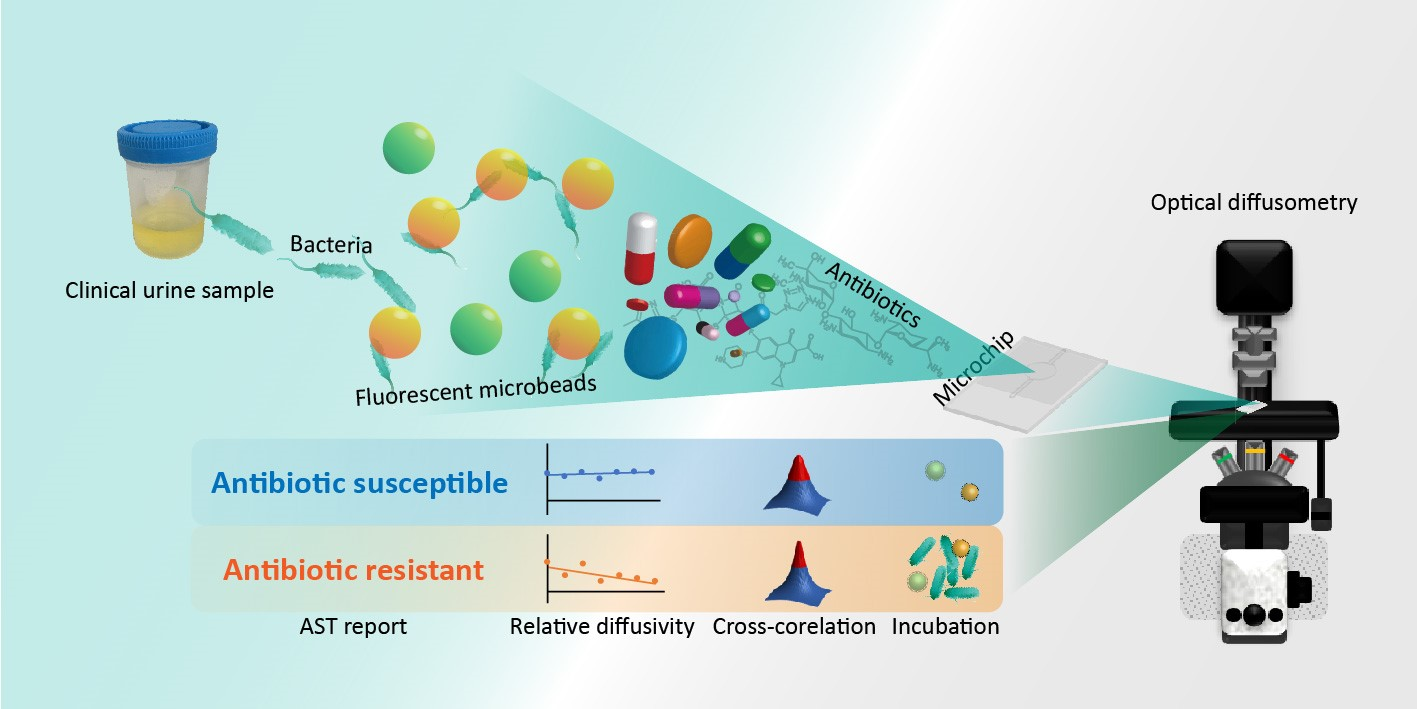
Developing Rapid Antimicrobial Susceptibility Testing for Motile/Non-Motile Bacteria Treated with Antibiotics Covering Five Bactericidal Mechanisms on the Basis of Bead-Based Optical Diffusometry


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Experimental Setup and Microchip Fabrication
2.3. Functionalization of Probe Microbeads
2.4. Preparations of Bacteria and Antibiotics
2.5. Preparation of Clinical Samples
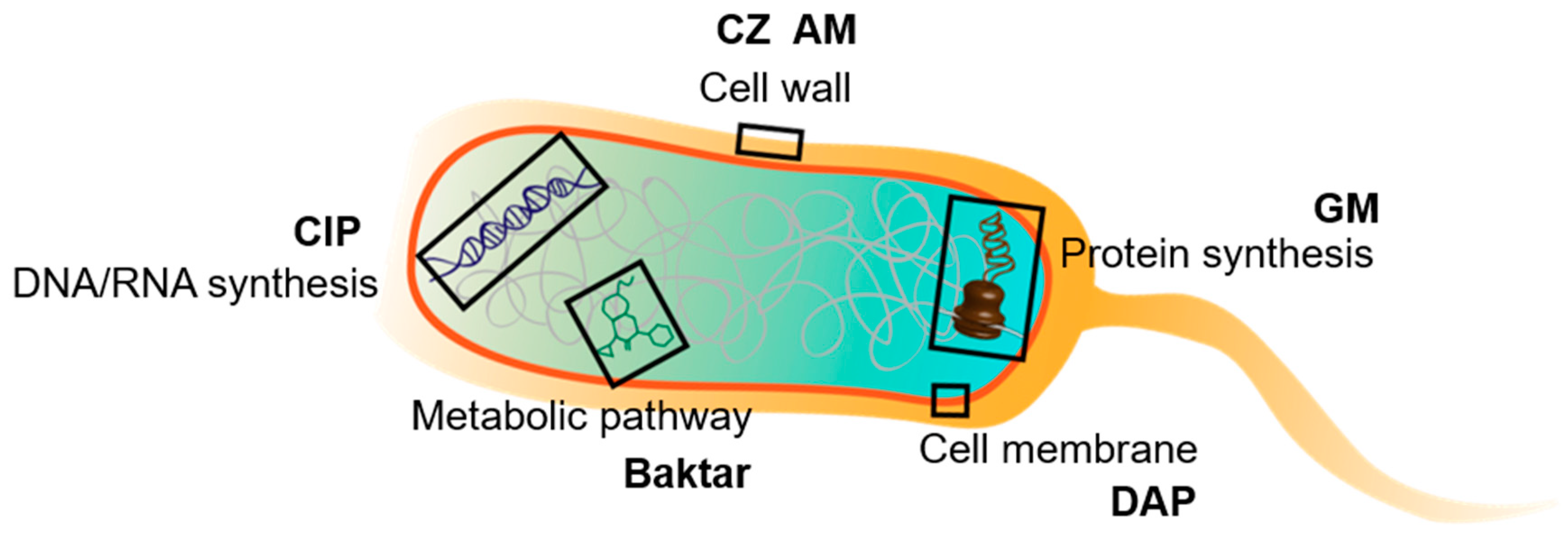
2.6. Mechanisms of Bacterial Inhibition from Antibiotics
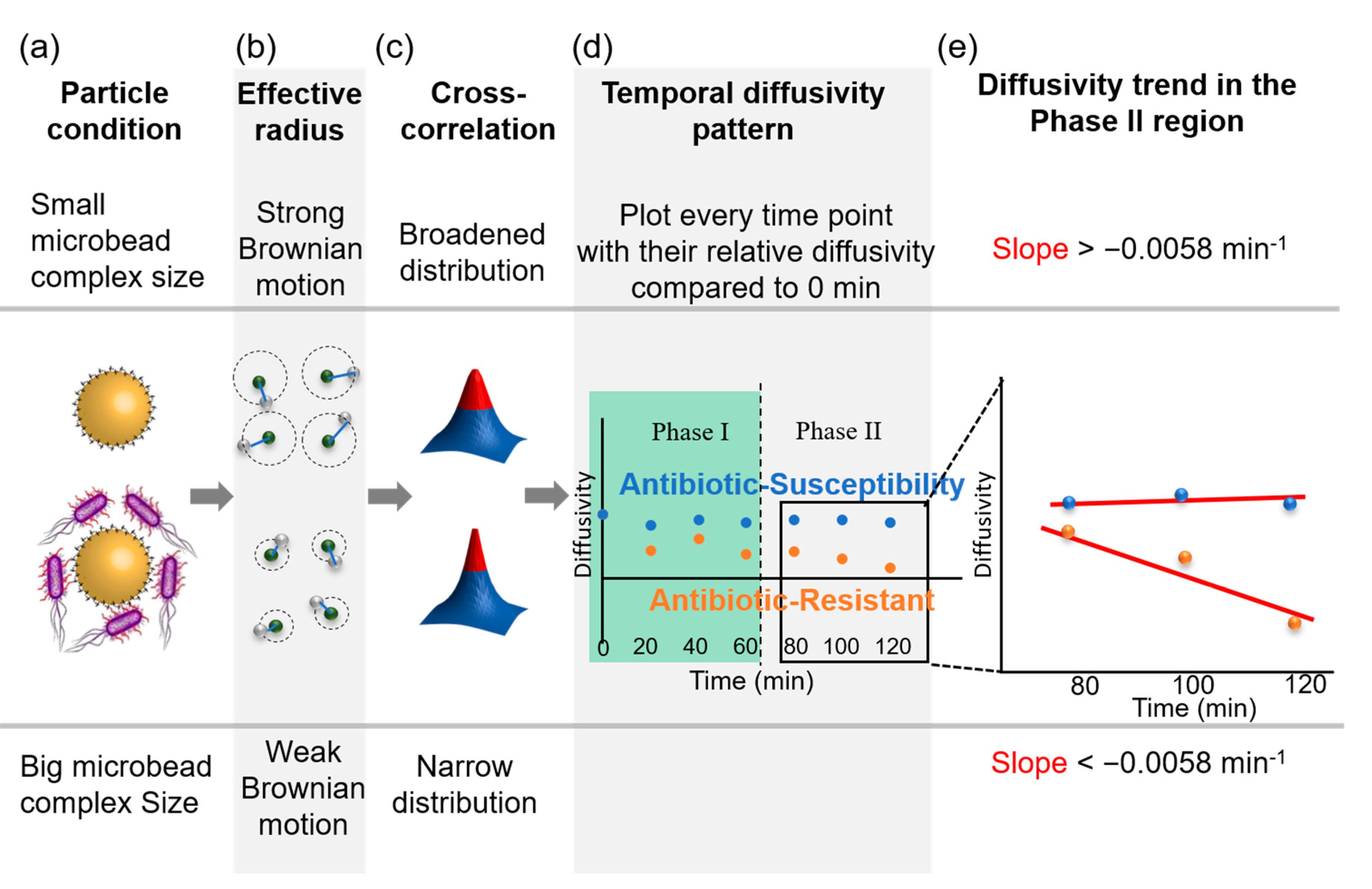
2.7. Determination of the Optimal Threshold for Rapid AST
3. Results and Discussion
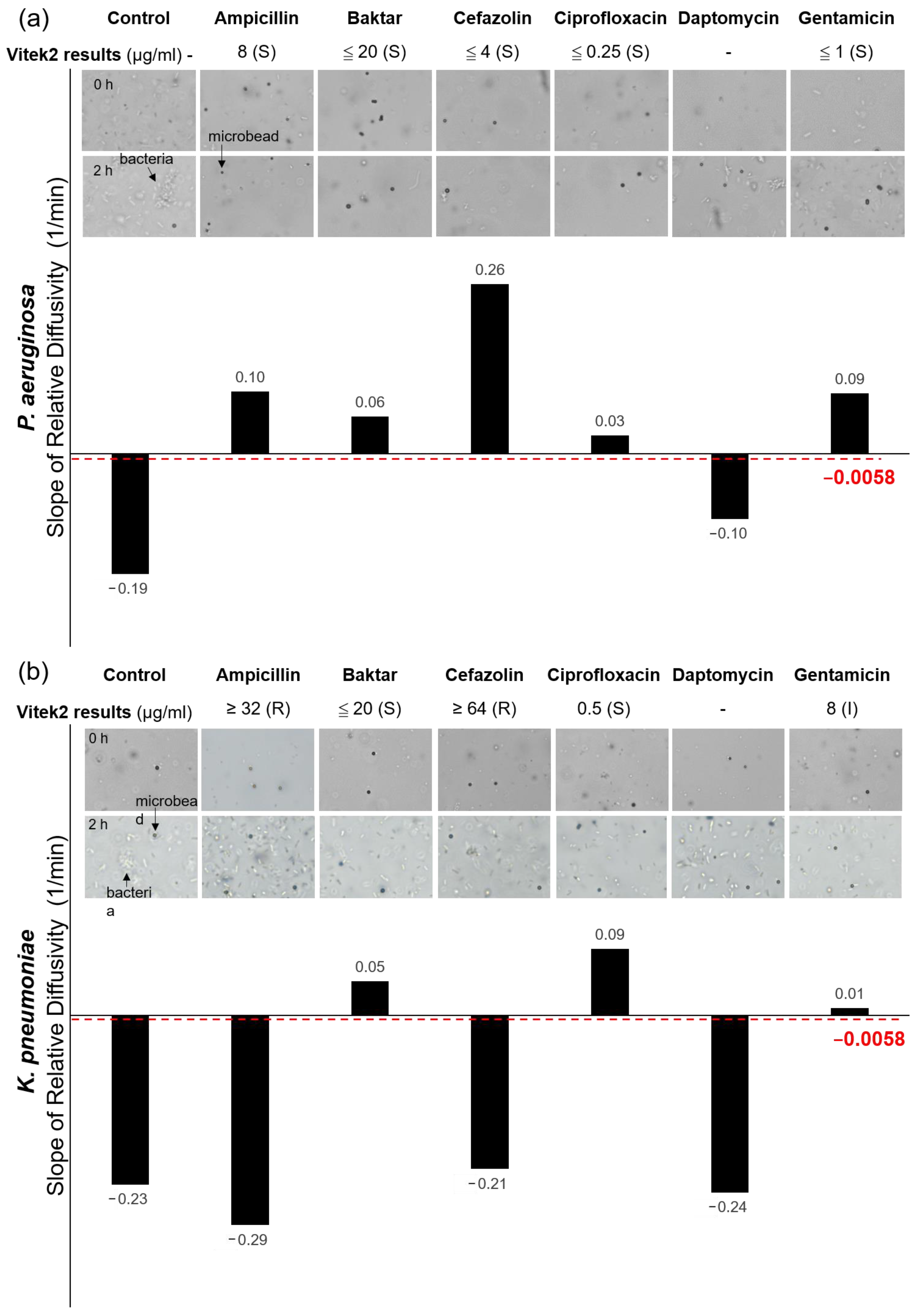
3.1. Empirical AST Threshold Derived from Clinical Samples
3.2. Diffusivity Changes in Response to Interactions between Bacteria and Antibiotics
3.3. Validations of the Optical Diffusometry
3.4. Evaluations of the Clinical Samples
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Thornsberry, C.; Mcdougal, L.K. Successful use of broth microdilution in susceptibility tests for methicillin-resistant (heteroresistant) staphylococci. J. Clin. Microbiol. 1983, 18, 1084–1091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drew, W.L.; Barry, A.; O’Toole, R.; Sherris, J.C. Reliability of the Kirby-Bauer disc diffusion method for detecting methicillin-resistant strains of Staphylococcus aureus. Appl. Environ. Microbiol 1972, 24, 240–247. [Google Scholar] [CrossRef] [Green Version]
- Chung, C.-Y.; Wang, J.-C.; Chuang, H.-S. Simultaneous and quantitative monitoring of co-cultured Pseudomonas aeruginosa and Staphylococcus aureus with antibiotics on a diffusometric platform. Sci. Rep. 2017, 7, 46336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.-K.; Cheng, H.