
Prognostic Role of Serum Procalcitonin Measurement in Adult Patients Admitted to the Emergency Department with Fever

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Variables
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. In-Hospital Mortality in Patients with Non-Suspected Sepsis (NSep Group)
3.3. Patients with Suspected Sepsis at ED Admission (Sep Group)
3.4. Sub-Analysis of PCT Prognostic Value According to Discharge Diagnosis
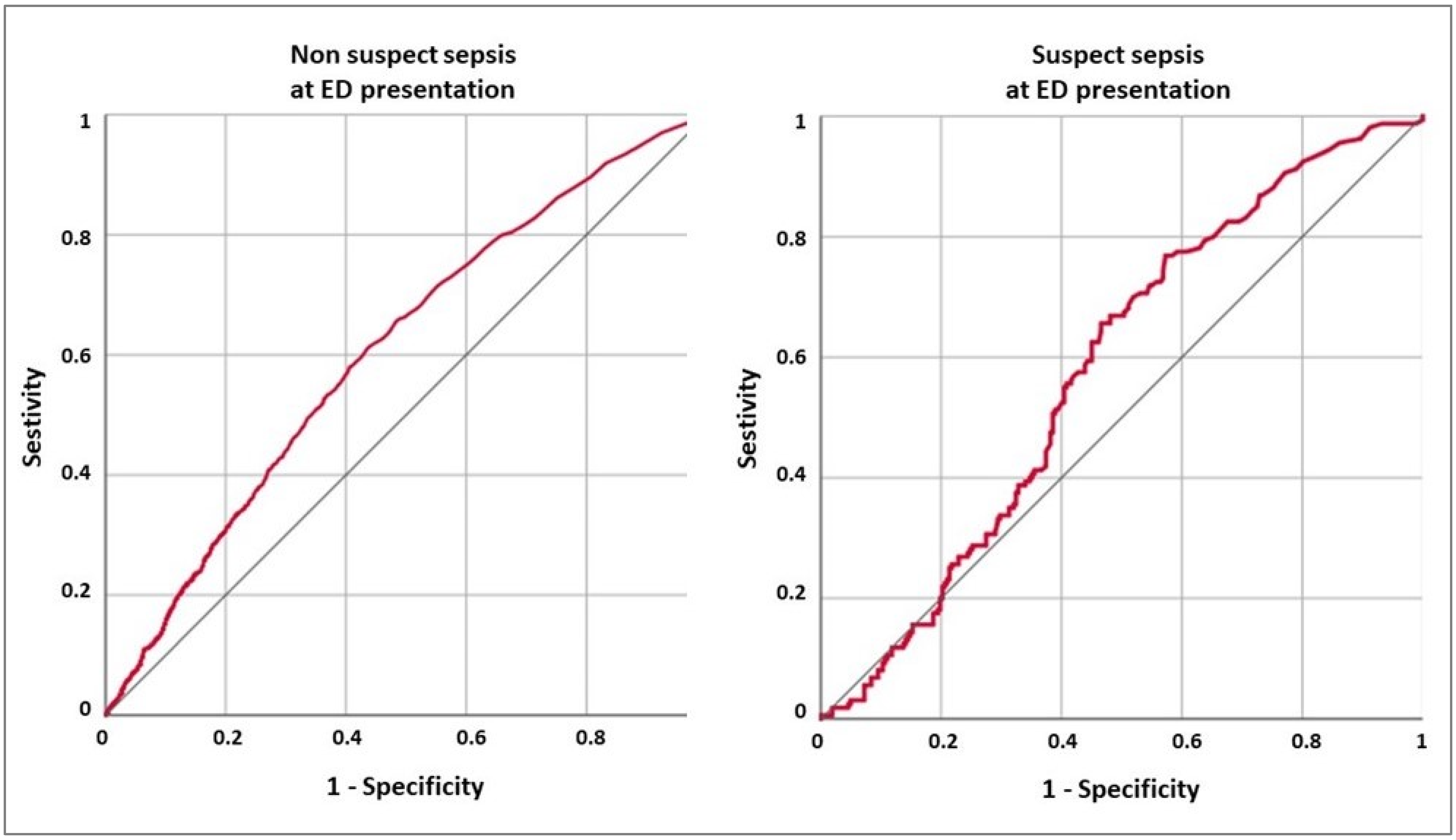
3.5. ROC Curve Analysis of PCT Value for All-Cause In-Hospital Death
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Almaie, S.M. Ability of adult patients to predict absence or presence of fever in an emergency department triage clinic. J. Fam. Community Med. 1999, 6, 29–34. [Google Scholar]
- Hatzistilianou, M. Diagnostic and Prognostic Role of Procalcitonin in Infections. Sci. World J. 2010, 10, 1941–1946. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock [Sepsis-3]. JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.J.; Song, Y.G.; Kim, C.O.; Kim, H.W.; Ku, N.S.; Han, S.H.; Choi, J.Y.; Kim, J.M. Measurement of plasma sTREm-1 in patients with severe sepsis receiving early early goal directed therapy and evaluation of its usefulness. Shock 2012, 37, 574–578. [Google Scholar] [CrossRef]
- Hausfater, P. Biomarkers and infection in the emergency unit. Med. Mal. Infect. 2014, 44, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Jekarl, D.W.; Kim, J.Y.; Lee, S.; Kim, M.; Kim, Y.; Han, K.; Woo, S.H.; Lee, W.J. Diagnosis and evaluation of severity of sepsis via the use of biomarkers and profiles of 13 cytokine: A multiplex analysis. Clin. Med. Lab. Med. 2015, 53, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Covino, M.; Manno, A.; Merra, G.; Simeoni, B.; Piccioni, A.; Carbone, L.; Forte, E.; Ojetti, V.; Franceschi, F.; Murri, R. Reduced utility of early procalcitonin and blood culture determination in patients with febrile urinary tract infections in the emergency department. Intern. Emerg. Med. 2019, 15, 119–125. [Google Scholar] [CrossRef]
- Covino, M.; Piccioni, A.; Bonadia, N.; Onder, G.; Sabia, L.; Carbone, L.; Candelli, M.; Ojetti, V.; Murri, R.; Franceschi, F. Early procalcitonin determination in the emergency department and clinical outcome of community-acquired pneumonia in old and oldest old patients. Eur. J. Intern. Med. 2020, 79, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Rıos-Toro, J.J.; Marquez-Coello, M.; Marıa Garcıa-Alvarez, J.M.; Martın-Aspas, A.; Rivera-Fernandez, R.; Saez de Be-nito, A.; Giron Gonzalez, J.A. Soluble membrane receptors, interleukin 6, procalcitonin and C reactive protein as prognostic markers in patients with severe sepsis and septic shock. PLoS ONE 2017, 12, e0175254. [Google Scholar] [CrossRef]
