
Assessing Knowledge and Perception Regarding Antimicrobial Stewardship and Antimicrobial Resistance in University Students of Pakistan: Findings and Implications

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Demographic Information of the Participants
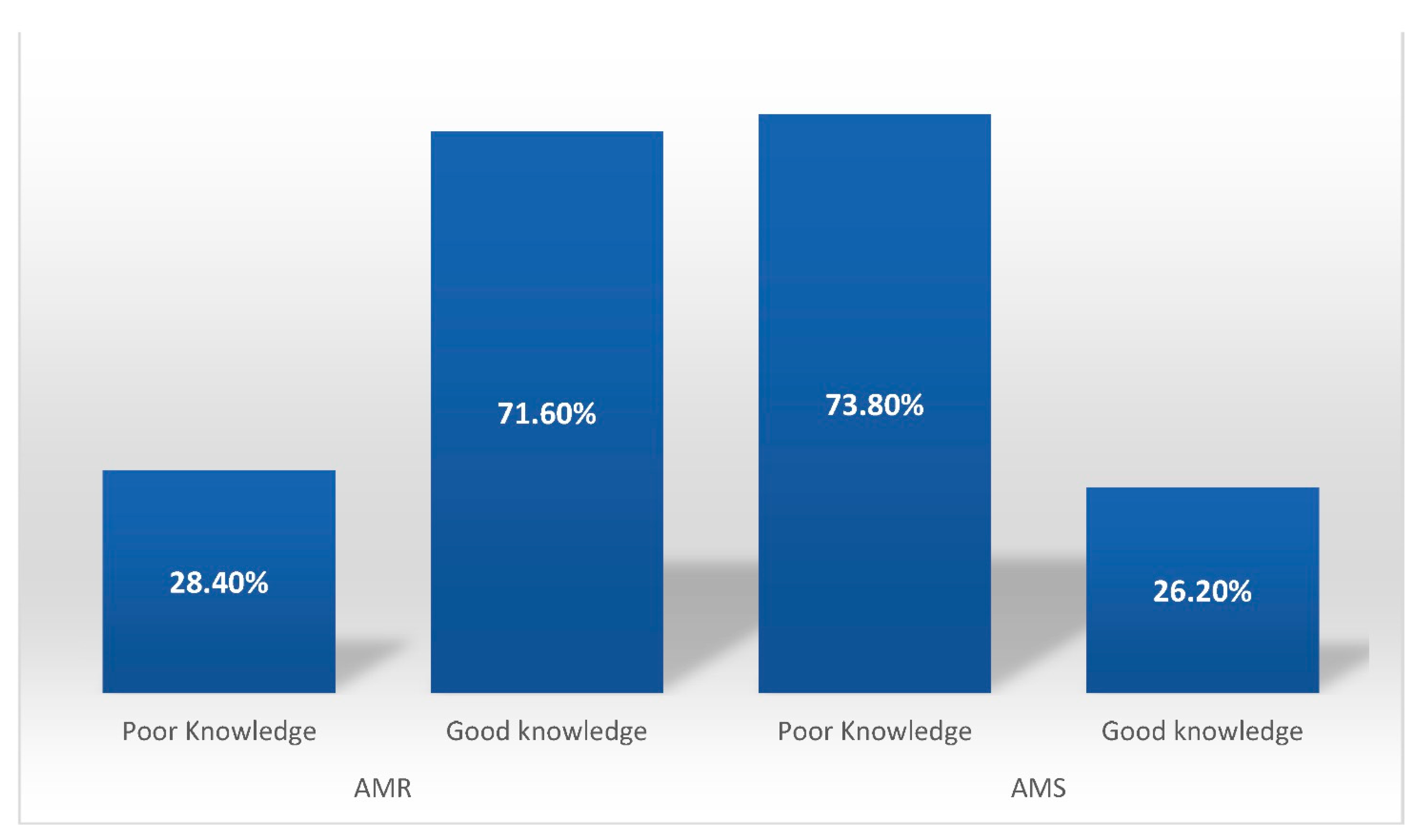
2.2. Knowledge of Antimicrobial Resistance
2.3. Perception about Antibiotic Resistance
2.4. Knowledge regarding Antimicrobial Stewardship
2.5. Perception about Antimicrobial Stewardship
3. Discussion
3.1. Recommendations
3.2. Study Limitations
4. Materials and Methods
4.1. Study Design and Settings
4.2. Study Instrument
4.3. Data Collection
4.4. Ethical Approval
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burnham, C.-A.D.; Leeds, J.; Nordmann, P.; O’Grady, J.; Patel, J. Diagnosing antimicrobial resistance. Nat. Rev. Genet. 2017, 15, 697–703. [Google Scholar] [CrossRef] [PubMed]
- Abushaheen, M.A.; Muzaheed; Fatani, A.J.; Alosaimi, M.; Mansy, W.; George, M.; Acharya, S.; Rathod, S.; Divakar, D.D.; Jhugroo, C.; et al. Antimicrobial resistance, mechanisms and its clinical significance. Dis. Month 2020, 66, 100971. [Google Scholar] [CrossRef]
- Blaser, J.; Stone, B.B.; Groner, M.C.; Zinner, S.H. Comparative study with enoxacin and netilmicin in a pharmacodynamic model to determine importance of ratio of antibiotic peak concentration to MIC for bactericidal activity and emergence of resistance. Antimicrob. Agents Chemother. 1987, 31, 1054–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchbanks, C.R.; McKiel, J.R.; Gilbert, D.H.; Robillard, N.J.; Painter, B.; Zinner, S.H.; Dudley, M.N. Dose ranging and fractionation of intravenous ciprofloxacin against Pseudomonas aeruginosa and Staphylococcus aureus in an in vitro model of infection. Antimicrob. Agents Chemother. 1993, 37, 1756–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandamme, E.J.; Mortelmans, K. A century of bacteriophage research and applications: Impacts on biotechnology, health, ecology and the economy! J. Chem. Technol. Biotechnol. 2019, 94, 323–342. [Google Scholar] [CrossRef]
- World Health Organization. Antibiotic Resistance. Available online: https://www.who.int/news-room/fact-sheets/detail/antibiotic-resistance (accessed on 18 June 2021).
- Machowska, A.; Lundborg, C.S. Drivers of Irrational Use of Antibiotics in Europe. Int. J. Environ. Res. Public Health 2018, 16, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Momanyi, L.B. Antibiotic Prescribing Patterns at Rift Valley Provincial General Hospital: A Point Prevalence Survey. Ph.D. Thesis, University of Nairobi, Nairobi, Kenya, 2017. [Google Scholar]
- Chauhan, I.; Yasir, M.; Kumari, M.; Verma, M. The pursuit of rational drug use: Understanding factors and interventions. Pharmaspire 2018, 10, 44–48. [Google Scholar]
