
Antimicrobial Prescribing in the Emergency Department; Who Is Calling the Shots?

Abstract
:1. Introduction
2. Methods
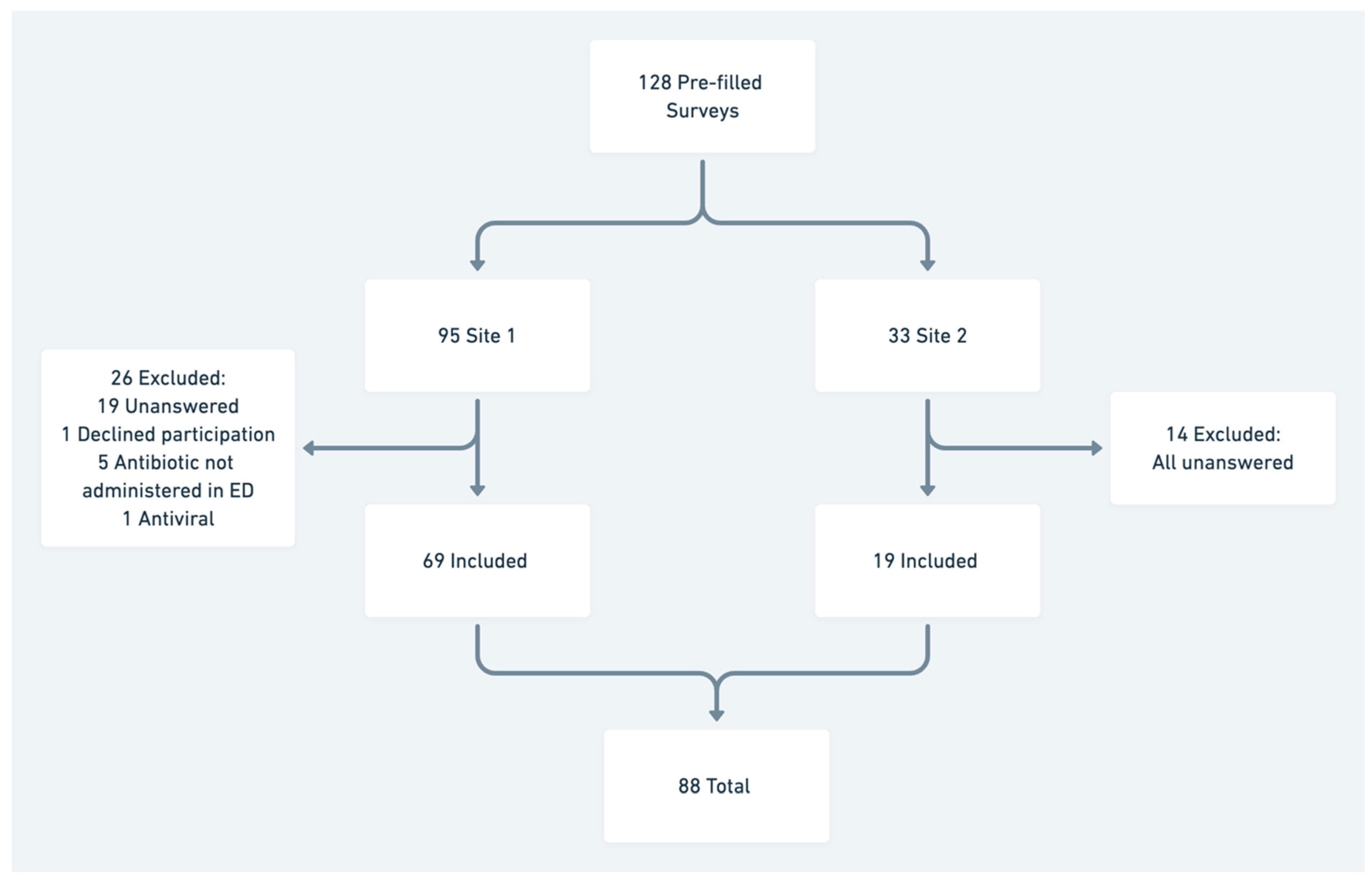
2.1. Design, Setting and Participants
2.2. Questionnaire Design and Data Collection
2.3. Assessment of Appropriateness
2.4. Data Analysis
3. Results
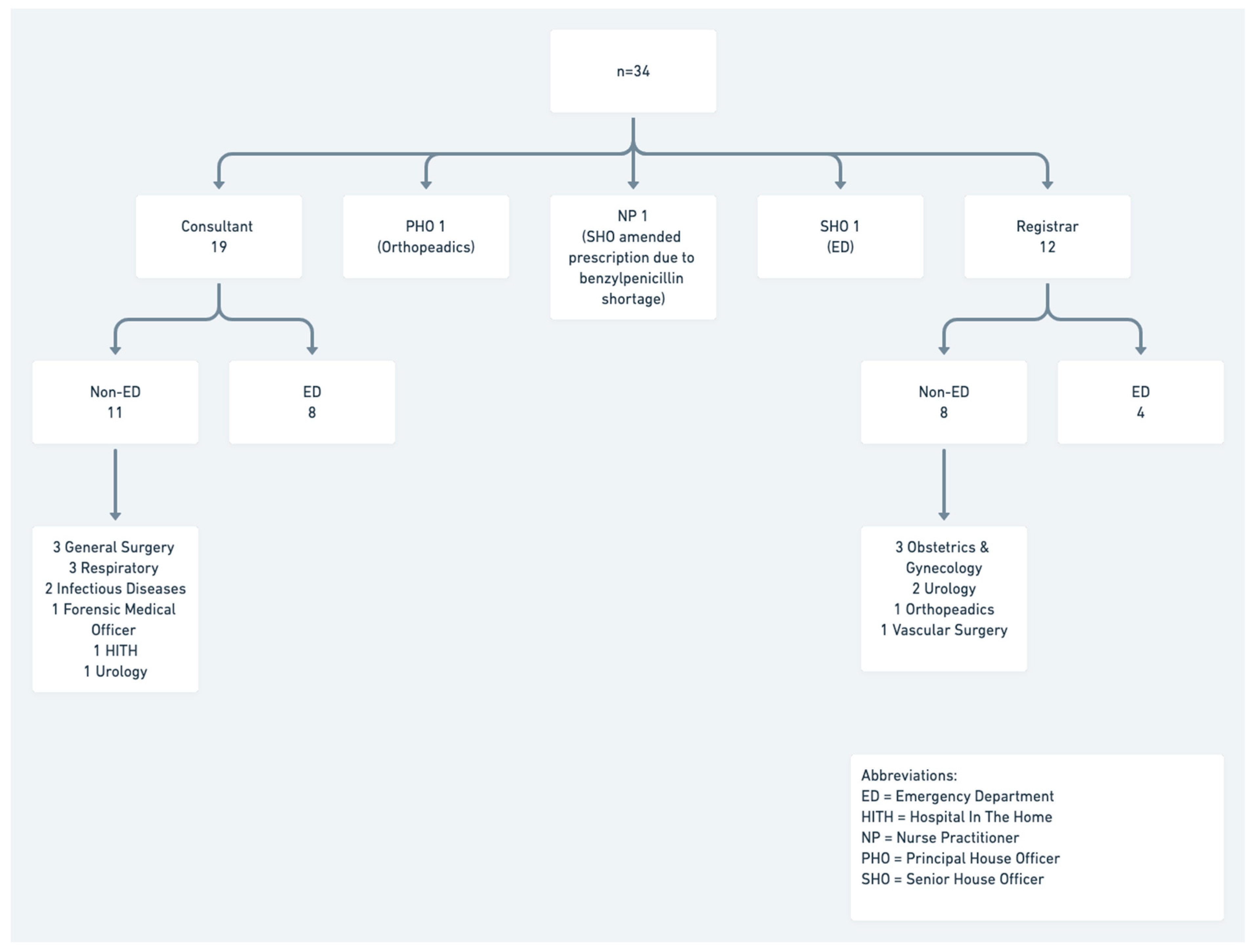
3.1. Seniority and Specialty of Prescribing Decision-Making
3.2. Resource Use
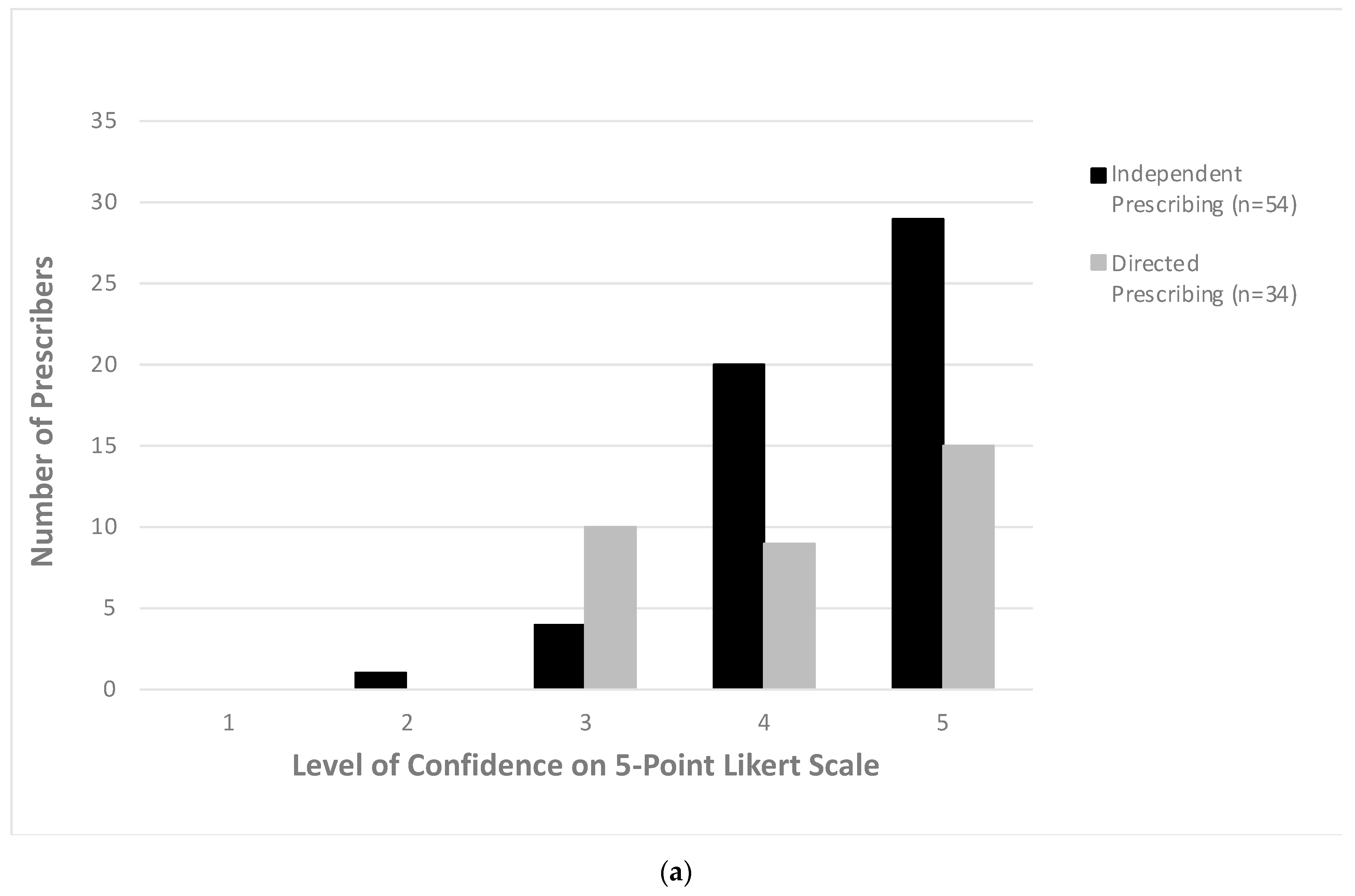
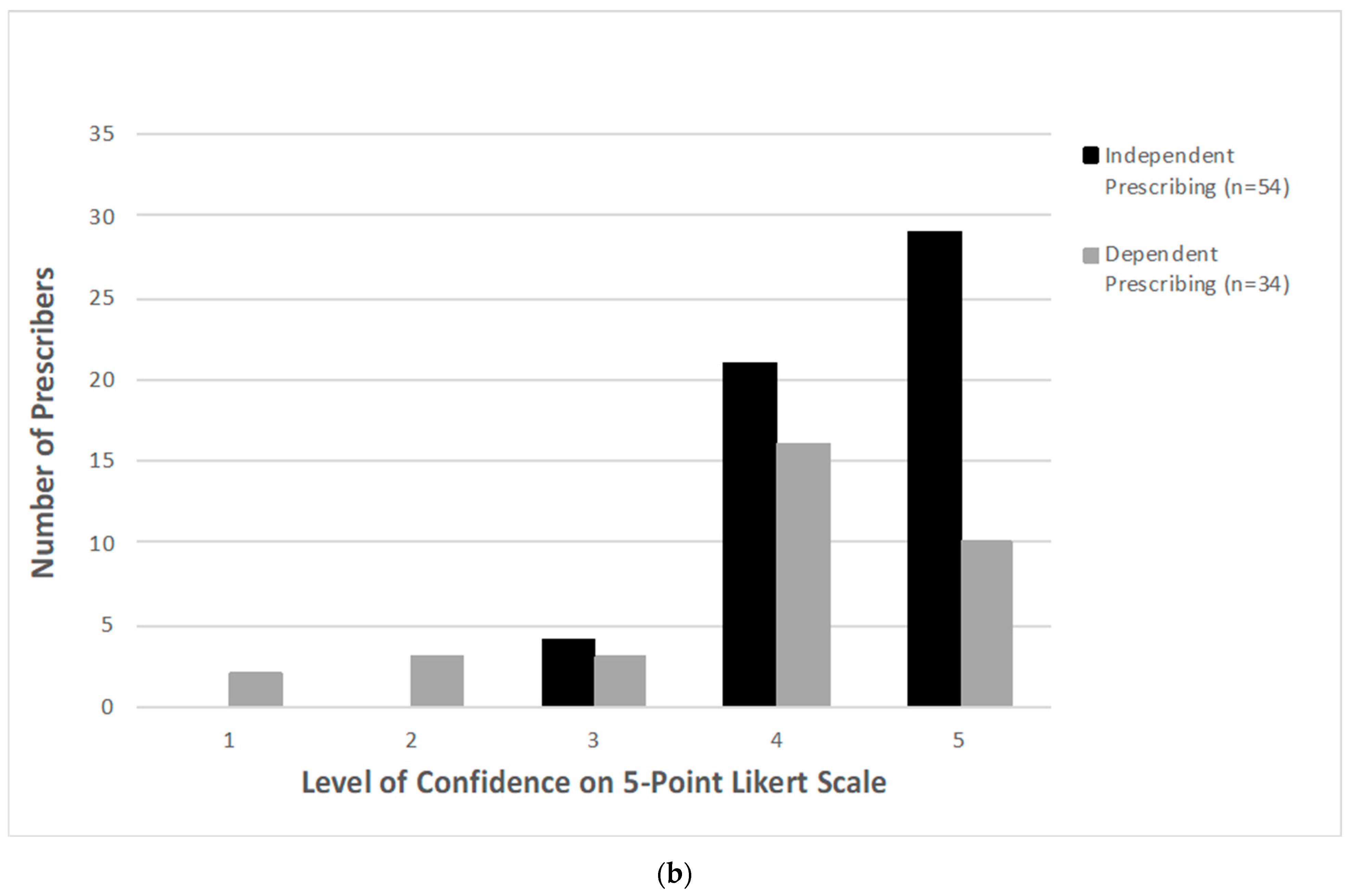
3.3. Prescribing Confidence by Decision-Maker and Seniority
3.4. Appropriateness of Prescribing
4. Discussion
4.1. Seniority and Specialty of Decision-Making
4.2. Prescribing Details
4.3. Prescribing Confidence
4.4. Appropriateness
4.5. Limitations
4.6. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Questionnaire
| Antibiotic Prescribing in ED We are aiming to understand more about antibiotic prescribing in the ED. There are seven (7) questions which should take <5 min to complete. Q1. What is your role in ED? | |
| |
| In your most recent experience with antibiotic prescribing during the shift on the following date: __________________ Q2. What antibiotic was prescribed? Antibiotic Type __________________________________ Antibiotic Dose __________________________________ Antibiotic Frequency ______________________________ Q3. What condition were antibiotics prescribed for? (i.e., working diagnosis: UTI, febrile neutropenia) ___________________________________________________ Q4. Did you make the decision to prescribe? | |
| |
| Q5. If No, then who made the decision? (indicate level of training and speciality) | |
Level of Training
| Speciality
|