- Assicot, M.; Gendrel, D.; Carsin, H.; Raymond, J.; Guilbaud, J.; Bohuon, C. High serum procalcitonin concentration in patients with sepsis and infection. Lancet 1993, 341, 515–518. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nun-nally, M.E.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock of 2016. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.U.; Heslet, L.; Jensen, T.H.; Espersen, K.; Steffensen, P.; Tvede, M. Procalcitonin increase in early identificartion of critically ill patients at high risk of mortality. Crit. Care Med. 2006, 34, 2596–2602. [Google Scholar] [CrossRef] [PubMed]
- Covino, M.; Gallo, A.; Montalto, M.; De Matteis, G.; Burzo, M.; Simeoni, B.; Murri, R.; Candelli, M.; Ojetti, V.; Franceschi, F. The Role of Early Procalcitonin Determination in the Emergency Department in Adults Hospitalized with Fever. Medicina 2021, 57, 179. [Google Scholar] [CrossRef]
- Covino, M.; Fransvea, P.; Rosa, F.; Cozza, V.; Quero, G.; Simeoni, B.; Gasbarrini, A.; Alfieri, S.; Franceschi, F.; Sganga, G. Early Procalcitonin Assessment in the Emergency Department in Patients with Intra-Abdominal Infection: An Excess or a Need? Surg. Infect. 2021. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Singh, P.; Sing, P.M.; Trikha, A. Procalcitonin levels in survivors and non survivors of sepsis: Systematic review and meta-analysis. Shock 2015, 43, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Zaccone, V.; Falsetti, L.; Nitti, C.; Gentili, T.; Marchetti, A.; Piersantelli, M.N.; Sampaolesi, M.; Riccomi, F.; Raponi, A.; Salvi, A. The Prognostic Role of Procalcitonin in Critically Ill Patients Admitted in a Medical Stepdown Unit: A Retrospective Cohort Study. Sci. Rep. 2020, 10, 4531–4538. [Google Scholar] [CrossRef]
- Yunus, I.; Fasih, A.; Wang, Y. The use of procalcitonin in the determination of severity of sepsis, patient outcomes and infection characteristics. PLoS ONE 2018, 13, e0206527. [Google Scholar] [CrossRef]
- Ryoo, S.M.; Han, K.S.; Ahn, S.; Shin, T.G.; Hwang, S.Y.; Chung, S.P.; Hwang, Y.J.; Park, Y.S.; Jo, Y.H.; Chang, H.L.; et al. The usefulness of C-reactive protein and procalcitonin to predict prognosis in septic shock patients: A multicenter prospective registry-based observational study. Sci. Rep. 2019, 9, 6579. [Google Scholar] [CrossRef]
- Tosoni, A.; Paratore, M.; Piscitelli, P.; Addolorato, G.; De Cosmo, S.; Mirijello, A.; on behalf of the Internal Medicine Sepsis Study Group. The use of procalcitonin for the management of sepsis in Internal Medicine wards: Current evidence. Panminerva Med. 2020, 62, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Azzini, A.M.; Dorizzi, R.M.; Sette, P.; Vecchi, M.; Coledan, I.; Righi, E.; Tacconelli, E. A 2020 review on the role of procalci-tonin in different clinical settings: An update conducted with the tools of the Evidence Based Laboratory Medicine. Ann. Transl. Med. 2020, 8, 610–624. [Google Scholar] [CrossRef]
