Machine Learning-Guided Prediction of Central Anterior Chamber Depth Using Slit Lamp Images from a Portable Smartphone Device

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Recruitment and Image Capture
- Willing and able to participate in study
- Be at least 60 years old (inclusive)
- Had not had prior intraocular surgery or laser procedures to the eye
- Be fit enough for keep eyes open for adequate image acquisition
- Not have concurrent eye pathologies that may obscure photo-taking of the eye
- Not have previous laser or surgical glaucoma interventions
2.2. Image Capture Protocol
- Set-up A: Smartphone (Samsung® Galaxy S7, Seoul, South Korea) with a MIDAS portable slit lamp mount prototype.
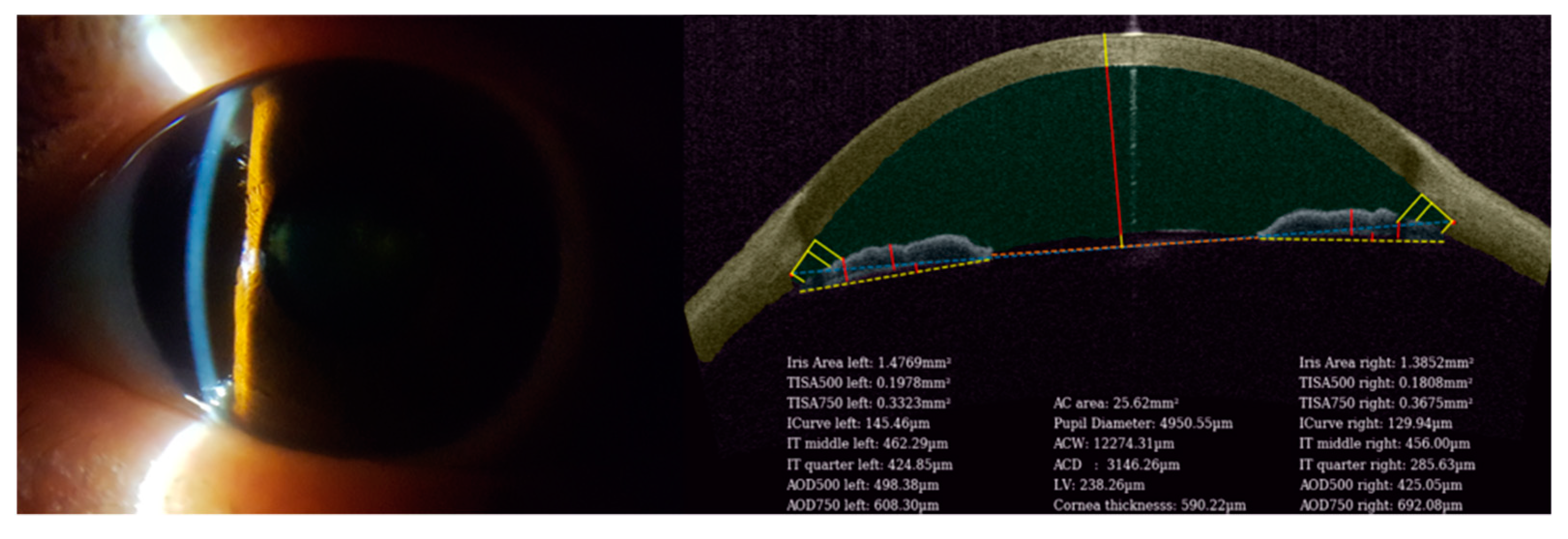
- Set-up B: Corneal anterior segment non-invasive three-dimensional swept source imaging system (Tomey® SS-1000 CASIA ASOCT, Nagoya, Japan).
