
Comparing Treatment Outcomes of Ampicillin-Sulbactam, Other β-Lactams, and Vancomycin in Blood Culture-Negative Infective Endocarditis

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
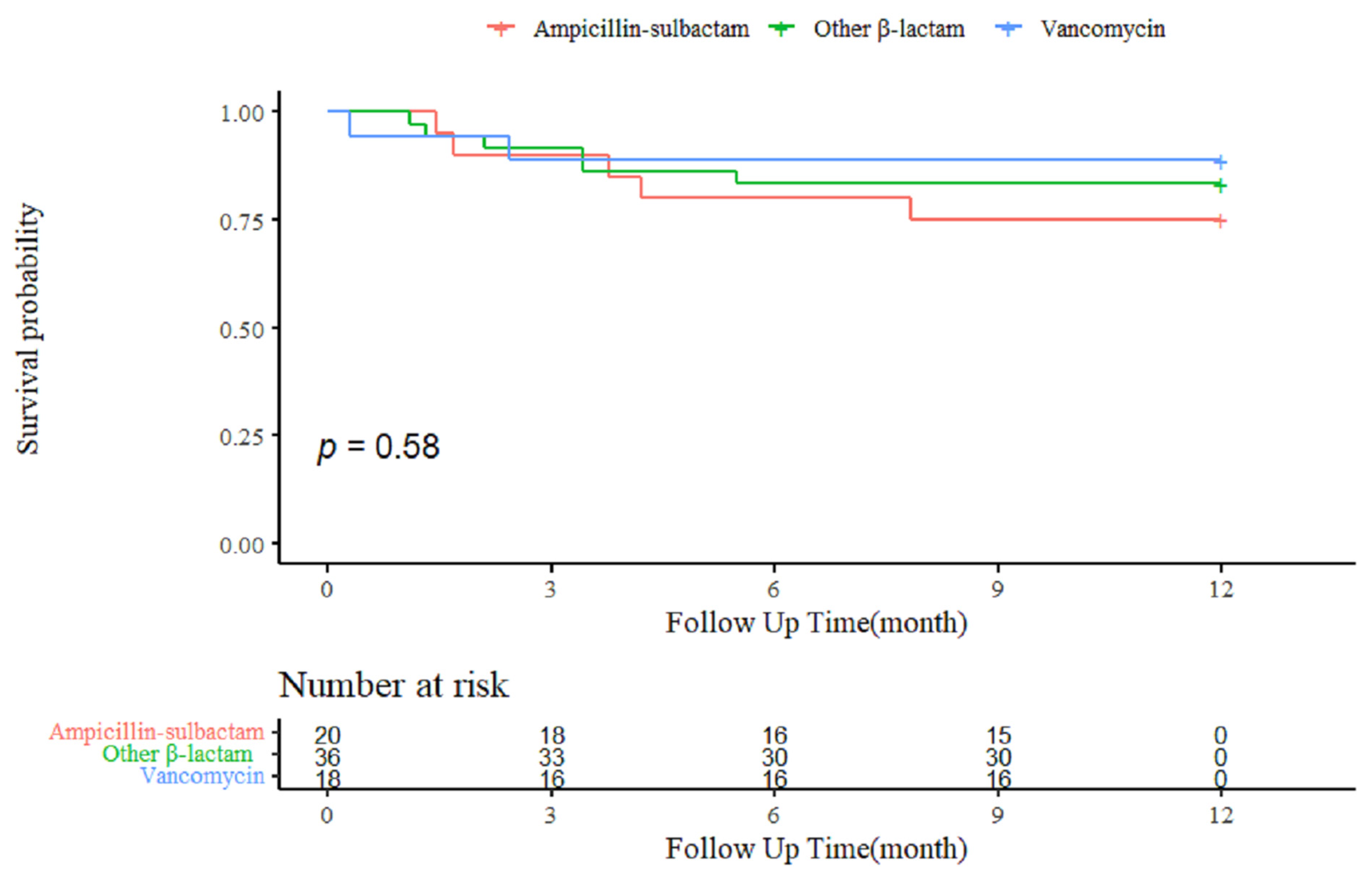
2.2. Treatment Outcomes
2.3. Factors Associated with 1-Year Mortality of BCNIE
3. Discussion
4. Materials and Methods
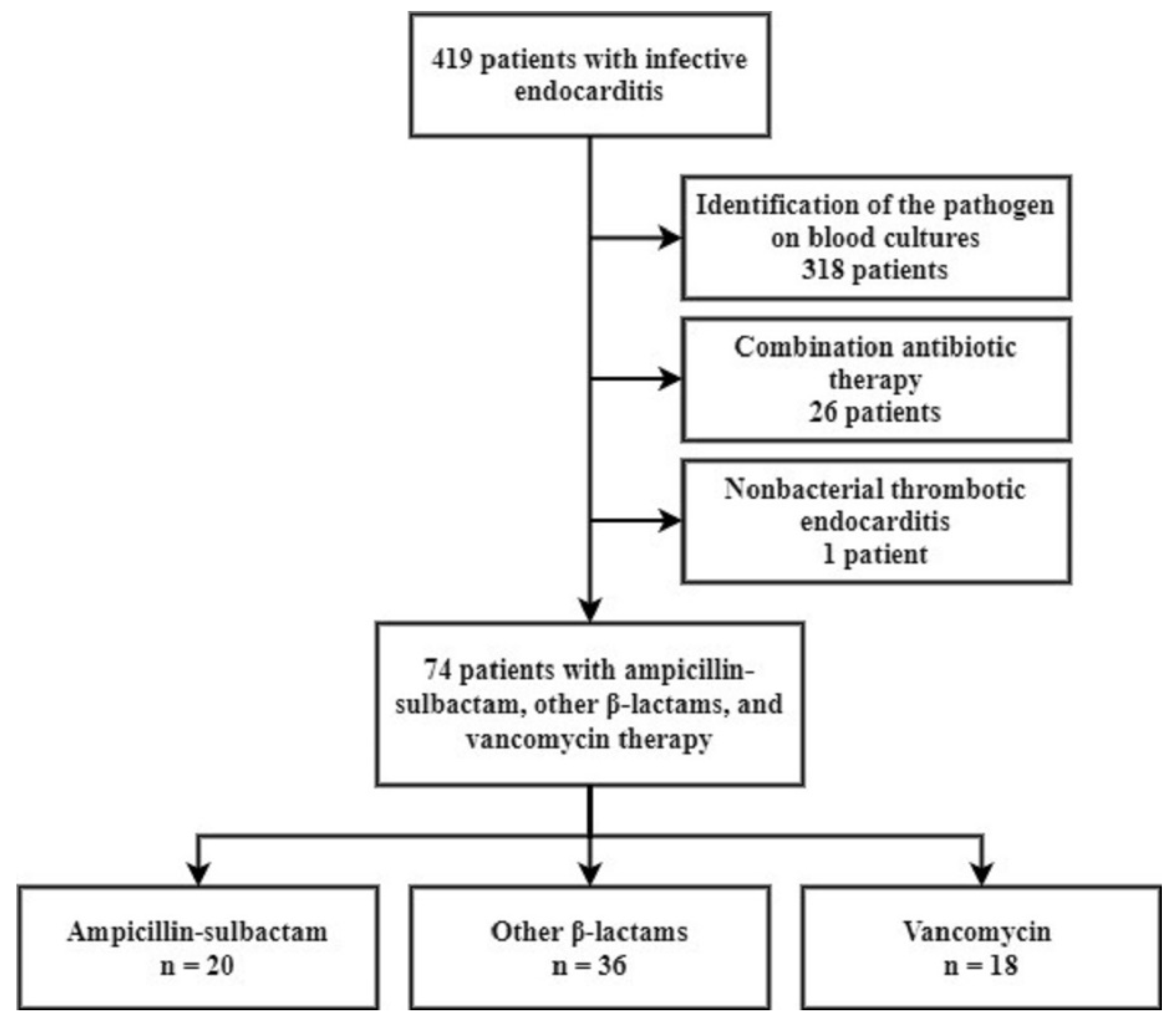
4.1. Study Design and Patient Population
4.2. Antibiotic Groups
4.3. Variables and Definitions
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dayer, M.J.; Jones, S.; Prendergast, B.; Baddour, L.M.; Lockhart, P.B.; Thornhill, M.H. Incidence of infective endocarditis in England, 2000–2013: A secular trend, interrupted time-series analysis. Lancet 2015, 385, 1219–1228. [Google Scholar] [CrossRef] [Green Version]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [CrossRef] [PubMed]
- Baddour, L.M.; Wilson, W.R.; Bayer, A.S.; Fowler, V.G., Jr.; Tleyjeh, I.M.; Rybak, M.J.; Barsic, B.; Lockhart, P.B.; Gewitz, M.H.; Levison, M.E.; et al. Infective Endocarditis in Adults: Diagnosis, Antimicrobial Therapy, and Management of Complications: A Scientific Statement for Healthcare Professionals From the American Heart Association. Circulation 2015, 132, 1435–1486. [Google Scholar] [CrossRef] [PubMed]