- Dong, R.; Wan, B.; Lin, S.; Wang, M.; Huang, J.; Wu, Y.; Wu, Y.; Zhang, N.; Zhu, Y. Procalcitonin and Liver Disease: A Litera-ture Review. J. Clin. Transl. Hepatol. 2019, 7, 51–55. [Google Scholar]
- Buratti, T.; Ricevuti, G.; CPechlaner, C.; Joannidis, M.; Wiedermann, F.J.; Gritti, D.; Herold, M.; Wiedermann, C.J. Plasma levels of procalcitonin and interleukin-6 in acute myocardial infarction. Inflammation 2001, 25, 97–100. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Hausfater, P.; Juillien, G.; Madona-Py, B.; Haroche, J.; Bernard, M.; Riou, B. Serum procalcitonin measurement as diagnos-tic and prognostic marker in febrile adult patients presenting to the emergency department. Crit. Care 2007, 11, R60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hausfater, P.; Garric, S.; Ayed, S.B.; Rosenheim, M.; Bernard, M.; Riou, B. Usefulness of procalcitonin as a marker os systemic in emergency department patients: A prospective study. Clin. Infect. Dis. 2002, 34, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Viallon, A.; Guyomarc’h, S.; Marjollet, O.; Berger, C.; Carricajo, A.; Robert, F.; Laporte, S.; Lambert, C.; Page, Y.; Zéni, F.; et al. Can emergency phisicians identify a high mortality subgroup of patients with septis: Role of procalcitonin. Eur. J. Emerg. Med. 2008, 15, 26–33. [Google Scholar] [CrossRef]
- Magrini, L.; Travaglino, F.; Marino, R.; Ferri, E.; De Berardinis, B.; Cardelli, P.; Salerno, G.; Di Somma, S. Procalcitonin varia-tions after Emergency Department admission are higly predictive of hospital mortality in patients with acute infectious diseases. Eur. Rev. Med. Pharmacol. Sci. 2013, 17, 133–142. [Google Scholar] [PubMed]
- Zhao, Y.; Li, C.; Jia, Y. Evaluation of the Mortality in Emergency Department Sepsis score combined with procalcitonin in septic patients. Am. J. Emerg. Med. 2013, 31, 1086–1091. [Google Scholar] [CrossRef]
- Kenzaka, T.; Okayama, M.; Kuroki, S.; Fukui, M.; Yahata, S.; Hayashi, H.; Kitao, A.; Kajii, E.; Hashimoto, M. Use of a semi-quantitative procalcitoni kit for evaluating severity and predicting mortality in patients with sepsis. Int. J. Gen. Med. 2012, 55, 483–488. [Google Scholar] [CrossRef]
- Saeed, K.; Wilson, D.C.; Bloos, F.; Schuetz, P.; van der Does, Y.; Melander, O.; Hausfater, P.; Legramante, J.M.; Claessens, Y.-E.; Amin, D.; et al. The early identification of disease progression in patients with suspected infection presenting to the emergency department: A multi-centre derivation and validation study. Crit. Care 2019, 23, 1–15, Erratum in: Crit. Care 2019, 23, 255. [Google Scholar] [CrossRef] [Green Version]
