
Impact of Adjunctive Laser Irradiation on the Bacterial Load of Dental Root Canals: A Randomized Controlled Clinical Trial





Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Treatment Procedure
- Removal of the temporary filling material.
- Chemomechanical preparation was performed manually to size 25.02 using hand files in a pulling movement only (Hedström, VDW GmbH, Munich, Germany) and mechanically to size 30.09 (ProTaper Gold F1-F3 employing SiroNiti Apex endodontic handpiece; Dentsply Sirona GmbH, Bensheim, Germany) along the glide path with each insertion deeper than the previous one until the working length was reached. The root canal system was irrigated with sodium hypochlorite (3%; total 5 mL, applied over the duration of the root canal preparation) and ethylenediaminetetraacetic acid (15%; 2 mL, 1 min).
- Adjuvant disinfection in accordance with one of the following three group-specific protocols:
- (a)
- Additional rinsing with 5 mL sodium hypochlorite (3%; Speiko–Dr. Speier GmbH, Bielefeld, Germany) for 1 min.
- (b)
- Laser irradiation (SiroLaser Blue; Dentsply Sirona) in continuous-wave mode, at a power setting of 0.6 W for 4 × 10 s with an attached 200-μm fiber tip (Easy Tip Endo; Dentsply Sirona) (Figure 1).
- (c)
- A combination of sodium hypochlorite rinsing and laser irradiation using the same settings as described above (a + b).
2.3. Laser Application
2.4. Microbiological Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Haapasalo, M. Endodontische Mikrobiologie. In Endodontologie, 2nd ed.; Baumann, M.A., Beer, R., Eds.; Thieme Verlag KG: Stuttgart, Germany, 2007; pp. 21–30. [Google Scholar]
- Hülsmann, M. Endodontie; Thieme Verlag KG: Stuttgart, Germany, 2008. [Google Scholar]
- Bergenholtz, G. Assessment of treatment failure in endodontic therapy. J. Oral Rehabil. 2016, 43, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Blome, B.; Braun, A.; Sobarzo, V.; Jepsen, S. Molecular identification and quantification of bacteria from endodontic infections using real-time polymerase chain reaction. Oral Microbiol. Immunol. 2008, 23, 384–390. [Google Scholar] [CrossRef]
- Koçkapan, C. Curriculum Endodontie; Quintessenz Publishing: Berlin, Germany, 2003. [Google Scholar]
- Vatkar, N.A.; Hegde, V.; Sathe, S. Vitality of Enterococcus faecalis inside dentinal tubules after five root canal disinfection methods. J. Conserv. Dent. 2016, 19, 445–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berutti, E.; Marini, R.; Angeretti, A. Penetration ability of different irrigants into dentinal tubules. J. Endod. 1997, 23, 725–727. [Google Scholar] [CrossRef]
- Kouchi, Y.; Ninomiya, J.; Yasuda, H.; Fukui, K.; Moriyama, T.; Okamoto, H. Location of Streptococcus mutans in the dentinal tubules of open infected root canals. J. Dent. Res. 1980, 59, 2038–2046. [Google Scholar] [CrossRef] [Green Version]
