
Is Penicillin Allergy a Risk Factor for Early Dental Implant Failure? A Systematic Review

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
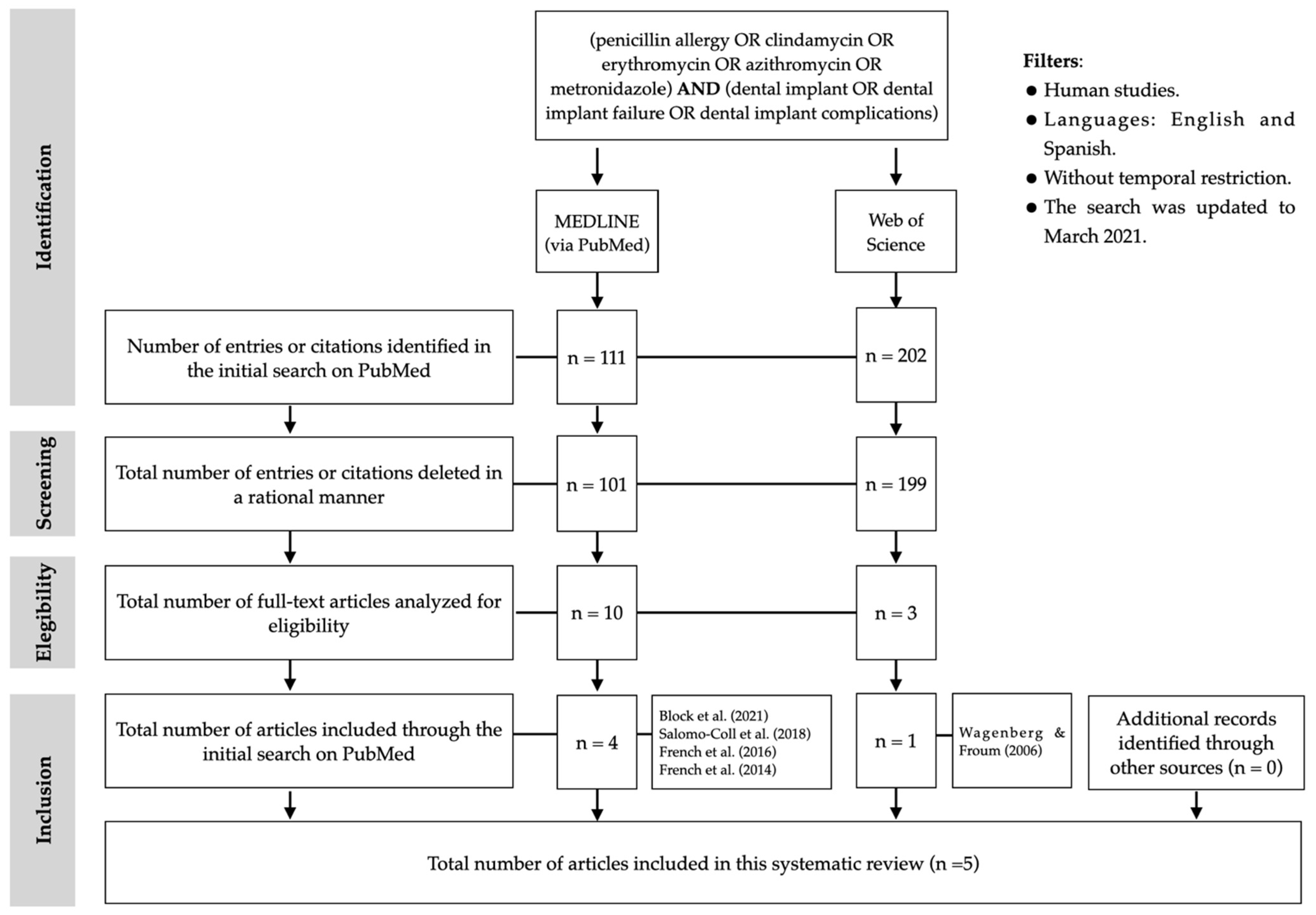
2.1. Search Strategy
2.2. Eligibility Criteria
2.2.1. Exclusion Criteria
2.2.2. Inclusion Criteria
2.3. Study Records
2.4. Risk of Bias
3. Results
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
4. Discussion
4.1. Suboptimal Efficacy of Alternative Antibiotics, Such as Clindamycin
4.2. Penicillin Allergy as a Genetic Factor Predisposing to an Increased Risk of Implant Failure
4.3. Negative Influence of Clindamycin on Osseointegration
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Howe, M.-S.; Keys, W.; Richards, D. Long-term (10-year) dental implant survival: A systematic review and sensitivity meta-analysis. J. Dent. 2019, 84, 9–21. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Reasons for failures of oral implants. J. Oral Rehabil. 2014, 41, 443–476. [Google Scholar] [CrossRef]
- Chrcanovic, B.; Kisch, J.; Albrektsson, T.; Wennerberg, A. Factors influencing early dental implant failures. J. Dent. Res. 2016, 95, 995–1002. [Google Scholar] [CrossRef]
- Baqain, Z.H.; Moqbel, W.; Sawair, F.A. Early dental implant failure: Risk factors. Br. J. Oral Maxillofac. Surg. 2012, 50, 239–243. [Google Scholar] [CrossRef]
- Giannobile, W.V.; Lang, N.P. Are dental implants a panacea or should we better strive to save teeth? J. Dent. Res. 2016, 95, 5–6. [Google Scholar] [CrossRef] [Green Version]
- Adell, R.; Lekholm, U.; Rockler, B.; Branemark, P.I. A 15-year study of osseointegrated implants in the treatment of the edentulous jaw. Int. J. Oral Surg. 1981, 10, 387–416. [Google Scholar] [CrossRef]
- Smith, A.J.; Jackson, M.S.; Bagg, J. The ecology of Staphylococcus species in the oral cavity. J. Med. Microbiol. 2001, 50, 940–946. [Google Scholar] [CrossRef]
- Benítez-Páez, A.; Belda-Ferre, P.; Simón-Soro, A.; Mira, A. Microbiota diversity and gene expression dynamics in human oral biofilms. BMC Genom. 2014, 15, 311. [Google Scholar] [CrossRef]
- Salgado-Peralvo, A.-O.; Kewalramani, N.; Peña-Cardelles, J.F.; Mateos-Moreno, M.V.; Monsalve-Guil, L.; Jiménez-Guerra, Á.; Ortiz-García, I.; Velasco-Ortega, E. Preventive Antibiotic Prescribing Habits among Professionals Dedicated to Oral Implantology: An Observational Study. Antibiotics 2021, 10, 301. [Google Scholar] [CrossRef]
- Canadian Dental Association. CDA Position on the Prevention of Infective Endocarditis; Canadian Dental Association: Ottawa, ON, Canada, 2014. [Google Scholar]
- Lee, J.W.; Lee, J.Y.; Kim, S.M.; Kim, M.J.; Lee, J.H. Prophylactic antibiotics in intra-oral bone grafting procedures: A prospective, randomized, double-blind clinical trial. J. Korean Assoc. Oral Maxillofac. Surg. 2012, 38, 90–95. [Google Scholar] [CrossRef] [Green Version]