2.3. Image Feature Extraction and Application of Machine Learning Techniques
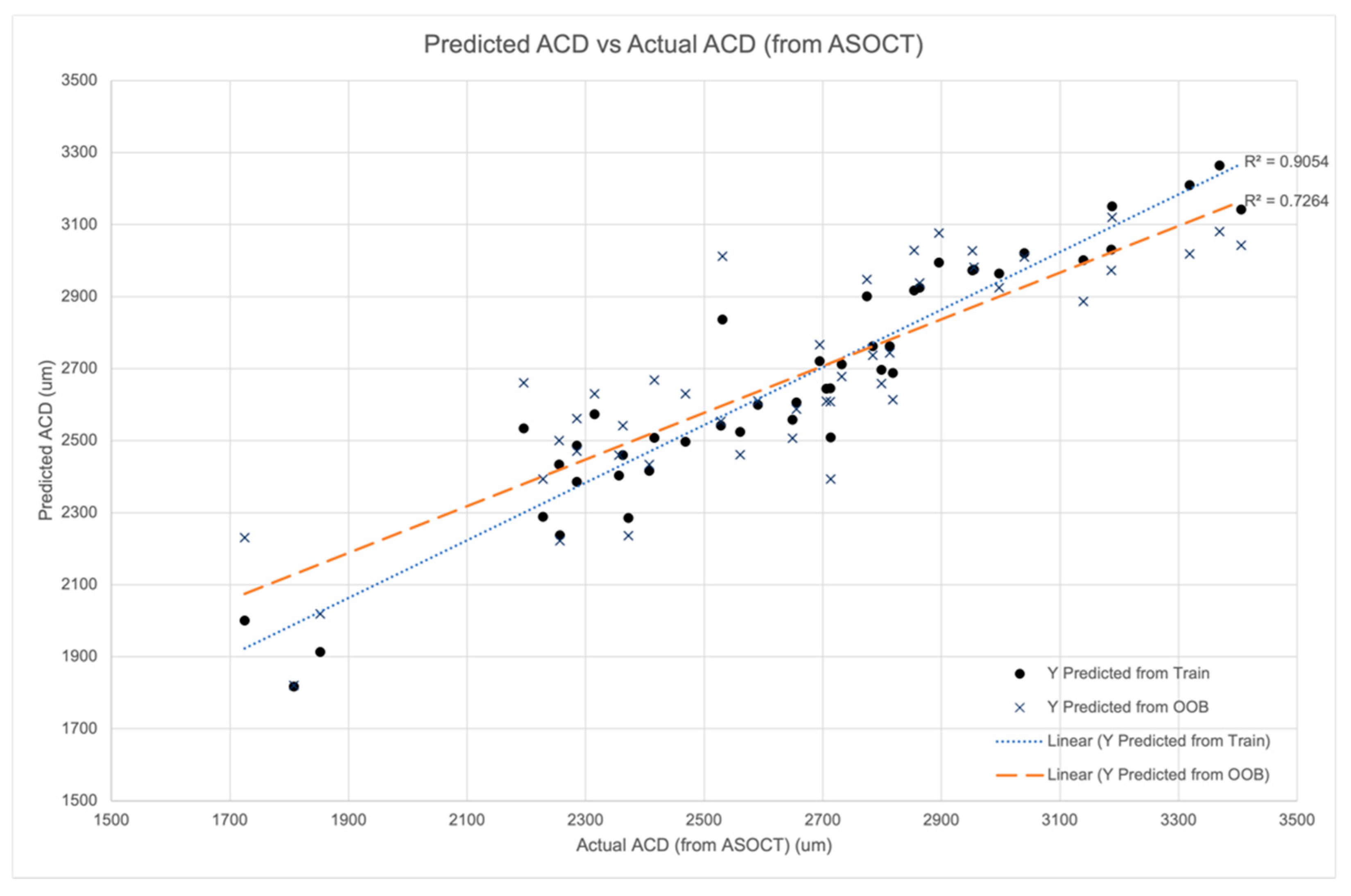
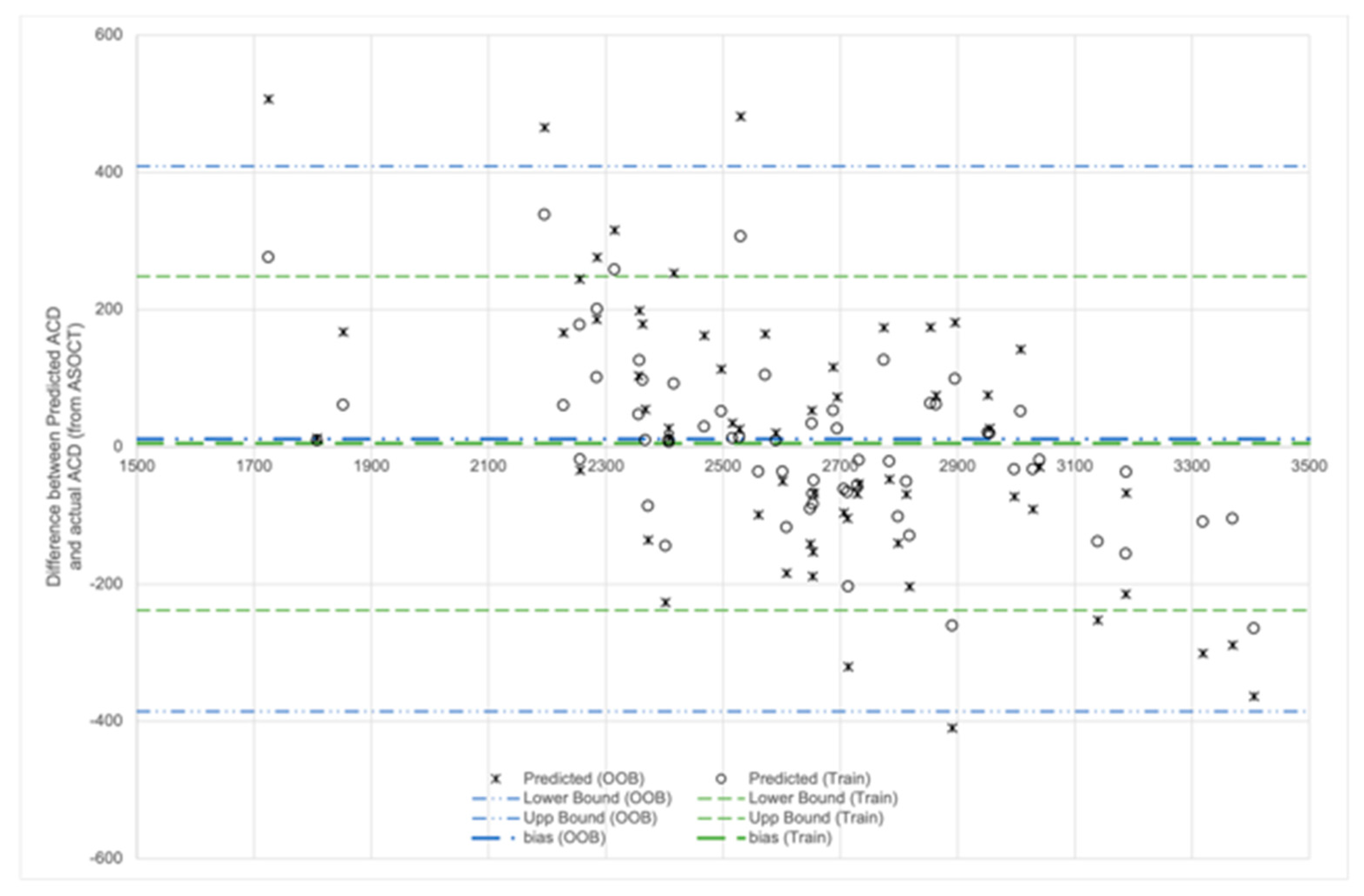
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yip, J.L.Y.; Foster, P.J. Ethnic differences in primary angle-closure glaucoma. Curr. Opin. Ophthalmol. 2006, 17, 175–180. [Google Scholar] [CrossRef]
- Foster, P.J. Glaucoma in China: How big is the problem? Br. J. Ophthalmol. 2001, 85, 1277–1282. [Google Scholar] [CrossRef] [Green Version]
- Foster, P.J.; Oen, F.T.S.; Machin, D.; Ng, T.-P.; Devereux, J.G.; Johnson, G.J.; Khaw, P.T.; Seah, S.K.L. The Prevalence of Glaucoma in Chinese Residents of Singapore: A Cross-Sectional Population Survey of the Tanjong Pagar District. Arch. Ophthalmol. 2000, 118, 1105–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seah, S.K.L.; Foster, P.J.; Chew, P.T.K.; Jap, A.; Oen, F.; Fam, H.B.; Lim, A.S.M. Incidence of Acute Primary Angle-closure Glaucoma in Singapore. Arch. Ophthalmol. 1997, 115, 1436–1440. [Google Scholar] [CrossRef]
- Wong, T.Y.; Foster, P.J.; Seah, S.K.L.; Chew, P.T.K. Rates of hospital admissions for primary angle closure glaucoma among Chinese, Malays, and Indians in Singapore. Br. J. Ophthalmol. 2000, 84, 990–992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Congdon, N.G.; Quigley, H.A.; Hung, P.T.; Wang, T.H.; Ho, T. Screening techniques for angle-closure glaucoma in rural Taiwan. Acta Ophthalmol. Scand. 2009, 74, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Foster, P.J.; Baasanhu, J.; Alsbirk, P.H.; Munkhbayar, D.; Uranchimeg, D.; Johnson, G.J. Glaucoma in Mongolia. Arch. Ophthalmol. 1996, 114, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.-C.; Chew, P.T. What is the direct cost of treatment of acute primary angle closure glaucoma? The Singapore model. Clin. Exp. Ophthalmol. 2004, 32, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Ang, M.; Baskaran, M.; Werkmeister, R.M.; Chua, J.; Schmidl, D.; dos Santos, V.A.; Garhöfer, G.; Mehta, J.S.; Schmetterer, L. Anterior segment optical coherence tomography. Prog. Retin. Eye Res. 2018, 66, 132–156. [Google Scholar] [CrossRef]
