
Antibiotic Consumption and Its Relationship with Bacterial Resistance Profiles in ESKAPE Pathogens in a Peruvian Hospital

 , ,
, ,
Abstract
:1. Introduction
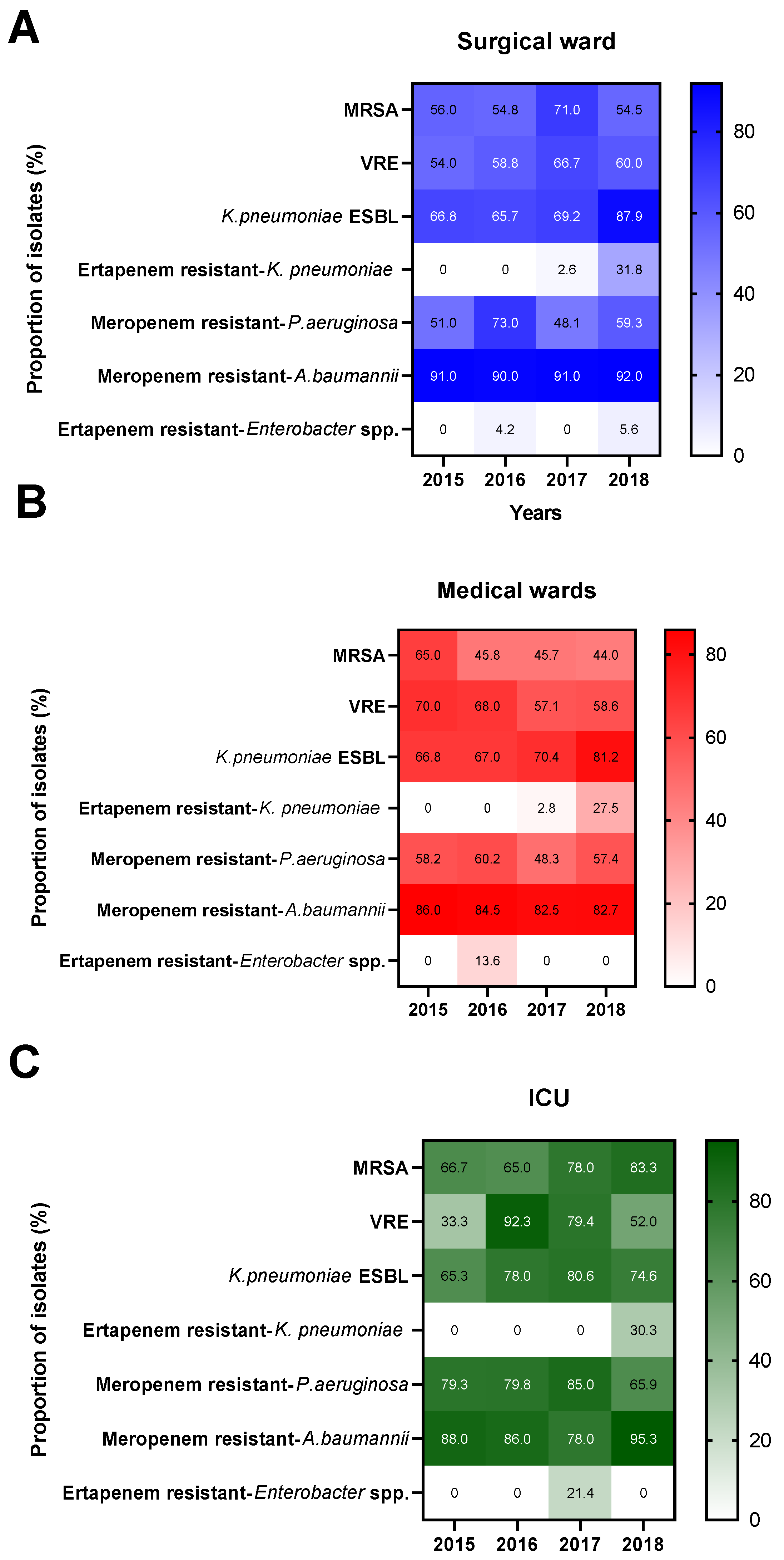
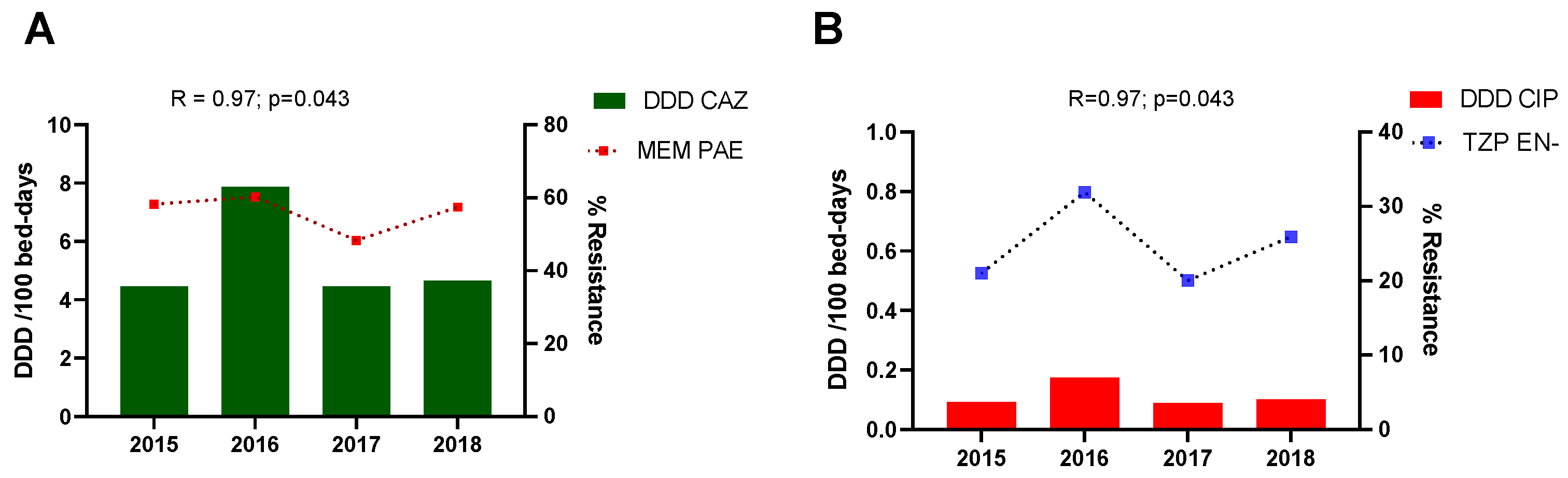
2. Results
3. Discussion
4. Materials and Methods
4.1. Antimicrobial Resistance Profiles
4.2. Antimicrobial Consumption
4.3. Antimicrobial Consumption-Bacterial Resistance Correlation
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Rice, L.B. Federal Funding for the Study of Antimicrobial Resistance in Nosocomial Pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef]
- Pendleton, J.N.; Gorman, S.P.; Gilmore, B.F. Clinical relevance of the ESKAPE pathogens. Expert Rev. Anti-infective Ther. 2013, 11, 297–308. [Google Scholar] [CrossRef]
- Benkő, R.; Gajdács, M.; Matuz, M.; Bodó, G.; Lázár, A.; Hajdú, E.; Papfalvi, E.; Hannauer, P.; Erdélyi, P.; Pető, Z. Prevalence and Antibiotic Resistance of ESKAPE Pathogens Isolated in the Emergency Department of a Tertiary Care Teaching Hospital in Hungary: A 5-Year Retrospective Survey. Antibiotics 2020, 9, 624. [Google Scholar] [CrossRef] [PubMed]
- CDC. Antibiotic Resistance Threats in the United States, 2019; Department of Health and Human Services, CDC: Atlanta, GA, USA, 2019. Available online: www.cdc.gov/DrugResistance/Biggest-Threats.html (accessed on 21 May 2021). [CrossRef] [Green Version]