-W.; Liao, C.-C.; Lin, S.-J.; Chen, Y.-Z.; Wang, J.-K.; Wang, Y.-L.; Huang, N.-T. Bacteria encapsulation and rapid antibiotic susceptibility test using a microfluidic microwell device integrating surface-enhanced Raman scattering. Lab Chip 2020, 20, 2520–2528. [Google Scholar] [CrossRef]
- Leekha, S.; Terrell, C.L.; Edson, R.S. General principles of antimicrobial therapy. Mayo Clin. Proc. 2011, 86, 156–167. [Google Scholar] [CrossRef] [Green Version]
- Kinnunen, P.; Sinn, I.; McNaughton, B.H.; Newton, D.W.; Burns, M.A.; Kopelman, R. Monitoring the growth and drug susceptibility of individual bacteria using asynchronous magnetic bead rotation sensors. Biosens. Bioelectron. 2011, 26, 2751–2755. [Google Scholar] [CrossRef] [Green Version]
- Sinn, I.; Kinnunen, P.; Albertson, T.; McNaughton, B.H.; Newton, D.W.; Burns, M.A.; Kopelman, R. Asynchronous magnetic bead rotation (AMBR) biosensor in microfluidic droplets for rapid bacterial growth and susceptibility measurements. Lab Chip 2011, 11, 2604–2611. [Google Scholar] [CrossRef]
- Chung, C.-C.; Cheng, I.-F.; Chen, H.-M.; Kan, H.-C.; Yang, W.-H.; Chang, H.-C. Screening of antibiotic susceptibility to β-Lactam-Induced Elongation of gram-negative bacteria based on dielectrophoresis. Anal. Chem. 2012, 84, 3347–3354. [Google Scholar] [CrossRef]
- Mohan, R.; Sanpitakseree, C.; Desai, A.V.; Sevgen, S.E.; Schroeder, C.M.; Kenis, P.J. A microfluidic approach to study the effect of bacterial interactions on antimicrobial susceptibility in polymicrobial cultures. RSC Adv. 2015, 5, 35211–35223. [Google Scholar] [CrossRef]
- Cheng, I.-F.; Chang, H.-C.; Chen, T.-Y.; Hu, C.; Yang, F.-L. Rapid (<5 min) identification of pathogen in human blood by electrokinetic concentration and surface-enhanced Raman spectroscopy. Sci. Rep. 2013, 3, 2365. [Google Scholar]