- Iandolo, A.; Amato, M.; Dagna, A.; Poggio, C.; Abdellatif, D.; Franco, V.; Pantaleo, G. Intracanal heating of sodium hypochlorite: Scanning electron microscope evaluation of root canal walls. J. Conserv. Dent. 2018, 21, 569–573. [Google Scholar] [CrossRef] [PubMed]
- Amato, M.; Pantaleo, G.; Abtellatif, D.; Blasi, A.; Gagliani, M.; Iandolo, A. An in vitro evaluation of the degree of pulp tissue dissolution through different root canal irrigation protocols. J. Conserv. Dent. 2018, 21, 175–179. [Google Scholar] [CrossRef]
- Galler, K.M.; Grubmüller, V.; Schlichting, R.; Widbiller, M.; Eidt, A.; Schuller, C.; Wölflick, M.; Hiller, K.; Buchalla, W. Penetration depth of irrigants into root dentine after sonic, ultrasonic and photoacoustic activation. Int. Endod. J. 2019, 52, 1210–1217. [Google Scholar] [CrossRef]
- Dioguardi, M.; Di Gioia, G.; Illuzzi, G.; Laneve, E.; Cocco, A.; Troiano, G. Endodontic irrigants: Different methods to improve efficacy and related problems. Eur. J. Dent. 2018, 12, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Saydjari, Y.; Kuypers, T.; Gutknecht, N. Laser Application in Dentistry: Irradiation Effects of Nd:YAG 1064 nm and Diode 810 nm and 980 nm in Infected Root Canals—A Literature Overview. BioMed Res. Int. 2016, 2016, 8421656. [Google Scholar] [CrossRef] [Green Version]
- Alda, J. Laser and Gaussian beam propagation and transformation. In Encyclopedia of Optical and Photonic Engineering; Driggers, R., Ed.; Dekker: New York, NY, USA, 2003; Volume 3, pp. 999–1013. ISBN 0-8247-4252-4. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Jillsdale, NJ, USA, 1988. [Google Scholar]
- Kaiwar, A.; Usha, H.L.; Meena, N.; Ashwini, P.; Murthy, C.S. The efficiency of root canal disinfection using a diode laser: In vitro study. Indian J. Dent. Res. 2013, 24, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Asnaashari, M.; Safavi, N. Disinfection of Contaminated Canals by Different Laser Wavelengths, while Performing Root Canal Therapy. J. Lasers Med. Sci. 2013, 4, 8–16. [Google Scholar]
- Schoop, U.; Kluger, W.; Moritz, A.; Nedjelik, N.; Georgopoulos, A.; Sperr, W. Bactericidal effect of different laser systems in the deep layers of dentin. Lasers Surg. Med. 2004, 35, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Kreisler, M.; Kohnen, W.; Beck, M.; Al Haj, H.; Christoffers, A.; Götz, H.; Duschner, H.; Jansen, B.; D’Hoedt, B. Efficacy of NaOCl/H2O2 irrigation and GaAlAs laser in decontamination of root canals in vitro. Lasers Surg. Med. 2003, 32, 189–196. [Google Scholar] [CrossRef]