- Gould, F.K.; Denning, D.W.; Elliott, T.S.; Foweraker, J.; Perry, J.D.; Prendergast, B.D.; Sandoe, J.A.; Spry, M.J.; Watkin, R.W. Guidelines for the diagnosis and antibiotic treatment of endocarditis in adults: A report of the Working Party of the British Society for Antimicrobial Chemotherapy. J. Antimicrob. Chemother. 2012, 67, 269–289. [Google Scholar] [CrossRef] [Green Version]
- Fournier, P.E.; Thuny, F.; Richet, H.; Lepidi, H.; Casalta, J.P.; Arzouni, J.P.; Maurin, M.; Célard, M.; Mainardi, J.L.; Caus, T.; et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: A prospective study of 819 new cases. Clin. Infect. Dis. 2010, 51, 131–140. [Google Scholar] [CrossRef] [Green Version]
- Hoen, B.; Selton-Suty, C.; Lacassin, F.; Etienne, J.; Briançon, S.; Leport, C.; Canton, P. Infective endocarditis in patients with negative blood cultures: Analysis of 88 cases from a one-year nationwide survey in France. Clin. Infect. Dis. 1995, 20, 501–506. [Google Scholar] [CrossRef]
- Werner, M.; Andersson, R.; Olaison, L.; Hogevik, H. A clinical study of culture-negative endocarditis. Medicine (Baltimore) 2003, 82, 263–273. [Google Scholar] [CrossRef]
- Murashita, T.; Sugiki, H.; Kamikubo, Y.; Yasuda, K. Surgical results for active endocarditis with prosthetic valve replacement: Impact of culture-negative endocarditis on early and late outcomes. Eur. J. Cardiothorac. Surg. 2004, 26, 1104–1111. [Google Scholar] [CrossRef]