- Narayanaswamy, A.; Sakata, L.M.; He, M.-G.; Friedman, D.S.; Chan, Y.-H.; Lavanya, R.; Baskaran, M.; Foster, P.J.; Aung, T. Diagnostic Performance of Anterior Chamber Angle Measurements for Detecting Eyes with Narrow Angles. Arch. Ophthalmol. 2010, 128, 1321. [Google Scholar] [CrossRef]
- Ting, D.S.; Peng, L.; Varadarajan, A.V.; Keane, P.A.; Burlina, P.M.; Chiang, M.F.; Schmetterer, L.; Pasquale, L.R.; Bressler, N.M.; Webster, D.R.; et al. Deep learning in ophthalmology: The technical and clinical considerations. Prog. Retin. Eye Res. 2019, 72, 100759. [Google Scholar] [CrossRef]
- Grzybowski, A.; Brona, P.; Lim, G.; Ruamviboonsuk, P.; Tan, G.S.W.; Abramoff, M.; Ting, D.S.W. Artificial intelligence for diabetic retinopathy screening: A review. Eye 2020, 34, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Gargeya, R.; Leng, T. Automated Identification of Diabetic Retinopathy Using Deep Learning. Ophthalmology 2017, 124, 962–969. [Google Scholar] [CrossRef] [PubMed]
- Burlina, P.M.; Joshi, N.; Pekala, M.; Pacheco, K.D.; Freund, D.E.; Bressler, N.M. Automated Grading of Age-Related Macular Degeneration From Color Fundus Images Using Deep Convolutional Neural Networks. JAMA Ophthalmol. 2017, 135, 1170–1176. [Google Scholar] [CrossRef]
- Grassmann, F.; Mengelkamp, J.; Brandl, C.; Harsch, S.; Zimmermann, M.E.; Linkohr, B.; Peters, A.; Heid, I.M.; Palm, C.; Weber, B.H. A Deep Learning Algorithm for Prediction of Age-Related Eye Disease Study Severity Scale for Age-Related Macular Degeneration from Color Fundus Photography. Ophthalmology 2018, 125, 1410–1420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, C.; Johnson, T.V.; Garg, A.; Boland, M. Artificial intelligence in glaucoma. Curr. Opin. Ophthalmol. 2019, 30, 97–103. [Google Scholar] [CrossRef]
