
Clinically Relevant Interactions with Anti-Infectives on Intensive Care Units—A Multicenter Delphi Study

 , ,
, ,
Abstract
:1. Introduction
2. Results
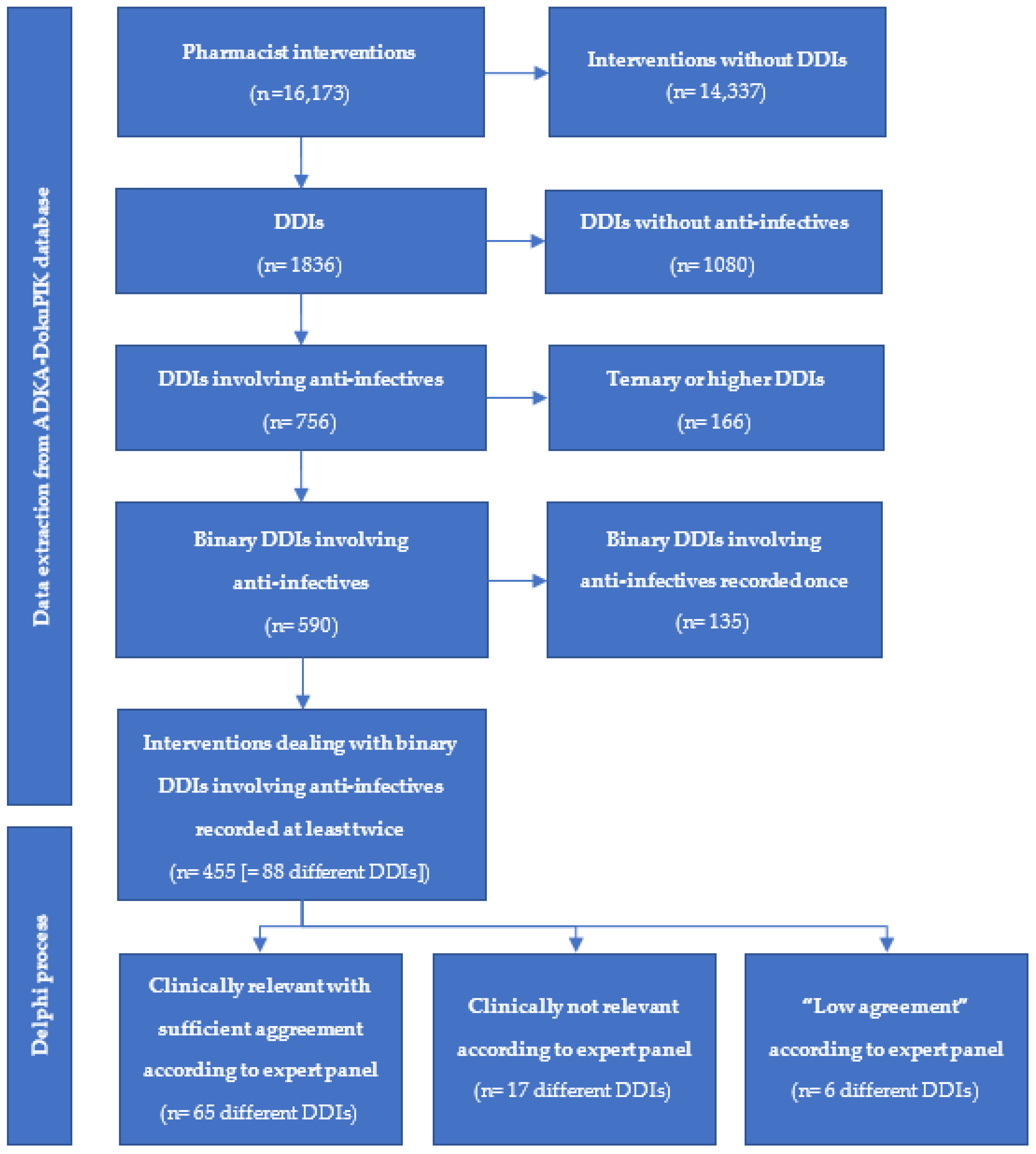
2.1. Drug–Drug Interactions from the ADKA-DokuPIK Database
2.2. Ratings of the Expert Panel within the Modified Two-Step Delphi Process
2.3. Interaction Fact Sheets
2.3.1. Cephalosporins
Ceftriaxone and Calcium-Containing Intravenous Solutions
2.3.2. Carbapenems
Carbapenems and Valproic Acid
2.3.3. Fluoroquinolones
Fluoroquinolones and QTc Prolonging Drugs
Fluoroquinolones and Polyvalent Cations or Simvastatin
2.3.4. Macrolides
Macrolides and CYP 3A4 Substrates
Macrolides and Antidepressants or Antipsychotics
2.3.5. Antifungals
Echinocandins
Azole Antifungals
2.3.6. Miscellaneous Anti-Infectives
Daptomycin
Rifampicin
Linezolid and Serotonergic Agents
3. Discussion
4. Materials and Methods
4.1. Expert Panel and Modified Two-Step Delphi Process
- Mode category 1: “Not clinically relevant, since adverse effects of this DDI are negligible”.
