
Population Pharmacokinetic Modeling and Dose Optimization of Vancomycin in Chinese Patients with Augmented Renal Clearance


Abstract
:1. Introduction
2. Results
2.1. Patients and Data Collection
2.2. Population Modeling
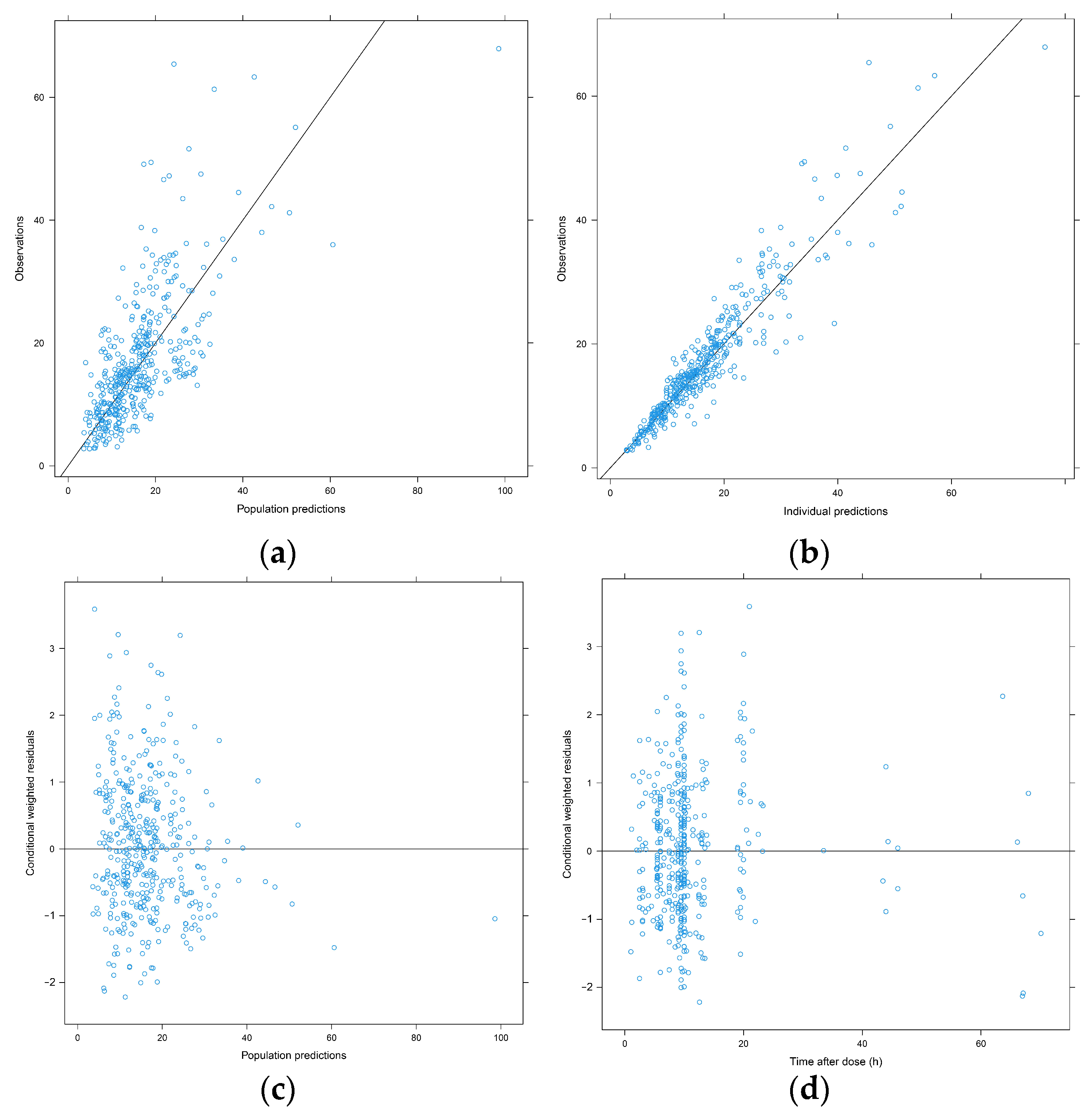
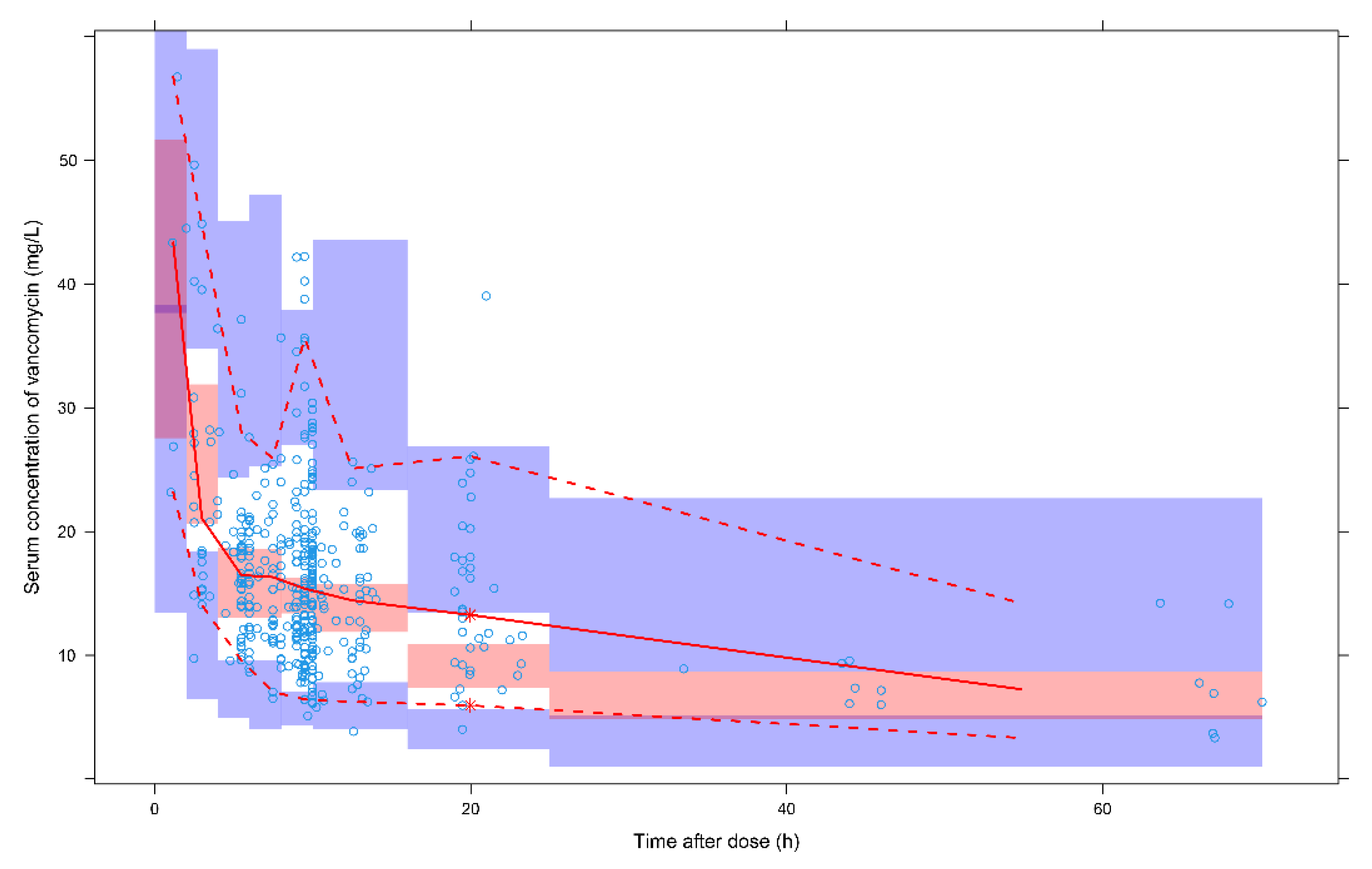
2.3. Model Evaluation
2.4. Dosage Recommendation
3. Discussion
4. Materials and Methods
4.1. Patients and Data Collection
4.2. Evaluation of Serum Vancomycin Concentration
4.3. Population Pharmacokinetic Modeling
4.4. Model Validation
4.5. Simulation and Dose Optimization
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Levine, D.P. Vancomycin: A history. Clin. Infect. Dis. 2006, 42, S5–S12. [Google Scholar] [CrossRef]
- Geraci, J.E.; Heilman, F.R.; Nichols, D.R.; Ross, G.T.; Wellman, W.E. Some laboratory and clinical experiences with a new antibiotic, vancomycin. Proc. Staff Meet. Mayo Clin. 1956, 31, 564–582. [Google Scholar] [PubMed]
- Spadaro, S.; Berselli, A.; Fogagnolo, A.; Capuzzo, M.; Ragazzi, R.; Marangoni, E.; Bertacchini, S.; Volta, C.A. Evaluation of a protocol for vancomycin administration in critically patients with and without kidney dysfunction. BMC Anesth. 2015, 15, 95. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, J.; Yang, Z.T.; Qian, X.; Zhao, B.; Mao, E.Q.; Chen, E.Z.; Bian, X.L. A higher dose of vancomycin is needed in critically ill patients with augmented renal clearance. Transl. Androl. Urol. 2020, 9, 2166–2171. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.; Zhang, B.; Liu, Y.; Tang, J.; Dong, D.; Gu, Q. Clinical study of vancomycin for appropriate dosing in severe infective patients with augmented renal clearance. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2018, 30, 646–651. [Google Scholar] [CrossRef]
- He, C.Y.; Qin, Y.R.; Liu, C.J.; Ren, J.; Fan, J.S. Effect of augmented renal clearance on plasma concentration of vancomycin and treatment outcome in children with methicillin-resistant Staphylococcus aureus infection. Zhongguo Dang Dai Er Ke Za Zhi 2019, 21, 904–909. [Google Scholar] [PubMed]