- Xu, B.Y.; Chiang, M.; Chaudhary, S.; Kulkarni, S.; Pardeshi, A.A.; Varma, R. Deep Learning Classifiers for Automated Detection of Gonioscopic Angle Closure Based on Anterior Segment OCT Images. Am. J. Ophthalmol. 2019, 208, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Fu, H.; Xu, Y.; Lin, S.; Wong, D.W.K.; Baskaran, M.; Mahesh, M.; Aung, T.; Liu, J. Angle-Closure Detection in Anterior Segment OCT Based on Multilevel Deep Network. IEEE Trans. Cybern. 2019, 50, 3358–3366. [Google Scholar] [CrossRef] [Green Version]
- Fu, H.; Xu, Y.; Lin, S.; Zhang, X.; Wong, D.W.K.; Liu, J.; Frangi, A.F.; Baskaran, M.; Aung, T. Segmentation and Quantification for Angle-Closure Glaucoma Assessment in Anterior Segment OCT. IEEE Trans. Med. Imaging 2017, 36, 1930–1938. [Google Scholar] [CrossRef] [Green Version]
- Van Herick, W.; Shaffer, R.N.; Schwartz, A. Estimation of Width of Angle of Anterior Chamber. Am. J. Ophthalmol. 1969, 68, 626–629. [Google Scholar] [CrossRef]
- Blieden, L.S.; Chuang, A.Z.; Baker, L.A.; Bell, N.P.; Fuller, T.S.; Mankiewicz, K.A.; Feldman, R.M. Optimal Number of Angle Images for Calculating Anterior Angle Volume and Iris Volume Measurements. Investig. Ophthalmol. Vis. Sci. 2015, 56, 2842–2847. [Google Scholar] [CrossRef] [Green Version]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Manwar, R.; Li, X.; Mahmoodkalayeh, S.; Asano, E.; Zhu, D.; Avanaki, K. Deep learning protocol for improved photoacoustic brain imaging. J. Biophotonics 2020, 13, e202000212. [Google Scholar] [CrossRef]
- Qiu, B.; Huang, Z.; Liu, X.; Meng, X.; You, Y.; Liu, G.; Yang, K.; Maier, A.; Ren, Q.; Lu, Y. Noise reduction in optical coherence tomography images using a deep neural network with perceptually-sensitive loss function. Biomed. Opt. Express 2020, 11, 817–830. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.; Redmond, T.; Agarwal, R.; Marshall, L.R.; Evans, B.J.W. Repeatability and comparison of clinical techniques for anterior chamber angle assessment. Ophthalmic Physiol. Opt. 2015, 35, 170–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.B.; Sung, K.R.; Kang, S.Y.; Jo, J.W.; Lee, K.S.; Kook, M.S. Assessment of narrow angles by gonioscopy, Van Herick method and anterior segment optical coherence tomography. Jpn. J. Ophthalmol. 2011, 55, 343–350. [Google Scholar] [CrossRef]
