
The Graphical Representation of Cell Count Representation: A New Procedure for the Diagnosis of Periprosthetic Joint Infections


Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, C.; Renz, N.; Trampuz, A. Management of periprosthetic joint infection. Hip Pelvis 2018, 30, 138–146. [Google Scholar] [CrossRef]
- Fehring, T.K.; Griffin, W.L. Revision of failed cementless total knee implants with cement. Clin. Orthop. Relat. Res. 1998, 356, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Saleh, K.J.; Rand, J.A.; McQueen, A. Current status of revision total knee arthroplasty: How do we assess results? J. Bone Jt. Surg. Am. 2003, 85 (Suppl. S1), 18–20. [Google Scholar] [CrossRef] [PubMed]
- Scuderi, G.R.; Insall, J.N.; Windsor, R.E.; Moran, M.C. Survivorship of cemented knee replacements. J. Bone Jt. Surg. Br. 1989, 71, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Della Valle, C.J.; Zuckermann, J.D.; Di Cesare, P.E. Periprosthetic sepsis. Clin. Orthop. Relat. Res. 2004, 420, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Hanssen, A.D. Managing the infected knee: As good as it gets. J. Arthroplast. 2002, 17, 98–101. [Google Scholar] [CrossRef] [PubMed]
- Della Valle, C.J.; Sporer, S.M.; Jacobs, J.J.; Berger, R.A.; Rosenberg, A.G.; Paprosky, W.G. Perioperative testing for sepsis before revision total knee arthroplasty. J. Arthroplast. 2007, 22 (Suppl. S2), 90–93. [Google Scholar] [CrossRef]
- Trampuz, A.; Hanssen, A.D.; Osmon, D.R.; Mandrekar, J.; Steckelberg, J.M.; Patel, R. Synovial fluid leukocyte count and differential for the diagnosis of periprosthetic knee infection. Am. J. Med. 2004, 117, 556–562. [Google Scholar] [CrossRef]
- Parvizi, J.; Zmistowski, B.; Berbari, E.F.; Bauer, T.W.; Springer, B.D.; Della Valle, C.J.; Garvin, K.L.; Mont, M.A.; Wongworawat, M.D.; Zalavras, C.G. New definition for periprosthetc joint infection: From the workgroup of the musculoskeletal infection society. Clin. Orthop. Relat. Res. 2011, 469, 2992–2994. [Google Scholar] [CrossRef] [Green Version]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Workgroup Convened by the Musculoskeletal Infection Society. New definition for periprosthetic joint infection. J. Arthroplast. 2011, 26, 1136–1138. [Google Scholar] [CrossRef]