- Lodise, T.P.; Drusano, G.L.; Zasowski, E.; Dihmess, A.; Lazariu, V.; Cosler, L.; McNutt, L.A. Vancomycin exposure in patients with methicillin-resistant Staphylococcus aureus bloodstream infections: How much is enough? Clin. Infect. Dis. 2014, 59, 666–675. [Google Scholar] [CrossRef] [Green Version]
- Claus, B.O.; Hoste, E.A.; Colpaert, K.; Robays, H.; Decruyenaere, J.; De Waele, J.J. Augmented renal clearance is a common finding with worse clinical outcome in critically ill patients receiving antimicrobial therapy. J. Crit. Care 2013, 28, 695–700. [Google Scholar] [CrossRef]
- Liu, T.T.; Pang, H.M.; Jing, L.; Wei, W.X.; Qin, X.L.; Guo, Q.; Lu, H.; Cheng, D.H.; Jiang, W.Z. A population pharmacokinetic model of vancomycin for dose individualization based on serum cystatin C as a marker of renal function. J. Pharm. Pharmacol. 2019, 71, 945–955. [Google Scholar] [CrossRef]
- Pitaksontayothin, K.; Santimaleeworagun, W.; Pongchaidecha, M.; Houngsaitong, J.; Srisena, P. The use of monte carlo simulation to predict vancomycin dosage for methicillin-resistant staphylococcus aureus in Thai patients of various ages and with varying degrees of renal function. Asian Biomed. 2017, 11, 379–385. [Google Scholar] [CrossRef] [Green Version]
- Deng, C.; Liu, T.; Zhou, T.; Lu, H.; Cheng, D.; Zhong, X.; Lu, W. Initial dosage regimens of vancomycin for Chinese adult patients based on population pharmacokinetic analysis. Int. J. Clin. Pharmacol. Ther. 2013, 51, 407–415. [Google Scholar] [CrossRef] [PubMed]
- Thomson, A.H.; Staatz, C.E.; Tobin, C.M.; Gall, M.; Lovering, A.M. Development and evaluation of vancomycin dosage guidelines designed to achieve new target concentrations. J. Antimicrob. Chemother. 2009, 63, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Dolton, M.; Xu, H.; Cheong, E.; Maitz, P.; Kennedy, P.; Gottlieb, T.; Buono, E.; McLachlan, A.J. Vancomycin pharmacokinetics in patients with severe burn injuries. Burns 2010, 36, 469–476. [Google Scholar] [CrossRef]