| Q6. For your most recent experience, which of the following were used to decide on antibiotic selection? (tick all which apply)? O Electronic Therapeutic Guidelines (eTG) O Other guidelines (please specify _________________________) O ED consultant recommendation (please specify if in person or vs phone call) O Infectious disease recommendation please specify if registrar or consultant please specify if in person or phone call please specify if you talked to ID, or someone else; if so, who _____________ O Microbiology recommendation please specify if registrar or consultant please specify if in person or phone call please specify if you talked to ID, or someone else; if so, who _____________ O Other recommendation (please specify ___________________________) O I don’t know Q7. At time of pre-scribing, how con-fident were you on a scale of 1-5 that antibiotics were in-dicated? (please circle) Q8. At the time of prescribing, how confident were you on a scale of 1-5 that an appropriate antibiotic was prescribed? (please circle) Thank you for participating! | |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Appropriateness | If Endorsed Guidelines Are Present | If Endorsed Guidelines Are Absent or Not Applicable | ||
|---|---|---|---|---|
| Appropriate | 1 | Optimal * | Antimicrobial prescription follows either the Therapeutic Guidelines ^ or endorsed local guidelines optimally, including antimicrobial choice, dosage, route and duration #, including for surgical prophylaxis | The antimicrobial prescription has been reviewed and endorsed by a clinician with expert antimicrobial prescribing knowledge $ OR The prescribed antimicrobial will cover the likely causative pathogen/s and there is not a narrower spectrum or more appropriate antimicrobial choice, dosage, route or duration available (including for surgical prophylaxis) |