- Mode category 2: “Clinically relevant; the adverse effects of this DDI will, however, be limited since routine monitoring to timely identify adverse effects is present”.
- Mode category 3: “Clinically relevant; the adverse effects of this DDI can, however, be limited by additional monitoring and/or changes in dosage/frequency/timing”.
- Mode category 4: “Clinically relevant, the adverse effects of this DDI on the patient can be substantial; however, these effects are acceptable and treatable”.
- Mode category 5: “Clinically relevant; the adverse effect of this DDI on the patient should preferably be avoided”.
- Are both drugs indispensable for the individual patient?
- Is there a therapeutic alternative available for one of the drugs?
- Is there any feasible monitoring available to early identify AE?
4.2. Interaction Fact Sheets
4.3. Data Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Plaza, J.; Alamo, M.; Torres, P.; Fuentes, A.; López, F. Drug interactions and adverse events induced by drugs used in an intensive care unit. Revista Medica de Chile 2010, 138, 452–460. [Google Scholar]
- Cvikl, M.; Sinkovič, A. Interventions of a clinical pharmacist in a medical intensive care unit—A retrospective analysis. Bosn. J. Basic Med. Sci. 2020, 20, 495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masjedi, M.; Mirjalili, M.; Mirzaei, E.; Mirzaee, H.; Vazin, A. The effect of different intensivist staffing patterns on the rate of potential drug-drug interactions in adult trauma intensive care units. Ther. Adv. Drug Saf. 2020, 11, 2042098620980640. [Google Scholar] [CrossRef]
- Fitzmaurice, M.G.; Wong, A.; Akerberg, H.; Avramovska, S.; Smithburger, P.L.; Buckley, M.S.; Kane-Gill, S.L. Evaluation of potential drug-drug interactions in adults in the intensive care unit: A systematic review and meta-analysis. Drug Saf. 2019, 42, 1035–1044. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.Y.; Richardson, L.C.; Li, L.; Day, R.O.; Westbrook, J.I.; Baysari, M.T. Drug-drug interactions and their harmful effects in hospitalised patients: A systematic review and meta-analysis. Eur. J. Clin. Pharmacol. 2018, 74, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Bakker, T.; Abu-Hanna, A.; Dongelmans, D.A.; Vermeijden, W.J.; Bosman, R.J.; de Lange, D.W.; Klopotowska, J.E.; de Keizer, N.F.; Hendriks, S.; Ten Cate, J.; et al. Clinically relevant potential drug-drug interactions in intensive care patients: A large retrospective observational multicenter study. J. Crit. Care 2021, 62, 124–130. [Google Scholar] [CrossRef] [PubMed]
- Pereira, J.M.; Paiva, J.A. Antimicrobial drug interactions in the critically ill patients. Curr. Clin. Pharmacol. 2013, 8, 25–38. [Google Scholar] [PubMed]
- Tanaka, E. Clinically important pharmacokinetic drug-drug interactions: Role of cytochrome P450 enzymes. J. Clin. Pharm. Ther. 1998, 23, 403–416. [Google Scholar] [CrossRef]
- Polasek, T.M.; Lin, F.P.; Miners, J.O.; Doogue, M.P. Perpetrators of pharmacokinetic drug-drug interactions arising from altered cytochrome P450 activity: A criteria-based assessment. Br. J. Clin. Pharmacol. 2011, 71, 727–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, H.; Zhang, L.; Liu, J.; Liu, Y.; Kowey, P.R.; Zhang, Y.; Chen, Y.; Wei, Y.; Gao, L.; Li, H.; et al. Acquired long QT syndrome in hospitalized patients. Heart Rhythm 2017, 14, 974–978. [Google Scholar] [CrossRef]
- Tisdale, J.E.; Jaynes, H.A.; Kingery, J.R.; Mourad, N.A.; Trujillo, T.N.; Overholser, B.R.; Kovacs, R.J. Development and validation of a risk score to predict QT interval prolongation in hospitalized patients. Circulation 2013, 6, 479–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, K.; McGloin, R.; Gellatly, R.M. Predictive validity of a QTc interval prolongation risk score in the intensive care unit. Pharmacotherapy 2020, 40, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Scotton, W.J.; Hill, L.J.; Williams, A.C.; Barnes, N.M. Serotonin syndrome: Pathophysiology, clinical features, management, and potential future directions. Int. J. Tryptophan. Res. 2019, 12, 1178646919873925. [Google Scholar] [CrossRef] [Green Version]
- Werneke, U.; Truedson-Martiniussen, P.; Wikström, H.; Ott, M. Serotonin syndrome: A clinical review of current controversies. J. Integr. Neurosci. 2020, 19, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Bakker, T.; Klopotowska, J.E.; de Keizer, N.F.; van Marum, R.; van der Sijs, H.; de Lange, D.W.; de Jonge, E.; Abu-Hanna, A.; Dongelmans, D.A. Improving medication safety in the Intensive Care by identifying relevant drug-drug interactions—Results of a multicenter Delphi study. J. Crit. Care 2020, 57, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Ceftriaxone (rocephin): Incompatible with Solutions Containing Calcium. Available online: https://www.gov.uk/drug-safety-update/ceftriaxone-rocephin-incompatible-with-solutions-containing-calcium (accessed on 30 September 2021).