- Sanchez, J.L.; Dominguez, A.R.; Lane, J.R.; Anderson, P.O.; Capparelli, E.V.; Cornejo-Bravo, J.M. Population pharmacokinetics of vancomycin in adult and geriatric patients: Comparison of eleven approaches. Int. J. Clin. Pharmacol. Ther. 2010, 48, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Aiba, T.; Otsuka, T.; Suemaru, K.; Nishimiya, T.; Inoue, T.; Murase, M.; Kurosaki, Y.; Araki, H. Population pharmacokinetic analysis of vancomycin using serum cystatin C as a marker of renal function. Antimicrob. Agents Chemother. 2010, 54, 778–782. [Google Scholar] [CrossRef] [Green Version]
- Chu, Y.; Luo, Y.; Qu, L.; Zhao, C.; Jiang, M. Application of vancomycin in patients with varying renal function, especially those with augmented renal clearance. Pharm. Biol. 2016, 54, 2802–2806. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, J.F.; Hahn, S.R.; Goncalves, J.; Fresco, P. Vancomycin therapeutic drug monitoring and population pharmacokinetic models in special patient subpopulations. Pharmacol. Res. Perspect. 2018, 6, e420. [Google Scholar] [CrossRef]
- Chen, Y.; Liu, L.; Zhu, M. Effect of augmented renal clearance on the therapeutic drug monitoring of vancomycin in patients after neurosurgery. J. Int. Med. Res. 2020, 48, 1220748628. [Google Scholar] [CrossRef]
- He, J.; Mao, E.; Jing, F.; Jiang, H.; Xu, W.; Yang, W.; Chen, E. PK/PD of vancomycin in patients with severe acute pancreatitis combined with augmented renal clearance. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2017, 29, 810–814. [Google Scholar] [CrossRef]
- Chu, Y.; Luo, Y.; Ji, S.; Jiang, M.; Zhou, B. Population pharmacokinetics of vancomycin in Chinese patients with augmented renal clearance. J. Infect. Public Health 2020, 13, 68–74. [Google Scholar] [CrossRef]
- Roberts, J.A.; Taccone, F.S.; Udy, A.A.; Vincent, J.L.; Jacobs, F.; Lipman, J. Vancomycin dosing in critically ill patients: Robust methods for improved continuous-infusion regimens. Antimicrob. Agents Chemother. 2011, 55, 2704–2709. [Google Scholar] [CrossRef] [Green Version]
- Del, M.F.D.G.; Revilla, N.; Calvo, M.V.; Dominguez-Gil, A.; Sanchez, N.A. Pharmacokinetic/pharmacodynamic analysis of vancomycin in ICU patients. Intensive Care Med. 2007, 33, 279–285. [Google Scholar] [CrossRef]