- Rivers, E.; Nguyen, B.; Havstad, S.; Ressler, J.; Muzzin, A.; Knoblich, B.; Peterson, E.; Tomlanovich, M. Early goal–directed therapy in the treatment of severe sepsis and septic shock. N. Engl. J. Med. 2001, 345, 1368–1377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fantoni, M.; Taddei, E.; Cauda, R.; Incalzi, R.A.; Capone, A.; Cortese, F.; Sanguinetti, M.; Spandonaro, F.; Urbani, A.; Murri, R. The role of procalcitonin outside of the Intensive Care Unit (ICU): A multidisciplinary approach. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 2978–2985. [Google Scholar] [PubMed]
- van der Does, Y.; Limper, M.; Jie, K.E.; Schuit, S.C.E.; Jansen, H.; Pernot, N.; van Rosmalen, J.; Poley, M.J.; Ramakers, C.; Patka, P.; et al. Procalcitonin-guided antibiotic therapy in patients with fever in a general emer-gency department population: A multicentre non-inferiority randomized clinical trial [HiTEMP study]. Clin. Micro-Biol. Infect. 2018, 24, 1282–1289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westwood, M.; Ramaekers, B.; Whiting, P.; Tomini, F.; Joore, M.; Armstrong, N.; Ryder, S.; Stirk, L.; Severens, J.; Kleijnen, J. Pro-calcitonin testing to guide antibiotic therapy for the treatment of sepsis in intensive care settings and for suspected bacterial infection in emergency department settings: A systematic review and cost-effectiveness analysis. Health Technol. Assess. 2015, 19, 1–236. [Google Scholar] [PubMed] [Green Version]
- Huang, D.T.; Yealy, D.M.; Filbin, M.R.; Brown, A.M.; Chang, C.H.; Doi, Y.; Donnino, M.W.; Fine, J.; Fine, M.J.; Fischer, M.A.; et al. Procalciton-in-Guided Use of Antibiotics for Lower Respiratory Tract Infection. N. Engl. J. Med. 2018, 379, 236–249. [Google Scholar] [CrossRef] [Green Version]
- Wirz, Y.; Meier, M.A.; Bouadma, L.; Luyt, C.E.; Wolff, M.; Chastre, J.; Tubach, F.; Schroeder, S.; Nobre, V.; Annane, D.; et al. Effect of procalcitonin-guided antibiotic treatment on clinical outcomes in intensive care unit patients with infection and sepsis patients: A patient-level meta-analysis of randomized trials. Crit. Care 2018, 22, 1–11. [Google Scholar] [CrossRef] [Green Version]
- de Jong, E.; van Oers, J.A.; Beishuizen, A.; Vos, P.; Vermeijden, W.J.; Haas, L.E.; Loef, B.G.; Dormans, T.; van Melsen, G.C.; Kluiters, Y.C.; et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: A randomised, controlled, open-label trial. Lancet Infect Dis. 2016, 16, 819–827. [Google Scholar] [CrossRef]
- Yu, H.; Nie, L.; Liu, A.; Wu, K.; Hsein, Y.-C.; Yen, D.W.; Lee, M.-T.G.; Lee, C.-C. Combining procalcitonin with the qSOFA and sepsis mortality prediction. Medicine 2019, 98, e15981. [Google Scholar] [CrossRef]
- Schuetz, P.; Falsey, A.R. Procalcitonin in patients with fever: One approach does not fit all. Clin. Microbiol. Infect. 2018, 24, 1229–1230. [Google Scholar] [CrossRef] [Green Version]