- Choi, H.-R.; Agrawal, K.; Bedair, H. The diagnostic thresholds for synovial fluid analysis in late periprosthetic infection of the hip depend on the duration of symptoms. Bone Jt. J. 2016, 98, 1355–1359. [Google Scholar] [CrossRef]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef] [Green Version]
- Shahi, A.; Deirmengian, C.; Higuera, C.; Chen, A.; Restrepo, C.; Zmistowski, B.; Oliveira, A. Premature therapeutic antimicrobial treat-ments can compromise the diagnosis of late periprosthetic joint infection. Clin. Orthop. Relat. Res. 2015, 473, 2244–2249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahi, A.; Parvizi, J.; Kazarian, G.S.; Higuera, C.; Frangiamore, S.; Bingham, J.; Beauchamp, C.; Della Valle, C.; Deirmengian, C. The Alpha-defensin test for periprosthetic joint infections is not affected by prior antibiotic administration. Clin. Orthop. Relat. Res. 2016, 474, 1610–1615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwarzkopf, R.; Carlson, E.M.; Tibbo, M.E.; Josephs, L.; Scott, R.D. Syonvial fluid differential cell count in wear debris synovitis after total knee arthroplasty. Knee 2014, 21, 1023–1028. [Google Scholar] [CrossRef]
- Yi Ba, P.H.; Corss, M.B.; Moric, M.; Levine, B.R.; Sporer, S.M.; Paprosky, W.G.; Jacobs, J.J.; Della Valle, C.J. Do serologic and synovial tests help diagnose infection in revision hip arthroplasty with metal-on-metal bearings or corrosion? Clin. Orthop. Relat. Res. 2015, 473, 498–505. [Google Scholar]
- Deirmengian, C.A.; Kazarian, G.S.; Feeley, S.P.; Sizer, S.C. False-positive automated synovial fluid white blood cell counting Is a concern for both hip and knee arthroplasty aspirates. J. Arthroplast. 2020, 35, S304–S307. [Google Scholar] [CrossRef] [PubMed]
