
Challenges in Steroid and Anticoagulant Therapy in Severe COVID-19 Pneumonia: A Prospective Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Diagnostic Criteria for Severe COVID-19 Pneumonia
2.3. Patients Were Submitted for
2.3.1. History, Clinical, and Radiological Assessment
2.3.2. Laboratory Tests
2.3.3. Management Policy for Severe COVID-19 Pneumonia Patients and Prospective Design
- Group A: Patients with severe COVID-19 pneumonia, treated with dexamethasone and anticoagulants according to the D-dimer levels.
- Group B: Patients with severe COVID-19 pneumonia, treated with prednisolone or methylprednisolone and anticoagulants according to D-dimer levels.
- Group C: Patients with severe COVID-19 pneumonia, treated with prednisolone or methylprednisolone and anticoagulants according to the flexible protocol.
Treatment Policies
- Corticosteroids:
- −
- Dexamethasone: a dosage of 6 mg was administered in a once-daily oral (liquid or tablet) or intravenous (IV) preparation, to be used for up to 10 days, until discharged, or until the patient became asymptomatic.
- −
- Prednisolone or equivalent methylprednisolone: prednisolone, at dosage of 60 mg, was administered to patients on non-rebreathing masks equal to or less than 10 L, intravenously or orally, divided into three equal doses per day For patients on non-rebreathing masks equal to or greater than 10 L or mechanical ventilation, the dose was 120 mg infusion over 24 h. After clinical and radiological improvement and the reduction of FiO2, the dose was titrated down by 25%, and then by 50%, according to clinical response and oxygen requirement. The dose was decreased to 40 mg orally when O2 requirements fell to 6 L or less. When patients were ready for discharge and O2 saturation was more than 93% on room air, the dose was 30 mg OD in the morning, gradually decreased by 5 mg every 7 days. Some patients in the first group were discharged on oxygen therapy.
- Anticoagulation:
- −
- Anticoagulation According to D-dimer Level
- if D-dimer was less than 1 µg/mL
- if bodyweight was less than 100 kg, Enoxaparin at 40 mg was given subcutaneously (SC) daily.
- if bodyweight was between100 kg and 150 kg, SC Enoxaparin at 40 mg was given twice daily.
- if bodyweight was more than 150 kg, SC Enoxaparin at 60 mg was given twice daily.
- if D-dimer more than 1 µg/mL
- if bodyweight was less than 100 kg, SC Enoxaparin at 40 mg was given twice daily.
- if bodyweight was between 100 kg and 150 kg, SC Enoxaparin at 80 mg was given twice daily.
- if bodyweight was more than 150 kg, SC Enoxaparin at 120 mg was given twice daily.
- −
- Anticoagulation According to the Flexible Protocol
2.3.4. Follow-Up for Surviving Patients for 3 Months after Discharge from the Hospital
- Cure: considered if patients returned to their usual activities before COVID-19 with O2 saturations 96% or above, for patients with no history of respiratory failure before COVID-19, or for patients who returned to their baseline saturations with clearance of the chest by X-ray or chest CT.
- Death.
- Mild residual fibrosis with desaturation from 90 to 95 with residual lung fibrosis, including mid-reticular infiltrates but not requiring long-term O2 therapy.
- Moderate lung infiltrations with desaturation from 85 to 89 requiring O2 therapy and further follow-up, with bilateral residual lung infiltrates but occupy less than 50% of both lung fields.
- Severe disability and O2 saturation below 84% with the need for long-term oxygen therapy and chest X-ray or CT showing bilateral extensive lung fibrosis of more than 50% of the lung field, with the need for long-term rehabilitation.