- Ferrera, C.; Vilacosta, I.; Fernández, C.; López, J.; Olmos, C.; Sarriá, C.; Revilla, A.; Vivas, D.; Sáez, C.; Rodríguez, E.; et al. Reassessment of blood culture-negative endocarditis: Its profile is similar to that of blood culture-positive endocarditis. Rev. Esp. Cardiol. 2012, 65, 891–900. [Google Scholar] [CrossRef]
- Meidrops, K.; Zuravlova, A.; Osipovs, J.D.; Kalejs, M.; Groma, V.; Petrosina, E.; Reinis, A.; Strike, E.; Dumpis, U.; Erglis, A.; et al. Comparison of outcome between blood culture positive and negative infective endocarditis patients undergoing cardiac surgery. J. Cardiothorac. Surg. 2021, 16, 147. [Google Scholar] [CrossRef]
- Clinical Guideline for the Diagnosis and Treatment of Cardiovascular Infections. Infect. Chemother. 2011, 43, 129–177. [CrossRef]
- Werner, M.; Andersson, R.; Olaison, L.; Hogevik, H. A 10-year survey of blood culture negative endocarditis in Sweden: Aminoglycoside therapy is important for survival. Scand. J. Infect. Dis. 2008, 40, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Menu, E.; Gouriet, F.; Casalta, J.P.; Tissot-Dupont, H.; Vecten, M.; Saby, L.; Hubert, S.; Salaun, E.; Theron, A.; Grisoli, D.; et al. Evaluation of empirical treatment for blood culture-negative endocarditis. J. Antimicrob. Chemother. 2017, 72, 290–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2017–2018. Available online: https://www.who.int/publications/i/item/9789241515061 (accessed on 1 January 2019).