- Xiong, Q.; Lim, C.Y.; Ren, J.; Zhou, J.; Pu, K.; Chan-Park, M.B.; Mao, H.; Lam, Y.C.; Duan, H. Magnetic nanochain integrated microfluidic biochips. Nat. Commun. 2018, 9, 1743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltekin, Ö.; Boucharin, A.; Tano, E.; Andersson, D.I.; Elf, J. Antibiotic susceptibility testing in less than 30 min using direct single-cell imaging. Proc. Natl. Acad. Sci. USA 2017, 114, 9170–9175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syal, K.; Iriya, R.; Yang, Y.; Yu, H.; Wang, S.; Haydel, S.E.; Chen, H.-Y.; Tao, N. Antimicrobial susceptibility test with plasmonic imaging and tracking of single bacterial motions on nanometer scale. ACS Nano 2016, 10, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Chung, C.-Y.; Wang, J.-C.; Chuang, H.-S. Rapid bead-based antimicrobial susceptibility testing by optical diffusometry. PLoS ONE 2016, 11. [Google Scholar] [CrossRef]
- Clayton, K.N.; Moehling, T.J.; Lee, D.H.; Wereley, S.T.; Linnes, J.C.; Kinzer-Ursem, T.L. Particle Diffusometry: An Optical Detection Method for Vibrio cholerae Presence in Environmental Water Samples. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Clayton, K.N.; Lee, D.; Wereley, S.T.; Kinzer-Ursem, T.L. Measuring biotherapeutic viscosity and degradation on-chip with particle diffusometry. Lab Chip 2017, 17, 4148–4159. [Google Scholar] [CrossRef]
- Kholodenko, A.L.; Douglas, J.F. Generalized Stokes-Einstein equation for spherical particle suspensions. Phys. Rev. E 1995, 51, 1081. [Google Scholar] [CrossRef]
- Chen, C.-J.; Chen, W.-L.; Phong, P.H.; Chuang, H.-S. Investigation of Micro-volume Viscosity with Janus Microbeads Based on Rotational Brownian Motion. Sensors 2019, 19, 1217. [Google Scholar] [CrossRef] [Green Version]