- Moritz, A.; Gutknecht, N.; Goharkhay, K.; Schoop, U.; Wernisch, J.; Sperr, W. In vitro irradiation of infected root canals with a diode laser: Results of microbiologic, infrared spectrometric, and stain penetration examinations. Quintessence Int. 1997, 28, 205–209. [Google Scholar]
- Shehatou, C.; Logunov, S.L.; Dunman, P.M.; Haidaris, C.G.; Klubben, W.S. Characterizing the Antimicrobial Properties of 405 nm Light and the Corning® Light-Diffusing Fiber Delivery System. Lasers Surg. Med. 2019, 51, 887–896. [Google Scholar] [CrossRef] [Green Version]
- Niemz, M.H. Laser-Tissue Interactions: Fundamentals and Applications; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Franzen, R.; Al Hassan, N.; Conrads, G.; Gutknecht, N. Der 445-nm-Diodenlase rin der Endodontie: Erste In-vitro Ergebnisse. Int. Mag. Laser Dent. 2016, 8, 45. [Google Scholar]
- De Oliveira, F.A.; Matos, A.A.; Matsuda, S.S.; Buzalaf, M.A.R.; Bagnato, V.S.; Machado, M.A.D.A.M.; Damante, C.A.; de Oliveira, R.C.; Peres-Buzalaf, C. Low level laser therapy modulates viability, alkaline phosphatase and matrix metalloproteinase-2 activities of osteoblasts. J. Photochem. Photobiol. B Biol. 2017, 169, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, L.A.B.; de Souza Lopes, Z.M.; de Sá, R.C.; Novaes, A.B., Jr.; Romualdo, P.C.; Lucisano, M.P.; Nelfon-Filho, P.; da Silva, R.A.B. Comparison of apical periodontitis repair in endodontic treatment with calcium hydroxide-dressing and aPDT. Braz. Oral Res. 2019, 33, e092. [Google Scholar] [CrossRef] [PubMed]
- Klinke, T.; Klimm, W.; Gutknecht, N. Antibacterial effects of Nd:YAG laser irradiation within root canal dentin. J. Clin. Laser Med. Surg. 1997, 15, 29–31. [Google Scholar] [CrossRef]
- Mohammadi, Z.; Jafarzadeh, H.; Shalavi, S.; Sahebalam, R.; Kinoshita, J.-I.; Patil, S. Laser-based Disinfection of the Root Canal System: An Update. J. Contemp. Dent. Pract. 2017, 18, 74–77. [Google Scholar] [PubMed]
- Stabholz, A.; Zeltser, R.; Sela, M.; Peretz, B.; Moshonov, J.; Ziskind, D.; Stabholz, A. The use of lasers in dentistry: Principles of operation and clinical applications. Compend. Contin. Educ. Dent. 2003, 24, 935–948. [Google Scholar]
- Plotino, G.; Cortese, T.; Grande, N.M.; Leonardi, D.; Di Giorgio, G.; Testarelli, L.; Gambarini, G. New Technologies to Improve Root Canal Disinfection. Braz. Dent. J. 2016, 27, 3–8. [Google Scholar] [CrossRef]
- European Society of Endodontology. Quality guidelines for endodontic treatment: Consensus report of the European Society of Endodontology. Int. Endod. J. 2006, 39, 921–930. [Google Scholar] [CrossRef] [PubMed]
- Katalinić, I.; Budimir, A.; Bošnjak, Z.; Jakovljević, S.; Anić, I. The photo-activated and photo-thermal effect of the 445/970 nm diode laser on the mixed biofilm inside root canals of human teeth in vitro: A pilot study. Photodiagn. Photodyn. 2019, 26, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Hülsmann, M.; Rödig, T. Desinfektion. In Endodontologie, 2nd ed.; Baumann, M.A., Beer, R., Eds.; Thieme Verlag KG: Stuttgart, Germany, 2007; pp. 189–197. [Google Scholar]