- Bhattacharya, S. The facts about penicillin allergy: A review. J. Adv. Pharm. Technol. Res. 2010, 1, 11–17. [Google Scholar]
- Wilson, W.R.; Gewitz, M.; Lockhart, P.B.; Bolger, A.F.; DeSimone, D.C.; Kazi, D.S.; Couper, D.J.; Beaton, A.; Kilmartin, C.; Miro, J.M.; et al. Prevention of Viridans Group Streptococcal Infective Endocarditis: A Scientific Statement From the American Heart Association. Circulation 2021, 143, 963–978. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Joanna Briggs Institute. Checklist for Systematic Reviews and Research Syntheses; Joanna Briggs Institute: Adelaide, Australia, 2017. [Google Scholar]
- Salomo-Coll, O.; Lozano-Carrascal, N.; Lazaro-Abdulkarim, A.; Hernandez-Alfaro, F.; Gargallo-Albiol, J.; Satorres-Nieto, M. Do Penicillin-Allergic Patients Present a Higher Rate of Implant Failure? Int. J. Oral Maxillofac. Implants 2018, 33, 1390–1395. [Google Scholar] [CrossRef]
- French, D.; Noroozi, M.; Shariati, B.; Larjava, H. Clinical retrospective study of self-reported penicillin allergy on dental implant failures and infections. Quintessence Int. 2016, 47, 861–870. [Google Scholar] [CrossRef]
- Wagenberg, B.; Froum, S.J. A retrospective study of 1925 consecutively placed immediate implants from 1988 to 2004. Int. J. Oral Maxillofac. Implants 2006, 21, 71–80. [Google Scholar]
- French, D.; Larjava, H.; Ofec, R. Retrospective cohort study of 4591 Straumann implants in private practice setting, with up to 10-year follow-up. Part 1: Multivariate survival analysis. Clin. Oral Implants Res. 2015, 26, 1345–1354. [Google Scholar] [CrossRef]
- Block, M.S.; Christensen, B.J.; Mercante, D.E.; Chapple, A.G. What Factors Are Associated With Implant Failure? J. Oral Maxillofac. Surg. 2021, 79, 91–97. [Google Scholar] [CrossRef]
- Inglis, J.M.; Caughey, G.E.; Smith, W.; Shakib, S. Documentation of penicillin adverse drug reactions in electronic health records: Inconsistent use of allergy and intolerance labels. Intern. Med. J. 2017, 47, 1292–1297. [Google Scholar] [CrossRef]
- MacFadden, D.R.; LaDelfa, A.; Leen, J.; Gold, W.L.; Daneman, N.; Weber, E.; Al-Busaidi, I.; Petrescu, D.; Saltzman, I.; Devlin, M.; et al. Impact of reported beta-lactam allergy on inpatient outcomes: A multicenter prospective cohort study. Clin. Infect. Dis. 2016, 63, 904–910. [Google Scholar] [CrossRef]
- Trubiano, J.A.; Adkinson, N.F.; Phillips, E.J. Penicillin allergy is not necessarily forever. JAMA 2017, 318, 82–83. [Google Scholar] [CrossRef] [PubMed]
- Bourke, J.; Pavlos, R.; James, I.; Phillips, E. Improving the effectiveness of penicillin allergy de-labeling. J. Allergy Clin. Immunol. Pract. 2015, 3, 365–374. [Google Scholar] [CrossRef] [PubMed]