- Llopis-Salvia, P.; Jimenez-Torres, N.V. Population pharmacokinetic parameters of vancomycin in critically ill patients. J. Clin. Pharm. Ther. 2006, 31, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Niederman, M.S.; Baron, R.M.; Bouadma, L.; Calandra, T.; Daneman, N.; DeWaele, J.; Kollef, M.H.; Lipman, J.; Nair, G.B. Initial antimicrobial management of sepsis. Crit. Care 2021, 25, 307. [Google Scholar] [CrossRef] [PubMed]
- Povoa, P.; Moniz, P.; Pereira, J.G.; Coelho, L. Optimizing Antimicrobial Drug Dosing in Critically Ill Patients. Microorganisms 2021, 9, 1401. [Google Scholar] [CrossRef] [PubMed]
- De Paepe, P.; Belpaire, F.M.; Buylaert, W.A. Pharmacokinetic and pharmacodynamic considerations when treating patients with sepsis and septic shock. Clin. Pharmacokinet. 2002, 41, 1135–1151. [Google Scholar] [CrossRef] [PubMed]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Societe Francaise de Pharmacologie et Therapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Societe Francaise d’Anesthesie et Reanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Backer, D.; Cecconi, M.; Lipman, J.; Machado, F.; Myatra, S.N.; Ostermann, M.; Perner, A.; Teboul, J.L.; Vincent, J.L.; Walley, K.R. Challenges in the management of septic shock: A narrative review. Intensive Care Med. 2019, 45, 420–433. [Google Scholar] [CrossRef]
- Roberts, J.A.; Abdul-Aziz, M.H.; Lipman, J.; Mouton, J.W.; Vinks, A.A.; Felton, T.W.; Hope, W.W.; Farkas, A.; Neely, M.N.; Schentag, J.J.; et al. Individualised antibiotic dosing for patients who are critically ill: Challenges and potential solutions. Lancet Infect. Dis. 2014, 14, 498–509. [Google Scholar] [CrossRef] [Green Version]
- Okada, A.; Kariya, M.; Irie, K.; Okada, Y.; Hiramoto, N.; Hashimoto, H.; Kajioka, R.; Maruyama, C.; Kasai, H.; Hamori, M.; et al. Population Pharmacokinetics of Vancomycin in Patients Undergoing Allogeneic Hematopoietic Stem-Cell Transplantation. J. Clin. Pharmacol. 2018, 58, 1140–1149. [Google Scholar] [CrossRef]
- Finch, N.A.; Zasowski, E.J.; Murray, K.P.; Mynatt, R.P.; Zhao, J.J.; Yost, R.; Pogue, J.M.; Rybak, M.J. A Quasi-Experiment To Study the Impact of Vancomycin Area under the Concentration-Time Curve-Guided Dosing on Vancomycin-Associated Nephrotoxicity. Antimicrob. Agents Chemother. 2017, 61, e01293-17. [Google Scholar] [CrossRef] [Green Version]