- Avci, Z.; Koktener, A.; Uras, N.; Catal, F.; Karadag, A.; Tekin, O.; Degirmencioglu, H.; Baskin, E. Nephrolithiasis associated with ceftriaxone therapy: A prospective study in 51 children. Arch. Dis. Child. 2004, 89, 1069–1072. [Google Scholar] [CrossRef] [Green Version]
- Voeten, M.; Landstra, A.M.; Maseland, M.H.; van Setten, P.A. Serious side effects of frequently used antibiotics in childhood: Biliary sludge or stones induced by ceftriaxone and thrombocytopenia induced by co-trimoxazole. Nederlands Tijdschrift voor Geneeskunde 2007, 151, 1299–1303. [Google Scholar] [PubMed]
- Bartkowska-Śniatkowska, A.; Jończyk-Potoczna, K.; Zielińska, M.; Rosada-Kurasińska, J. Adverse reaction to ceftriaxone in a 28-day-old infant undergoing urgent craniotomy due to epidural hematoma: Review of neonatal biliary pseudolithiasis. Ther. Clin. Risk Manag. 2015, 11, 1035–1041. [Google Scholar] [CrossRef] [Green Version]
- Al-Quteimat, O.; Laila, A. Valproate interaction with carbapenems: Review and recommendations. Hosp. Pharm. 2020, 55, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Carnovale, C.; Pozzi, M.; Mazhar, F.; Mosini, G.; Gentili, M.; Peeters, G.G.; Clementi, E.; Radice, S. Interactions between antiepileptic and antibiotic drugs: A systematic review and meta-analysis with dosing implications. Clin. Pharmacokinet. 2019, 58, 875–886. [Google Scholar] [CrossRef]
- Chai, P.Y.-C.; Chang, C.-T.; Chen, Y.-H.; Chen, H.-Y.; Tam, K.-W. Effect of drug interactions between carbapenems and valproate on serum valproate concentration: A systematic review and meta-analysis. Expert Opin. Drug Saf. 2021, 20, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Kojima, S.; Nadai, M.; Kitaichi, K.; Wang, L.; Nabeshima, T.; Hasegawa, T. Possible mechanism by which the carbapenem antibiotic panipenem decreases the concentration of valproic acid in plasma in rats. Antimicrob. Agents Chemother. 1998, 42, 3136–3140. [Google Scholar] [CrossRef] [Green Version]
- Yokogawa, K.; Iwashita, S.; Kubota, A.; Sasaki, Y.; Ishizaki, J.; Kawahara, M.; Matsushita, R.; Kimura, K.; Ichimura, F.; Miyamoto, K.I. Effect of meropenem on disposition kinetics of valproate and its metabolites in rabbits. Pharm. Res. 2001, 18, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, Y.; Mizobuchi, M.; Nakamura, M.; Takagi, H.; Inagaki, H.; Kominami, G.; Koike, M.; Yamaguchi, T. Mechanism of the drug interaction between valproic acid and carbapenem antibiotics in monkeys and rats. Drug Metab. Dispos. 2004, 32, 1383–1391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamamura, N.; Imura, K.; Naganuma, H.; Nishimura, K. Panipenem, a carbapenem antibiotic, enhances the glucuronidation of intravenously administered valproic acid in rats. Drug Metab. Dispos. 1999, 27, 724–730. [Google Scholar]
- Suzuki, E.; Nakai, D.; Ikenaga, H.; Fusegawa, K.; Goda, R.; Kobayashi, N.; Kuga, H.; Izumi, T. In vivo inhibition of acylpeptide hydrolase by carbapenem antibiotics causes the decrease of plasma concentration of valproic acid in dogs. Xenobiotica 2016, 46, 126–131. [Google Scholar] [CrossRef]
- Omoda, K.; Murakami, T.; Yumoto, R.; Nagai, J.; Maeda, Y.; Kiribayashi, Y.; Takano, M. Increased erythrocyte distribution of valproic acid in pharmacokinetic interaction with carbapenem antibiotics in rat and human. J. Pharm. Sci. 2005, 94, 1685–1693. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, K.; Yumoto, R.; Hamada, N.; Nagai, J.; Takano, M. Interaction of valproic acid and carbapenem antibiotics with multidrug resistance-associated proteins in rat erythrocyte membranes. Epilepsy Res. 2006, 71, 76–87. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-R.; Lin, C.-H.; Hsiao, S.-C.; Chen, N.-C.; Tsai, W.-C.; Chen, S.-D.; Lu, Y.-T.; Chuang, Y.