{kind=link}
{kind=link}
| Baseline | Root Canal Preparation | Adjunctive Disinfection | |
|---|---|---|---|
| NaOCl (Group a) | |||
| Mean | 5.74 × 106 | 5.14 × 105 | 1.98 × 105 |
| Standard Deviation | 2.32 × 107 | 1.26 × 106 | 5.54 × 105 |
| Median | 1.84 × 105 | 9.25 × 104 | 4.03 × 104 |
| Minimum | 3.06 × 104 | 8.81 × 102 | 1.98 × 102 |
| Maximum | 1.01 × 108 | 4.48 × 106 | 2.36 × 106 |
| Interquartile Range | 9.75 × 104 | 1.30 × 105 | 4.59 × 104 |
| n | 19 | 19 | 19 |
| Laser Irradiation (Group b) | |||
| Mean | 2.97 × 106 | 5.12 × 105 | 2.27 × 105 |
| Standard Deviation | 9.75 × 106 | 1.59 × 106 | 7.05 × 105 |
| Median | 2.03 × 105 | 9.81 × 104 | 5.43 × 104 |
| Minimum | 1.14 × 103 | 1.02 × 103 | 5.79 × 102 |
| Maximum | 4.18 × 107 | 7.00 × 106 | 3.13 × 106 |
| Interquartile Range | 2.36 × 105 | 1.85 × 105 | 1.05 × 105 |
| n | 19 | 19 | 19 |
| NaOCl + Laser Irradiation (Group c) | |||
| Mean | 1.72 × 106 | 1.89 × 105 | 5.64 × 104 |
| Standard Deviation | 3.94 × 106 | 5.06 × 105 | 1.00 × 105 |
| Median | 2.00 × 105 | 4.83 × 104 | 2.11 × 104 |
| Minimum | 1.11 × 104 | 2.29 × 103 | 7.31 × 102 |
| Maximum | 1.49 × 107 | 2.26 × 106 | 4.18 × 105 |
| Interquartile Range | 1.50 × 105 | 9.24 × 104 | 3.52 × 104 |
| n | 19 | 19 | 19 |
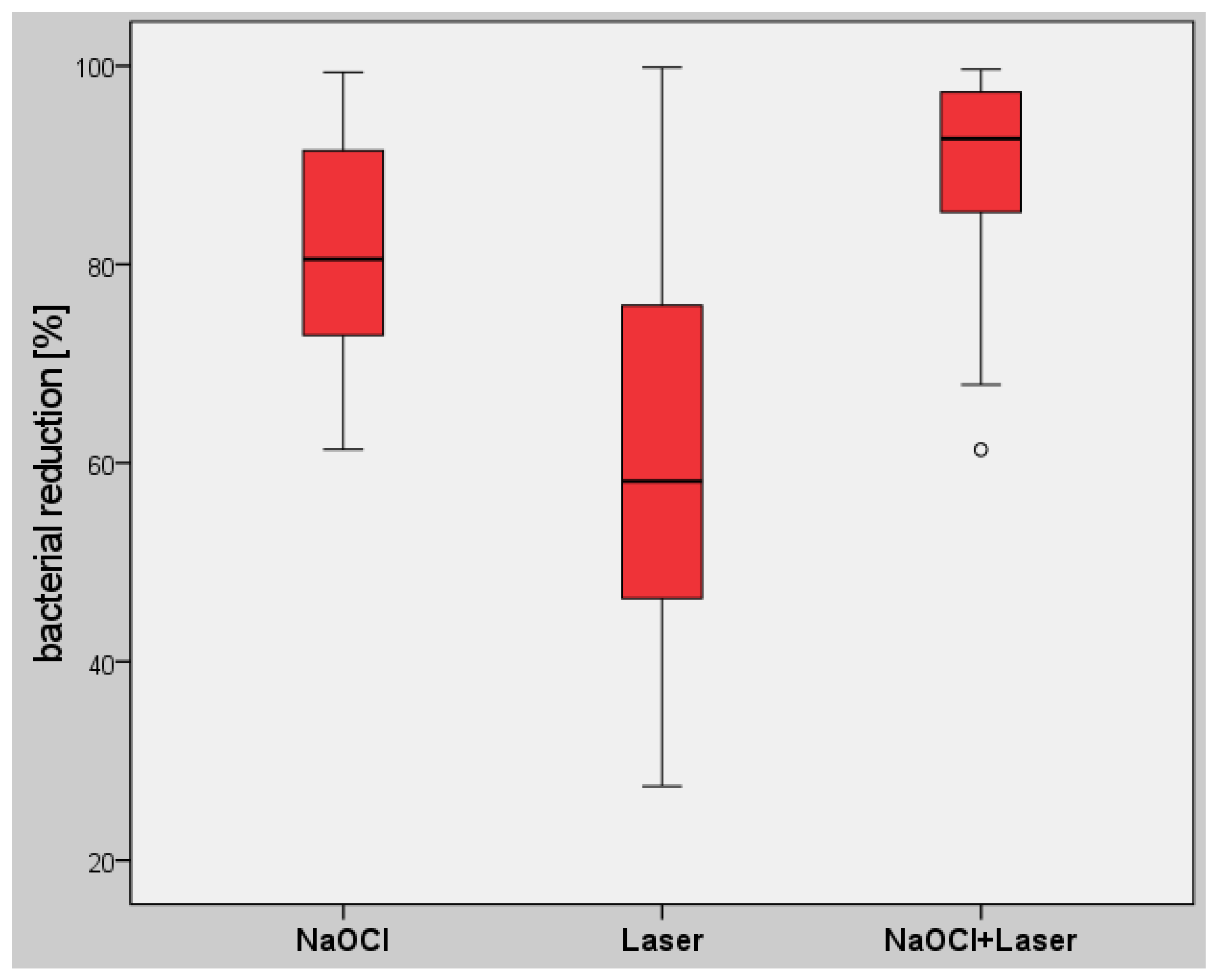
| NaOCl (Group a) | Laser (Group b) | NaOCl + Laser Irradiation (Group c) | |
|---|---|---|---|
| Mean | 80.61 | 63.06 | 89.40 |
| Standard Deviation | 12.32 | 21.98 | 10.43 |
| Median | 80.54 | 58.18 | 92.69 |
| Minimum | 61.38 | 27.46 | 61.35 |
| Maximum | 99.35 | 99.87 | 99.67 |
| Interquartile Range | 18.58 | 29.51 | 12.08 |
| n | 19 | 19 | 19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wenzler, J.-S.; Falk, W.; Frankenberger, R.; Braun, A. Impact of Adjunctive Laser Irradiation on the Bacterial Load of Dental Root Canals: A Randomized Controlled Clinical Trial. Antibiotics 2021, 10, 1557. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10121557
Wenzler J-S, Falk W, Frankenberger R, Braun A. Impact of Adjunctive Laser Irradiation on the Bacterial Load of Dental Root Canals: A Randomized Controlled Clinical Trial. Antibiotics. 2021; 10(12):1557. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10121557
Chicago/Turabian StyleWenzler, Johannes-Simon, Wolfgang Falk, Roland Frankenberger, and Andreas Braun. 2021. "Impact of Adjunctive Laser Irradiation on the Bacterial Load of Dental Root Canals: A Randomized Controlled Clinical Trial" Antibiotics 10, no. 12: 1557. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10121557