- Liu, C.; Yoon, E.J.; Kim, D.; Shin, J.H.; Shin, J.H.; Shin, K.S.; Kim, Y.A.; Uh, Y.; Kim, H.S.; Kim, Y.R.; et al. Antimicrobial resistance in South Korea: A report from the Korean global antimicrobial resistance surveillance system (Kor-GLASS) for 2017. J. Infect. Chemother. 2019, 25, 845–859. [Google Scholar] [CrossRef]
- Barnes, S.L.; Rock, C.; Harris, A.D.; Cosgrove, S.E.; Morgan, D.J.; Thom, K.A. The Impact of Reducing Antibiotics on the Transmission of Multidrug-Resistant Organisms. Infect. Control Hosp. Epidemiol. 2017, 38, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Lamas, C.C.; Fournier, P.E.; Zappa, M.; Brandão, T.J.; Januário-da-Silva, C.A.; Correia, M.G.; Barbosa, G.I.; Golebiovski, W.F.; Weksler, C.; Lepidi, H.; et al. Diagnosis of blood culture-negative endocarditis and clinical comparison between blood culture-negative and blood culture-positive cases. Infection 2016, 44, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Arregle, F.; Gouriet, F.; Amphoux, B.; Edouard, S.; Chaudet, H.; Casalta, J.P.; Habib, G.; Fournier, P.E.; Raoult, D. Western Immunoblotting for the Diagnosis of Enterococcus faecalis and Streptococcus gallolyticus Infective Endocarditis. Front. Cell. Infect. Microbiol. 2019, 9, 314. [Google Scholar] [CrossRef] [PubMed]
- Katip, W.; Oberdorfer, P. A Monocentric Retrospective Study of AUC/MIC Ratio of Vancomycin Associated with Clinical Outcomes and Nephrotoxicity in Patients with Enterococcal Infections. Pharmaceutics 2021, 13, 1378. [Google Scholar] [CrossRef]
- Chirouze, C.; Athan, E.; Alla, F.; Chu, V.H.; Ralph Corey, G.; Selton-Suty, C.; Erpelding, M.L.; Miro, J.M.; Olaison, L.; Hoen, B. Enterococcal endocarditis in the beginning of the 21st century: Analysis from the International Collaboration on Endocarditis-Prospective Cohort Study. Clin. Microbiol. Infect. 2013, 19, 1140–1147. [Google Scholar] [CrossRef] [Green Version]
- van Loon, K.; Voor In ’t Holt, A.F.; Vos, M.C. A Systematic Review and Meta-analyses of the Clinical Epidemiology of Carbapenem-Resistant Enterobacteriaceae. Antimicrob. Agents Chemother. 2018, 62. [Google Scholar] [CrossRef] [Green Version]
- Falagas, M.E.; Kopterides, P. Risk factors for the isolation of multi-drug-resistant Acinetobacter baumannii and Pseudomonas aeruginosa: A systematic review of the literature. J. Hosp. Infect. 2006, 64, 7–15. [Google Scholar] [CrossRef] [PubMed]
- Kiefer, T.; Park, L.; Tribouilloy, C.; Cortes, C.; Casillo, R.; Chu, V.; Delahaye, F.; Durante-Mangoni, E.; Edathodu, J.; Falces, C.; et al. Association between valvular surgery and mortality among patients with infective endocarditis complicated by heart failure. JAMA 2011, 306, 2239–2247. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Lee, H.J.; Ku, N.S.; Lee, S.H.; Lee, S.; Choi, J.Y.; Yeom, J.S. Infective endocarditis at a tertiary care hospital in South Korea. Heart 2021, 107, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, O.; Sexton, D.J.; Wang, A.; Pappas, P.A.; Kourany, W.; Chu, V.; Fowler, V.G., Jr.; Woods, C.W.; Engemann, J.J.; Corey, G.R.; et al. Early surgery in patients with infective endocarditis: A propensity score analysis. Clin. Infect. Dis. 2007, 44, 364–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamas, C.C.; Eykyn, S.J. Blood culture negative endocarditis: Analysis of 63 cases presenting over 25 years. Heart 2003, 89, 258–262. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.W.; Park, S.W.; Cho, E.J.; Lee, G.Y.; Kim, E.K.; Chang, S.A.; Park, S.J.; Lee, S.C.; Kang, C.I.; Chung, D.R.; et al. Risk factors for poor prognosis in nosocomial infective endocarditis. Korean J. Intern. Med. 2018, 33, 102–112. [Google Scholar] [CrossRef] [Green Version]
- Ortega-Loubon, C.; Muñoz-Moreno, M.F.; Andrés-García, I.; Álvarez, F.J.; Gómez-Sánchez, E.; Bustamante-Munguira, J.; Lorenzo-López, M.; Tamayo-Velasco, Á.; Jorge-Monjas, P.; Resino, S.; et al. Nosocomial vs. Community-Acquired Infective Endocarditis in Spain: Location, Trends, Clinical Presentation, Etiology, and Survival in the 21st Century. J. Clin. Med. 2019, 8. [Google Scholar] [CrossRef] [Green Version]
- Gilleece, A.; Fenelon, L. Nosocomial infective endocarditis. J. Hosp. Infect. 2000, 46, 83–88. [Google Scholar] [CrossRef]
- Houpikian, P.; Raoult, D. Blood culture-negative endocarditis in a reference center: Etiologic diagnosis of 348 cases. Medicine (Baltimore) 2005, 84, 162–173. [Google Scholar] [CrossRef]
- Lim, M.H.; Chung, D.R.; Kim, W.S.; Park, K.S.; Ki, C.S.; Lee, N.Y.; Kim, S.M. First case of Bartonella quintana endocarditis in Korea. J. Korean Med. Sci. 2012, 27, 1433–1435. [Google Scholar] [CrossRef] [Green Version]
- Kwak, W.; Chu, H.; Hwang, S.; Park, J.H.; Hwang, K.J.; Gwack, J.; Choi, Y.S.; Youn, S.K.; Park, M.Y. Epidemiological characteristics of serologically confirmed q Fever cases in South Korea, 2006-2011. Osong Public Health Res. Perspect. 2013, 4, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Siciliano, R.F.; Mansur, A.J.; Castelli, J.B.; Arias, V.; Grinberg, M.; Levison, M.E.; Strabelli, T.M. Community-acquired culture-negative endocarditis: Clinical characteristics and risk factors for mortality. Int. J. Infect. Dis. 2014, 25, 191–195. [Google Scholar] [CrossRef] [Green Version]
- Slipczuk, L.; Codolosa, J.N.; Davila, C.D.; Romero-Corral, A.; Yun, J.; Pressman, G.S.; Figueredo, V.M. Infective endocarditis epidemiology over five decades: A systematic review. PLoS ONE 2013, 8, e82665. [Google Scholar] [CrossRef] [PubMed]
- Hidron, A.I.; Edwards, J.R.; Patel, J.; Horan, T.C.; Sievert, D.M.; Pollock, D.A.; Fridkin, S.K. NHSN annual update: Antimicrobial-resistant pathogens associated with healthcare-associated infections: Annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect. Control Hosp. Epidemiol. 2008, 29, 996–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.S.; Sexton, D.J.; Mick, N.; Nettles, R.; Fowler, V.G., Jr.; Ryan, T.; Bashore, T.; Corey, G.R. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. 2000, 30, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total (n = 74) | Ampicillin-Sulbactam (n = 20) | Other β-Lactams (n = 36) | Vancomycin (n = 18) | p-Value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Age, years, median (IQR) | 54.5 (44.25–67.75) | 54 (32.75–69.25) | 54 (48.5–68) | 55 (45.25–65.75) | 0.908 |
