
Antibiotics Prescription by Spanish General Practitioners in Primary Dental Care

 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
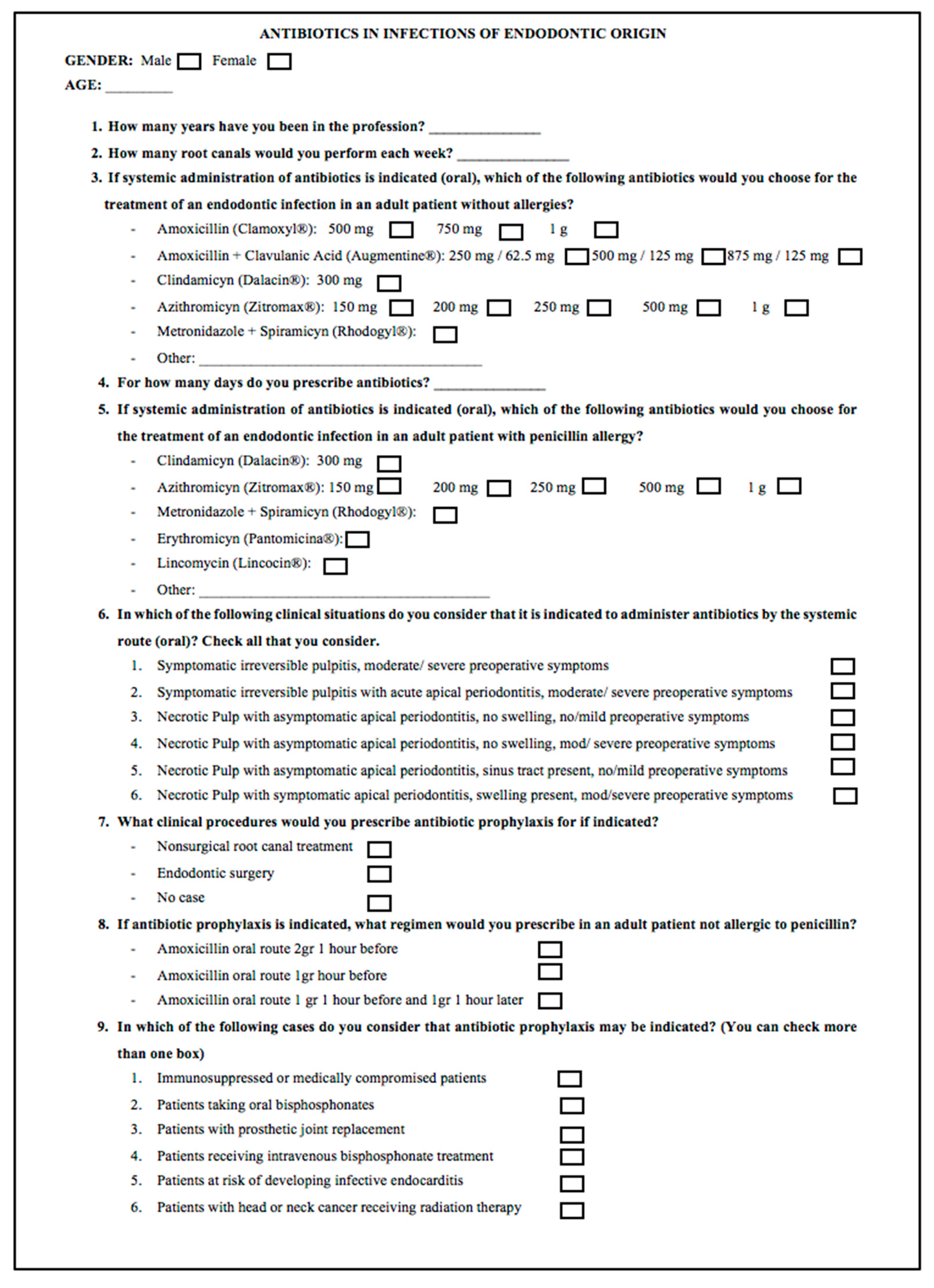
2.2. Questionnaire
2.3. Data Collection and Statistical Analysis
3. Results
3.1. Participation and Description of Respondents
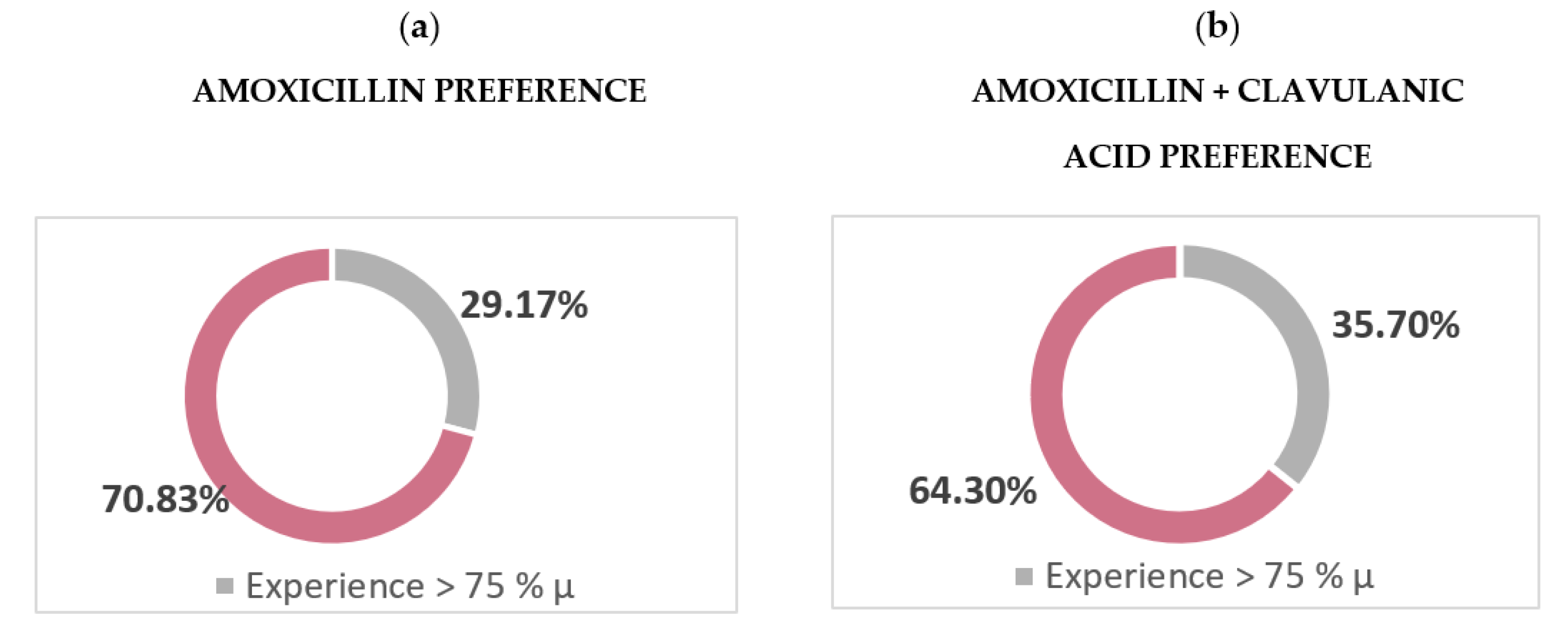
3.2. Preferred Antibiotics
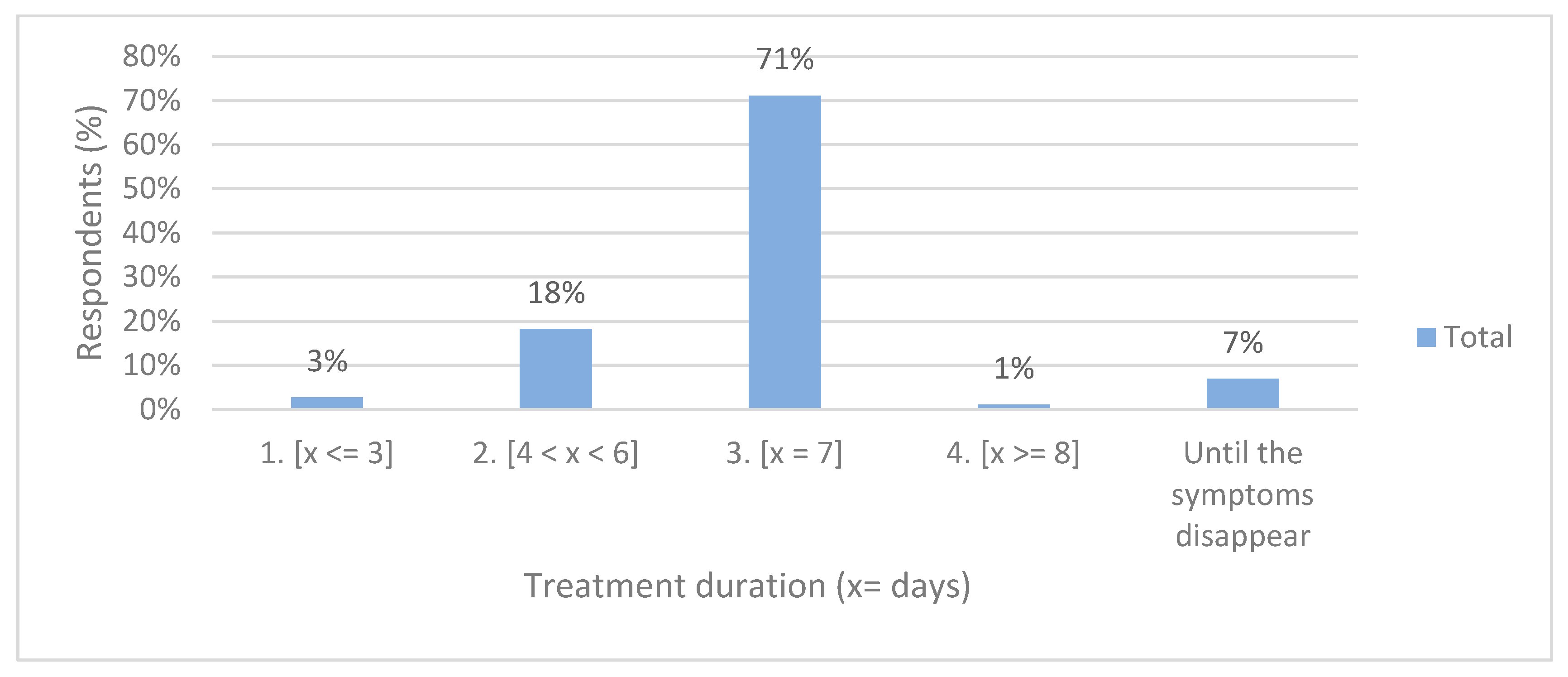
3.3. Duration of Antibiotic Treatment
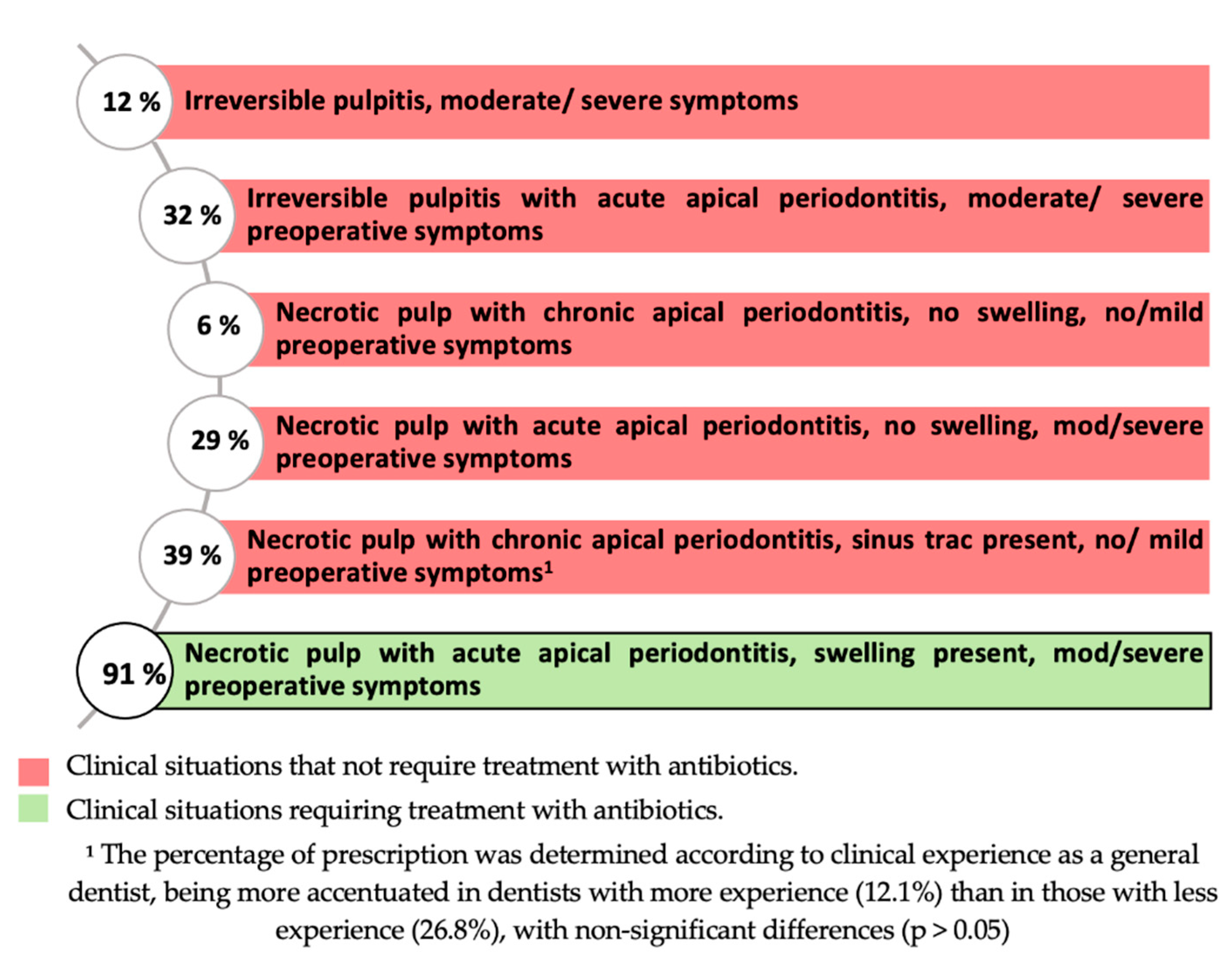
3.4. Antibiotic Prescription in Each Clinical Situation
3.5. Antibiotic Prophylaxis in Endodontics
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
References
- Rodriguez-Núñez, A.; Cisneros-Cabello, R.; Velasco-Ortega, E.; Llamas-Carreras, J.M.; Tórres-Lagares, D.; Segura-Egea, J.J. Antibiotic Use by Members of the Spanish Endodontic Society. J. Endod. 2009, 35, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Segura-Egea, J.J.; Gould, K.; Hakan, S.B.; Jonasson, P.; Cotti, E.; Mazzoni, A.; Sunay, H.; Tjaderhane, L.; Dummer, P.M.H. Antibiotics in Endodontics: A review. Int. Endod. J. 2017, 50, 1169–1184. [Google Scholar] [CrossRef] [PubMed]