- Wasterlain, A.S.; Goswami, K.; Ghasemi, S.A.; Parvizi, J. Diagnosis of periprosthetic infection. J. Bone Jt. Surg. Am. Vol. 2020, 102, 1366–1375. [Google Scholar] [CrossRef]
- Cooper, H.J.; Della Valle, C.J.; Berger, R.A.; Tetreault, M.; Paprosky, W.G.; Sporer, S.M.; Jacobs, J.J. Corrosion at the head-neck taper as a cause for adverse local tissue reactions after total hip arthroplasty. J. Bone Jt. Surg. Am. Vol. 2012, 94, 1655–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, H.J.; Urban, R.M.; Wixson, R.L.; Meneghini, R.M.; Jacobs, J.J. Adverse local tissue reaction arising form corrosion at the femoral neck-body junction in a dual-taper stem with a cobalt-chromium modular neck. J. Bone Jt. Surg. Am. 2013, 95, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Earll, M.D.; Earll, P.G.; Rougeux, R.S. Wound drainage after metal-on-metal hip arthroplasty secondary to presumed delayed hypersensitivity reaction. J. Arthroplast. 2011, 26, 338.e5–338.e7. [Google Scholar] [CrossRef] [PubMed]
- Mikhael, M.M.; Hanssen, A.D.; Sierra, R.J. Failure of metal-on-metal total hip arthroplasty mimicking hip infection. J. Bone Jt. Surg. Am. Vol. 2009, 91, 443–446. [Google Scholar] [CrossRef]
- Wyles, C.C.; Larson, D.R.; Houdek, M.T.; Sierra, R.J.; Trousdale, R.T. Utility of synovial fluid aspirations in failed metal-on-metal total hip arthroplasty. J. Arthroplast. 2013, 28, 818–823. [Google Scholar] [CrossRef] [PubMed]
- Balato, G.; Franceschini, V.; Ascione, T.; Lamberti, A.; Balboni, F.; Baldini, A. Diagnostic accuracy of synovial fluid, blood markers, and microbiological testing in chronic knee prosthetic infections. Arch. Orthop. Trauma Surg. 2018, 138, 165–171. [Google Scholar] [CrossRef]