- Founou, R.C.; Founou, L.L.; Essack, S. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189621. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karam, G.; Chastre, J.; Wilcox, M.H.; Vincent, J.-L. Antibiotic strategies in the era of multidrug resistance. Crit. Care 2016, 20, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEwen, S.A.; Collignon, P.J. Antimicrobial Resistance: A One Health Perspective. Microbiol. Spectr. 2018, 6. [Google Scholar] [CrossRef] [Green Version]
- Harbarth, S.; Balkhy, H.H.; Goossens, H.; Jarlier, V.; Kluytmans, J.; Laxminarayan, R.; Saam, M.; Van Belkum, A.; Pittet, D. Antimicrobial resistance: One world, one fight! Antimicrob. Resist. Infect. Control. 2015, 4, 49. [Google Scholar] [CrossRef] [Green Version]
- Holmes, A.H.; Moore, L.S.P.; Sundsfjord, A.; Steinbakk, M.; Regmi, S.; Karkey, A.; Guerin, P.; Piddock, L. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet 2016, 387, 176–187. [Google Scholar] [CrossRef]
- Gajdács, M. The Concept of an Ideal Antibiotic: Implications for Drug Design. Molecules 2019, 24, 892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Versporten, A.; Zarb, P.; Caniaux, I.; Gros, M.-F.; Drapier, N.; Miller, M.; Jarlier, V.; Nathwani, D.; Goossens, H.; Koraqi, A.; et al. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: Results of an internet-based global point prevalence survey. Lancet Glob. Health 2018, 6, e619–e629. [Google Scholar] [CrossRef] [Green Version]
- Una, C.M.; Rodríguez-Noriega, E.; Bavestrello, L.; Guzman-Blanco, M. Gram-Negative Infections in Adult Intensive Care Units of Latin America and the Caribbean. Crit. Care Res. Pract. 2014, 2014, 480463. [Google Scholar] [CrossRef]