- Rybak, M.J.; Le, J.; Lodise, T.; Levine, D.; Bradley, J.; Liu, C.; Mueller, B.; Pai, M.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Executive Summary: Therapeutic Monitoring of Vancomycin for Serious Methicillin-Resistant Staphylococcus aureus Infections: A Revised Consensus Guideline and Review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. J. Pediatr. Infect. Dis. Soc. 2020, 9, 281–284. [Google Scholar] [CrossRef] [PubMed]
- Men, P.; Li, H.B.; Zhai, S.D.; Zhao, R.S. Association between the AUC0-24/MIC Ratio of Vancomycin and Its Clinical Effectiveness: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e146224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aljefri, D.M.; Avedissian, S.N.; Rhodes, N.J.; Postelnick, M.J.; Nguyen, K.; Scheetz, M.H. Vancomycin Area Under the Curve and Acute Kidney Injury: A Meta-analysis. Clin. Infect. Dis. 2019, 69, 1881–1887. [Google Scholar] [CrossRef] [PubMed]
- He, N.; Su, S.; Ye, Z.; Du, G.; He, B.; Li, D.; Liu, Y.; Yang, K.; Zhang, X.; Zhang, Y.; et al. Evidence-based Guideline for Therapeutic Drug Monitoring of Vancomycin: 2020 Update by the Division of Therapeutic Drug Monitoring, Chinese Pharmacological Society. Clin. Infect. Dis. 2020, 71, S363–S371. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Patients (N = 209) |
|---|---|
| Male, n (%) | 126 (60.3%) |
| ICU, n (%) | 82 (39.2%) |
| CLcr ≥ 130 mL/min, n (%) | 51 (24.4%) |
| Shock, n (%) | 39 (18.7%) |
| MOF, n (%) | 7 (3.3%) |
| Age, years (mean ± SD) | 66.0 ± 16.4 |
| TBW, kg (mean ± SD) | 63.4 ± 12.9 |
| Mean CLcr a, mL/min (median (range)) | 86.7 (18.4–390.7) |
| Number of samples, n | 424 |
| Number of samples per patient, n (%) | |
| 1 | 103 (49.3%) |
| 2 | 50 (23.9%) |
| 3 | 29 (13.9%) |
| ≥4 | 27 (12.9%) |
| Mean daily dosage, mg (median (IQR)) | 1875.0 (1461.9–2352.0) |
| Number of samples collected after the start of infusion, n (%) | |
| <3 h | 25 (5.9%) |
| 3–5 h | 16 (3.8%) |
| 5–12 h | 294 (69.3%) |
| 12–24 h | 75 (17.7%) |
