
| 100 gf–10 s | 0.235 (0.092) h | 0.287 (0.092) gh | 0.052 |
| 100 gf–30 s | 0.227 (0.062) h | 0.452 (0.099) fgh | 0.225 |
| 300 gf–10 s | 0.270 (0.109) gh | 0.477 (0.095) fgh | 0.206 |
| 300 gf–30 s | 0.273 (0.086) gh | 0.603 (0.092) efgh | 0.330 |
| GC Fuji II LC CAPSULE | |||
| 100 gf–10 s | 0.661 (0.111) efg | 0.806 (0.215) def | 0.145 |
| 100 gf–30 s | 0.639 (0.150) efg | 0.874 (0.442) cde | 0.235 |
| 300 gf–10 s | 0.586 (0.149) efgh | 0.940 (0.359) cde | 0.354 |
| 300 gf–30 s | 0.611 (0.111) efgh | 0.775 (0.149) def | 0.163 |
| GC Fuji IX GP EXTRA CAPSULE | |||
| 100 gf–10 s | 1.339 (0.314) ab | 1.108 (0.263) bcd | −0.231 |
| 100 gf–30 s | 1.441 (0.447) ab | 1.237 (0.539) abc | −0.205 |
| 300 gf–10 s | 1.445 (0.279) ab | 0.899 (0.356) cde | −0.547 |
| 300 gf–30 s | 1.530 (0.383) a | 0.839 (0.253) def | −0.691 |
| Baseline | After Prophylaxis | ΔRy | |
|---|---|---|---|
| Estelite Universal Flow | |||
| 100 gf–10 s | 0.532 (0.123) hijk | 0.412 (0.160) jk | −0.120 |
| 100 gf–30 s | 0.422 (0.101) ijk | 0.383 (0.124) jk | −0.039 |
| 300 gf–10 s | 0.436 (0.124) ijk | 0.420 (0.184) jk | −0.016 |
| 300 gf–30 s | 0.355 (0.117) jk | 0.407 (0.152) jk | 0.052 |
| BEAUTIFIL Flow Plus | |||
| 100 gf–10 s | 0.278 (0.102) k | 0.360 (0.113) jk | 0.081 |
| 100 gf–30 s | 0.260 (0.079) k | 0.623 (0.154) ghijk | 0.363 |
| 300 gf–10 s | 0.312 (0.142) k | 0.687 (0.137) ghijk | 0.375 |
| 300 gf–30 s | 0.284 (0.082) k | 0.831 (0.166) fghij | 0.546 |
| GC Fuji II LC CAPSULE | |||
| 100 gf–10 s | 0.969 (0.176) fgh | 1.096 (0.264) efg | 0.127 |
| 100 gf–30 s | 0.951 (0.208) fgh | 1.209 (0.559) def | 0.258 |
| 300 gf–10 s | 0.823 (0.176) fghij | 1.274 (0.343) def | 0.451 |
| 300 gf–30 s | 0.900 (0.127) fghi | 1.172 (0.225) def | 0.272 |
| GC Fuji IX GP EXTRA CAPSULE | |||
| 100 gf–10 s | 1.871 (0.280) abc | 1.555 (0.357) cde | −0.316 |
| 100 gf–30 s | 1.927 (0.533) abc | 1.648 (0.646) bcd | −0.278 |
| 300 gf–10 s | 2.152 (0.458) a | 1.199 (0.355) def | −0.954 |
| 300 gf–30 s | 2.107 (0.456) ab | 1.205 (0.351) def | −0.902 |
| Estelite Universal Flow | Beautifil Flow Plus | GC Fuji II LC CAPSULE | GC Fuji IX GP EXTRA CAPSULE | |
|---|---|---|---|---|
| 100 gf–10 s | 0.391 | 0.594 | 0.450 | 0.124 |
| 100 gf–30 s | 0.185 | 2.100 | 0.995 | 0.200 |
| 300 gf–10 s | 0.692 | 1.020 | 0.659 | 0.341 |
| 300 gf–30 s | 0.516 | 1.021 | 1.673 | 0.224 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyashita-Kobayashi, A.; Haruyama, A.; Nakamura, K.; Wu, C.-Y.; Kuroiwa, A.; Yoshinari, N.; Kameyama, A. Changes in Gloss Alteration, Surface Roughness, and Color of Direct Dental Restorative Materials after Professional Dental Prophylaxis. J. Funct. Biomater. 2024, 15, 8. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb15010008
Miyashita-Kobayashi A, Haruyama A, Nakamura K, Wu C-Y, Kuroiwa A, Yoshinari N, Kameyama A. Changes in Gloss Alteration, Surface Roughness, and Color of Direct Dental Restorative Materials after Professional Dental Prophylaxis. Journal of Functional Biomaterials. 2024; 15(1):8. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb15010008
Chicago/Turabian StyleMiyashita-Kobayashi, Aya, Akiko Haruyama, Keigo Nakamura, Chia-Ying Wu, Akihiro Kuroiwa, Nobuo Yoshinari, and Atsushi Kameyama. 2024. "Changes in Gloss Alteration, Surface Roughness, and Color of Direct Dental Restorative Materials after Professional Dental Prophylaxis" Journal of Functional Biomaterials 15, no. 1: 8. https://0-doi-org.brum.beds.ac.uk/10.3390/jfb15010008