- Bergin, P.F.; Doppelt, J.D.; Hamilton, W.G.; Mirick, G.E.; Jones, A.E.; Sritulanondha, S.; Helm, J.M.; Tuan, R.S. Detection of periprosthetic infections with use of ribosomal rna-based polymerase chain reaction. J. Bone Jt. Surg. Am. Vol. 2010, 92, 654–663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanem, E.; Parvizi, J.; Burnett, R.S.J.; Sharkey, P.F.; Keshavarzi, N.; Aggarwal, A.; Barrack, R.L. Cell count and differential of aspirated fluid in the diagnosis of infection at the site of total knee arthroplasty. J. Bone Jt. Surg. Am. Vol. 2008, 90, 1637–1643. [Google Scholar] [CrossRef] [PubMed]
- Mason, J.B.; Fehring, T.K.; Odum, S.M.; Griffin, W.L.; Nussman, D.S. The value of white blood cell counts before revision total knee arthroplasty. J. Arthroplast. 2003, 18, 1038–1043. [Google Scholar] [CrossRef]
- Parvizi, J.; Ghanem, E.; Menashe, S.; Barrack, R.L.; Bauer, T.W. Periprosthetic infection: What are the diagnostic challenges? J. Bone Jt. Surg. Am. Vol. 2006, 88, 138–147. [Google Scholar] [CrossRef]
- Zmistowski, B.; Restrepo, C.; Huang, R.; Hozack, W.J.; Parvizi, J. Periprosthetic joint infection diagnosis: A complete understanding of white blood cell count and differential. J. Arthroplast. 2012, 27, 1589–1593. [Google Scholar] [CrossRef]
- De Vecchi, E.; Romano, C.L.; De Grandi, R.; Cappelletti, L.; Villa, F.; Drago, L. Alpha defensin, leukocyte esterase, C-reactive protein, and leukocyte count in synovial fluid for pre-operative diagnosis of periprosthetic infection. Int. J. Immunopathol. Pharmacol. 2018, 32, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinneen, A.; Guyot, A.; Clements, J.; Bradley, N. Synovial fluid white cell and differential count in the diagnosis or exclusion of prosthetic joint infection. Bone Jt. J. 2013, 95, 554–557. [Google Scholar] [CrossRef] [PubMed]
- Higuera, C.A.; Zmistowski, B.; Malcom, T.; Barsoum, W.K.; Sporer, S.M.; Mommsen, P.; Kendoff, D.; Della Valle, C.J.; Parvizi, J. Synovial fluid cell count for diagnosis of chronic periprosthetic hip infection. J. Bone Jt. Surg. Am. Vol. 2017, 99, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Spangehl, M.J.; Masri, B.A.; O’connell, J.X.; Duncan, C.P. Prospective analysis of preoperative and intraoperative investigations for the diagnosis of infection at the sites of two hundred and two revision total hip arthroplasties. J. Bone Jt. Surg. Am. 1999, 81, 672–683. [Google Scholar] [CrossRef]