- Hernández-Gómez, C.; Hercilla, L.; Mendo, F.; Pérez-Lazo, G.; Contreras, E.; Ramírez, E.; Flores, W.; Julca; Chuquiray, N.; Arenas, B.; et al. Programas de optimización del uso de antimicrobianos en Perú: Un acuerdo sobre lo fundamental. [Antimicrobial Stewardship programs in Peru: A fundamental agreement]. Rev. Chil. Infectol. 2019, 36, 565–575. (In Spanish) [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quirós, R.E.; Bardossy, A.C.; Angeleri, P.; Zurita, J.; Espinoza, W.R.A.; Carneiro, M.; Guerra, S.; Medina, J.; Luquerna, X.C.; Guerra, A.; et al. Antimicrobial stewardship programs in adult intensive care units in Latin America: Implementation, assessments, and impact on outcomes. Infect. Control Hosp. Epidemiol. 2021, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, J.S.; Motoa, G.; Escandón-Vargas, K.; Bavestrello, L.; Quiros, R.; Hernandez, C. Current Antimicrobial Stewardship Practices in Latin America: Where Are we? Open Forum. Infect. Dis. 2015, 2 (Suppl. 1), 192. Available online: https://0-academic-oup-com.brum.beds.ac.uk/ofid/article/2/suppl_1/192/2635214 (accessed on 21 May 2021). [CrossRef]
- Pan American Health Organization. Magnitude and Trends of Antimicrobial Resistance in Latin America. ReLAVRA 2014, 2015, 2016. Summary Report. 2020. Available online: https://www.paho.org/en/documents/magnitude-and-trends-antimicrobial-resistance-latin-america-relavra-2014-2015-2016 (accessed on 21 May 2021).