- McDanel, D.L.; Azar, A.E.; Dowden, A.M.; Murray-Bainer, S.; Noiseux, N.O.; Willenborg, M.; Clark, C.R.; Callaghan, J.J.; Haleem, A. Screening for beta-lactam allergy in joint arthroplasty patients to improve surgical prophylaxis practice. J. Arthroplast. 2017, 32, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Trubiano, J.A.; Thursky, K.A.; Stewardson, A.J.; Urbancic, K.; Worth, L.J.; Jackson, C.; Stevenson, W.; Sutherland, M.; Slavin, M.A.; Grayson, M.L.; et al. Impact of an Integrated Antibiotic Allergy Testing Program on antimicrobial stewardship: A multicenter evaluation. Clin. Infect. Dis. 2017, 65, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Khoury, F.; Javed, F.; Romanos, G.E. Sinus augmentation failure and postoperative infections associated with prophylactic clindamycin therapy: An observational case series. Int. J. Oral Maxillofac. Implants 2018, 33, 1136–1139. [Google Scholar] [CrossRef]
- Wagenberg, B.D.; Froum, S.J.; Eckert, S.E. Long-term bone stability assessment around 1187 immediately placed implants with 1-to 22-year follow-up. Int. J. Oral Maxillofac. Implants 2013, 28, 605–612. [Google Scholar] [CrossRef] [Green Version]
- Wagenberg, B.; Froum, S.J. A Retrospective Study of Bone Level Stability Around 441 Mandibular and 350 Maxillary Molar Implants Placed with an Immediate Implant Protocol. Int. J. Periodontics Restor. Dent. 2020, 40, 635–643. [Google Scholar] [CrossRef]
- Froum, S.J.; Rosen, P.S.; Wang, W.C.; Froum, S.H.; Vinayak, S. Retrospective Evaluation of Factors Related to the Outcomes of Regenerative Therapy for Implants Affected by Peri-implantitis. Int. J. Periodontics Restor. Dent. 2018, 38, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Basma, H.S.; Misch, C.M. Extraction Socket Grafting and Ridge Augmentation Failures Associated with Clindamycin Antibiotic Therapy: A Retrospective Study. Int. J. Oral Maxillofac. Implants 2021, 36, 122–125. [Google Scholar] [CrossRef]
- Cosyn, J.; De Lat, L.; Seyssens, L.; Doornewaard, R.; Deschepper, E.; Vervaeke, S. The effectiveness of immediate implant placement for single tooth replacement compared to delayed implant placement: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 224–241. [Google Scholar] [CrossRef] [Green Version]
- Wyles, C.C.; Hevesi, M.; Osmon, D.R.; Park, M.A.; Habermann, E.B.; Lewallen, D.G.; Berry, D.J.; Sierra, R.J. 2019 John Charnley Award: Increased risk of prosthetic joint infection following primary total knee and hip arthroplasty with the use of alternative antibiotics to cefazolin: The value of allergy testing for antibiotic prophylaxis. Bone Joint J. 2019, 101, 9–15. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Lu, N.; Zhang, Y.; Li, Y.; Walensky, R.P.; Choi, H.K. Risk of meticillin resistant Staphylococcus aureus and Clostridium difficile in patients with a documented penicillin allergy: Population based matched cohort study. BMJ 2018, 361, k2400. [Google Scholar] [CrossRef] [Green Version]