- Cheng, H.-P.; Chuang, H.-S. Rapid and Sensitive Nano-Immunosensors for Botulinum. ACS Sens. 2019, 4, 1754–1760. [Google Scholar] [CrossRef]
- Chuang, H.-S.; Chen, Y.-J.; Cheng, H.-P. Enhanced diffusometric immunosensing with grafted gold nanoparticles for detection of diabetic retinopathy biomarker tumor necrosis factor-α. Biosens. Bioelectron. 2018, 101, 75–83. [Google Scholar] [CrossRef]
- Wang, J.-C.; Tung, Y.-C.; Ichiki, K.; Sakamoto, H.; Yang, T.-H.; Suye, S.-I.; Chuang, H.-S. Culture-free detection of methicillin-resistant Staphylococcus aureus by using self-driving diffusometric DNA nanosensors. Biosens. Bioelectron. 2020, 148, 111817. [Google Scholar] [CrossRef] [PubMed]
- Clayton, K.N.; Berglund, G.D.; Linnes, J.C.; Kinzer-Ursem, T.L.; Wereley, S.T. DNA microviscosity characterization with particle diffusometry for downstream DNA detection applications. Anal. Chem. 2017, 89, 13334–13341. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-C.; Chi, S.-W.; Shieh, D.-B.; Chuang, H.-S. Development of a self-driving bioassay based on diffusion for simple detection of microorganisms. Sens. Actuat. B. Chem. 2019, 278, 140–146. [Google Scholar] [CrossRef]
- Wang, J.C.; Chi, S.W.; Yang, T.H.; Chuang, H.S. Label-Free Monitoring of Microorganisms and Their Responses to Antibiotics Based on Self-Powered Microbead Sensors. ACS Sens. 2018, 3, 2182–2190. [Google Scholar] [CrossRef] [PubMed]
- Kell, A.J.; Stewart, G.; Ryan, S.; Peytavi, R.; Boissinot, M.; Huletsky, A.; Bergeron, M.G.; Simard, B. Vancomycin-Modified Nanoparticles for Efficient Targeting and Preconcentration of Gram-Positive and Gram-Negative Bacteria. ACS Nano 2008, 2, 1777–1788. [Google Scholar] [CrossRef]
- Lin, Y.-S.; Tsai, P.-J.; Weng, M.-F.; Chen, Y.-C. Affinity Capture Using Vancomycin-Bound Magnetic Nanoparticles for the MALDI-MS Analysis of Bacteria. Anal. Chem. 2005, 77, 1753–1760. [Google Scholar] [CrossRef]