-C. Drug interaction between valproic acid and carbapenems in patients with epileptic seizures. Kaohsiung J. Med Sci. 2017, 33, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.-C.; Pai, T.-Y.; Hsiao, F.-Y.; Shen, L.-J.; Wu, F.-L.L. The effect of different carbapenem antibiotics (ertapenem, imipenem/cilastatin, and meropenem) on serum valproic acid concentrations. Ther. Drug Monit. 2016, 38, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Parkins, M.; Duggan, K. Ertapenem-induced reduction in valproate levels: Case report and review of the literature. Can. J. Hosp. Pharm. 2010, 63, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bede, P.; Lawlor, D.; Solanki, D.; Delanty, N. Carbapenems and valproate: A consumptive relationship. Epilepsia Open 2017, 2, 107–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khatib, R.; Sabir, F.R.N.; Omari, C.; Pepper, C.; Tayebjee, M.H. Managing drug-induced QT prolongation in clinical practice. Postgrad. Med. J. 2021, 97, 452–458. [Google Scholar] [CrossRef]
- Armahizer, M.J.; Seybert, A.L.; Smithburger, P.L.; Kane-Gill, S.L. Drug-drug interactions contributing to QT prolongation in cardiac intensive care units. J. Crit. Care 2013, 28, 243–249. [Google Scholar] [CrossRef]
- Wiśniowska, B.; Tylutki, Z.; Wyszogrodzka, G.; Polak, S. Drug-drug interactions and QT prolongation as a commonly assessed cardiac effect—Comprehensive overview of clinical trials. BMC Pharmacol. Toxicol. 2016, 17, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kantola, T.; Kivistö, K.T.; Neuvonen, P.J. Erythromycin and verapamil considerably increase serum simvastatin and simvastatin acid concentrations. Clin. Pharmacol. Ther. 1998, 64, 177–182. [Google Scholar] [CrossRef]
- Grunden, J.W.; Fisher, K.A. Lovastatin-induced rhabdomyolysis possibly associated with clarithromycin and azithromycin. Ann. Pharmacother. 1997, 31, 859–863. [Google Scholar] [CrossRef] [PubMed]
- Westphal, J.F. Macrolide–induced clinically relevant drug interactions with cytochrome P-450A (CYP) 3A4: An update focused on clarithromycin, azithromycin and dirithromycin. Br. J. Clin. Pharmacol. 2000, 50, 285–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yee, G.C.; McGuire, T.R. Pharmacokinetic drug interactions with cyclosporin (Part I). Clin. Pharmacokinet. 1990, 19, 319–332. [Google Scholar] [CrossRef]
- Salimi, A.; Eybagi, S.; Seydi, E.; Naserzadeh, P.; Kazerouni, N.P.; Pourahmad, J. Toxicity of macrolide antibiotics on isolated heart mitochondria: A justification for their cardiotoxic adverse effect. Xenobiotica 2016, 46, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Volberg, W.A.; Koci, B.J.; Su, W.; Lin, J.; Zhou, J. Blockade of human cardiac potassium channel human ether-a-go-go-related gene (HERG) by macrolide antibiotics. J. Pharmacol. Exp. Ther. 2002, 302, 320–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milberg, P.; Eckardt, L.; Bruns, H.J.; Biertz, J.; Ramtin, S.; Reinsch, N.; Fleischer, D.; Kirchhof, P.; Fabritz, L.; Breithardt, G.; et al. Divergent proarrhythmic potential of macrolide antibiotics despite similar QT prolongation: Fast phase 3 repolarization prevents early afterdepolarizations and torsade de pointes. J. Pharmacol. Exp. Ther. 2002, 303, 218–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorelik, E.; Masarwa, R.; Perlman, A.; Rotshild, V.; Muszkat, M.; Matok, I. Systematic review, meta-analysis, and network meta-analysis of the cardiovascular safety of macrolides. Antimicrob. Agents Chemother. 2018, 62, e00438-18. [Google Scholar] [CrossRef] [Green Version]
- Lewis, R.E.; Beyda, N.D.; Kontoyiannis, D.P. Caspofungin. In Kucers’ The Use of Antibiotics: A Clinical Review of Antibacterial, Antifungal, Antiparasitic, and Antiviral Drugs, 7th ed.; Grayson, M.L., Cosgrove, S.E., Crowe, S., Eds.; CRC Press: Boca Raton, FL, USA, 2017; Volume 7, pp. 2659–2680. [Google Scholar]