- Alba, G.A.; Truong, Q.A.; Gaggin, H.K.; Gandhi, P.U.; De Berardinis, B.; Magrini, L. Global Research on Acute Conditions Team [GREAT] Network. Diagnostic and Prognostic Utility of Procalcitonin in Patients Presenting to the Emergency Department with Dyspnea. Am. J. Med. 2016, 129, 96–104. [Google Scholar] [CrossRef] [Green Version]
- Makam, A.N.; Auerbach, A.D.; Steinman, M.A. Blood culture use in the emergency department in patients hospitalized for community acquired pneumonia. JAMA Intern. Med. 2014, 174, 803–806. [Google Scholar] [CrossRef] [Green Version]
- Möckel, M.; Searle, J.; Maisel, A. The role of procalcitonin in acute heart failure patients. ESC Hear. Fail. 2017, 4, 203–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, D.; Su, L.; Han, G.; Yan, P.; Xie, L. Prognostic Value of Procalcitonin in Adult Patients with Sepsis: A Systematic Re-view and Meta-Analysis. PLoS ONE 2015, 10, e0129450. [Google Scholar] [CrossRef] [PubMed]
- Viasus, D.; Del Rio-Pertuz, G.; Simonetti, A.F.; Garcia-Vidal, C.; Acosta-Reyes, J.; Garavito, A.; Carratala, J. Biomarkers for predicting short-term mortality in community-acquired pneumonia: A systematic review and meta-analysis. J. Infect. 2016, 72, 273–282. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | All Patients n = 6595 | NSep n = 6173 | Sep n = 422 | p |
|---|---|---|---|---|
| Age | 71 [58–81] | 71 [58–81] | 79 [68–86] | <0.001 |
| Sex (Male) | 3734 (55.6) | 3518 (57.0) | 216 (51.2) | 0.020 |
| PCT > 0.5 ng/mL | 2866 (43.5) | 2630 (42.6) | 236 (55.9) | <0.001 |
| PCT value | 0.38 [0.14–1.78] | 0.36 [0.14–1.65] | 0.71 [0.23–5.61] | <0.001 |
| Emergency Department Presentation | ||||
| Dyspnea | 1571 (23.8) | 1370 (22.2) | 201 (47.6) | <0.001 |
| Cough | 442 (6.7) | 416 (6.7) | 26 (6.2) | 0.646 |
| Abdominal pain | 1051 (16.7) | 1028 (16.6) | 23 (5.5) | <0.001 |
| Vomiting | 704 (10.7) | 676 (11.0) | 28 (6.6) | 0.005 |
| Diarrhea | 425 (6.4) | 403 (6.5) | 22 (5.2) | 0.287 |
| Neurological symptoms | 285 (4.3) | 272 (4.4) | 13 (3.1) | 0.195 |
| Syncope | 296 (4.5) | 276 (4.5) | 20 (4.7) | 0.797 |
| Malaise/asthenia | 851 (12.9) | 806 (13.1) | 45 (10.7) | 0.156 |
| Vital Parameters | ||||
| Heart rate | 94 [80–110] | 94 [80–110] | 93 [76–111] | 0.279 |
| Respiratory rate | 19 [15–20] | 19 [15–20] | 21 [20–25] | <0.001 |
| GCS | 15 [15–15] | 15 [15–15] | 14 [13–15] | <0.001 |
| Systolic BP | 122 [107–140] | 123 [110–140] | 90 [80–115] | <0.001 |
| Diastolic BP | 72 [61–82] | 73 [63–83] | 60 [50–70] | <0.001 |
| SaO2 | 96 [93–98] | 96 [93–98] | 89 [85–92] | <0.001 |
| Comorbidities | ||||
| Charlson Index | 5 [3–7] | 5 [3–7] | 6 [4–8] | <0.001 |
| Severe obesity | 135 (2.0) | 121 (2.0) | 14 (3.3) | 0.057 |