- Kheir, M.M.; Tan, T.L.; Azboy, I.; Tan, D.D.; Parvizi, J. Vancomycin Prophylaxis for Total Joint Arthroplasty: Incorrectly Dosed and Has a Higher Rate of Periprosthetic Infection Than Cefazolin. Clin. Orthop. Relat. Res. 2017, 475, 1767–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, T.L.; Springer, B.D.; Ruder, J.A.; Ruffolo, M.R.; Chen, A.F. Is Vancomycin-only Prophylaxis for Patients With Penicillin Allergy Associated With Increased Risk of Infection After Arthroplasty? Clin. Orthop. Relat. Res. 2016, 474, 1601–1606. [Google Scholar] [CrossRef]
- Rashid, M.; Weintraub, A.; Nord, C. Development of antimicrobial resistance in the normal anaerobic microbiota during one year after administration of clindamycin or ciprofloxacin. Anaerobe 2015, 31, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Lafaurie, G.I.; Sabogal, M.A.; Castillo, D.M.; Rincón, M.V.; Gómez, L.A.; Lesmes, Y.A.; Chambrone, L. Microbiome and Microbial Biofilm Profiles of Peri-Implantitis: A Systematic Review. J. Periodontol. 2017, 88, 1066–1089. [Google Scholar] [CrossRef] [PubMed]
- Rams, T.E.; Balkin, B.E.; Roberts, T.W.; Molzan, A.K. Microbiological aspects of human mandibular subperiosteal dental implants. J. Oral Implantol. 2013, 39, 714–722. [Google Scholar] [CrossRef] [PubMed]
- Persson, G.R.; Renvert, S. Cluster of bacteria associated with peri-implantitis. Clin. Implant Dent. Relat. Res. 2014, 16, 783–793. [Google Scholar] [CrossRef]
- Salvi, G.E.; Fürst, M.M.; Lang, N.P.; Persson, G.R. One-year bacterial colonization patterns of Staphylococcus aureus and other bacteria at implants and adjacent teeth. Clin. Oral Implants Res. 2008, 19, 242–248. [Google Scholar] [CrossRef]
- Charalampakis, G.; Leonhardt, Å.; Rabe, P.; Dahlén, G. Clinical and microbiological characteristics of peri-implantitis cases: A retrospective multicentre study. Clin. Oral Implants Res. 2012, 23, 1045–1054. [Google Scholar] [CrossRef]
- Leonhardt, A.; Dahlén, G.; Renvert, S. Five-year clinical, microbiological, and radiological outcome following treatment of peri-implantitis in man. J. Periodontol. 2003, 74, 1415–1422. [Google Scholar] [CrossRef]
- Zirk, M.; Dreiseidler, T.; Pohl, M.; Rothamel, D.; Buller, J.; Peters, F.; Zöller, J.E.; Kreppel, M. Odontogenic sinusitis maxillaris: A retrospective study of 121 cases with surgical intervention. J. Cranio Maxillofac. Surg. 2017, 45, 520–525. [Google Scholar] [CrossRef]
- Rosenfeld, R.M.; Piccirillo, J.F.; Chandrasekhar, S.S.; Brook, I.; Ashok Kumar, K.; Kramper, M.; Orlandi, R.R.; Palmer, J.N.; Patel, Z.M.; Peters, A.; et al. Clinical practice guideline (update): Adult sinusitis. Otolaryngol. Head Neck Surg. 2015, 152, 1–39. [Google Scholar] [CrossRef] [Green Version]
- Pigrau, C.; Almirante, B.; Rodriguez, D.; Larrosa, N.; Bescos, S.; Raspall, G.; Pahissa, A. Osteomyelitis of the jaw: Resistance to clindamycin in patients with prior antibiotics exposure. Eur. J. Clin. Microbiol. Infect. Dis. 2009, 28, 317–323. [Google Scholar] [CrossRef]