- Preston, C.L. (Ed.) Stockley’s Drug Interactions; Phamaceutical Press: London, UK, 2019; Volume 12. [Google Scholar]
- Groetzner, J.; Kaczmarek, I.; Wittwer, T.; Strauch, J.; Meiser, B.; Wahlers, T.; Daebritz, S.; Reichart, B. Caspofungin as first-line therapy for the treatment of invasive aspergillosis after thoracic organ transplantation. J. Heart Lung Transplant. 2008, 27, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Lomaestro, B.M.; Piatek, M.A. Update on drug interactions with azole antifungal agents. Ann. Pharmacother. 1998, 32, 915–928. [Google Scholar] [CrossRef] [PubMed]
- Toda, F.; Tanabe, K.; Ito, S.; Shinmura, H.; Tokumoto, T.; Ishida, H.; Toma, H. Tacrolimus trough level adjustment after administration of fluconazole to kidney recipients. Transplant. Proc. 2002, 34, 1733–1735. [Google Scholar] [CrossRef]
- Sugar, A.M.; Saunders, C.; Idelson, B.A.; Bernard, D.B. Interaction of fluconazole and cyclosporine. Ann. Intern. Med. 1989, 110, 844. [Google Scholar] [CrossRef] [PubMed]
- Mihara, A.; Mori, T.; Aisa, Y.; Yamazaki, R.; Iketani, O.; Tanigawara, Y.; Ikeda, Y.; Okamoto, S. Greater impact of oral fluconazole on drug interaction with intravenous calcineurin inhibitors as compared with intravenous fluconazole. Eur. J. Clin. Pharmacol. 2008, 64, 89–91. [Google Scholar] [CrossRef]
- Muirhead, G.J.; Wulff, M.B.; Fielding, A.; Kleinermans, D.; Buss, N. Pharmacokinetic interactions between sildenafil and saquinavir/ritonavir. Br. J. Clin. Pharmacol. 2000, 50, 99–107. [Google Scholar] [CrossRef]
- Mihailescu, R.; Furustrand Tafin, U.; Corvec, S.; Oliva, A.; Betrisey, B.; Borens, O.; Trampuz, A. High activity of Fosfomycin and Rifampin against methicillin-resistant staphylococcus aureus biofilm in vitro and in an experimental foreign-body infection model. Antimicrob. Agents Chemother. 2014, 58, 2547–2553. [Google Scholar] [CrossRef] [Green Version]
- Ullmann, A.J.; Aguado, J.M.; Arikan-Akdagli, S.; Denning, D.W.; Groll, A.H.; Lagrou, K.; Lass-Flörl, C.; Lewis, R.E.; Munoz, P.; Verweij, P.E.; et al. Diagnosis and management of Aspergillus diseases: Executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 2018, 24, e1–e38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alffenaar, J.W.; van Assen, S.; van der Werf, T.S.; Kosterink, J.G.; Uges, D.R. Omeprazole significantly reduces posaconazole serum trough level. Clin. Infect. Dis. 2009, 48, 839. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraft, W.K.; Chang, P.S.; van Iersel, M.L.; Waskin, H.; Krishna, G.; Kersemaekers, W.M. Posaconazole tablet pharmacokinetics: Lack of effect of concomitant medications altering gastric pH and gastric motility in healthy subjects. Antimicrob. Agents Chemother. 2014, 58, 4020–4025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dare, R.K.; Tewell, C.; Harris, B.; Wright, P.W.; Van Driest, S.L.; Farber-Eger, E.; Nelson, G.E.; Talbot, T.R. Effect of statin coadministration on the risk of daptomycin-associated myopathy. Clin. Infect. Dis. 2018, 67, 1356–1363. [Google Scholar] [CrossRef]
- Bhavnani, S.M.; Rubino, C.M.; Ambrose, P.G.; Drusano, G.L. Daptomycin exposure and the probability of elevations in the creatine phosphokinase level: Data from a randomized trial of patients with bacteremia and endocarditis. Clin. Infect. Dis. 2010, 50, 1568–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galar, A.; Muñoz, P.; Valerio, M.; Cercenado, E.; García-González, X.; Burillo, A.; Sánchez-Somolinos, M.; Juárez, M.; Verde, E.; Bouza, E. Current use of daptomycin and systematic therapeutic drug monitoring: Clinical experience in a tertiary care institution. Int. J. Antimicrob. Agents 2019, 53, 40–48. [Google Scholar] [CrossRef]