| Male sex (%) | 41 (55.4) | 9 (45.0) | 23 (63.9) | 9 (50.0) | 0.343 |
| Community acquired (%) | 57 (77.0) | 15 (75.0) | 28 (77.8) | 14 (77.8) | 0.969 |
| Nosocomial (%) | 17 (23.0) | 5 (25.0) | 8 (22.2) | 4 (22.2) | 0.969 |
| Valve Status (%) | 0.189 | ||||
| Native valve | 65 (87.7) | 17 (85.0) | 34 (94.4) | 14 (77.8) | |
| Prosthetic valve | 9 (12.2) | 3 (15.0) | 2 (5.6) | 4 (22.2) | |
| Involved valve (%) | 0.351 | ||||
| Aortic valve | 31 (41.9) | 9 (45.0) | 17 (47.2) | 5 (27.8) | 0.373 |
| Mitral valve | 42 (56.8) | 12 (60.0) | 18 (50.0) | 12 (66.7) | 0.478 |
| Tricuspid valve | 5 (6.8) | 1 (5.0) | 3 (8.3) | 1 (5.6) | 0.869 |
| Pulmonary valve | 4 (5.4) | 2 (10.0) | 0 | 2 (11.1) | 0.133 |
| Multiple valves | 7 (9.5) | 4 (20.0) | 1 (2.8) | 2 (11.1) | 0.104 |
| Comorbidities (%) | |||||
| Previous IE | 2 (2.7) | 0 (0.0) | 1 (2.8) | 1 (5.6) | 0.573 |
| Predisposing valve condition | 25 (33.8) | 5 (25.0) | 13 (36.1) | 7 (38.9) | 0.611 |
| Patients with previous valve surgery or prosthesis | 13 (17.6) | 4 (20.0) | 4 (11.1) | 5 (27.8) | 0.299 |
| Patients with cardiac devices | 3 (4.1) | 0 | 1 (2.8) | 2 (11.1) | 0.192 |
| Diabetes mellitus | 13 (17.6) | 1 (5.0) | 10 (27.8) | 2 (11.1) | 0.071 |
| Chronic heart failure | 2 (2.7) | 1 (5.0) | 1 (2.8) | 0 (0.0) | 0.637 |
| Renal disease | 3 (4.1) | 1 (5.0) | 1 (2.8) | 1 (5.6) | 0.860 |
| Liver disease | 2 (2.7) | 0 | 1 (2.8) | 1 (5.6) | 0.573 |
| Solid cancer | 9 (12.2) | 4 (20.0) | 4 (11.1) | 1 (5.6) | 0.382 |
| Hematologic malignancy | 2 (2.7) | 0 | 2 (5.6) | 0 | 0.338 |
| Recent chemotherapy | 5 (6.8) | 3 (15.0) | 2 (5.6) | 0 | 0.170 |
| Connective tissue disease | 1 (1.4) | 1 (5.0) | 0 | 0 | 0.254 |
| Immunosuppressive therapy | 1 (1.4) | 1 (5.0) | 0 | 0 | 0.254 |
| Charlson comorbidity index, median (IQR) | 4 (0–4) | 2 (0–3.25) | 1 (0–3.25) | 1 (0.25–2.75) | 0.805 1 |
| SOFA score, median (IQR) | 1 (1–2) | 1 (1–2) | 1 (1–2) | 1 (1–2) | 0.984 1 |
| Antibiotics use in the last 3 months (%) | 11 (14.9) | 2 (10.0) | 6 (16.7) | 3 (16.7) | 0.774 |
| Central venous access (%) | 6 (8.1) | 3 (15.0) | 2 (5.6) | 1 (5.6) | 0.417 |
| Modified Duke criteria (%) | 0.507 | ||||
| Definite IE | 29 (39.2) | 9 (45.0) | 15 (41.7) | 5 (27.8) | |
| Possible IE | 45 (60.8) | 11 (55.0) | 21 (58.3) | 13 (72.2) | |
| Gentamicin combination (%) | 54 (73.0) | 18 (90.0) | 24 (66.7) | 12 (66.7) | 0.133 |
| Total (n = 74) | Ampicillin-Sulbactam (n = 20) | Other β-Lactams (n = 36) | Vancomycin (n = 18) | p-Value | |
|---|---|---|---|---|---|
| Duration of antibiotics treatment, days, median (IQR) | 30 (23.25–42.75) | 31 (20.75–42) | 30.5 (24.75–50) | 28 (23.25–41.5) | 0.670 1 |