- Krebs, K.; Bovijn, J.; Zheng, N.; Lepamets, M.; Censin, J.C.; Jürgenson, T.; Särg, D.; Abner, E.; Laisk, T.; Luo, Y.; et al. Genome-wide Study Identifies Association between HLA-B(∗)55:01 and Self-Reported Penicillin Allergy. Am. J. Hum. Genet. 2020, 107, 612–621. [Google Scholar] [CrossRef]
- Raslan, H.M.; Attia, H.R.; Salama, I.; Ibrahim, M.H.; Hassan, E.M.; El Hussieny, M.S.; El Menyawi, M.M.; Amr, K.S. Association of PTPN22 1858C→T polymorphism, HLA-DRB1 shared epitope and autoantibodies with rheumatoid arthritis. Rheumatol. Int. 2016, 36, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Bossini-Castillo, L.; de Kovel, C.; Kallberg, H.; van ’t Slot, R.; Italiaander, A.; Coenen, M.; Tak, P.P.; Posthumus, M.D.; Wijmenga, C.; Huizinga, T.; et al. A genome-wide association study of rheumatoid arthritis without antibodies against citrullinated peptides. Ann. Rheum. Dis. 2015, 74, e15. [Google Scholar] [CrossRef] [Green Version]
- Nagy, R.; Szabo, K.; Szucs, A.; Ruszin, T.; Joob-Fancsaly, A. Impact of rheumatoid arthritis in oral surgery and implantology treatment based on literature. Fogorv. Szle. 2017, 110, 3–6. [Google Scholar]
- Naal, F.D.; Salzmann, G.M.; von Knoch, F.; Tuebel, J.; Diehl, P.; Gradinger, R.; Schauwecker, J. The effects of clindamycin on human osteoblasts in vitro. Arch. Orthop. Trauma Surg. 2008, 128, 317–323. [Google Scholar] [CrossRef] [PubMed]
- Duewelhenke, N.; Krut, O.; Eysel, P. Influence on mitochondria and cytotoxicity of different antibiotics administered in high concentrations on primary human osteoblasts and cell lines. Antimicrob. Agents Chemother. 2007, 51, 54–63. [Google Scholar] [CrossRef] [Green Version]
- Romandini, M.; De Tullio, I.; Congedi, F.; Kalemaj, Z.; D’Ambrosio, M.; Lafori, A.; Quaranta, C.; Buti, J.; Perfetti, G. Antibiotic prophylaxis at dental implant placement: Which is the best protocol? A systematic review and network meta-analysis. J. Clin. Periodontol. 2019, 46, 382–395. [Google Scholar] [CrossRef] [PubMed]
- Salgado-Peralvo, A.-O.; Mateos-Moreno, M.V.; Velasco-Ortega, E.; Peña-Cardelles, J.F.; Kewalramani, N. Preventive antibiotic therapy in Bone Augmentation Procedures in Oral Implantology: A systematic review. J. Stomatol. Oral Maxillofac. Surg. 2021, 22. [Google Scholar] [CrossRef]


{kind=link}
| Component | Description |
|---|---|
| P (problem/population) | DI 1 failure |
| I (intervention) | Prescription of antibiotics other than penicillin |
| C (comparison) | Comparison between patients with/without allergy to penicillin |
| O (outcome) | Prevention of DI failure |
| PICO question | In penicillin-allergic patients who are not prescribed these antibiotics, is there an increased risk of DI failure compared to non-allergic patients? |
| Author(s)/ Year | Allergy Confirmation | Procedure | N 1/DI 2 | Failure Rates (at Implant Level) | Antibiotics Used | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| NA 3 | A 4 | NA | A | RI 5 | p6 (95%) | NA | A | |||