- Schinsky, M.F.; Della Valle, C.J.; Sporer, S.M.; Paprosky, W.G. Perioperative testing for joint infection in patients undergoing revision total hip arthroplasty. J. Bone Jt. Surg. Am. Vol. 2008, 90, 1869–1875. [Google Scholar] [CrossRef] [Green Version]
- Krenn, V.; Otto, M.; Morawietz, L.; Hopf, T.; Jakobs, M.; Klauser, W.; Schwantes, B.; Gehrke, T. Histopathologic diagnostics in endoprosthetics: Periprosthetic neosynovialitis, hypersensitivity reaction, and arthrofibrosis. Orthopäde 2009, 38, 520–530. [Google Scholar] [CrossRef] [PubMed]
- Krenn, V.; Morawietz, L.; Perino, G.; Kienapfel, H.; Ascherl, R.; Hassenpflug, G.; Thomsen, M.; Thomas, P.; Huber, M.; Kendoff, D.; et al. Revised histopathological consensus classification of joint implant related pathology. Pathol. Res. Pract. 2014, 210, 779–786. [Google Scholar] [CrossRef]
- Müller, M.; Morawietz, L.; Hasart, O.; Strube, P.; Perka, C.; Tohtz, S. Histopathological diagnosis of periprosthetic joint infection following total hip arthroplasty: Use of a standardized classification system of the periprosthetic interface membrane. Orthopade 2009, 38, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Deirmengian, C.; Feeley, S.; Kazarian, G.S.; Kardos, K. Synovial fluid aspirates dilated with saline or blood reduce the sensitivity of traditional and contemporary synovial fluid biomarkers. Clin. Orthop. Relat. Res. 2020, 478, 1805–1813. [Google Scholar] [CrossRef]
- Li, R.; Lu, Q.; Zhou, Y.-G.; Chai, W.; Lu, S.-B.; Chen, J.-Y. Centrifugation may change the results of leukocyte esterase strip testing in the diagnosis of periprosthetic joint infection. J. Arthroplast. 2018, 33, 2981–2985. [Google Scholar] [CrossRef]