| 2 | Adequate | Antimicrobial prescription does not optimally follow the Therapeutic Guidelines ^ or endorsed local guidelines, including antimicrobial choice, dosage, route or duration #, however, is a reasonable alternative choice for the likely causative or cultured pathogens OR For surgical prophylaxis, as above and duration # is less than 24 h | Antimicrobial prescription including antimicrobial choice, dosage, route and duration # is not the most optimal, however, is a reasonable alternative choice for the likely causative or cultured pathogens | |
| Inappropriate | 3 | Suboptimal | Antimicrobial prescription including antimicrobial choice, dosage, route and duration # is an unreasonable choice for the likely causative pathogen/s, including: Spectrum excessively broad or an unnecessary overlap in spectrum of activity OR There may be a mild or non-life-threatening allergy mismatch | |
| 4 | Inadequate | Antimicrobial prescription including antimicrobial choice, dosage, route or duration # is unlikely to treat the likely causative or cultured pathogens OR An antimicrobial is not indicated for the documented or presumed indication OR There may be a severe or possibly life-threatening allergy mismatch | ||
| 5 | Not assessable | The indication is not documented and unable to be determined from the notes OR The notes are not comprehensive enough to assess appropriateness OR The patient is too complex, due to multiple co-morbidities, allergies or microbiology results, etc. | ||
| Condition | n | Appropriate n (%) | Inappropriate n (%) |
|---|---|---|---|
| Aspiration pneumonitis | 2 | 2 (2.3) | 0 (0) |
| Bartholin’s | 2 | 0 (0) | 2 (2.3) |
| Bronchitis | 2 | 2 (2.3) | 0 (0) |
| Community Acquired Pneumonia | 13 | 12 (13.6) | 1 (1.1) |
| C. difficile/diarrhoea | 2 | 1 (1.1) | 1 (1.1) |
| Cholecystitis | 2 | 1 (1.1) | 1 (1.1) |
| Dental abscess/infection | 3 | 3 (3.4) | 0 (0) |
| Diverticulitis | 1 | 1 (1.1) | 0 (0) |
| Dog bite prophylaxis | 2 | 2 (2.3) | 0 (0) |
| Ear Infection | 1 | 1 (1.1) | 0 (0) |
| Epididymitis | 1 | 1 (1.1) | 0 (0) |
| Facial bone fractures | 2 | 0 (0) | 2 (2.3) |