- Krapp, F.; Amaro, C.; Ocampo, K.; Astocondor, L.; Hinostroza, N.; Riveros, M.; Garcia, C. 1189. A Comprehensive Characterization of the Emerging Carbapenem-Resistant Klebsiella pneumoniae Clinical Isolates From a Public Hospital in Lima, Peru. Open Forum Infect. Dis. 2018, 5 (Suppl. 1), S359–S360. [Google Scholar] [CrossRef]
- Resurrección-Delgado, C.; Montenegro-Idrogo, J.J.; Chiappe-Gonzalez, A.; Vargas-Gonzales, R.; Cucho-Espinoza, C.; Mamani-Condori, D.H.; Huaroto-Valdivia, L.M. Klebsiella pneumoniae New Delhi metalo-lactamase in a Peruvian national hospital. Rev. Peru. Med. Exp. Salud Publica 2017, 34, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Falagas, M.E.; Tansarli, G.S.; Karageorgopoulos, D.E.; Vardakas, K.Z. Deaths attributable to carbapenem-resistant enterobacteriaceae infections. Emerg. Infect. Dis. 2014, 20, 1170–1175. [Google Scholar] [CrossRef]
- Chen, Q.; Li, D.; Beiersmann, C.; Neuhann, F.; Moazen, B.; Lu, G.; Müller, O. Risk factors for antibiotic resistance development in healthcare settings in China: A systematic review. Epidemiol. Infect. 2021, 149, E141. [Google Scholar] [CrossRef]
- Cardoso, T.; Ribeiro, O.; Aragão, I.C.; Costa-Pereira, A.; Sarmento, A.E. Additional risk factors for infection by multidrug-resistant pathogens in healthcare-associated infection: A large cohort study. BMC Infect. Dis. 2012, 12, 375. [Google Scholar] [CrossRef] [Green Version]
- KKofteridis, D.P.; Valachis, A.; Dimopoulou, D.; Maraki, S.; Christidou, A.; Mantadakis, E.; Samonis, G. Risk factors for carbapenem-resistant Klebsiella pneumoniae infection/colonization: A case–case-control study. J. Infect. Chemother. 2014, 20, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Van Loon, K.; Holt, A.F.V.I.; Vos, M.C. A Systematic Review and Meta-analyses of the Clinical Epidemiology of Carbapenem-Resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2018, 62, e01730-17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinig, E.J.; Duchene, S.; Robinson, D.A.; Monecke, S.; Yokoyama, M.; Laabei, M.; Slickers, P.; Andersson, P.; Williamson, D.; Kearns, A.; et al. Evolution and Global Transmission of a Multidrug-Resistant, Community-Associated Methicillin-Resistant Staphylococcus aureus Lineage from the Indian Subcontinent. mBio 2019, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, A.M.; Daneman, N.; Tan, C.; Brownstein, J.S.; MacFadden, D.R. Evaluating the Relationship Between Hospital Antibiotic Use and Antibiotic Resistance in Common Nosocomial Pathogens. Infect. Control Hosp. Epidemiol. 2017, 38, 1457–1463. [Google Scholar] [CrossRef]
- Lesho, E.P.; Clifford, R.J.; Chukwuma, U.; Kwak, Y.I.; Maneval, M.; Neumann, C.; Xie, S.; Nielsen, L.E.; Julius, M.D.; McGann, P.; et al. Carbapenem-resistant Enterobacteriaceae and the correlation between carbapenem and fluoroquinolone usage and resistance in the US military health system. Diagn. Microbiol. Infect. Dis. 2015, 81, 119–125. [Google Scholar] [CrossRef]