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
3.1. Baseline Characteristics of the Studied Cohort
3.2. CBC Finding of the Studied Cohort
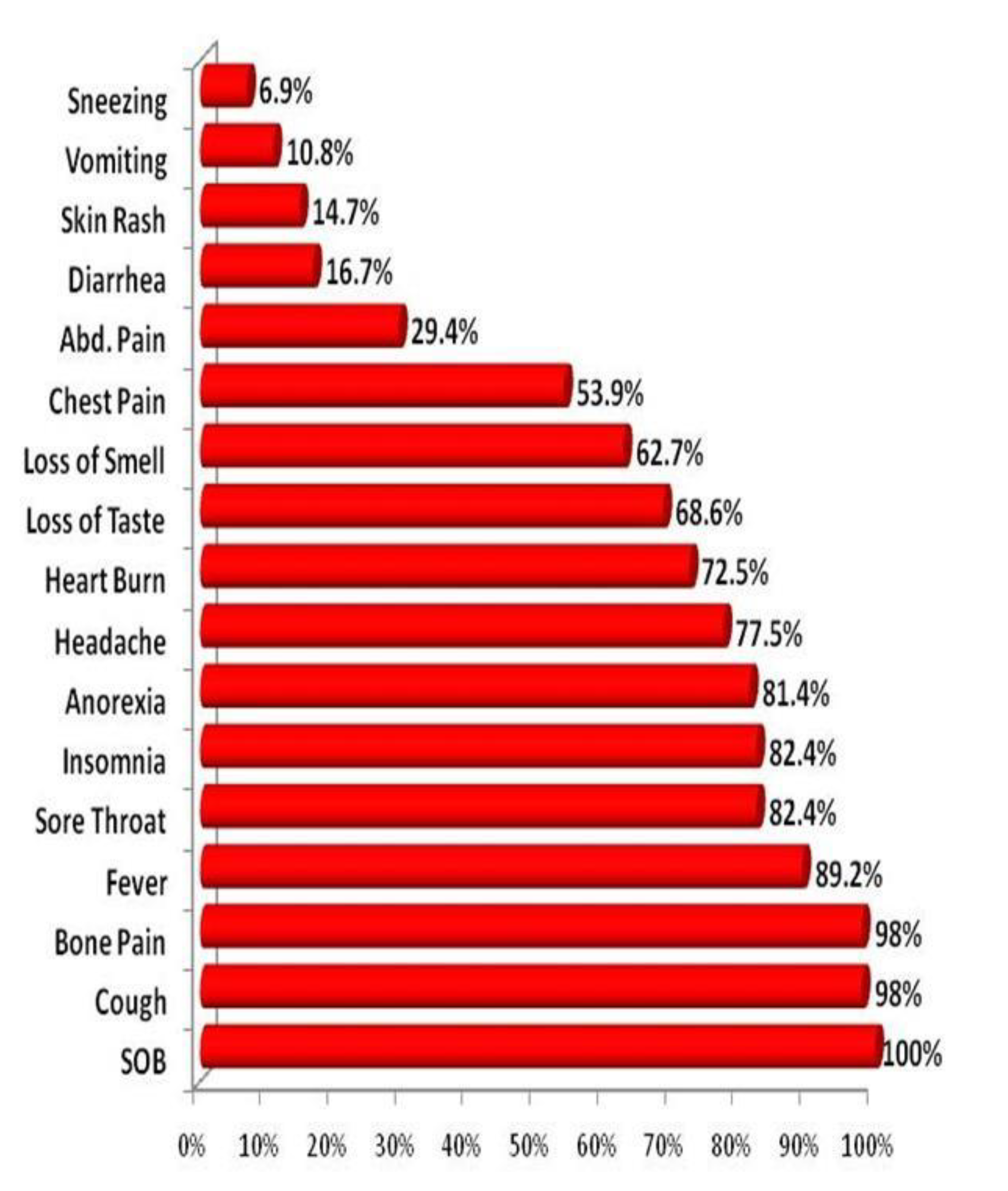
3.3. Prevalence of Symptoms among Severe COVID-19 Pneumonia Patients
3.4. Laboratory Panel of the Studied Cohort
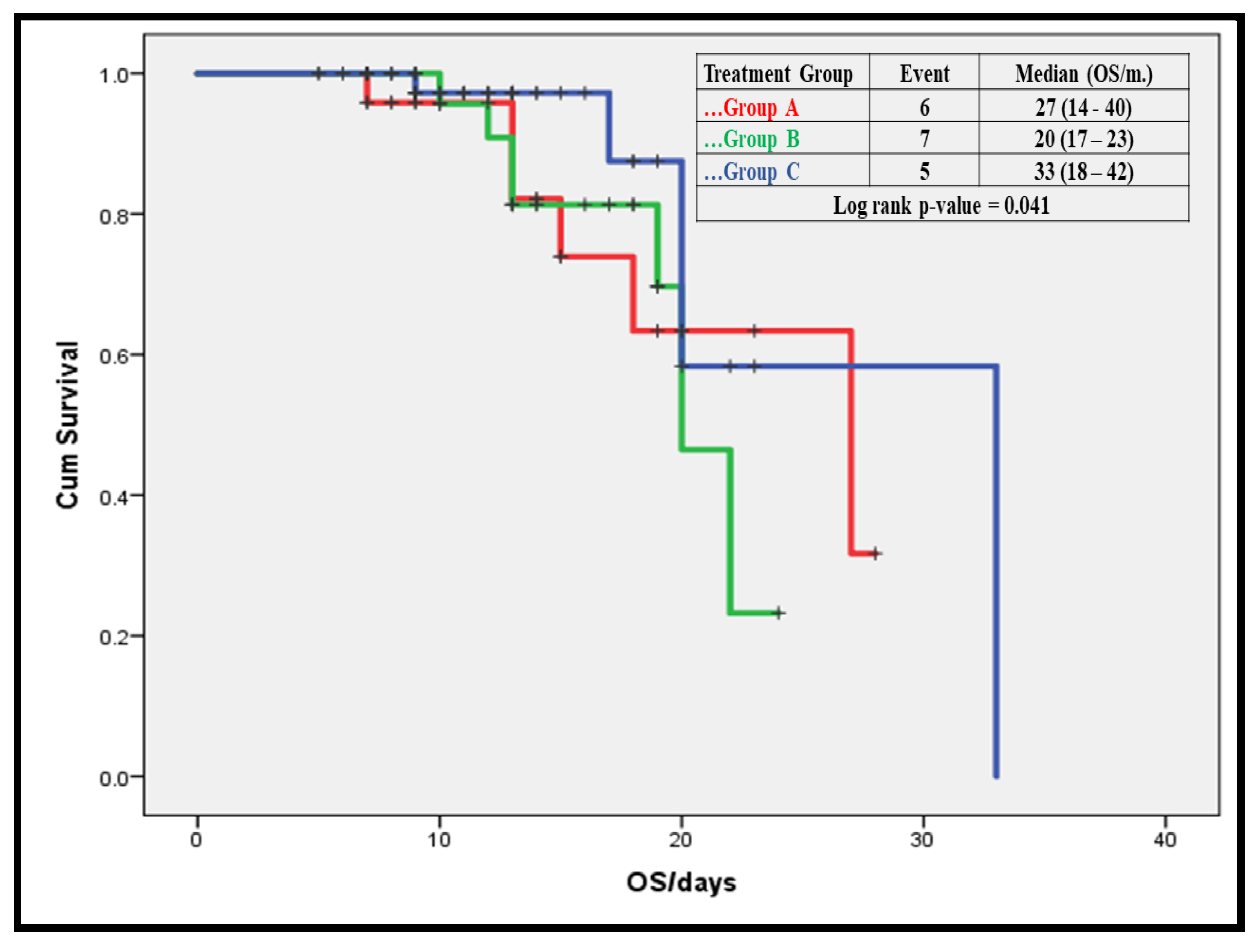
3.5. Relationship between Disease Outcome/Complication and Treatment Modality
3.6. Mortality Predictors among Severe COVID-19 Patients
4. Discussion
Clinical Therapeutic Staging Proposal
- Stage I: Mild (Early Infection): steroid administration during this stage could result in boosting viral replication and perhaps hindering the initiation of immune response.
- Stage II-a: Moderate (Pulmonary Involvement without Hypoxia) and Stage II-b: Moderate (Pulmonary Involvement with Hypoxia): the use of low-dose steroids during the pulmonary stage might be beneficial (by alleviating inflammation severity and thereby preventing a severe hyper-inflammation phase).
5. Study Strengths and Limitations
6. Conclusions and Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alhazzani, W.; Møller, M.H.; Arabi, Y.M.; Loeb, M.; Gong, M.N.; Fan, E.; Oczkowski, S.; Levy, M.M.; Derde, L.; Dzierba, A.; et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Intensive Care Med. 2020, 46, 854–887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rezaie, S. COVID-19: Clinical/Therapeutic Staging Proposal and Treatment: REBEL EM Blog. 2020. Available online: https://rebelem.com/covid-19-clinical-therapeutic-staging-proposal-and-treatment (accessed on 10 December 2020).