| Febrile neutropenia | 1 | 1 (1.1) | 0 (0) |
| Infected prosthesis | 2 | 2 (2.3) | 0 (0) |
| Hepatic encephalopathy | 1 | 1 (1.1) | 0 (0) |
| Infectious Exacerbation COPD | 2 | 2 (2.3) | 0 (0) |
| Mastitis | 1 | 1 (1.1) | 0 (0) |
| MRSA Osteomyelitis | 1 | 1 (1.1) | 0 (0) |
| Periorbital cellulitis | 2 | 2 (2.3) | 0 (0) |
| Pharyngitis | 5 | 4 (4.5) | 1 (1.1) |
| Pelvic Inflammatory Disease | 5 | 5 (5.7) | 0 (0) |
| Post-Indwelling Catheter insertion | 1 | 0 (0) | 1 (1.1) |
| Post-operative infection | 2 | 2 (2.3) | 0 (0) |
| Pyelonephritis | 3 | 3 (3.4) | 0 (0) |
| Sepsis | 2 | 2 (2.3) | 0 (0) |
| Skin infection (cellulitis) | 9 | 9 (10.2) | 0 (0) |
| Sexually Transmitted Inefection | 1 | 1 (1.1) | 0 (0) |
| Surgical prophylaxis | 1 | 1 (1.1) | 0 (0) |
| Urinary tract infection (UTI) | 10 | 10 (11.4) | 0 (0) |
| UTI prophylaxis | 1 | 0 (0) | 1 (1.1) |
| Uvulitis | 1 | 0 (0) | 1 (1.1) |
| Wound collection | 1 | 1 (1.1) | 0 (0) |
| Wound prophylaxis | 3 | 1 (1.1) | 2 (2.3) |
| Total | 88 | 75 (85.2) | 13 (14.8) |
References
- United Nations Interagency Coordination Group on Antimicrobial Resistance (IACG). No Time to Wait: Securing the Future from Drug-Resistant Infections. Available online: https://www.who.int/antimicrobial-resistance/interagency-coordination-group/IACG_final_report_EN.pdf?ua=1 (accessed on 11 February 2021).
- Kumar, A.; Roberts, D.; Wood, K.E.; Light, B.; Parrillo, J.E.; Sharma, S.; Suppes, R.; Feinstein, D.; Zanotti, S.; Taiberg, L.; et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 2006, 34, 1589–1596. [Google Scholar] [CrossRef]
- Kumar, A.; Ellis, P.; Arabi, Y.; Roberts, D.; Light, B.; Parrillo, J.E.; Dodek, P.; Wood, G.; Kumar, A.; Simon, D.; et al. Initiation of Inappropriate Antimicrobial Therapy Results in a Fivefold Reduction of Survival in Human Septic Shock. Chest 2009, 136, 1237–1248. [Google Scholar] [CrossRef]