- Salinas, M.; Rosas, J.; Iborra, J.; Manero, H.; Pascual, E. Comparison of manual and automated cell counts in EDTA preserved synovial fluids. Storage has little influence on the results. Ann. Rheum. Dis. 1997, 56, 622–626. [Google Scholar] [CrossRef] [PubMed]
- de Jonge, R.; Brouwer, R.; Smit, M.; de Frankrijker-Merkestijn, M.; Dolhain, R.J.E.M.; Hazes, J.M.W.; van Toorenenbergen, A.W.; Lindemans, J. Automated counting of white blood cells in synovial fluid. Rheumatology 2004, 43, 170–173. [Google Scholar] [CrossRef]
- Schumacher, H.R.; Sieck, M.S.; Rothfuss, S.; Clayburne, G.M.; Baumgarten, D.F.; Mochan, B.S.; Kant, J.A. Reproducibility of synovial fluid analyses. A study among four laboratories. Arthritis Rheum. 1986, 29, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Sugiuchi, H.; Ando, Y.; Manabe, M.; Nakamura, E.; Mizuta, H.; Nagata, S.; Okabe, H. Measurement of total and differential white blood cell counts in synovial fluid by means of an automated hematology analyzer. J. Lab. Clin. Med. 2005, 146, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Tahta, M.; Simsek, M.E.; Isik, C.; Akkaya, M.; Gursoy, S.; Bozkurt, M. Does inflammatory joint diseases affect the accuracy of infection biomarkers in patients with periprosthetic joint infections? A prospective comparative reliability study. J. Orthop. Sci. 2019, 24, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Schäfer, P.; Fink, B.; Sandow, D.; Margull, A.; Berger, I.; Frommelt, L. Prolonged bacterial culture to identify late periprosthetic joint infection: A promising strategy. Clin. Infect. Dis. 2008, 47, 1403–1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Autor | N | Cut-Off | Sensi-Tivity | Specifi-City | PPV | NPV | Accu-Racy |
|---|---|---|---|---|---|---|---|
| Balato 2018 [25] | 167 K | >2800/µL >72% PMN | 83.8% 84% | 89.7% 91% | |||
| Bergin 2010 [26] | 64 K | >2500/µL >60% PMN | 71% | 98% | 91% | 93% | 92% |
| Della Valle 2007 [7] | 105 K | >3000/µL >65% PMN | 100% | 98.1% | 97.6% | 100% | 98.9% |