- Hong, H.-J.; Hutchings, M.I.; Buttner, M.J. Vancomycin resistance VanS/VanR two-component systems. In Bacterial Signal Transduction: Networks and Drug Targets; Springer: New York, NY, USA, 2008; pp. 200–213. [Google Scholar]
- Johnston, B.; Conly, J. Tumour necrosis factor inhibitors and infection: What is there to know for infectious diseases physicians? Can. J. Infect. Dis. Med. Microbiol. 2006, 17, 209–212. [Google Scholar] [CrossRef] [Green Version]
- Baltch, A.L.; Smith, R.P. Pseudomonas Aeruginosa: Infections and Treatment; Marcel Dekker, Inc.: New York, NY, USA, 1994. [Google Scholar]
- Kluytmans, J.; Van Belkum, A.; Verbrugh, H. Nasal carriage of Staphylococcus aureus: Epidemiology, underlying mechanisms, and associated risks. Clin. Microbiol. Rev. 1997, 10, 505–520. [Google Scholar] [CrossRef]
- Bergeron, C.R.; Prussing, C.; Boerlin, P.; Daignault, D.; Dutil, L.; Reid-Smith, R.J.; Zhanel, G.G.; Manges, A.R. Chicken as reservoir for extraintestinal pathogenic Escherichia coli in humans, Canada. Emerg. Infect. Dis. 2012, 18, 415–421. [Google Scholar] [CrossRef]
- Djordjevic, Z.; Folic, M.M.; Zivic, Z.; Markovic, V.; Jankovic, S.M. Nosocomial urinary tract infections caused by Pseudomonas aeruginosa and Acinetobacter species: Sensitivity to antibiotics and risk factors. Am. J. Infect. Control. 2013, 41, 1182–1187. [Google Scholar] [CrossRef]
- Von Daehne, W.; Frederiksen, E.; Gundersen, E.; Lund, F.; Moerch, P.; Petersen, H.J.; Roholt, K.; Tybring, L.; Godtfredsen, W.O. Acyloxymethyl esters of ampicillin. J. Med. Chem. 1970, 13, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Neu, H.C. Penicillin-binding proteins and role of amdinocillin in causing bacterial cell death. Am. J. Med. 1983, 75, 9–20. [Google Scholar] [CrossRef]