- Dellinger, R.P.; The Surviving Sepsis Campaign Guidelines Committee including The Pediatric Subgroup*; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis and Septic Shock, 2012. Intensiv. Care Med. 2013, 39, 165–228. [Google Scholar] [CrossRef] [PubMed]
- Global Antimicrobial Resistance Surveillance System (GLASS) Report: Early Implementation 2016–2017; World Health Organization: Geneva, Switzerland, 2017; p. 164. Available online: https://www.who.int/docs/default-source/searo/amr/global-antimicrobial-resistance-surveillance-system-(glass)-report-early-implementation-2016-2017.pdf?sfvrsn=ea19cc4a_2 (accessed on 11 February 2021).
- Franklin, B.D.; O’Grady, K.; Donyai, P.; Jacklin, A.; Barber, N. The impact of a closed-loop electronic prescribing and administration system on prescribing errors, administration errors and staff time: A before-and-after study. Qual. Saf. Heal. Care 2007, 16, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Lewis, P.J.; Dornan, T.; Taylor, D.; Tully, M.P.; Wass, V.; Ashcroft, D. Prevalence, Incidence and Nature of Prescribing Errors in Hospital Inpatients. Drug Saf. 2009, 32, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Wittich, C.M.; Burkle, C.M.; Lanier, W.L. Medication Errors: An Overview for Clinicians. Mayo Clin. Proc. 2014, 89, 1116–1125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brien, A.P.; Rawlins, M.D.; Ingram, P.R. Appropriateness and Determinants of Antibiotic Prescribing in an Australian Emergency Department. Emerg. Med. Australas. EMA 2015, 27, 83–84. [Google Scholar] [CrossRef]
- May, L.; Gudger, G.; Armstrong, P.; Brooks, G.; Hinds, P.; Bhat, R.; Moran, G.J.; Schwartz, L.; Cosgrove, S.E.; Klein, E.Y.; et al. Multisite Exploration of Clinical Decision Making for Antibiotic Use by Emergency Medicine Providers Using Quantitative and Qualitative Methods. Infect. Control. Hosp. Epidemiol. 2014, 35, 1114–1125. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign. Crit. Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef]