- Morgan, D.J.; Okeke, I.; Laxminarayan, R.; Perencevich, E.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect. Dis. 2011, 11, 692–701. [Google Scholar] [CrossRef] [Green Version]
- Gajdács, M.; Urbán, E.; Stájer, A.; Baráth, Z. Antimicrobial Resistance in the Context of the Sustainable Development Goals: A Brief Review. Eur. J. Investig. Health Psychol. Educ. 2021, 11, 71–82. [Google Scholar] [CrossRef]
- Lescure, D.; Paget, J.; Schellevis, F.; Van Dijk, L. Determinants of Self-Medication with Antibiotics in European and Anglo-Saxon Countries: A Systematic Review of the Literature. Front. Public Health 2018, 6, 370. [Google Scholar] [CrossRef]
- Aslam, A.; Gajdács, M.; Zin, C.S.; Ab Rahman, N.S.; Ahmed, S.I.; Zafar, M.Z.; Jamshed, S. Evidence of the Practice of Self-Medication with Antibiotics among the Lay Public in Low- and Middle-Income Countries: A Scoping Review. Antibiotics 2020, 9, 597. [Google Scholar] [CrossRef]
- Da Silva, A.A.; Dias, D.A.D.A.; Marques, A.; di Biase, C.B.; Murni, I.; Dramowski, A.; Sharland, M.; Huebner, J.; Zingg, W. Role of antimicrobial stewardship programmes in children: A systematic review. J. Hosp. Infect. 2018, 99, 117–123. [Google Scholar] [CrossRef]
- Pulcini, C.; Binda, F.; Lamkang, A.; Trett, A.; Charani, E.; Goff, D.; Harbarth, S.; Hinrichsen, S.; Levy-Hara, G.; Mendelson, M.; et al. Developing core elements and checklist items for global hospital antimicrobial stewardship programmes: A consensus approach. Clin. Microbiol. Infect. 2019, 25, 20–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heijl, I.V. Antibiotic Stewardship in Community-acquired Pneumonia. Ph.D. Thesis, Utrecht University, Utrecht, The Netherlands, 2020. [Google Scholar]
- Borchardt, R.A.; Rolston, K.V.I. ANTIMICROBIAL STEWARDSHIP: A proactive approach to combating resistance. J. Am. Acad. Physician Assist. 2012, 25, 22. [Google Scholar] [CrossRef] [PubMed]
- Mccarthy, K.; Dempsey, E.; Bch, M. Impact of an Antimicrobial Stewardship and Emergency Department Initiated Dal-bavancin Guideline for Patients with Acute Bacterial Skin and Soft-Tissue Infections. In Open Forum Infectious Diseases; Oxford University Press: Oxford, UK, 2017. [Google Scholar]
- Asghar, S.; Atif, M.; Mushtaq, I.; Malik, I.; Hayat, K.; Babar, Z.-U.-D. Factors associated with inappropriate dispensing of antibiotics among non-pharmacist pharmacy workers. Res. Soc. Adm. Pharm. 2020, 16, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, K.; Molinier, L.; Hallit, S.; Sartelli, M.; Catena, F.; Coccolini, F.; Hardcastle, T.C.; Roques, C.; Salameh, P. Drivers of Antibiotic Resistance Transmission in Low- and Middle-Income Countries from a “One Health” Perspective—A Review. Antibiotics 2020, 9, 372. [Google Scholar] [CrossRef]