- Liu, L.; Liu, B.; Li, Y.; Zhang, W. Successful control of resistance in Pseudomonas aeruginosa using antibiotic stewardship and infection control programs at a Chinese university hospital: A 6-year prospective study. Infect. Drug Resist. 2018, 11, 637–646. [Google Scholar] [CrossRef] [Green Version]
- Plüss-Suard, C.; Pannatier, A.; Kronenberg, A.; Mühlemann, K.; Zanetti, G. Impact of Antibiotic Use on Carbapenem Resistance in Pseudomonas aeruginosa: Is There a Role for Antibiotic Diversity? Antimicrob. Agents Chemother. 2013, 57, 1709–1713. [Google Scholar] [CrossRef] [Green Version]
- Cohen, M.; Block, C.; Moses, A.; Nir-Paz, R. Exposure to ertapenem is possibly associated with Pseudomonas aeruginosa antibiotic resistance. Clin. Microbiol. Infect. 2014, 20, O188–O196. [Google Scholar] [CrossRef] [Green Version]
- McDougall, D.A.J.; Morton, A.P.; Playford, E.G. Association of ertapenem and antipseudomonal carbapenem usage and carbapenem resistance in Pseudomonas aeruginosa among 12 hospitals in Queensland, Australia. J. Antimicrob. Chemother. 2012, 68, 457–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, L.; Castelo-Corral, L.; Gutiérrez-Urbón, J.-M.; Molina, F.; López-Calviño, B.; Bou, G.; Llinares, P. Impact of ertapenem use on Pseudomonas aeruginosa and Acinetobacter baumannii imipenem susceptibility rates: Collateral damage or positive effect on hospital ecology? J. Antimicrob. Chemother. 2013, 68, 1917–1925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuesta, D.P.; Blanco, V.M.; Vallejo, M.E.; Hernández-Gómez, C.; Maya, J.J.; Motoa, G.; Correa, A.; Matta, L.; Rosso, F.; Camargo, R.D.; et al. Clinical impact of ertapenem de-escalation in critically-ill patients with Enterobacteriaceae infections. Rev. Chil. Infectol. 2019, 36, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Karaiskos, I.; Giamarellou, H. Carbapenem-Sparing Strategies for ESBL Producers: When and How. Antibiotics 2020, 9, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, C.-K.; Tang, H.-J.; Lai, C.-C.; Chen, Y.-Y.; Chang, P.-C.; Liu, W.-L. Correlation between antibiotic consumption and carbapenem-resistant Acinetobacter baumannii causing health care-associated infections at a hospital from 2005 to 2010. J. Microbiol. Immunol. Infect. 2015, 48, 540–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, C.-C.; Shi, Z.-Y.; Chen, Y.-H.; Wang, F.-D. Effects of various antimicrobial stewardship programs on antimicrobial usage and resistance among common gram-negative bacilli causing health care-associated infections: A multicenter comparison. J. Microbiol. Immunol. Infect. 2016, 49, 74–82. [Google Scholar] [CrossRef] [PubMed]
- ATC/DDD Index 2019 [Internet]. Noruega: WHO Collaborating Centre for Drug Statistics Methodology [New ATC/DDDs and Alterations from the March 2019 Meeting]. Available online: http://www.whocc.no/atc_ddd_index/ (accessed on 12 October 2019).