| Ghanem 2008 [27] | 429 K | >1100/µL >64% PMN | 90.7% 95.0% | 88.1% 94.7% | 87.2% 91.6% | 91.5% 96.9% | |
| Mason 2003 [28] | 86 K | >2500/mL >60%PMN | 98% | 95% | 91% | 82% | |
| Parvizi 2006 [29] | 145 K | >1760/µL >73%PMN | |||||
| Trampuz 2004 [8] | 133 K | >1700/µL >65% PMN | 94% 97% | 88% 98% | 73% 94% | 98% 99% | |
| Zmistowski 2012 [30] | 150 K | >3000/µL >75%PMN | 93% 93% | 94% 83% | 93% 84% | 94% 93% | 93% 88% |
| Choi 2016 [12] | 138 H | >5750/µL ≤ 2 w >1556/µL > 2 w | 94% 91% | 100% 94% | 100% 87% | 89% 97% | 99% 95% |
| De Vecchi 2018 [31] | 21 H + 45 K | >1600/µL >3000/µl | 100% 93.7% | 82.3% 91.2% | 84.2% 90.9% | 100% 93.9% | |
| Dinneen 2013 [32] | 75 H | >1580/µL >80% PMN | 89.5% 89.7% | 91.3% 86.6% | |||
| Higuera 2017 [33] | 453 H | >3966/µL >80% PMN | 89.5% 92.1% | 91.2% 85.8% | 76.4% 59.3% | 97.5% 98.0% | 93.0% 87.0% |
| Spangehl 1999 [34] | 202 H | >5000/µL >80% PMN | 89% | 85% | 52% | 98% | |
| Schinsky 2008 [35] | 201 H | >4200/µL >80% PMN | 84% 84% | 93% 82% | 81% 65% | 93% 93% | 90% 83% |
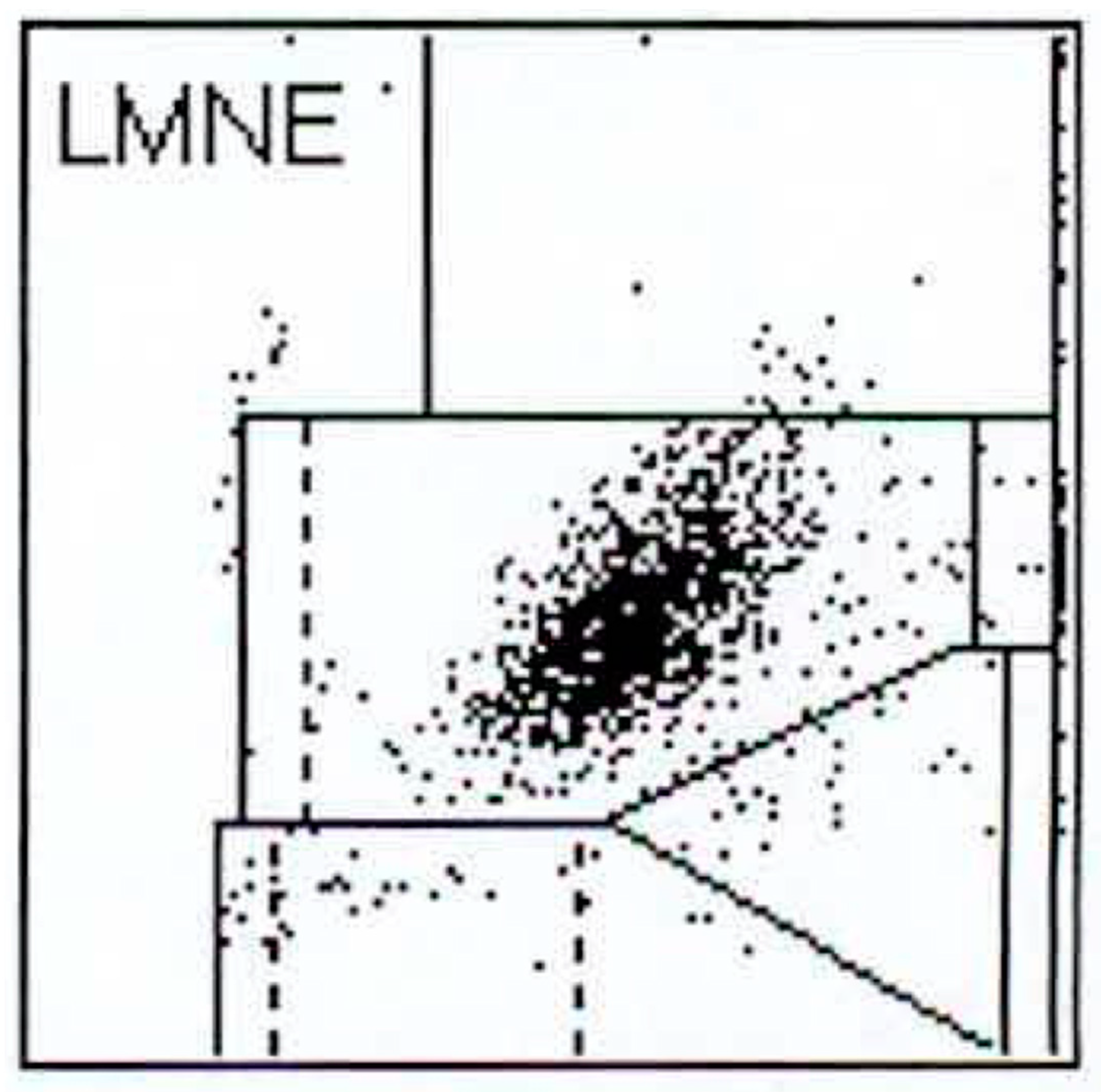
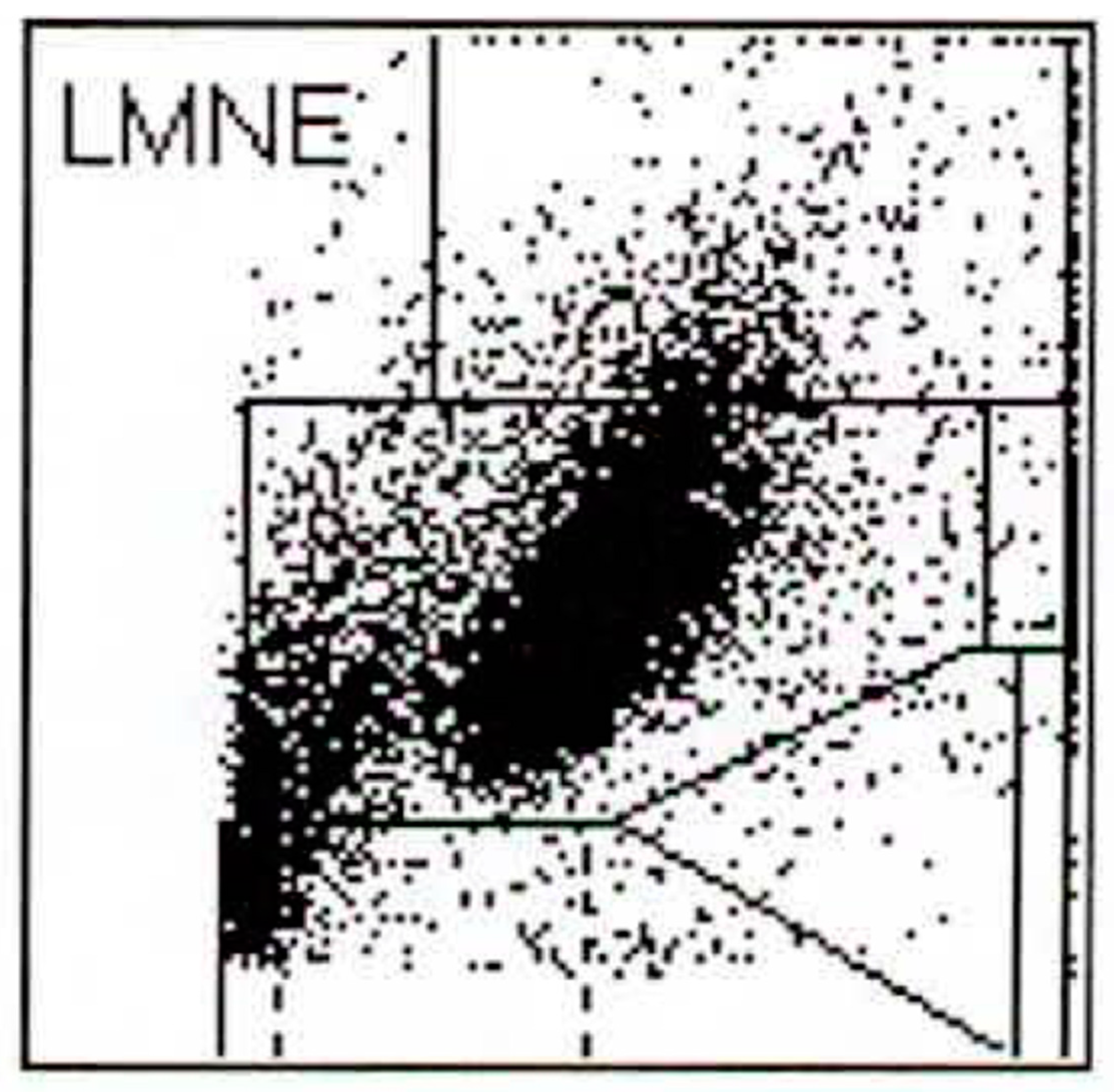
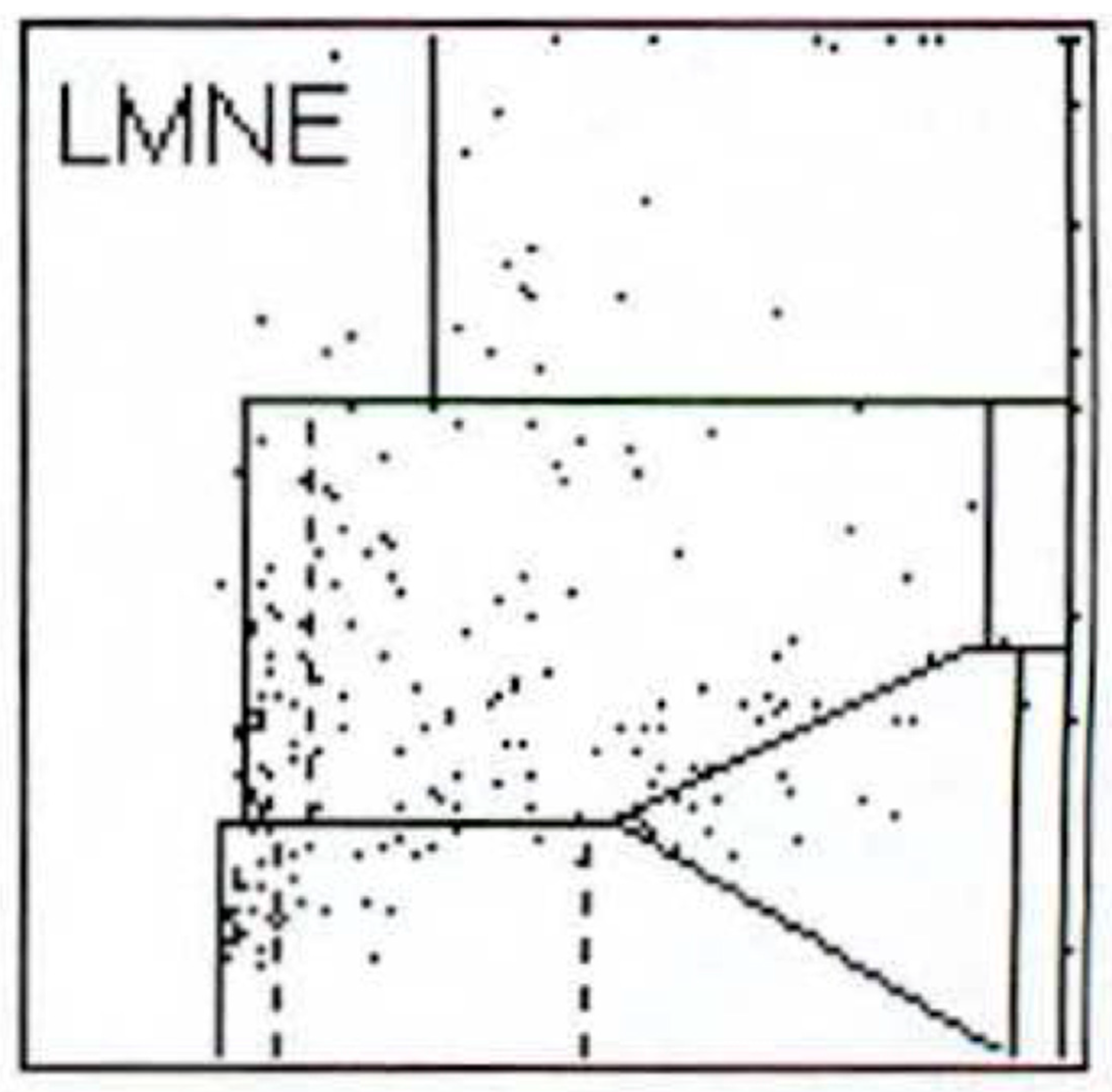
| LMNE-Type | Histological Classification | ||||
|---|---|---|---|---|---|
| TYPE I | TYPE II | TYPE III | TYPE IV | TOTAL | |
| LMNE-Type I | 65 | 0 | 1 | 25 | 91 |
| LMNE-Type II | 5 | 68 | 5 | 2 | 80 |
| LMNE-Type III | 15 | 21 | 6 | 8 | 50 |
| LMNE-Type IV | 36 | 0 | 2 | 63 | 101 |
| TOTAL | 121 | 89 | 14 | 98 | 322 |
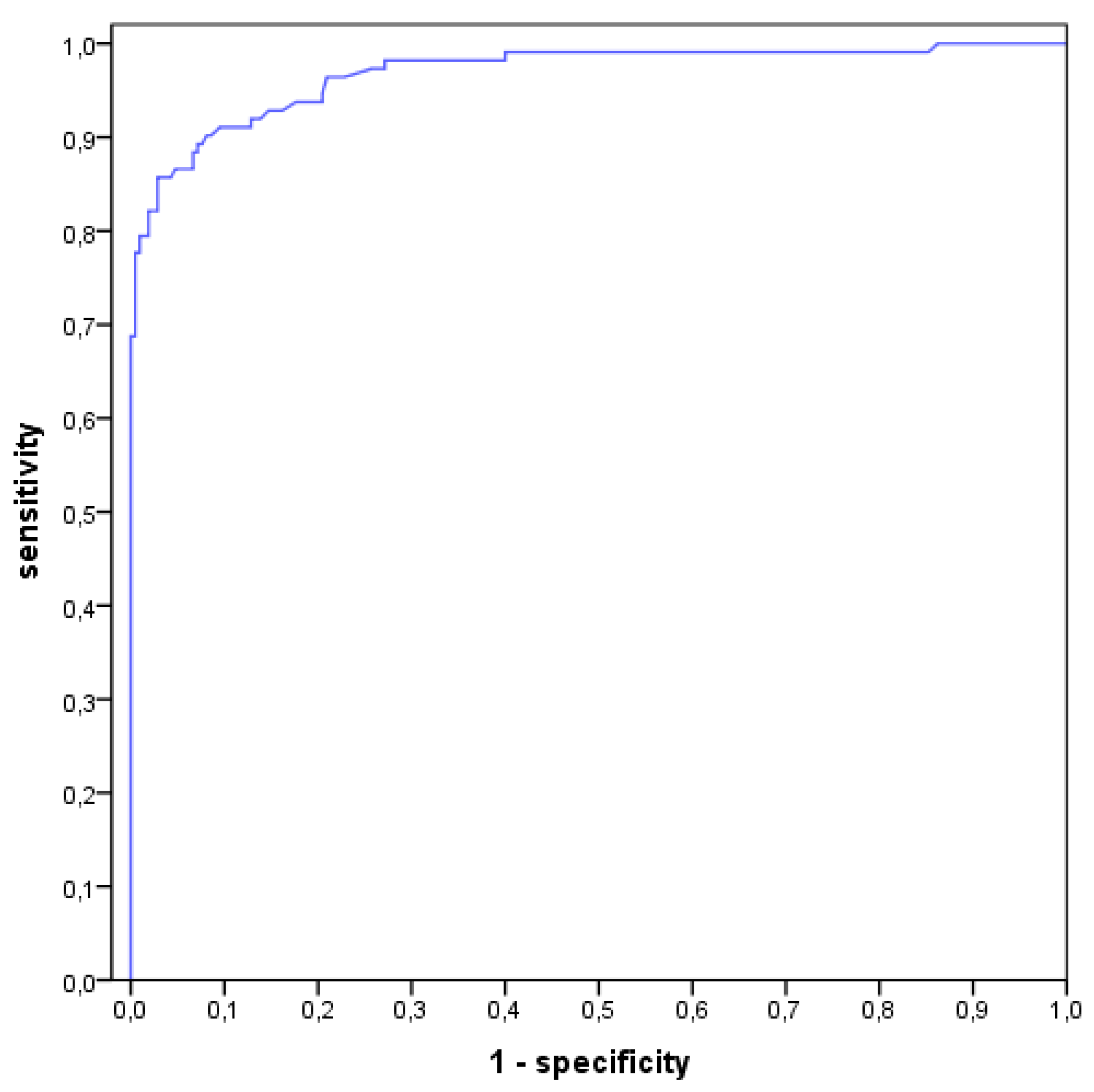
| Threshold of Cell Count | Diagnostic | Value | Likelihood Ratio Positive | Likelihood Ratio Negative | ||||
|---|---|---|---|---|---|---|---|---|
| PJI | Accuracy | 93.5% | ||||||
| yes | no | Sensitivity | 98.2% | 10.86 | 0.02 | |||
| X = 500 | pos. | 110 | 19 | 129 | Specificity | 91.0% | ||
| neg. | 2 | 191 | 193 | PPV | 85.3% | |||
| 112 | 210 | 322 | NPV | |||||
| PJI | Accuracy | 93.2% | ||||||
| yes | no | Sensitivity | 93.8% | 13.13 | 0.07 | |||