- Chan, J.F.W.; Yip, C.C.Y.; To, K.K.W.; Tang, T.H.C.; Wong, S.C.Y.; Leung, K.H.; Fung, A.Y.F.; Ng, A.C.K.; Zou, Z.; Tsoi, H.W.; et al. Improved Molecular Diagnosis of COVID-19 by the Novel, Highly Sensitive and Specific COVID-19-RdRp/Hel Real-Time Reverse Transcription-PCR Assay Validated In Vitro and with Clinical Specimens. J. Clin. Microbiol. 2020, 58, e00310-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollina, U.; Karadağ, A.S.; Rowland-Payne, C.; Chiriac, A.; Lotti, T. Cutaneous Signs in COVID-19Patients: A Review. Dermatol. Ther. 2020, 33, e13549. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.M.; Monogue, M.L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 323, 1824–1836. [Google Scholar] [CrossRef]
- Bhimraj, A.; Morgan, R.L.; Shumaker, A.H.; Lavergne, V.; Baden, L.; Cheng, V.C.C.; Edwards, K.M.; Gandhi, R.; Muller, W.J.; O’Horo, J.C.; et al. Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19. Clin. Infect. Dis. 2020. [CrossRef]
- World Health Organization. Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases: Interim Guidance, 14 January 2020. Bull. World Health Organ. 2020. Available online: https://www.who.int/publications/i/item/10665-331501 (accessed on 30 April 2021).
- Epidemiology Working Group for NCIP Epidemic Response CCfDCaP. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19) in China. Zhonghualiuxingbingxuezazhi 2020, 41, 145–151. [Google Scholar]
- Wayne, P. Blood Gas and pH Analysis and Related Measurements. Approv. Guidel. 2009, 21, 14. [Google Scholar]
- Fadel, R.; Morrison, A.R.; Vahia, A.; Smith, Z.R.; Chaudhry, Z.; Bhargava, P.; Miller, J.; Kenney, R.M.; Alangaden, G.; Ramesh, M.S.; et al. Early Short-Course Corticosteroids in Hospitalized Patients With COVID-19. Clin. Infect. Dis. 2020, 71, 2114–2120. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Lu, L.; Cao, W.; Li, T. Hypothesis for Potential Pathogenesis of SARS-CoV-2 Infection—A Review of Immune Changes in Patients with Viral Pneumonia. Emerg. Microbes Infect. 2020, 9, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Bavaro, D.; Diella, L.; Fabrizio, C.; Sulpasso, R.; Bottalico, I.; Calamo, A.; Santoro, C.; Brindicci, G.; Bruno, G.; Mastroianni, A.; et al. Peculiar Clinical Presentation of COVID-19 and Predictors of Mortality in the Elderly: A MulticentreRetrospective Cohort study. Int. J. Infect. Dis. 2021, 105, 709–715. [Google Scholar] [CrossRef]
- Cao, W.; Li, T. COVID-19: Towards Understanding of Pathogenesis. Cell Res. 2020, 30, 367–369. [Google Scholar] [CrossRef]