- Finch, C.K.; Chrisman, C.R.; Baciewicz, A.M.; Self, T.H. Rifampin and rifabutin drug interactions: An update. Arch. Intern. Med. 2002, 162, 985–992. [Google Scholar] [CrossRef] [PubMed]
- Kyrklund, C.; Backman, J.T.; Kivistö, K.T.; Neuvonen, M.; Laitila, J.; Neuvonen, P.J. Rifampin greatly reduces plasma simvastatin and simvastatin acid concentrations. Clin. Pharmacol. Ther. 2000, 68, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Teng, R.; Mitchell, P.; Butler, K. Effect of rifampicin on the pharmacokinetics and pharmacodynamics of ticagrelor in healthy subjects. Eur. J. Clin. Pharmacol. 2013, 69, 877–883. [Google Scholar] [CrossRef]
- Wang, Z.Y.; Chen, M.; Zhu, L.L.; Yu, L.S.; Zeng, S.; Xiang, M.X.; Zhou, Q. Pharmacokinetic drug interactions with clopidogrel: Updated review and risk management in combination therapy. Ther. Clin. Risk Manag. 2015, 11, 449–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farid, N.A.; Jakubowski, J.A.; Payne, C.D.; Li, Y.G.; Jin, Y.; Ernest, I.C.; Winters, K.J.; Brandt, J.T.; Salazar, D.E.; Small, D.S. Effect of rifampin on the pharmacokinetics and pharmacodynamics of prasugrel in healthy male subjects. Curr. Med. Res. Opin. 2009, 25, 1821–1829. [Google Scholar] [CrossRef] [PubMed]
- Moellering, R.C. Linezolid: The first oxazolidinone antimicrobial. Ann. Intern. Med. 2003, 138, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Hernández, J.L.; Ramos, F.J.; Infante, J.; Rebollo, M.; González-Macías, J. Severe serotonin syndrome induced by mirtazapine monotherapy. Ann. Pharmacother. 2002, 36, 641–643. [Google Scholar] [CrossRef] [PubMed]
- Ubogu, E.E.; Katirji, B. Mirtazapine-induced serotonin syndrome. Clin. Neuropharmacol. 2003, 26, 54–57. [Google Scholar] [CrossRef] [PubMed]
- DeBellis, R.J.; Schaefer, O.P.; Liquori, M.; Volturo, G.A. Linezolid-associated serotonin syndrome after concomitant treatment with citalopram and mirtazepine in a critically ill bone marrow transplant recipient. J. Intensive Care Med. 2005, 20, 351–353. [Google Scholar] [CrossRef] [PubMed]
- Foong, A.L.; Grindrod, K.A.; Patel, T.; Kellar, J. Demystifying serotonin syndrome (or serotonin toxicity). Can. Fam. Physician 2018, 64, 720–727. [Google Scholar] [PubMed]
- Boyer, E.W.; Shannon, M. The serotonin syndrome. N. Engl. J. Med. 2005, 352, 1112–1120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodes, U.; Troeger, U.; Neuling, F.; Jacob, D.; Meyer, F. Drug Interaction Stewardship (DIS) and therapeutic drug monitoring for anti-infective treatment in intensive care, a single centre observational study. Zentralblatt fur Chirurgie 2020, 145, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Ihbe-Heffinger, A.; Langebrake, C.; Hohmann, C.; Leichenberg, K.; Hilgarth, H.; Kunkel, M.; Lueb, M.; Schuster, T. Prospective survey-based study on the categorization quality of hospital pharmacists’ interventions using DokuPIK. Int. J. Clin. Pharm. 2019, 41, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Loj, P.; Olender, A.; Slezak, W.; Krzych, L.J. Pharmacokinetic drug-drug interactions in the intensive care unit—single-centre experience and literature review. Anaesthesiol. Intensive Ther. 2017, 49, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.H.; Yamazaki, M. Role of P-glycoprotein in pharmacokinetics: Clinical implications. Clin. Pharmacokinet. 2003, 42, 59–98. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Yung Chan, S.; Cher Goh, B.; Chan, E.; Duan, W.; Huang, M.; McLeod, H.L. Mechanism-based inhibition of cytochrome P450 3A4 by therapeutic drugs. Clin. Pharmacokinet. 2005, 44, 279–304. [Google Scholar] [CrossRef] [PubMed]