| X = 1000 | pos. | 105 | 15 | 120 | Specificity | 92.9% | ||
| neg. | 7 | 195 | 202 | PPV | 87.5% | |||
| 112 | 210 | 322 | NPV | |||||
| PJI | Accuracy | 93.8% | ||||||
| yes | no | Sensitivity | 90.2% | 21.04 | 0.10 | |||
| X = 1500 | pos. | 101 | 9 | 110 | Specificity | 95.7% | ||
| neg. | 11 | 201 | 212 | PPV | 91.8% | |||
| 112 | 210 | 322 | NPV | |||||
| PJI | Accuracy | 93.2% | ||||||
| yes | no | Sensitivity | 86.6% | 25.98 | 0.14 | |||
| X = 2000 | pos. | 97 | 7 | 104 | Specificity | 96.7% | ||
| neg. | 15 | 203 | 218 | PPV | 93.3% | |||
| 112 | 210 | 322 | NPV | |||||
| PJI | Accuracy | 93.8% | ||||||
| yes | no | Sensitivity | 84.8% | 59.38 | 0.15 | |||
| X = 2500 | pos. | 95 | 3 | 98 | Specificity | 98.6% | ||
| neg. | 17 | 207 | 224 | PPV | 96.9% | |||
| 112 | 210 | 322 | NPV | |||||
| PJI | Accuracy | 93.2% | ||||||
| yes | no | Sensitivity | 82.1% | 86.25 | 0.18 | |||
| X = 3000 | pos. | 92 | 2 | 94 | Specificity | 99.0% | ||
| neg. | 20 | 208 | 228 | PPV | 97.9% | |||
| 112 | 210 | 322 | NPV | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fink, B.; Hoyka, M.; Weissbarth, E.; Schuster, P.; Berger, I. The Graphical Representation of Cell Count Representation: A New Procedure for the Diagnosis of Periprosthetic Joint Infections. Antibiotics 2021, 10, 346. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040346
Fink B, Hoyka M, Weissbarth E, Schuster P, Berger I. The Graphical Representation of Cell Count Representation: A New Procedure for the Diagnosis of Periprosthetic Joint Infections. Antibiotics. 2021; 10(4):346. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040346
Chicago/Turabian StyleFink, Bernd, Marius Hoyka, Elke Weissbarth, Philipp Schuster, and Irina Berger. 2021. "The Graphical Representation of Cell Count Representation: A New Procedure for the Diagnosis of Periprosthetic Joint Infections" Antibiotics 10, no. 4: 346. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10040346