| Hypertension | 1895 (28.7) | 1761 (28.5) | 134 (31.8) | 0.157 |
| CAD | 1102 (16.7) | 1022 (16.6) | 80 (19.0) | 0.201 |
| Heart failure | 1250 (19.0) | 1131 (18.3) | 119 (28.2) | <0.001 |
| PVD | 1452 (22.0) | 1326 (21.5) | 126 (29.9) | <0.001 |
| Dementia | 422 (6.4) | 237 (5.3) | 185 (8.8) | <0.001 |
| COPD | 938 (14.2) | 838 (13.6) | 100 (23.7) | <0.001 |
| Diabetes | 1461 (22.2) | 1344 (21.8) | 117 (27.7) | 0.004 |
| CKD | 1480 (22.4) | 1351 (21.9) | 129 (30.6) | <0.001 |
| Leukemia/lymphoma | 545 (8.3) | 517 (8.4) | 28 (6.6) | 0.209 |
| Malignancy | 1789 (27.1) | 1708 (27.7) | 81 (19.2) | <0.001 |
| Outcomes | ||||
| Mechanical Ventilation | 584 (8.9) | 518 (8.4) | 66 (15.6) | <0.001 |
| Death | 1161 (17.6) | 1001 (16.2) | 160 (37.9) | <0.001 |
| Length of hospital stay | 10.6 [6.5–18.5] | 10.6 [6.5–18.5] | 10.9 [5.9–18.4] | 0.461 |
| Variable | Survived n = 5172 | Deceased n = 1001 | Univar. p | Hazard Ratio | Multiv. p |
|---|---|---|---|---|---|
| Age | 70 [56–80] | 78 [68–85] | <0.001 | 1.03 [1.02–1.03] | <0.001 |
| Sex (Male) | 2950 (57.0) | 568 (56.7) | 0.863 | ||
| PCT > 0.5 ng/mL | 2063 (39.9) | 567 (56.6) | <0.001 | 1.80 [1.59–2.59] | <0.001 |
| PCT value | 0.33 [0.13–1.45] | 0.73 [0.23–3.66] | <0.001 | ||
| Charlson Index | 5 [3–7] | 6 [4.5–8] | <0.001 | ||
| Severe obesity | 102 (2.0) | 19 (1.9) | 0.877 | ||
| Hypertension | 1498 (29.0) | 263 (26.3) | 0.084 | ||
| CAD | 804 (15.5) | 218 (21.8) | <0.001 | 1.11 [0.92–1.33] | 0.284 |
| Heart failure | 833 (16.1) | 298 (29.8) | <0.001 | 1.43 [1.23–1.24] | <0.001 |
| PVD | 1054 (20.4) | 272 (27.2) | <0.001 | 0.95 [0.80–1.13] | 0.587 |
| Dementia | 232 (4.5) | 78 (7.8) | <0.001 | 1.25 [1.02–1.52] | 0.028 |
| COPD | 694 (13.4) | 144 (14.4) | 0.413 | ||
| Diabetes | 1107 (21.4) | 237 (23.7) | 0.111 | ||
| CKD | 1045 (20.2) | 306 (30.6) | <0.001 | 1.10 [0.96–1.27] | 0.170 |
| Leukemia/lymphoma | 412 (8.0) | 105 (10.5) | 0.008 | 1.24 [1.09–1.43] | 0.002 |
| Malignancy | 1410 (27.3) | 298 (29.8) | 0.104 |
| Variable | Survived n = 262 | Deceased n = 160 | Univar. p | Hazard Ratio | Multiv. p |
|---|---|---|---|---|---|
| Age | 78 [68–85] | 82 [70–87] | 0.003 | 1.02 [1.01–1.04] | 0.003 |
| Sex (Male) | 131 (50.0) | 85 (53.1) | 0.533 | ||
| PCT > 0.5 ng/mL | 129 (49.2) | 107 (66.9) | <0.001 | 1.77 [1.27–2.48] | 0.001 |
| PCT value | 0.49 [0.17–4.93] | 1.11 [0.34–6.56] | 0.006 | ||
| Charlson Index | 6 [4–8] | 7 [5–9] | 0.003 | ||
| Severe obesity | 10 (3.8) | 4 (2.5) | 0.582 | ||
| Hypertension | 86 (32.8) | 48 (30.0) | 0.545 | ||
| CAD | 44 (16.8) | 36 (22.5) | 0.147 | ||
| Heart failure | 63 (24.0) | 56 (35.0) | 0.015 | 1.34 [0.95–1.88] | 0.097 |
| PVD | 74 (28.2) | 52 (32.5) | 0.354 | ||
| Dementia | 36 (13.7) | 16 (10.0) | 0.257 | ||
| COPD | 62 (23.7) | 38 (23.8) | 0.984 | ||