- Rodgers, F.; Tzianabos, A.; Elliott, T. The effect of antibiotics that inhibit cell-wall, protein, and DNA synthesis on the growth and morphology of Legionella pneumophila. J. Med. Microbiol. 1990, 31, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.J. Tarascon Pocket Pharmacopoeia; Jones & Bartlett Publishers: Burlington, VT, USA, 2012. [Google Scholar]
- Wormser, G.P.; Keusch, G.T.; Heel, R.C. Co-trimoxazole (trimethoprim-sulfamethoxazole). Drugs 1982, 24, 459–518. [Google Scholar] [CrossRef] [PubMed]
- Minkowski, P.; Staege, H.; Groscurth, P.; Schaffner, A. Effects of trimethoprim and co-trimoxazole on the morphology of Listeria monocytogenes in culture medium and after phagocytosis. J. Antimicrob. Chemother. 2001, 48, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Campoli-Richards, D.M.; Monk, J.P.; Price, A.; Benfield, P.; Todd, P.A.; Ward, A. Ciprofloxacin. Drugs 1988, 35, 373–447. [Google Scholar] [CrossRef]
- Pommier, Y.; Leo, E.; Zhang, H.; Marchand, C. DNA topoisomerases and their poisoning by anticancer and antibacterial drugs. Chem. Biol. 2010, 17, 421–433. [Google Scholar] [CrossRef] [Green Version]
- Diver, J.; Wise, R. Morphological and biochemical changes in Escherichia coli after exposure to ciprofloxacin. J. Antimicrob. Chemother. 1986, 18, 31–41. [Google Scholar] [CrossRef]
- Tally, F.P.; DeBruin, M.F. Development of daptomycin for gram-positive infections. J. Antimicrob. Chemother. 2000, 46, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Pogliano, J.; Pogliano, N.; Silverman, J.A. Daptomycin-mediated reorganization of membrane architecture causes mislocalization of essential cell division proteins. J. Bacteriol. 2012, 194, 4494–4504. [Google Scholar] [CrossRef]