- Martín-Jiménez, M.; Martín-Biedma, B.; López-López, J.; Alonso-Ezpeleta, O.; Velasco-Ortega, E.; Jiménez-Sánchez, M.C.; Segura-Egea, J.J. Dental students’ knowledge regarding the indications for antibiotics in the management of endodontic infections. Int. Endod. J. 2018, 51, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Segura-Egea, J.J.; Martín-González, J.; Jiménez-Sánchez, M.D.C.; Crespo-Gallardo, I.; Saúco-Márquez, J.J.; Velasco-Ortega, E. Worldwide pattern of antibiotic prescription in endodontic infections. Int. Dent. J. 2017, 67, 197–205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso-Ezpeleta, O.; Martín-Jiménez, M.; Martín-Biedma, B.; López-López, J.; Forner-Navarro, L.; Martín-González, J.; Montero-Miralles, P.; Jiménez-Sánchez, M.D.C.; Velasco-Ortega, E.; Segura-Egea, J.J. Use of antibiotics by spanish dentists receiving postgraduate training in endodontics. J. Clin. Exp. Dent. 2018, 10, e687–e695. [Google Scholar] [CrossRef] [PubMed]
- Segura-Egea, J.J.; Velasco-Ortega, E.; Torres-Lagares, D.; Velasco-Ponferrada, M.C.; Monsalve-Guil, L.; Llamas-Carreras, J.M. Pattern of antibiotic prescription in the management of endodontic infections amongst Spanish oral surgeons. Int. Endod. J. 2010, 43, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.A.O. Why we must reduce dental prescription of antibiotics: European Union Antibiotic Awareness Day. Br. Dent. J. 2008, 205, 537–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yingling, N.M.; Byrne, B.E.; Hartwell, G.R. Antibiotic Use by Members of the American Association of Endodontists in the Year 2000: Report of a National Survey. J. Endod. 