| Diabetes | 63 (24.0) | 54 (33.8) | 0.031 | 1.25 [0.89–1.74] | 0.187 |
| CKD | 69 (26.3) | 60 (37.5) | 0.016 | 1.21 [0.87–1.69] | 0.264 |
| Leukemia/lymphoma | 17 (6.5) | 11 (6.9) | 0.877 | ||
| Malignancy | 47 (17.9) | 34 (21.3) | 0.402 |
| Variable | Total Deceased | Deceased in PCT ≤ 0.5 ng/mL | Deceased in PCT > 0.5 ng/mL | p Value |
|---|---|---|---|---|
| Non-Septic Presentation in the ED | n = 1001 | n = 434 | n = 567 | |
| Pneumonia | 235 (23.5) | 116 (26.7) | 119 (21.0) | 0.034 |
| Abdominal infection | 67 (6.7) | 20 (4.6) | 47 (8.3) | 0.021 |
| Urinary tract infection | 55 (5.5) | 25 (5.8) | 30 (5.3) | 0.747 |
| Bloodstream infection | 346 (34.6) | 110 (25.3) | 236 (41.6) | <0.001 |
| Other infections | 40 (4.0) | 19 (4.4) | 21 (3.7) | 0.589 |
| Any infective diagnosis | 574 (57.3) | 225 (51.8) | 349 (61.6) | 0.002 |
| Cut-Off Value | Sensitivity | Specificity | Positive Predictive Value (PPV) | Negative Predictive Value (NPV) |
|---|---|---|---|---|
| >0.05 ng/mL | 98.2 [97.2–98.9] | 4.3 [3.8–4.9] | 16.6 [16.4–16.7] | 92.5 [88.5–95.2] |
| >0.5 ng/mL | 56.6 [53.5–59.7] | 60.1 [58.8–61.5] | 21.6 [20.5–22.7] | 87.8 [86.9–88.5] |
| >1 ng/mL | 42.6 [39.6–45.8] | 71.2 [69.9–72.4] | 22.3 [20.9–23.8] | 86.5 [85.8–87.2] |
| Cut-Off Value | Sensitivity | Specificity | Positive Predictive Value (PPV) | Negative Predictive Value (NPV) |
|---|---|---|---|---|
| >0.05 ng/mL | 98.7 [95.6–100.0] | 1.1 [0.2–3.3] | 37.9 [37.4–38.4] | 60.0 [20.2–89.9] |
| >0.5 ng/mL | 66.9 [59.0–74.1] | 50.8 [44.5–57.0] | 45.3 [41.3–49.4] | 71.5 [66.1–76.3] |
| >1 ng/mL | 51.2 [43.2–59.2] | 61.1 [54.9–67.0] | 44.6 [39.4–49.9] | 67.2 [63.0–71.2] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Covino, M.; Manno, A.; De Matteis, G.; Taddei, E.; Carbone, L.; Piccioni, A.; Simeoni, B.; Fantoni, M.; Franceschi, F.; Murri, R. Prognostic Role of Serum Procalcitonin Measurement in Adult Patients Admitted to the Emergency Department with Fever. Antibiotics 2021, 10, 788. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070788
Covino M, Manno A, De Matteis G, Taddei E, Carbone L, Piccioni A, Simeoni B, Fantoni M, Franceschi F, Murri R. Prognostic Role of Serum Procalcitonin Measurement in Adult Patients Admitted to the Emergency Department with Fever. Antibiotics. 2021; 10(7):788. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070788
Chicago/Turabian StyleCovino, Marcello, Alberto Manno, Giuseppe De Matteis, Eleonora Taddei, Luigi Carbone, Andrea Piccioni, Benedetta Simeoni, Massimo Fantoni, Francesco Franceschi, and Rita Murri. 2021. "Prognostic Role of Serum Procalcitonin Measurement in Adult Patients Admitted to the Emergency Department with Fever" Antibiotics 10, no. 7: 788. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070788