- Choudhari, N.S.; Chanda, S.; Khanna, R.; Senthil, S.; Garudadri, C.S. Diagnostic Accuracy of Van Herick Technique to Detect Pre-Disease States of Primary Angle Closure Glaucoma in a Resource Constraint Region. Ophthalmic Epidemiol. 2019, 26, 175–182. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, S.Z.; Li, L.; Thomas, R.; Wang, N.L. The Handan Eye Study: Comparison of Screening Methods for Primary Angle Closure Suspects in a Rural Chinese Population. Ophthalmic Epidemiol. 2014, 21, 268–275. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training Set | Out-of-Bag Samples | |
|---|---|---|
| Coefficient of Correlation, R2 | 0.91 | 0.73 |
| Bias | 542.85 | 955.18 |
| RMSE | 122.33 | 200.03 |
| Dimensions | Feature Importance (Normalized) |
|---|---|
| A | 0.15 |
| B | 0.13 |
| C | 0.18 |
| D | 0.16 |
| E | 0.16 |
| F | 0.10 |
| G | 0.11 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, D.; Ho, Y.; Sasa, Y.; Lee, J.; Yen, C.C.; Tan, C. Machine Learning-Guided Prediction of Central Anterior Chamber Depth Using Slit Lamp Images from a Portable Smartphone Device. Biosensors 2021, 11, 182. https://0-doi-org.brum.beds.ac.uk/10.3390/bios11060182
Chen D, Ho Y, Sasa Y, Lee J, Yen CC, Tan C. Machine Learning-Guided Prediction of Central Anterior Chamber Depth Using Slit Lamp Images from a Portable Smartphone Device. Biosensors. 2021; 11(6):182. https://0-doi-org.brum.beds.ac.uk/10.3390/bios11060182
Chicago/Turabian StyleChen, David, Yvonne Ho, Yuki Sasa, Jieying Lee, Ching Chiuan Yen, and Clement Tan. 2021. "Machine Learning-Guided Prediction of Central Anterior Chamber Depth Using Slit Lamp Images from a Portable Smartphone Device" Biosensors 11, no. 6: 182. https://0-doi-org.brum.beds.ac.uk/10.3390/bios11060182