| Surgery performed (%)Indication of surgery (%) | 56 (75.7) | 15 (75.0) | 28 (77.8) | 13 (72.2) | 0.901 |
| Congestive heart failure | 53 (71.6) | 15 (75.0) | 26 (72.2) | 12 (66.7) | 0.845 |
| Prevention of embolism | 24 (32.4) | 9 (45.0) | 11 (30.6) | 4 (22.2) | 0.308 |
| Paravalvular complications | 8 (10.8) | 2 (10.0) | 4 (11.1) | 2 (11.1) | 0.991 |
| Pacemaker infections | 2 (2.7) | 0 | 1 (2.8) | 1 (5.6) | 0.573 |
| Uncontrolled infections | 1 (1.4) | 1 (5.0) | 0 | 0 | 0.254 |
| Clinical outcomes (%) | |||||
| New-onset heart failure | 8 (10.8) | 3 (15.0) | 3 (8.3) | 2 (11.1) | 0.743 |
| New conduction abnormality | 8 (10.8) | 4 (20.0) | 2 (5.6) | 2 (11.1) | 0.249 |
| Paravalvular complication | 5 (6.8) | 1 (5.0) | 2 (5.6) | 2 (11.1) | 0.697 |
| Renal failure | 7 (9.5) | 3 (15.0) | 2 (5.6) | 2 (11.1) | 0.493 |
| CNS involvement | 19 (25.7) | 6 (30.0) | 10 (27.8) | 3 (16.7) | 0.593 |
| Systemic embolism | 6 (8.1) | 2 (10.0) | 2 (5.6) | 2 (11.1) | 0.730 |
| Mortality (%) | |||||
| 1-year mortality | 13 (17.6) | 5 (25.0) | 6 (16.7) | 2 (11.1) | 0.522 |
| In-hospital mortality | 7 (9.5) | 1 (5.0) | 4 (11.1) | 2 (11.1) | 0.727 |
| 28-days mortality | 4 (1.4) | 0 | 3 (8.3) | 1 (5.6) | 0.417 |
| Overall mortality | 15 (20.3) | 6 (30.0) | 7 (19.4) | 2 (11.1) | 0.346 |
| Univariate Analysis | Multivariate Analysis 1 | |||
|---|---|---|---|---|
| Hazard Ratio (95% CI) | p-Value | Hazard Ratio (95% CI) | p-Value | |
| Nosocomial IE | 14 (3.9–52) | <0.001 | 6.14 (1.41–26.69) | 0.015 |
| Surgery performed | 0.075 (0.02–0.27) | <0.001 | 0.18 (0.04–0.79) | 0.023 |
| SOFA score | 1.6 (1.1–2.3) | 0.008 | ||
| Charlson comorbidity index | 1.2 (1.1–1.4) | <0.001 | ||
| Gentamicin combination | 0.41 (0.14–1.2) | 0.11 | ||
| Antibiotics groups | ||||
| Ampicillin-sulbactam | Reference | |||
| Other β-lactams | 0.66 (0.20–2.17) | 0.498 | ||
| Vancomycin | 0.44 (0.09–2.27) | 0.326 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.J.; Kim, J.H.; Lee, H.J.; Lee, K.H.; Lee, E.H.; Baek, Y.J.; Kim, J.N.; Ahn, J.Y.; Jeong, S.J.; Ku, N.S.; et al. Comparing Treatment Outcomes of Ampicillin-Sulbactam, Other β-Lactams, and Vancomycin in Blood Culture-Negative Infective Endocarditis. Antibiotics 2021, 10, 1476. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10121476
Lee SJ, Kim JH, Lee HJ, Lee KH, Lee EH, Baek YJ, Kim JN, Ahn JY, Jeong SJ, Ku NS, et al. Comparing Treatment Outcomes of Ampicillin-Sulbactam, Other β-Lactams, and Vancomycin in Blood Culture-Negative Infective Endocarditis. Antibiotics. 2021; 10(12):1476. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10121476
Chicago/Turabian StyleLee, Se Ju, Jung Ho Kim, Hi Jae Lee, Ki Hyun Lee, Eun Hwa Lee, Yae Jee Baek, Jin Nam Kim, Jin Young Ahn, Su Jin Jeong, Nam Su Ku, and et al. 2021. "Comparing Treatment Outcomes of Ampicillin-Sulbactam, Other β-Lactams, and Vancomycin in Blood Culture-Negative Infective Endocarditis" Antibiotics 10, no. 12: 1476. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10121476