- Runfeng, L.; Yunlong, H.; Jicheng, H.; Weiqi, P.; Qinhai, M.; Yongxia, S.; Chufang, L.; Jin, Z.; Zhenhua, J.; Haiming, J.; et al. Lianhuaqingwen Exerts Anti-Viral and Anti-Inflammatory Activity Against Novel Coronavirus (SARS-CoV-2). Pharmacol. Res. 2020, 156, 104761. [Google Scholar] [CrossRef]
- Siddiqi, H.K.; Mehra, M.R. COVID-19 Illness in Native and Immunosuppressed States: A Clinical–Therapeutic Staging Proposal. J. Hear. Lung Transplant. 2020, 39, 405–407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical Course and Outcomes of Critically Ill Patients with SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A RetrospectiveCohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Ruan, Q.; Yang, K.; Wang, W.; Jiang, L.; Song, J. Clinical Predictors of Mortality due to COVID-19 Based on an Analysis of Data of 150 Patients from Wuhan, China. Intensive Care Med. 2020, 46, 846–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giamarellos-Bourboulis, E.J.; Netea, M.G.; Rovina, N.; Akinosoglou, K.; Antoniadou, A.; Antonakos, N.; Damoraki, G.; Gkavogianni, T.; Adami, M.-E.; Katsaounou, P.; et al. Complex Immune Dysregulation in COVID-19 Patients with Severe Respiratory Failure. Cell Host Microbe 2020, 27, 992–1000. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of Immune Response in Patients with COVID-19 in Wuhan, China. Oxford Academic. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Bester, J.; Matshailwe, C.; Pretorius, E. Simultaneous Presence of Hypercoagulation and Increased Clot Lysis Time due to IL-1β, IL-6 and IL-8. Cytokine 2018, 110, 237–242. [Google Scholar] [CrossRef]
- Wan, S.; Yi, Q.; Fan, S.; Lv, J.; Zhang, X.; Guo, L.; Lang, C.; Xiao, Q.; Xiao, K.; Yi, Z.; et al. Characteristics of Lymphocyte Subsets and Cytokines in Peripheral Blood of 123 Hospitalized Patients with 2019 Novel Coronavirus Pneumonia (NCP). Medrxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant Treatment is Associated with Decreased Mortality in Severe Coronavirus Disease 2019 Patients with Coagulopathy. J. Thromb. Haemost. 2020, 18, 1094–1099. [Google Scholar] [CrossRef] [PubMed]
- Barrett, C.D.; Moore, H.B.; Yaffe, M.B.; Moore, E.E. ISTH Interim Guidance on Recognition and Management of Coagulopathy in COVID-19: A Comment. J. Thromb. Haemost. 2020, 18, 2060–2063. [Google Scholar] [CrossRef] [PubMed]