- Hermosilla Nájera, L.; Canut Blasco, A.; Ulibarrena Sanz, M.; Abásolo Osinaga, E.; Abecia Inchaurregui, L.C. Evolución de la utilización de antimicrobianos durante los años 1996-2000 en un hospital general. Estudio pormenorizado de la UCI. Farm Hosp. 2003, 27, 31–37. [Google Scholar] [PubMed]
- Vega, E.; Fontana, D.; Iturrieta, M.; Segovia, L.; Rodríguez, G.; Agüero, S. Consumo de antimicrobianos en la Unidad de Terapia Intensiva del Hospital Dr. Guillermo Rawson-San Juan, Argentina. Rev. Chil. Infectol. 2015, 32, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Surgical Ward | Statistical Values | Medical Wards | Statistical Values | ICU | Statistical Values | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Antibiotic Consumption | Bacterial Resistance | R | p | Antibiotic Consumption | Bacterial Resistance | R | p | Antibiotic Consumption | Bacterial Resistance | R | p | |||
| TZP (↑) | TZP | PAE | 0.95 | 0.051 | TZP (↑) | TZP | PAE | 0.80 | 0.200 | TZP (↓) | TZP | PAE | 0.32 | 0.683 |
| TZP | EN- | 0.95 | 0.051 | TZP | EN- | 0.16 | 0.834 | TZP | EN- | −0.83 | 0.167 | |||
| IPM | KPN | 0.23 | 0.772 | IPM | KPN | 0.95 | 0.051 | IPM | KPN | 0.00 | 1.000 | |||
| MEM | KPN | 0.23 | 0.772 | MEM | KPN | 0.95 | 0.051 | MEM | KPN | 0.00 | 1.000 | |||
| MEM | PAE | 0.80 | 0.200 | MEM | PAE | 0.79 | 0.201 | MEM | PAE | 0.00 | 1.000 | |||
| MEM (↑) | MEM | KPN | −0.06 | 0.944 | MEM (↑) | MEM | KPN | 0.63 | 0.367 | IPM (↓) | IPM | KPN | −0.77 | 0.225 |
| TZP | EN- | 0.95 | 0.051 | TZP | EN- | 0.36 | 0.635 | IPM | PAE | −0.40 | 0.600 | |||
| TZP | KPN | 0.57 | 0.431 | TZP | KPN | 0.85 | 0.153 | MEM | KPN | −0.77 | 0.225 | |||
| MEM | PAE | 0.95 | 0.051 | MEM | PAE | 0.89 | 0.102 | TZP | KPN | −0.40 | 0.600 | |||
| MEM | ABA | −0.63 | 0.367 | MEM | ABA | 0.80 | 0.200 | TZP | EN- | −0.74 | 0.262 | |||
| ETP (↑) | ETP | KPN | 0.63 | 0.367 | ETP (↑) | ETP | KPN | 0.83 | 0.166 | ETP (↔) | ETP | KPN | −0.77 | 0.225 |
| ETP | EN- | 0.89 | 0.105 | ETP | EN- | 0.00 | 1.000 | ETP | EN- | 0.77 | 0.225 | |||
| IPM | PAE | 0.60 | 0.400 | IPM | PAE | 0.95 | 0.051 | IPM | PAE | −0.34 | 0.656 | |||
| MEM | PAE | 0.60 | 0.400 | MEM | PAE | 0.63 | 0.367 | MEM | PAE | 0.74 | 0.262 | |||
| CAZ (↔) | MEM | ABA | −0.93 | 0.007 | CAZ (↔) | MEM | ABA | 0.60 | 0.400 | CAZ (↓) | MEM | ABA | −0.34 | 0.685 |
| IPM | ABA | −0.93 | 0.007 | IPM | ABA | 0.60 | 0.400 | IPM | ABA | −0.30 | 0.699 | |||
| MEM | PAE | 0.80 | 0.200 | MEM | PAE | 0.97 | 0.031 | MEM | PAE | 0.21 | 0.789 | |||
| IPM | PAE | 0.80 | 0.200 | IPM | PAE | 0.50 | 0.497 | IPM | PAE | −0.27 | 0.722 | |||
| CIP (↔) | CRO | EN- | 0.20 | 0.800 | CIP (↔) | CRO | EN- | 0.88 | 0.115 | CIP (↓) | CRO | EN- | −0.80 | 0.200 |
| CAZ | KPN | 0.80 | 0.200 | CAZ | KPN | −0.05 | 0.953 | CAZ | KPN | 0.20 | 0.800 | |||
| CAZ | EN- | 0.40 | 0.600 | CAZ | EN- | 0.63 | 0.367 | CAZ | EN- | −0.60 | 0.400 | |||
| MEM | EN- | −0.89 | 0.105 | TZP | EN- | 0.83 | 0.171 | TZP | EN- | −0.95 | 0.051 | |||