- Condrad, R.S. The effects of daptomycin on chemical composition and morphology of Staphylococcus aureus. Proc. Okla. Acad. Sci. 1998, 78, 15–22. [Google Scholar]
- Dao, E.H.; Poitevin, F.; Sierra, R.G.; Gati, C.; Rao, Y.; Ciftci, H.I.; Akşit, F.; McGurk, A.; Obrinski, T.; Mgbam, P. Structure of the 30S ribosomal decoding complex at ambient temperature. RNA 2018, 24, 1667–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacqueline, C.; Caillon, J.; Le Mabecque, V.; Miègeville, A.-F.; Donnio, P.-Y.; Bugnon, D.; Potel, G. In vitro activity of linezolid alone and in combination with gentamicin, vancomycin or rifampicin against methicillin-resistant Staphylococcus aureus by time–kill curve methods. J. Antimicrob. Chemother. 2003, 51, 857–864. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibson, B.; Wilson, D.J.; Feil, E.; Eyre-Walker, A. The distribution of bacterial doubling times in the wild. Proc. R. Soc. B Biol. Sci. 2018, 285, 20180789. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Dong, G.; Zhang, S.; Zhang, X.; Zhao, Y.; Cao, J.; Zhou, T.; Wu, Q. Effects of iron on the growth, biofilm formation and virulence of Klebsiella pneumoniae causing liver abscess. BMC Microbiol. 2020, 20, 36. [Google Scholar] [CrossRef] [Green Version]
- Rodloff, A.; Bauer, T.; Ewig, S.; Kujath, P.; Muller, E. Susceptible, intermediate, and resistant—The intensity of antibiotic action. Dtsch. Arztebl. Int. 2008, 105, 657–662. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| # | Control | Ampicillin | Baktar | Cefazolin | Ciprofloxacin | Daptomycin | Gentamicin | |
|---|---|---|---|---|---|---|---|---|
| 1 | H | <(GNB)* | -*** | - | - | - | - | - |
| V | No colony | - | - | - | - | - | - | |
| O | No bacteria | - | - | - | - | - | - | |
| 2 | H | <(GNB) | - | - | - | - | - | - |
| V | No colony | - | - | - | - | - | - | |