- Kreuziger, L.; Lee, A.; Garcia, D.; Cuker, A.; Cushman, M.; DeSancho, M.; Connors, J.M. COVID-19 and VTE/Anticoagulation: Frequently Asked Questions American Society of Hematology. 2021. Available online: https://www.hematology.org/covid-19/covid-19-and-vte-anticoagulation (accessed on 30 April 2021).
- Shi, C.; Wang, C.; Wang, H.; Yang, C.; Cai, F.; Zeng, F.; Cheng, F.; Liu, Y.; Zhou, T.; Deng, B.; et al. The potential of Low Molecular Weight Heparin to Mitigate Cytokine Storm in Severe COVID-19 Patients: A Retrospective Clinical Study. Medrxiv 2020. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Category | (n = 123) |
|---|---|---|
| Age (years) |
| 50.62 ± 16.4 |
| 51.5 (22) | |
| Sex |
| 90 (73.2%) |
| 33 (26.8%) | |
| BMI |
| 28.29 ± 4.8 |
| 28 (5) | |
| Chronic Disease History: | Number (%) | |
| 37 (30.0%) | |
| 34 (27.6%) | |
| 27 (22.0%) | |
| 20 (16.3%) | |
| 19 (15.4%) | |
| 16 (13.0%) | |
| 14 (11.4%) | |
| 9 (7.3%) | |
| 6 (4.9%) | |
| 2 (1.6%) | |
| Parameter | Category | (n = 123) |
|---|---|---|
| CBC Parameters: | ||
| HGB level (g/dL) |
| 12.63 ± 1.9 |
| 12.5 (3.3) | |
| WBCs (*103) |
| 5.98 ± 2.8 |
| 5.5 (4) | |
| Platelet (*103) |
| 246.27 ± 93.2 |
| 218 (126) | |
| Lymphocytes (%) |
| 25.32 ± 16.5 |
| 19 (16) | |
| Neutrophils (%) |
| 64.70 ± 18.7 |
| 67 (30) | |
| Monocytes (%) |
| 9.11 ± 4.2 |
| 9 (6) | |
| NLR |
| 4.59 ± 4.0 |
| 3.5 (3) |
| Parameter | Category | (n = 123) |
|---|---|---|
| ESR (mm/1sthr) |
| 19.40 ± 13.8 |
| 14 (11) | |
| Serum creatinine (mg/dL) |
| 90.44 ± 15.9 |
| 91 (21) | |
| Liver function parameters: | ||
| ALT (U/L) |
| 34.22 ± 18.2 |
| 28.5 (18) | |
| AST (U/L) |
| 34.54 ± 14.3 |
| 31 (21) | |
| D-dimer (μg/mL) |
| 1.43 ± 0.8 |
| 1.2 (1) | |
| CRP |
| 13.94 ± 5.2 |
| 12 (7) | |
| Ferritin (ng/mL) |
| 459.55 ± 206.1 |
| 421 (293) |
| Group A (n = 32) | Group B (n = 45) | Group C (n = 46) | p | |
|---|---|---|---|---|
| Baseline Characteristics: | ||||
| Age (years) | 50.71 ± 15.6 | 46.44 ± 16.6 | 53.48 ± 16.4 | 0.177 ** |
| p *** | 0.334 | 0.063 | 0.501 | |
| Sex (Male/Female) | 24/8 | 33/11 | 34/12 | 0.963 |
| BMI | 29.42 ± 4.6 | 27.14 ± 4.3 | 28.49 ± 4.9 | 0.198 ** |
| p *** | 0.079 | 0.221 | 0.441 | |
| In-hospital outcome: | ||||
| Pulmonary embolism | 6 (18.8%) | 8 (17.8%) | 1 (2.2%) | 0.020 |
| Bleeding | 4 (12.5%) | 5 (11.1%) | 1 (2.2%) | 0.047 |
| Hematoma | 5 (15.6%) | 6 (13.3%) | 3 (6.5%) | 0.025 |
| Secondarybacterial infection | 13 (40.6%) | 19 (42.2%) | 21 (45.7%) | 0.349 |
| AKI | 4 (12.5%) | 5 (11.1%) | 2 (4.3%) | 0.031 |
| MI | 3 (9.4%) | 3 (6.7%) | 0 (0%) | 0.016 |