2002, 28, 396–404. [Google Scholar] [CrossRef] [PubMed]
- Ajantha, G.S.; Hegde, V. Antibacterial drug resistance and its impact on dentistry. N. Y. State Dent. J. 2012, 78, 38–41. [Google Scholar] [PubMed]
- Segura-Egea, J.J.; Gould, K.; Şen, B.H.; Jonasson, P.; Cotti, E.; Mazzoni, A.; Sunay, H.; Tjäderhane, L.; Dummer, P.M.H. European Society of Endodontology position statement: The use of antibiotics in endodontics. Int. Endod. J. 2018, 51, 20–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Segura-Egea, J.J.; Sánchez-Domínguez, B.; Montero-Millares, P.; Martín-González, J.; Alonso-Ezpeleta, Ó.; Forner-Navarro, L. Recomendaciones de la Asociación Española de Endodoncia sobre el uso de antibióticos en endodoncia. Rev. Off. Asoc. Española Endod. 2020, 38, 7–12. [Google Scholar]
- AAE. AAE Position Statement: AAE Guidance on the Use of Systemic Antibiotics in Endodontics. Am. Assoc. Endod. 2017, 43, 1409–1413. [Google Scholar]
- Fouad, A.F.; Rivera, E.M.; Walton, R.E. Penicillin as a supplement in resolving the localized acute apical abscess. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 81, 590–595. [Google Scholar] [CrossRef]
- Mainjot, A.; D’Hoore, W.; Vanheusden, A.; Van Nieuwenhuysen, J.-P. Antibiotic prescribing in dental practice in Belgium. Int. Endod. J. 2009, 42, 1112–1117. [Google Scholar] [CrossRef] [PubMed]
- Perić, M.; Perković, I.; Romić, M.; Simeon, P.; Matijević, J.; Mehičić, G.P.; Krmek, S.J. The Pattern of Antibiotic Prescribing by Dental Practitioners in Zagreb, Croatia. Cent. Eur. J. Public Health 2015, 23, 83–89. [Google Scholar]
- Skučaitė, N.; Pečiulienė, V.; Manelienė, R.; Mačiulskienė, V. Antibiotic prescription for the treatment of endodontic pathology: A survey among Lithuanian dentists. Medicina 2010, 46, 806–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatewood, R.S.; Himel, V.T.; Dorn, S.O. Treatment of the endodontic emergency: A decade later. J. Endod. 1990, 16, 284–291. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | n (%) |
| Male | 66 (34.7%) |
| Female | 124 (65.3%) |
| Age (y) | 30.5 ± 7.8 |
| ≤30 | 125 (65.8%) |
| 30–40 | 33 (17.4%) |
| ≥40 | 31 (16.3%) |
| Experience as a dentist (months) | 74.0 ± 88.7 |
| High experience (> 75% µ) | 65 (34.2%) |
| Low experience (< 75% µ) | 125 (65.8%) |
| Number of weekly root canals | 4.3 ± 4.7 |
| Antibiotics | n (%) |
|---|---|
| Amoxicillin | |
| 500 mg | 48 (25.3%) |
| 750 mg | 30 (15.8%) |
| 1000 mg | 19 (10.0%) |
| Amoxicillin/Clavulanic acid | |
| 225/62.5 mg | 3 (1.6%) |
| 500/125 mg | 28 (14.7%) |
| 875/125 mg | 56 (29.5%) |
| Clindamicym | |
| 300 mg | 1 (0.5%) |
| Azithromicyn | 0 (0%) |
| Metronidazole/Spiramicyn | |
| 125 mg/750.000 UI | 3 (1.6%) |
| Other | 1 (0.5%) |
| Blank answer | 1 (0.5%) |
| Antibiotics | n (%) |
|---|---|
| Clindamicym | |
| 300 mg | 133 (70.0%) |
| Azithromicyn | |
| 150 mg | 4 (2.1%) |
| 200 mg | 0 (0%) |
| 250 mg | 4 (2.1%) |
| 500 mg | 22 (11.6%) |
| 1000 mg | 0 (0%) |
| Metronidazole/Spiramicyn | 14 (7.4%) |
| Erythromicyn | 9 (4.7%) |
| Lincomicyn | 0 (0%) |
| Other | 1 (0.5%) |
| Blank answer | 0 (0%) |
| Clinical Procedures | N (%) |
| Nonsurgical root canal treatment | 51 (26.8%) |
| Endodontic surgery | 153 (80.5%) |
| No case | 34 (17.9%) |
| Prophylaxis regimens in patients without medical allergies | N (%) |
| Amoxicillin oral route 2 g 1 h before | 135 (71.1%) |
| Amoxicillin oral route 1 g 1 h before 1 | 33 (17.4%) |
| Amoxicillin oral route 1 g 1 h before and 1 g 1 h later 1 | 18 (9.5%) |
| Patients with indication for antibiotic prophylaxis | N (%) |
| Immunosuppressed patients | 133 (70.0%) |
| Patient taking oral bisphosphonates 1 | 31 (16.3%) |
| Patients with prosthetic joint replacement | 84 (44.2%) |
| Patients receiving intravenous bisphosphonate treatment | 49 (25.8%) |
| Patient at risk of developing infective endocarditis | 185 (97.4%) |
| Patients with head or neck cancer receiving radiation therapy | 61 (32.1%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domínguez-Domínguez, L.; López-Marrufo-Medina, A.; Cabanillas-Balsera, D.; Jiménez-Sánchez, M.C.; Areal-Quecuty, V.; López-López, J.; Segura-Egea, J.J.; Martin-González, J. Antibiotics Prescription by Spanish General Practitioners in Primary Dental Care. Antibiotics 2021, 10, 703. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10060703
Domínguez-Domínguez L, López-Marrufo-Medina A, Cabanillas-Balsera D, Jiménez-Sánchez MC, Areal-Quecuty V, López-López J, Segura-Egea JJ, Martin-González J. Antibiotics Prescription by Spanish General Practitioners in Primary Dental Care. Antibiotics. 2021; 10(6):703. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10060703
Chicago/Turabian StyleDomínguez-Domínguez, Laura, Alfonso López-Marrufo-Medina, Daniel Cabanillas-Balsera, María Carmen Jiménez-Sánchez, Victoria Areal-Quecuty, José López-López, Juan. J. Segura-Egea, and Jenifer Martin-González. 2021. "Antibiotics Prescription by Spanish General Practitioners in Primary Dental Care" Antibiotics 10, no. 6: 703. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10060703