- Rehman, I.U.; Asad, M.M.; Bukhsh, A.; Ali, Z.; Ata, H.; Dujaili, J.A.; Blebil, A.Q.; Khan, T.M. Knowledge and Practice of Pharmacists toward Antimicrobial Stewardship in Pakistan. Pharmacy 2018, 6, 116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry Of National Health Services, Regulations and Coordination. Antimicrobial Resistance National Action Plan Pakistan. Available online: https://www.nih.org.pk/wp-content/uploads/2018/08/AMR-National-Action-Plan-Pakistan.pdf (accessed on 18 June 2021).
- Limaye, D.; Limaye, V.; Krause, G.; Fortwengel, G. A systematic review of the literature to assess self-medication practices. Annals of Medical and Health Sciences Research. Ann. Med. Health Sci. Res. 2017, 7, 1–15. [Google Scholar]
- Laghari, S.H.; Abdullah, D.; Suheryani, I.; Abbas, J.; Yousuf, M.; Saleem, H.; Gul, A. Prevalence and Reasons of Antibiotics Self-Medication in Residents of Hyderabad, Pakistan. Lat. Am. J. Pharm. 2018, 37, 622–626. [Google Scholar]
- Nazir, S.; Azim, M. Assessment of antibiotic self-medication practice among public in the northwestern region of Pakistan. Eur. J. Hosp. Pharm. 2017, 24, 200. [Google Scholar] [CrossRef] [PubMed]
- Sakeena, M.H.F.; Bennett, A.A.; Jamshed, S.; Mohamed, F.; Herath, D.R.; Gawarammana, I.; McLachlan, A.J. Investigating knowledge regarding antibiotics and antimicrobial resistance among pharmacy students in Sri Lankan universities. BMC Infect. Dis. 2018, 18, 209. [Google Scholar] [CrossRef]
- Singh, R.; Tam, V.H. Optimizing dosage to prevent emergence of resistance—Lessons from in vitro models. Curr. Opin. Pharmacol. 2011, 11, 453–456. [Google Scholar] [CrossRef]
- Rajiah, K.; Ren, W.S.; Jamshed, S. Evaluation of the understanding of antibiotic resistance among Malaysian pharmacy students at public universities: An exploratory study. J. Infect. Public Health 2015, 8, 266–273. [Google Scholar] [CrossRef] [Green Version]
- Atif, M.; Asghar, S.; Mushtaq, I.; Malik, I.; Amin, A.; Babar, Z.-U.-D.; Scahill, S. What drives inappropriate use of antibiotics? A mixed methods study from Bahawalpur, Pakistan. Infect. Drug Resist. 2019, ume 12, 687–699. [Google Scholar] [CrossRef] [Green Version]
- Hayat, K.; Jamshed, S.; Rosenthal, M.; Haq, N.U.; Chang, J.; Rasool, M.F.; Malik, U.R.; Rehman, A.U.; Khan, K.M.; Fang, Y. Understanding of Pharmacy Students towards Antibiotic Use, Antibiotic Resistance and Antibiotic Stewardship Programs: A Cross-Sectional Study from Punjab, Pakistan. Antibiotics 2021, 10, 66. [Google Scholar] [CrossRef]