- Shallcross, L.J.; Freemantle, N.; Nisar, S.; Ray, D. A cross-sectional study of blood cultures and antibiotic use in patients admitted from the Emergency Department: Missed opportunities for antimicrobial stewardship. BMC Infect. Dis. 2016, 16, 166. [Google Scholar] [CrossRef] [Green Version]
- Xie, C.; Charles, P.G.; Urbancic, K. Inappropriate ceftriaxone use in the emergency department of a tertiary hospital in Melbourne, Australia. Emerg. Med. Australas. EMA 2013, 25, 94–96. [Google Scholar] [CrossRef]
- Pulcini, C. Antimicrobial stewardship in emergency departments: A neglected topic. Emerg. Med. J. 2015, 32, 506. [Google Scholar] [CrossRef]
- Llewelyn, M.J.; Hand, K.; Hopkins, S.; Walker, A.S. Antibiotic policies in acute English NHS trusts: Implementation of ‘Start Smart--Then Focus’ and relationship with Clostridium difficile infection rates. J. Antimicrob. Chemother. 2014, 70, 1230–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denny, K.J.; Cotta, M.O.; Parker, S.L.; Roberts, J.A.; Lipman, J. The use and risks of antibiotics in critically ill patients. Expert Opin. Drug Saf. 2016, 15, 667–678. [Google Scholar] [CrossRef] [PubMed]
- James, R.; Upjohn, L.; Cotta, M.; Luu, S.; Marshall, C.; Buising, K.; Thursky, K. Measuring antimicrobial prescribing quality in Australian hospitals: Development and evaluation of a national antimicrobial prescribing survey tool. J. Antimicrob. Chemother. 2015, 70, 1912–1918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turnidge, J.D.; Thursky, K.; Chen, C.S.; McNeil, V.R.; Wilkinson, I.J. Antimicrobial use in Australian hospitals: How much and how appropriate? Med. J. Aust. 2016, 205, S16–S20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strobe Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Therapeutic Guidelines Limited. eTG Complete. 2020. Available online: https://tgldcdp.tg.org.au/etgcomplete (accessed on 28 February 2021).