| O | No bacteria | - | - | - | - | - | - | |
| 3 | H | Klebsiella pneumoniae | R | S | R | S | - | S |
| V | Klebsiella pneumoniae | I | S | S | S | - | S | |
| O | √** | R | R | S | R | S | R | |
| 4 | H | 0 colony | - | - | - | - | - | - |
| V | No colony | - | - | - | - | - | - | |
| O | No bacteria | - | - | - | - | - | - | |
| 5 | H | Escherichia coli | S | S | S | S | - | S |
| V | Escherichia coli | S | S | S | S | - | S | |
| O | √ | S | S | S | S | S | ||
| 6 | H | <(GNB) | - | - | - | - | - | - |
| V | Low Discrimination (Escherichia coli) | R | R | R | R | - | S | |
| O | √ | R | R | R | R | R | S | |
| 7 | H | Escherichia coli | R | S | I | S | - | S |
| V | Escherichia coli | R | S | S | S | - | S | |
| O | √ | R | S | S | S | R | S |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.-T.; Wang, J.-C.; Chuang, H.-S. Developing Rapid Antimicrobial Susceptibility Testing for Motile/Non-Motile Bacteria Treated with Antibiotics Covering Five Bactericidal Mechanisms on the Basis of Bead-Based Optical Diffusometry. Biosensors 2020, 10, 181. https://0-doi-org.brum.beds.ac.uk/10.3390/bios10110181
Yang Y-T, Wang J-C, Chuang H-S. Developing Rapid Antimicrobial Susceptibility Testing for Motile/Non-Motile Bacteria Treated with Antibiotics Covering Five Bactericidal Mechanisms on the Basis of Bead-Based Optical Diffusometry. Biosensors. 2020; 10(11):181. https://0-doi-org.brum.beds.ac.uk/10.3390/bios10110181
Chicago/Turabian StyleYang, Yao-Tzu, Jhih-Cheng Wang, and Han-Sheng Chuang. 2020. "Developing Rapid Antimicrobial Susceptibility Testing for Motile/Non-Motile Bacteria Treated with Antibiotics Covering Five Bactericidal Mechanisms on the Basis of Bead-Based Optical Diffusometry" Biosensors 10, no. 11: 181. https://0-doi-org.brum.beds.ac.uk/10.3390/bios10110181