| >24 h | 14 (3.3%) |
| Mean concentration after the start of infusion, mg/L | |
| <3 h | 29.5 |
| 3–5 h | 22.9 |
| 5–12 h | 16.5 |
| 12–24 h | 15.3 |
| >24 h | 10.3 |
| Parameter | Base Model Estimate (RSE%) | Final Model Estimate (RSE%) | Bootstrap Median (95% CI) |
|---|---|---|---|
| CL (L/h) | 2.56(7%) | - | - |
| CLmax (L/h) | - | 5.58 (17%) | 5.58 (4.26–8.52) |
| CGCLmax50 (L/h) | - | 93.8 (24%) | 94.65 (66.99–178.63) |
| s | - | 1.5 (14%) | 1.49 (1.16–1.95) |
| Vc (L) | 13.1 (11%) | - | - |
| Vc non-ICU (L) | - | 8.02 (12%) | 7.90 (4.90–11.80) |
| Vc ICU (L) | - | 35.7 (13%) | 36.66 (26.68–48.37) |
| Q (L/h) | 4.9 (26%) | 2.66 (12%) | 2.64 (1.80–3.58) |
| Vp (L) | 40.2 (13%) | 36.8 (15%) | 36.26 (25.51–49.36) |
| IIV CL | 0.319 (12%) | 0.0771 (16%) | 0.075 (0.05–0.10) |
| IIV Vc | 1.65 (39%) | 0.223 (56%) | 0.20 (0.0039–0.53) |
| Additive residual error | 0.0479 (18%) | 0.0466 (14%) | 0.045 (0.032–0.060) |
| CLcr (mL/min) | Dosage | PTA (%) |
|---|---|---|
| 15–29 | 250 mg Q24 h | 41.44 |
| 30–44 | 500 mg Q24 h | 53.69 |
| 45–59 | 750 mg Q24 h | 57.64 |
| 60–89 | 1250 mg Q24 h | 57.32 |
| 90–119 | 750 mg Q12 h | 61.58 |
| 120–149 | 1750 mg Q24 h | 62.33 |
| 150–179 | 1000 mg Q12 h | 62.56 |
| ≥180 | 750 mg Q8 h | 61.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, S.; He, N.; Zhang, Y.; Wang, C.; Zhai, S.; Zhang, C. Population Pharmacokinetic Modeling and Dose Optimization of Vancomycin in Chinese Patients with Augmented Renal Clearance. Antibiotics 2021, 10, 1238. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101238
Zhao S, He N, Zhang Y, Wang C, Zhai S, Zhang C. Population Pharmacokinetic Modeling and Dose Optimization of Vancomycin in Chinese Patients with Augmented Renal Clearance. Antibiotics. 2021; 10(10):1238. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101238
Chicago/Turabian StyleZhao, Sixuan, Na He, Yahui Zhang, Chuhui Wang, Suodi Zhai, and Chao Zhang. 2021. "Population Pharmacokinetic Modeling and Dose Optimization of Vancomycin in Chinese Patients with Augmented Renal Clearance" Antibiotics 10, no. 10: 1238. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10101238