- Bertz, R.J.; Granneman, G.R. Use of in vitro and in vivo data to estimate the likelihood of metabolic pharmacokinetic interactions. Clin. Pharmacokinet. 1997, 32, 210–258. [Google Scholar] [CrossRef] [PubMed]
- Koinuma, K.; Tsuchitani, T.; Imaoka, A.; Akiyoshi, T.; Ohtani, H. Relative contributions of metabolic enzymes to systemic elimination can be estimated from clinical DDI studies: Validation using an in silico approach. Int. J. Clin. Pharmacol. Ther. 2021, 59, 231–238. [Google Scholar] [CrossRef]
- Langebrake, C.; Ihbe-Heffinger, A.; Leichenberg, K.; Kaden, S.; Kunkel, M.; Lueb, M.; Hilgarth, H.; Hohmann, C. Nationwide evaluation of day-to-day clinical pharmacists’ interventions in german hospitals. Pharmacotherapy 2015, 35, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Langebrake, C.; Hohmann, C.; Lezius, S.; Lueb, M.; Picksak, G.; Walter, W.; Kaden, S.; Hilgarth, H.; Ihbe-Heffinger, A.; Leichenberg, K. Clinical pharmacists’ interventions across German hospitals: Results from a repetitive cross-sectional study. Int. J. Clin. Pharm. 2021, 1–8, online ahead of print. [Google Scholar] [CrossRef]
- ATC/DDD Index 2021. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 30 September 2021).
- Boulkedid, R.; Abdoul, H.; Loustau, M.; Sibony, O.; Alberti, C. Using and reporting the delphi method for selecting healthcare quality indicators: A systematic review. PLoS ONE 2011, 6, e20476. [Google Scholar] [CrossRef]


{kind=link}
| Group | Clinically Relevant (n = 65) | Not Clinically Relevant or Low Agreement (n = 23) | Total (n = 88) |
|---|---|---|---|
| Penicillins | 0 | 1 | 1 |
| Cephalosporins | 1 | 1 | 2 |
| Carbapenems | 2 | 0 | 2 |
| Fluoroquinolones | 15 | 1 | 16 |
| Macrolides | 21 | 8 | 29 |
| Glycopeptides | 0 | 1 | 1 |
| Antifungals | 19 | 3 | 22 |
| Miscellaneous | 7 | 8 | 15 |
| Group | Drug 1 | Drug 2 | Mode Category | Additional Strategies to Reduce Patient Risk from Interaction |
|---|---|---|---|---|
| Cephalosporins | Ceftriaxone | Calcium (intravenous) | 3 | separate administration |
| Carbapenems | Imipenem | Valproic acid | 5 | TDM for valproic acid |
| Meropenem | Valproic acid | 5 | ||
| Fluoroquinolones | Ciprofloxacin | Calcium | 3 | separate administration by two hours, or use different administration routes (oral/intravenous) |
| Amiodarone | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium | ||
| Mirtazapine | 3 | |||
| Amitriptyline | 3 | |||
| Haloperidol | 3 | |||
| Theophylline | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium, TDM for theophylline, use 60% of regular theophylline dose | ||
| Iron | 3 | separate administration by two hours, or use different administration routes (oral/intravenous) | ||
| Melatonin | 3 | monitor for sleepiness | ||
| Simvastatin | 3 | CK-monitoring, monitor for signs of myalgia | ||
| Levofloxacin | Amiodarone | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium | |
| Levofloxacin | Haloperidol | 3 | ||
| Moxifloxacin | Amiodarone | 3 | ||
| Mirtazapine | 3 | |||
| Prednisolone | 4 | monitor for signs of tendinopathy | ||
| Macrolides | Azithromycin | Citalopram | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium |
| Haloperidol | 3 | |||
| Clarithromycin | Simvastatin | 5 | withhold/switch statin | |
| Atorvastatin | 5 | CK-monitoring, monitor for signs of myalgia, withhold/switch statin | ||
| Tacrolimus | 3 | TDM for tacrolimus | ||
| Cyclosporine | 3 | TDM for cyclosporine | ||
| Carbamazepine | 3 | where appropriate: switch clarithromycin to azithromycin, TDM for carbamazepine | ||
| Amiodarone | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium | ||
| Haloperidol | 3 | |||
| Ivabradine | 5 | QTc-monitoring, high-normal serum levels of potassium and magnesium, monitor for bradycardia | ||
| Moxifloxacin | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium | ||