| CIP (↔) | OXA | SAU | −0.20 | 0.800 | CIP (↔) | OXA | SAU | −0.80 | 0.200 | CIP (↓) | OXA | SAU | −0.75 | 0.242 |
| IPM | PAE | 0.80 | 0.200 | MEM | PAE | 0.80 | 0.200 | MEM | PAE | 0.21 | 0.789 | |||
| AMK | PAE | 0.40 | 0.600 | AMK | PAE | 0.80 | 0.200 | AMK | PAE | 0.80 | 0.200 | |||
| IPM | ABA | −0.89 | 0.041 | MEM | ABA | 0.80 | 0.200 | MEM | ABA | −0.30 | 0.695 | |||
| MEM | ABA | −0.89 | 0.041 | TZP | EN- | 0.97 | 0.031 | TZP | EN- | −0.74 | 0.262 | |||
| AMK (↔) | AMK | PAE | 0.63 | 0.367 | AMK (↓) | AMK | PAE | 0.13 | 0.868 | AMK (↓) | AMK | PAE | 0.31 | 0.688 |
| AMK | KPN | 0.63 | 0.367 | AMK | KPN | −0.83 | 0.163 | AMK | KPN | −0.67 | 0.327 | |||
| AMK | EN- | 0.32 | 0.683 | AMK | EN- | 0.32 | 0.683 | AMK | EN- | −0.57 | 0.427 | |||
| IPM (↔) | IPM | KPN | −0.95 | 0.051 | IPM (↔) | IPM | KPN | −0.83 | 0.167 | MEM (↔) | MEM | KPN | −0.56 | 0.436 |
| IPM | PAE | 0.40 | 0.600 | IPM | PAE | −0.32 | 0.683 | TZP | EN- | −0.21 | 0.789 | |||
| MEM | KPN | −0.95 | 0.051 | MEM | KPN | −0.81 | 0.183 | TZP | KPN | −0.80 | 0.200 | |||
| TZP | KPN | −0.20 | 0.800 | TZP | KPN | −0.32 | 0.683 | MEM | PAE | 0.74 | 0.262 | |||
| TZP | EN- | 0.20 | 0.800 | TZP | EN- | 0.32 | 0.683 | MEM | ABA | −0.01 | 0.847 | |||
| CLI (↔) | OXA | SAU | 0.40 | 0.600 | CLI (↔) | OXA | SAU | −0.40 | 0.600 | CLI (↓) | OXA | SAU | −0.94 | 0.051 |
| CLI | SAU | 0.40 | 0.600 | CLI | SAU | −0.40 | 0.600 | CLI | SAU | −0.80 | 0.200 | |||
| SAM (↔) | MEM | ABA | −0.77 | 0.225 | SAM (↔) | MEM | ABA | 0.32 | 0.683 | SAM (↓) | MEM | ABA | −0.31 | 0.683 |
| IPM | ABA | −0.77 | 0.225 | IPM | ABA | 0.32 | 0.683 | IPM | ABA | −0.33 | 0.665 | |||
| VAN (↔) | VAN | EFM | −0.20 | 0.800 | VAN (↔) | VAN | EFM | 0.95 | 0.051 | VAN (↓) | VAN | EFM | −0.25 | 0.746 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Lazo, G.; Abarca-Salazar, S.; Lovón, R.; Rojas, R.; Ballena-López, J.; Morales-Moreno, A.; Flores-Paredes, W.; Arenas-Ramírez, B.; Illescas, L.R. Antibiotic Consumption and Its Relationship with Bacterial Resistance Profiles in ESKAPE Pathogens in a Peruvian Hospital. Antibiotics 2021, 10, 1221. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101221
Pérez-Lazo G, Abarca-Salazar S, Lovón R, Rojas R, Ballena-López J, Morales-Moreno A, Flores-Paredes W, Arenas-Ramírez B, Illescas LR. Antibiotic Consumption and Its Relationship with Bacterial Resistance Profiles in ESKAPE Pathogens in a Peruvian Hospital. Antibiotics. 2021; 10(10):1221. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101221
Chicago/Turabian StylePérez-Lazo, Giancarlo, Susan Abarca-Salazar, Renata Lovón, Rocío Rojas, José Ballena-López, Adriana Morales-Moreno, Wilfredo Flores-Paredes, Berenice Arenas-Ramírez, and Luis Ricardo Illescas. 2021. "Antibiotic Consumption and Its Relationship with Bacterial Resistance Profiles in ESKAPE Pathogens in a Peruvian Hospital" Antibiotics 10, no. 10: 1221. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101221