| Salomó-Coll et al. [16] (2018) | SRPA 7 | Ordinary implants in healthy patients | 1133/2572 | 77/175 | 8.03% | 24.68% | RR 8 3.84 | 0.032 | Amoxicillin 2g 9, 1h PreOp + 750 mg 10/8h 11/7d 12 PostOp | Clindamycin 600 mg, 1h PreOp + 300 mg/6h/7d PostOp |
| French et al. [17] (2016) | SRPA | Various types: ordinary implants, with simultaneous GBR 13, immediate and sinus lifts ASA I or II patients | UNS 14/5106 | UNS 14/470 | 0.80% | 2.10% | OR 3.10 | 0.002 | Amoxicillin 2 g, 1h PreOp + 500 mg at 8h PostOp (If bone-grafting, immediate implant or sinus lift: 250 mg/8h/7d) | Clindamycin 600 mg/1h PreOp (If bone-grafting or immediate implant 150 mg/6h/7d. If sinus lift: levofloxacin 250 mg/12h/7d) |
| French et al. [19] (2015) | Preliminary test | Placement of implants in native bone with or without GBR, immediate implants and sinus lifts | 1898/UNS 14 | 162/UNS 14 | UNS 14 | UNS 14 | HR 2.16 | 0.11 | Amoxicillin (UNS 14 guidelines) | Clindamycin (UNS 14 guidelines) |
| Wagenberg and Froum [18] (2006) | SRPA | Placement of immediate implants, some with sinus lift and some with immediate loading | UNS 14/1561 | UNS 14/364 | 2.95% | 8.52% | RR 3.34 | <0.001 | Amoxicillin 500 mg/6h/2d PreOp + 10d PostOp | Clindamycin 300 mg/6h/2d PreOp + 10d PostOp |
| Block et al. [20] (2021) | Salomó-Coll et al. [16] (2018) | French et al. [17] (2016) | French et al. [19] (2015) | Wagenberg and Froum [18] (2006) | |
|---|---|---|---|---|---|
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
|  |  |  |  |  |
 Yes;
Yes;  No;
No;  Unclear;
Unclear;  Not applicable.
Not applicable.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salgado-Peralvo, A.-O.; Peña-Cardelles, J.-F.; Kewalramani, N.; Ortiz-García, I.; Jiménez-Guerra, Á.; Uribarri, A.; Velasco-Ortega, E.; Moreno-Muñoz, J.; Núñez-Márquez, E.; Monsalve-Guil, L. Is Penicillin Allergy a Risk Factor for Early Dental Implant Failure? A Systematic Review. Antibiotics 2021, 10, 1227. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101227
Salgado-Peralvo A-O, Peña-Cardelles J-F, Kewalramani N, Ortiz-García I, Jiménez-Guerra Á, Uribarri A, Velasco-Ortega E, Moreno-Muñoz J, Núñez-Márquez E, Monsalve-Guil L. Is Penicillin Allergy a Risk Factor for Early Dental Implant Failure? A Systematic Review. Antibiotics. 2021; 10(10):1227. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101227
Chicago/Turabian StyleSalgado-Peralvo, Angel-Orión, Juan-Francisco Peña-Cardelles, Naresh Kewalramani, Iván Ortiz-García, Álvaro Jiménez-Guerra, Andrea Uribarri, Eugenio Velasco-Ortega, Jesús Moreno-Muñoz, Enrique Núñez-Márquez, and Loreto Monsalve-Guil. 2021. "Is Penicillin Allergy a Risk Factor for Early Dental Implant Failure? A Systematic Review" Antibiotics 10, no. 10: 1227. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101227