| DM | 6 (18.8%) | 11 (24.4%) | 9 (19.6%) | 0.457 |
| Neuromuscular weakness | 9 (28.1%) | 14 (31.1%) | 11 (23.9%) | 0.255 |
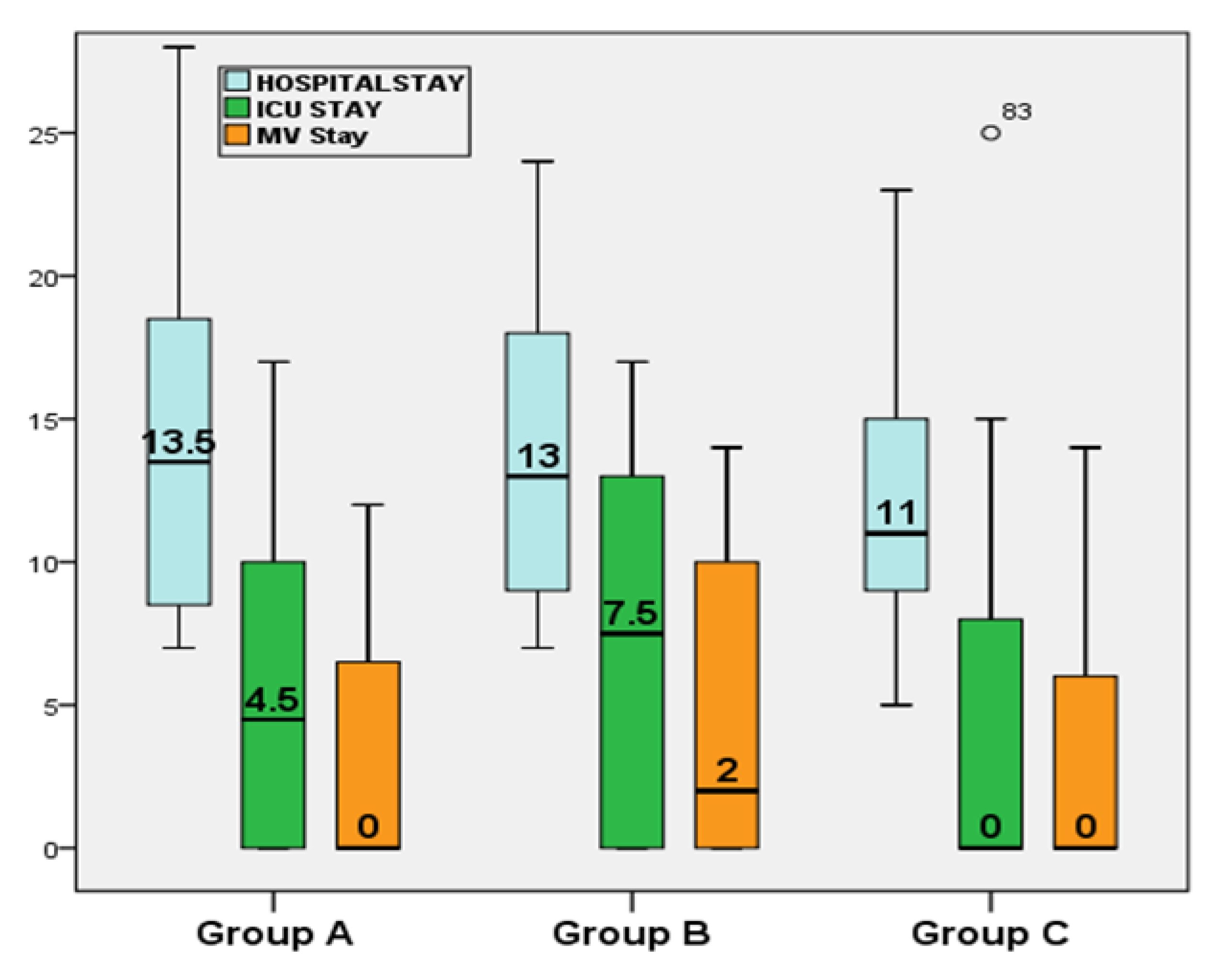
| Hospital stay/days | 14.13 ± 1.3 | 13.63 ± 0.9 | 12.46 ± 0.8 | 0.432 ** |
| p *** | 0.738 | 0.361 | 0.234 | |
| ICU stay (days) | 5.88 ± 1.2 | 7.03 ± 1.1 | 4.52 ± 0.9 | 0.178 ** |
| p *** | 0.473 | 0.070 | 0.368 | |
| MV duration (days) | 3.42 ± 0.9 | 4.53 ± 0.9 | 2.96 ± 0.6 | 0.334 ** |
| p *** | 0.375 | 0.142 | 0.694 | |
| Three-month outcome after discharge: | ||||
| 12 (37.5%) | 26 (57.8%) | 31 (67.4%) | 0.028 * |
| 14 (43.8%) | 11 (24.4%) | 10 (21.7%) | |
| 6 (18.8%) | 7 (15.6%) | 5 (10.9%) | |
| Variable | HR | 95% CI | P |
|---|---|---|---|
| Age (years) | 1.042 | 0.993–1.093 | 0.093 |
| Sex (male) | 2.099 | 0.989–1.111 | 0.303 |
| Treatment Modality: | |||
| 0.042 | ||
| 0.917 | 0.701–1.867 | 0.204 |
| 0.716 | 0.555–0.923 | 0.010 |
| History of Asthma | 4.516 | 1.849–11.035 | 0.031 |
| History of COPD | 14.678 | 1.610–33.785 | 0.017 |
| History of DM | 2.296 | 1.392–3.788 | 0.001 |
| History of CKD | 25.202 | 5.811–59.863 | 0.003 |
| History of Lung Fibrosis | 12.159 | 1.517–37.467 | 0.019 |
| History of MI | 6.878 | 1.923–51.271 | 0.022 |
| CRP | 1.181 | 1.012–1.377 | 0.034 |
| NLR | 1.062 | 1.008–1.348 | 0.046 |
| Hospital stay/days | 0.555 | 0.432–0.715 | ≤0.001 |
| ICU stay/days | 0.753 | 0.617–0.919 | 0.005 |
| MV duration/days | 0.790 | 0.650–0.960 | 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassan, A.T.; Elmoniem, A.E.A.; Abdelrady, M.M.; Mohamed, M.E.; Mokhtar, M.A.; Elsherif, A.A.; Saied, G.M.; Kasem, S.M. Challenges in Steroid and Anticoagulant Therapy in Severe COVID-19 Pneumonia: A Prospective Study. Antibiotics 2021, 10, 1214. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101214
Hassan AT, Elmoniem AEA, Abdelrady MM, Mohamed ME, Mokhtar MA, Elsherif AA, Saied GM, Kasem SM. Challenges in Steroid and Anticoagulant Therapy in Severe COVID-19 Pneumonia: A Prospective Study. Antibiotics. 2021; 10(10):1214. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101214
Chicago/Turabian StyleHassan, Alaa Thabet, Alaa E. Abd Elmoniem, Marwa Mahmoud Abdelrady, Mona Embarek Mohamed, Mohamed A. Mokhtar, Abdelhalim A. Elsherif, Ghada Mohamed Saied, and Soheir M. Kasem. 2021. "Challenges in Steroid and Anticoagulant Therapy in Severe COVID-19 Pneumonia: A Prospective Study" Antibiotics 10, no. 10: 1214. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101214