- Tong, S.; Pan, J.; Lu, S.; Tang, J. Patient compliance with antimicrobial drugs: A Chinese survey. Am. J. Infect. Control 2018, 46, e25–e29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saleem, Z.; Hassali, M.A.; Hashmi, F.; Azhar, F.; Mubarak, R.; Afzaal, A.; Munawar, U. Medical and pharmacy students’ knowledge, attitude and perception concerning antimicrobial use and resistance in Pakistan. Pharm. Educ. 2019, 19, 199–205. [Google Scholar]
- Abubakar, U.; Muhammad, H.T.; Sulaiman, S.A.S.; Ramatillah, D.L.; Amir, O. Knowledge and self-confidence of antibiotic resistance, appropriate antibiotic therapy, and antibiotic stewardship among pharmacy undergraduate students in three Asian countries. Curr. Pharm. Teach. Learn. 2020, 12, 265–273. [Google Scholar] [CrossRef]
- Ourghanlian, C.; Lapidus, N.; Antignac, M.; Fernandez, C.; Dumartin, C.; Hindlet, P. Pharmacists’ role in antimicrobial stewardship and relationship with antibiotic consumption in hospitals: An observational multicentre study. J. Glob. Antimicrob. Resist. 2020, 20, 131–134. [Google Scholar] [CrossRef]
- Gajdács, M.; Paulik, E.; Szabó, A. Knowledge, Attitude and Practice of Community Pharmacists Regarding Antibiotic Use and Infectious Diseases: A Cross-Sectional Survey in Hungary (KAPPhA-HU). Antibiotics 2020, 9, 41. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.-J.; Lee, S.-E.; Lee, D.S.; Kim, Y.-H. Risk assessment of human antibiotics in Korean aquatic environment. Environ. Toxicol. Pharmacol. 2008, 26, 216–221. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Pires, J.; Silvester, R.; Zhao, C.; Song, J.; Criscuolo, N.G.; Gilbert, M.; Bonhoeffer, S.; Laxminarayan, R. Global trends in antimicrobial resistance in animals in low-and middle-income countries. Science 2019, 365, 6459. [Google Scholar] [CrossRef] [Green Version]
- Bahauddin Zakariya University. University Description. Available online: https://www.bzu.edu.pk/ (accessed on 19 June 2021).
- Eysenbach, G. Improving the Quality of Web Surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, 34. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, S. The STROBE guidelines. Saudi J. Anaesth. 2019, 13, S31–S34. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | % | ||
|---|---|---|---|
| Age | 18–23 | 267 | 53.5 |
| >23 | 229 | 46.5 | |
| Department/faculty | Pharmaceutical sciences | 227 | 45.8 |
| Veterinary sciences | 131 | 26.4 | |
| Biological sciences | 138 | 27.8 | |
| Gender | Male | 285 | 57.5 |
| Female | 211 | 42.5 | |
| Marital status | single | 480 | 96.8 |
| married | 16 | 3.2 | |
| Education level | Undergraduate | 449 | 90.5 |
| Postgraduate | 47 | 9.5 | |
| Overall N (%) | Pharmaceutical Sciences | Veterinary Sciences | Biological Sciences | p-Value | ||
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||||
| