1. Introduction
Antibiotics are among the most commonly prescribed drug classes in developing countries such as Uganda. The rates of antibiotic prescriptions have greatly risen and are reported to be double beyond the World Health Organization (WHO) recommendation of 30%, especially in low- and middle-income countries (LMICs) [
1,
2]. The most prescribed antibiotics are the cephalosporins [
3,
4,
5,
6].
Ceftriaxone is a third-generation cephalosporin, beta-lactam antibiotic that is administered intravenously or intramuscularly for a broad range of susceptible infections. It is highly efficacious and largely safe, which underlies its popularity in clinical use in many parts of the world [
3,
7]. For instance, ceftriaxone is recommended for the treatment of over 30 conditions in the current Uganda Standard Treatment Guidelines (STGs) [
8]. It is the most commonly prescribed antibiotic for patients in hospitals, with over 80% exposure among all in-patients admitted to Mulago National Referral Hospital, Uganda [
9]. Findings from other studies in Spain, Ethiopia, Saudi Arabia, and South Korea have provided similar outlooks on ceftriaxone utilization [
3,
6,
7,
10]. Ceftriaxone is widely used in various countries for majorly surgical prophylaxis and in the management of respiratory tract infections (especially pneumonia) and urinary tract infections [
6,
7,
10,
11,
12,
13,
14].
Ceftriaxone, like most cephalosporins, has a high prevalence of inappropriate prescriptions [
3,
4,
5,
6]. Ceftriaxone has a high propensity for misuse because it is utilized in high quantities clinically and is prescribed in an uncontrolled manner in many countries including Uganda [
3,
9]. Inappropriate use of ceftriaxone is reported to occur in over 34–70% of cases [
3,
4,
10]. Furthermore, empiric use of ceftriaxone is estimated to be as high as 80–90% in hospitalized patients in some countries [
6,
15]. A cross-sectional survey previously carried out in Uganda at Mubende Regional Referral hospital on clinical utilization of ceftriaxone reported 81% inappropriate administration and no culture and sensitivity testing in over 93% of the patients sampled [
13]. Similar findings have been reported in studies carried out in other countries in Africa, Middle East, and Asia [
3,
7,
10,
12,
14,
16,
17,
18].
Inappropriate use of antibiotics such as ceftriaxone accelerates the emergence of antimicrobial resistance, increases costs of treatment, affects productivity, and exposes patients to unnecessary side effects, and can also result in death [
19,
20,
21,
22,
23]. Death rates are higher in surgical cases, especially patients who have undergone maternal cesarean section in low- and middle-income countries. The high mortality in this group is attributed to the development of post-surgical site infections that occur in 2–24% of patients, mainly as a result of inappropriate antibiotics use [
23,
24,
25,
26]. For instance, patients missing post-cesarean section antibiotic doses are 2.5 times more at risk of obtaining post-surgical site infections, and these infections can lead to death in over 5.3% of such patients [
23].
There are emerging reports of the ineffectiveness of certain antibiotics including ceftriaxone worldwide. This ineffectiveness is largely due to the escalation of antimicrobial resistance accelerated by inappropriate prescription and ineffective antimicrobial stewardship [
21,
27]. Non-susceptible organisms cause higher rates of morbidity and mortality and significantly cost more to be treated than the susceptible organisms [
3]. Worldwide, resistance to third-generation cephalosporins such as ceftriaxone is estimated to average 12% and 36% for methicillin-resistant
S. aureus and
E. coli, respectively [
20]. In East Africa, resistance to ceftriaxone among Gram-negative infections is reported to be as high as 24–69% [
28,
29]. In Uganda, for instance, multiple strains of
Klebsiella pneumoniae and
E. coli were reported to be non-susceptible to ceftriaxone in culture and sensitivity studies performed with rates of 85% and 15%, respectively [
30]. This pattern has causally been associated with several factors, most profoundly irrational use of antibiotics (overuse, misuse) and supposed low-quality antibiotics [
3,
22].
Several anecdote reports in Uganda blame the ineffectiveness of ceftriaxone on the quality of the commercially available brands on the market rather than inappropriate use. These were, however, dismissed by preliminary studies done by the National Drug Authority (NDA) on the quality of brands available on the Ugandan market that reported their conformity to pharmacopoeial standards adopted for Uganda. Ceftriaxone is in many ways an unrestricted antibiotic, and such atypical use of any antibiotic encourages the emergence of non-susceptible organisms. It can therefore be inferred that the reported cases of the inefficacy of ceftriaxone may be the result of this relationship. In the advent of these findings, a thorough assessment of the utilization of ceftriaxone in clinical settings in Uganda was the next logical step in attempting to understand the reasons for the reported inefficacy of ceftriaxone. In this study, therefore, we conducted a drug utilization evaluation (DUE) in nine (9) health facilities in Uganda to obtain a wider perspective.
3. Discussion
Our study aimed at evaluating the clinical use of ceftriaxone among in-patients in selected health facilities in Uganda based on eight (8) of the WHO’s recommended guidelines, and the overall appropriate use indicators were all below those recommended by the WHO. The WHO recommends the following indicators for drug utilization evaluation studies: indication, dose, duration, laboratory investigations, appropriate combination therapy, accurate dispensing, proper discontinuation, generic prescribing, proper continuation of therapy, and treatment outcomes [
32]. We used eight of these in our study, namely; indication, dose, duration, laboratory investigations, accurate dispensing, drug-drug interactions, generic prescribing, and treatment outcomes. The most common indications for prescribing ceftriaxone were surgical prophylaxis (trauma, labor, and pregnancy complications), RTIs (majorly pneumonia), sepsis, and GIT infections, and these were largely in agreement with those obtained in other studies performed on the African continent and beyond [
6,
7,
10,
11,
13,
14,
15]. However, in our study, surgical prophylaxis was a more common indication for which ceftriaxone was prescribed. The most prescribed dose of ceftriaxone was 2g, as was also previously reported in other related studies in Uganda, Eritrea, Saudi Arabia, and Ethiopia [
6,
10,
12,
13,
17]. The ceftriaxone dose recommended ranges from 1 to 2 g in adults and 50 to 100 mg/kg in children [
8]. The recommended dosing frequency for ceftriaxone varies from once daily to twice daily, depending on the condition, and the duration is 1 day to over 21 days, depending on treatment response [
8,
33]. The most prescribed frequency for the administration of ceftriaxone in this study was once daily (92.3%; 817/885), which was in agreement with similar studies in Tanzania [
11], Ghana [
34], and Saudi Arabia [
6], and also in Uganda, which reported 100% for once-daily administration [
13]. However, in a related study carried out in Ethiopia, twice-daily dosing was the most prescribed [
7]. The mean duration (3.87 days) over which ceftriaxone was prescribed in our study was similar to that reported in a related study conducted at one hospital in Uganda [
13]. Studies in Ethiopia and Eritrea reported a higher mean duration over which ceftriaxone was prescribed; i.e., 11.47 days [
14], 5.6 days [
17], 5.2 days [
10], and 6.79 days [
12]. In another related study carried out in 10 university hospitals in Korea, the mean duration prescribed was 10.3 days [
3]. The difference in the duration over which ceftriaxone is prescribed could be explained by the fact that these other studies were carried out at only higher tier facilities (regional referral and specialist hospitals), while our study involved both lower- and higher-tier health facilities. Higher-tier HFs usually manage referral patients, and most of these usually have conditions in more advanced stages that require longer treatment durations.
In this study, we found appropriate use significantly determined by gender, pregnancy status, days of hospitalization, facility level of care, facility type, and prescriber category. General hospitals (GH) under the level of care and private for-profit (PFP) under the type of facility had better ceftriaxone clinical use practices. Age was found not to be a significant determinant of the appropriateness of the use of ceftriaxone just like in other studies [
7,
14]. However, in these same studies, gender was reported as not being a significant determinant of the appropriateness of use of ceftriaxone, unlike in our study, wherein the appropriateness of ceftriaxone use was significantly better in male patients. Furthermore, our study found more rational clinical use of ceftriaxone among non-pregnant females as compared to pregnant ones. Just like in related studies [
7,
14], days of hospitalization were found as a significant determinant of the appropriateness of the use of ceftriaxone. In our study, inappropriate ceftriaxone use was found to be more likely in patients admitted for shorter periods (≤3 days). Furthermore, ceftriaxone prescriptions by intern doctors were more likely to be inappropriate when compared to those of most of the other prescribers. This could be due to the inadequate experience of intern doctors with the use of the STGs and possibly a desire to explore various antibiotics, including ceftriaxone. In this study, inappropriate ceftriaxone prescription by intern doctors was attributed to issues such as not specifying the duration of use of ceftriaxone, since over 22.9% of the prescriptions made by intern doctors lacked this.
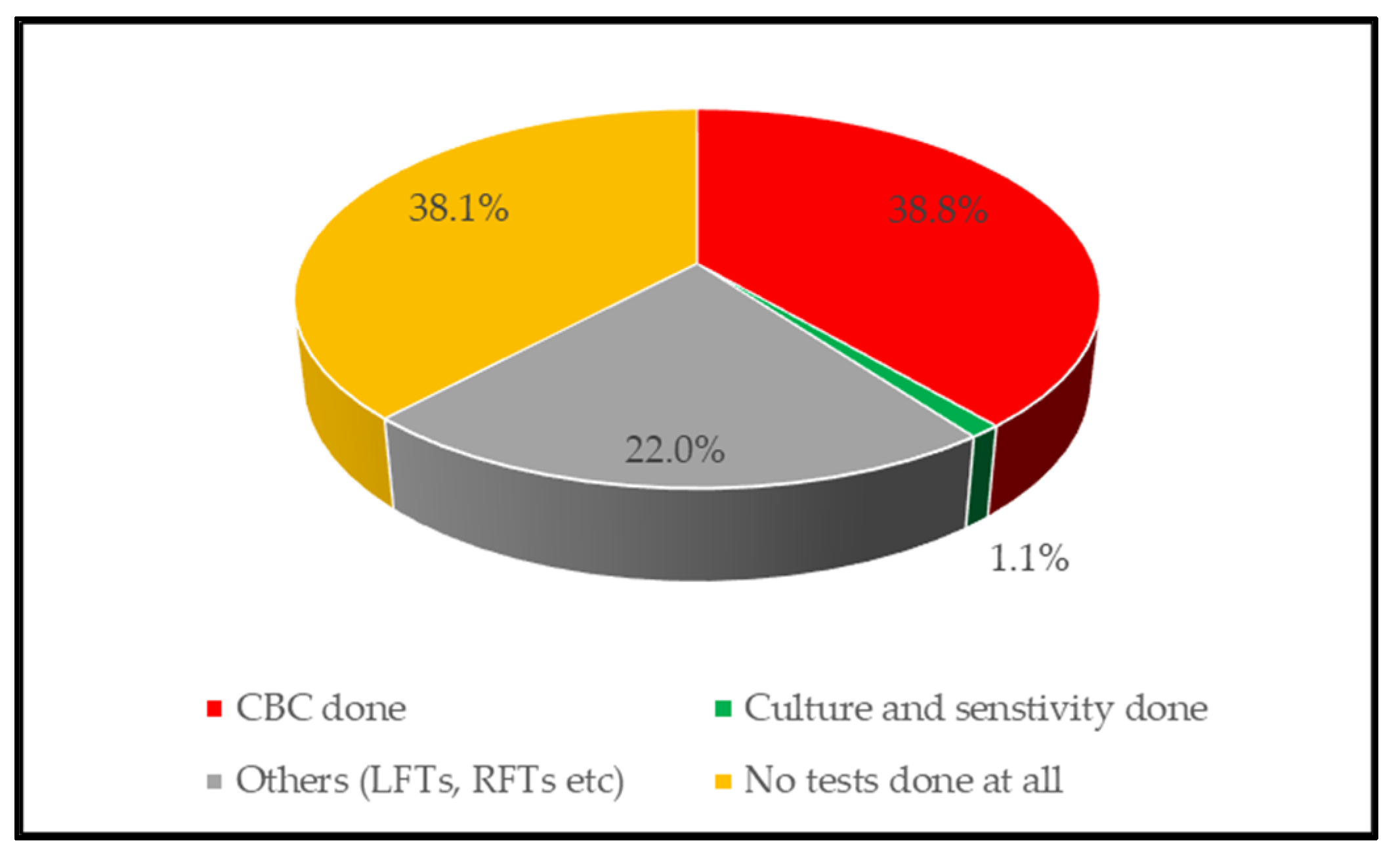
The overall inappropriate use score in our study was 32.1% and was lower than that reported in related studies in other countries. Inappropriate prescription of ceftriaxone has been determined to be at 39.4–87.9% in Ethiopia [
7,
10,
14,
17], 62.4% in Eritrea [
12], 53% in the USA [
19], and 34.5% in Korea [
3]. The differences in the score for inappropriate use could be attributed to factors such as country differences in the STGs, differences in prescribers’ qualifications and experiences, the extent of training of healthcare workers on the use of STGs, and the assessment protocols used. Inappropriate ceftriaxone use was largely due to inappropriate dispensing, inadequate laboratory testing, wrong indications, wrong doses, and wrong dose duration. Ceftriaxone was used in over 37.8% of the patients without any laboratory test performed. Furthermore, 61.2% and 98.9% of patients lacked CBC and culture and sensitivity test results, respectively. In related studies, culture and sensitivity testing was not conducted in; 93% of patients in Uganda [
13], 53.2–68.7% in Ethiopia [
7,
14], 91.1% in Sudan [
15], and 33.5% in Korea [
3]. CBC and culture and sensitivity tests are important in assessing treatment outcomes; for instance, a CBC value in normal limits (3.7–9.4 × 10
9 mm
3) [
35] while culture and sensitivity testing facilitates the selection of the most appropriate antibiotics [
27,
36,
37]. In LMICs, the capacity of clinical microbiology laboratories is very low, and even where capacity is not limited, such laboratories are underutilized [
22,
38,
39]. The inadequate capacity is majorly due to inadequate laboratory infrastructure, lack of adequately trained/qualified staff, and limited resources to procure laboratory consumables [
40,
41,
42]. In Uganda, a shortage of laboratory technologists exists in health facilities, with only 50% of posts for these filled at general hospitals. Furthermore, only 35.7% and 35.7% of laboratory technologist positions are filled at non-hub and hub hospital laboratories [
42]. Most physicians prefer not to request culture and drug sensitivity testing due to the related high costs and time delays [
12,
14,
36]. The high prevalence of lack of laboratory testing is an indicator of poor patient care management systems at these health facilities [
16]. Lack of microbiology laboratory testing escalates misdiagnosis and can result in power management of life-threatening conditions such as post-surgical site infections [
23,
25]. The challenges above call for more focus on support towards laboratory infrastructure, consumables, and laboratory human resources in line with the Antimicrobial Resistance National Action plan [
27].
The overall average inappropriate indication in this study was 16.7% and was lower than related retrospective studies carried out in Eritrea at 44% [
12] and Ethiopia at 39.4% [
10], as well as a prospective study in Ethiopia that had a score of 18.5%. It was, however, higher than that reported from other retrospective studies in Ethiopia at 4.7% [
7,
14]. Inappropriate indication in our study was attributed to some patients being treated with no diagnosis documented, as well as ceftriaxone being prescribed for non-recommended conditions. Ceftriaxone was also found to be prescribed for conditions not listed under the standard treatment guidelines [
8], for instance; malaria, anemia, peptic ulcer disease, pulmonary TB, and hypertension, among others. The drivers for this could be a lack of proper diagnostics infrastructure [
36,
41], deficiencies in knowledge among prescribers, or strive for monetary gains. Over 1.8% of patients were prescribed ceftriaxone with no diagnosis indicated. This was, however, much better than the reported prevalence from related studies in Ethiopia [
7,
16], Sudan [
15], and Tanzania [
18]. Prescribing a drug without including the diagnosis invalidates a prescription, and such a prescription should not be dispensed and administered to the patient since it makes monitoring of patients’ progress hard.
Furthermore, inappropriate utilization as regards prescribing correct doses and dose durations were 11.2% and 15.9%, respectively. The inappropriate dosing score was lower than the 45% reported in a related study in Eritrea [
12]. In addition, the score for the inappropriate duration was lower than the reported 47–71% scores in related studies in Ethiopia and Eritrea [
12,
14,
16,
17]. Most cases of inappropriate use are always due to inappropriate duration, unlike in our study where inappropriate indication was most prevalent. Injectable antibiotics such as ceftriaxone are recommended mostly for the initial management of severe infections and are they are supposed to be replaced with other alternatives when the patient’s condition improves. However, standard treatment guidelines specify given dosing frequencies and durations for some specific conditions. For instance, the UCG (2016) recommends at least 5–7 days for pneumonia, 14 days for pyelonephritis, 10–14 days for meningitis and typhoid, and 7–10 days for acute chest syndrome and acute abdomen in sickle cell disease (SCD) among others [
8].
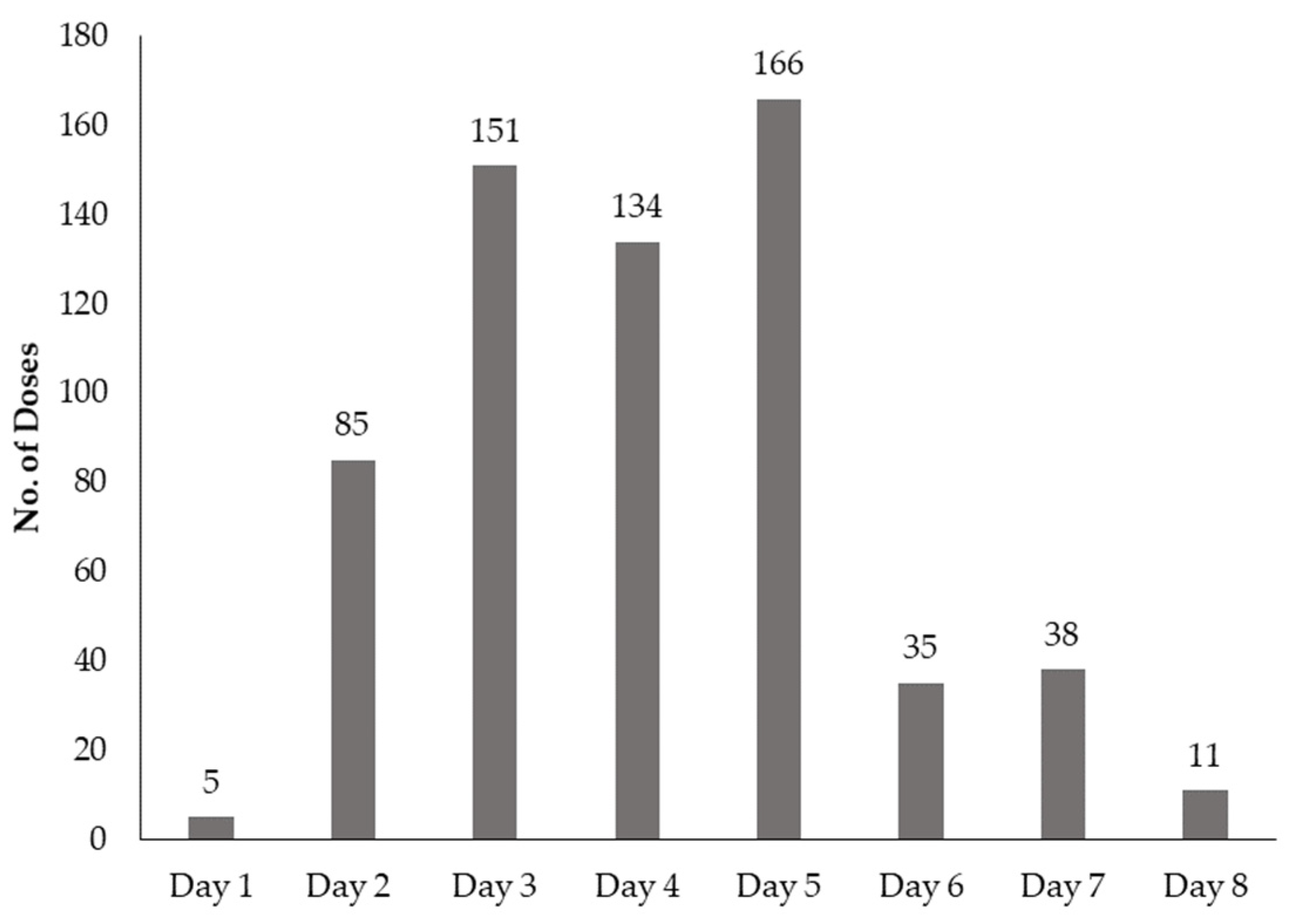
Over 85.6% of the patients were successfully discharged as having completely been treated. This figure was comparable to that reported in a previous study carried out by Manirakiza et al. (2019) in Uganda. However, the high rate of patients getting better cannot be directly attributed to the appropriateness of the use of ceftriaxone. The dismal rates of laboratory testing, with culture and sensitivity as low as 1.1% could not enable us to obtain generalizable results to make such conclusions. In our study, 5.6% of the patients were reported to have died, and this could be attributed to probably treatment failure, co-morbidities, or improper diagnosis. The possibility of occurrence of treatment failure could be justified by the fact that a very high proportion (41.7%; 369/885) of the ceftriaxone doses prescribed were not completed; culture and sensitivity testing rates were very low; and drug administration was irregular, with over 650 doses missed during the period of treatment. A related study in Uganda reported that only 18% of patients completed the prescribed doses of ceftriaxone and had regular administration [
13]. In our study, the overall score for possible interactions was 4%, and this was comparable to a related study in Sudan [
15]. Ringer’s lactate (contains calcium gluconate) was found to be prescribed alongside ceftriaxone in some cases, yet co-administration of ceftriaxone with calcium-containing products is reported to result in occasional occurrences of possible or probable embolic events [
43]. Furthermore, furosemide was also being co-administered with ceftriaxone, yet this is reported as having the potential to worsen kidney function [
44]. Co-administration of ceftriaxone with furosemide or Ringer’s lactate was also reported as being prevalent in related studies carried out in Ethiopia [
10] and Sudan [
15].



 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}