- Alanazi, M.A.; Tully, M.P.; Lewis, P.J. Prescribing errors by junior doctors- A comparison of errors with high risk medicines and non-high risk medicines. PLoS ONE 2019, 14, e0211270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papoutsi, C.; Mattick, K.; Pearson, M.; Brennan, N.; Briscoe, S.; Wong, G. Social and professional influences on antimicrobial prescribing for doctors-in-training: A realist review. J. Antimicrob. Chemother. 2017, 72, 2418–2430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panesar, P.; Jones, A.; Aldous, A.; Kranzer, K.; Halpin, E.; Fifer, H.; Macrae, B.; Curtis, C.; Pollara, G. Attitudes and Behaviours to Antimicrobial Prescribing following Introduction of a Smartphone App. PLoS ONE 2016, 11, e0154202. [Google Scholar] [CrossRef] [PubMed]
- Hamill, L.; Huynh, R.; Cross, J.; Alcorn, K.; Keijzers, G. DECIDE—Decision Support Webapp on Antimicrobial Care for Clinicians in the Emergency Department. ACEM 2019 ASM “The Changing Climate of Emergency Medicine”, 36th Annual Scientific Meeting, November 2019, Hobart, Tasmania. (2019) Poster Presentations. Emerg. Med. Australas. 2020, 32, 28–72. [Google Scholar] [CrossRef]
- Brinkman, D.J.; Tichelaar, J.; Graaf, S.; Otten, R.H.J.; Richir, M.C.; Van Agtmael, M.A. Do final-year medical students have sufficient prescribing competencies? A systematic literature review. Br. J. Clin. Pharmacol. 2018, 84, 615–635. [Google Scholar] [CrossRef] [PubMed]
- Broadwell Martin, M. “Teaching for Learning (XVI)”. (20 February 1969). Available online: https://www.businessballs.com/self-awareness/conscious-competence-learning-model///#conscious-competence-theory-origins. (accessed on 15 February 2021).