| Theophylline | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium, TDM for theophylline | ||
| Erythromycin | Simvastatin | 5 | withhold/switch statin | |
| Atorvastatin | 5 | CK-monitoring, monitor for signs of myalgia, withhold/switch statin | ||
| Quetiapine | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium | ||
| Tacrolimus | 3 | TDM for Tacrolimus | ||
| Amiodaron | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium | ||
| Carbamazepine | 5 | where appropriate: switch erythromycin to azithromycin, TDM for carbamazepine | ||
| Cyclosporine | 3 | where appropriate: switch erythromycin to azithromycin, TDM for cyclosporine | ||
| Erythromycin | Haloperidol | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium, where appropriate: switch erythromycin to azithromycin | |
| Melperon | 3 | QTc-monitoring, high-normal serum levels of potassium and magnesium | ||
| Antifungals | Caspofungin | Cyclosporine | 3 | TDM for cyclosporine |
| Fluconazole | Cyclosporine | 3 | ||
| Tacrolimus | 3 | TDM for tacrolimus | ||
| Simvastatin | 5 | CK-monitoring, monitor for signs of myalgia, withhold/switch statin | ||
| Atorvastatin | 3 | |||
| Carbamazepine | 5 | TDM for carbamazepine | ||
| Rifampicin | 3 | discuss alternatives | ||
| Itraconazole | Simvastatin | 5 | withhold/switch statin | |
| Posaconazole | Pantoprazol | 3 | intravenous administration of posaconazole, TDM for posaconazole | |
| Cyclosporine | 3 | TDM posaconazole and cyclosporine | ||
| Atorvastatin | 5 | withhold/switch statin | ||
| Carbamazepine | 3 | TDM carbamazepine | ||
| Tacrolimus | 3 | TDM posaconazole and tacrolimus | ||
| Voriconazole | Tacrolimus | 3 | TDM voriconazole and tacrolimus | |
| Simvastatin | 5 | withhold/switch statin | ||
| Atorvastatin | 5 | |||
| Cyclosporine | 3 | TDM for voriconazole and cyclosporine | ||
| Rifampicin | 5 | TDM for voriconazole, discuss alternatives | ||
| Sildenafil | 3 | dose reduction of sildenafil | ||
| Miscellaneous | Daptomycin | Atorvastatin | 3 | CK-monitoring, monitor for signs of myalgia, withhold/switch statin |
| Simvastatin | 3 | |||
| Linezolid | Mirtazapine | 3 | monitor for signs of serotonin syndrome | |
| Rifampicin | Cyclosporine | 3 | TDM for cyclosporine | |
| Clopidogrel | 5 | monitor for signs of bleeding, discuss alternatives | ||
| Simvastatin | 5 | withhold/switch statin | ||
| Ticagrelor | 5 | discuss alternatives |
| Azole | Weak Inhibition | Moderate Inhibition | Strong Inhibition | Substrate |
|---|---|---|---|---|
| Itraconazole | CYP 3A4 | CYP3A4 | ||
| Fluconazole | CYP 2C9 CYP 3A4 | CYP 2C19 | ||
| Voriconazole | CYP 2C9 | CYP 2C19 | CYP 3A4 | CYP 3A4 CYP 2C19 CYP 2C9 |
| Posaconazole | CYP 3A4 | P-gp | ||
| Isavuconazole | CYP 3A4 | CYP 3A4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koeck, J.A.; Hilgarth, H.; von Ameln-Mayerhofer, A.; Meyn, D.; Warlich, R.; Münstedt, A.; Horn, D.; König, C. Clinically Relevant Interactions with Anti-Infectives on Intensive Care Units—A Multicenter Delphi Study. Antibiotics 2021, 10, 1330. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111330
Koeck JA, Hilgarth H, von Ameln-Mayerhofer A, Meyn D, Warlich R, Münstedt A, Horn D, König C. Clinically Relevant Interactions with Anti-Infectives on Intensive Care Units—A Multicenter Delphi Study. Antibiotics. 2021; 10(11):1330. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111330
Chicago/Turabian StyleKoeck, Joachim Andreas, Heike Hilgarth, Andreas von Ameln-Mayerhofer, Damaris Meyn, Ruediger Warlich, Andreas Münstedt, Dagmar Horn, and Christina König. 2021. "Clinically Relevant Interactions with Anti-Infectives on Intensive Care Units—A Multicenter Delphi Study" Antibiotics 10, no. 11: 1330. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10111330