- Lewis, P.J.; Seston, E.; Tully, M.P. Foundation year one and year two doctors’ prescribing errors: A comparison of their causes. Postgrad. Med. J. 2018, 94, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Ryan, C.; Ross, S.; Davey, P.; Duncan, E.; Francis, J.J.; Fielding, S.; Johnston, M.; Ker, J.; Lee, A.J.; Macleod, M.J.; et al. Prevalence and Causes of Prescribing Errors: The PRescribing Outcomes for Trainee Doctors Engaged in Clinical Training (PROTECT) Study. PLoS ONE 2014, 9, e79802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charani, E.; Castro-Sánchez, E.; Sevdalis, N.; Kyratsis, Y.; Drumright, L.; Shah, N.; Holmes, A. Understanding the Determinants of Antimicrobial Prescribing Within Hospitals: The Role of “Prescribing Etiquette”. Clin. Infect. Dis. 2013, 57, 188–196. [Google Scholar] [CrossRef] [PubMed]




| Site 1 | Site 2 |
|---|---|
| 23/08/19 20:00–08:00 (Friday–Saturday) | 17/09/19 08:00–20:00 (Tuesday) |
| 26/08/19 08:00–20:00 (Monday) | 28/09/19 08:00–20:00 (Saturday) |
| 12/09/19 08:00–20:00 (Thursday) | 29/09/19 20:00–08:00 (Sunday–Monday) |
| Seniority Classification | n (%) | Job Role | n (%) | Specialty—n (%) |
|---|---|---|---|---|
| Senior | 31 (35.2) | Consultant | 3 (3.4) | Emergency—28 (90.3) Respiratory—2 (6.5) Urology—1 (3.2) |
| Registrar | 28 (31.8) | |||
| Mid-level | 38 (43.2) | Senior House Officer | 31 (35.2) | Emergency—35 (92.1) Obstetrics & Gynaecology—3 (7.9) |
| Principal House Officer | 7 (8.0) | |||
| Junior | 14 (15.9) | Junior House Officer | 4 (4.5) | Emergency—13 (92.9) Orthopaedics—1 (7.1) |
| Intern | 10 (11.4) | |||
| Other | 5 (5.7) | Nurse Practitioner | 4 (4.5) | |
| Unknown | 1 (1.1) |
| Seniority. | n (%) | Appropriate * n (%) | |
|---|---|---|---|
| Seniority of Respondents | Senior | 31 (35.2) | 26 (84) |
| Mid-level | 38 (43.2) | 33 (87) | |
| Junior | 14 (15.9) | 12 (86) | |
| Other | 4 (4.5) | 3 (75) | |
| Unknown | 1 (1.1) | 1 (100) | |
| Seniority of decision maker | Senior | 51 (60.0) | 44 (86) |
| Mid-level | 28 (31.8) | 24 (86) | |
| Junior | 3 (3.4) | 3 (100) | |
| Other | 5 (5.7) | 4 (80) | |
| Unknow | 1 (1.1) | 1 (100) | |
| Decision | Independent | 54 (61.4) | 47 (87) |
| Directed | 34 (38.6) | 28 (82) | |
| Confidence level Antibiotic Indicated—Independent | 4 or 5 | 49 (91) | 43 (88) |
| 1, 2 or 3 | 5 (9) | 4 (80) | |
| Confidence level Antibiotic Indicated—Directed | 4 or 5 | 24 (71) | 19 (79) |
| 1, 2 or 3 | 10 (29) | 9 (90) | |
| Confidence level Antibiotic Appropriate—Independent | 4 or 5 | 50 (93) | 44 (88) |
| 1, 2 or 3 | 4 (7) | 3 (75) | |
| Confidence level Antibiotic Appropriate—Directed | 4 or 5 | 26 (76) | 21 (81) |
| 1, 2 or 3 | 8 (24) | 7 (88) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamill, L.M.; Bonnett, J.; Baxter, M.F.; Kreutz, M.; Denny, K.J.; Keijzers, G. Antimicrobial Prescribing in the Emergency Department; Who Is Calling the Shots? Antibiotics 2021, 10, 843. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070843
Hamill LM, Bonnett J, Baxter MF, Kreutz M, Denny KJ, Keijzers G. Antimicrobial Prescribing in the Emergency Department; Who Is Calling the Shots? Antibiotics. 2021; 10(7):843. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070843
Chicago/Turabian StyleHamill, Laura M., Julia Bonnett, Megan F. Baxter, Melina Kreutz, Kerina J. Denny, and Gerben Keijzers. 2021. "Antimicrobial Prescribing in the Emergency Department; Who Is Calling the Shots?" Antibiotics 10, no. 7: 843. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070843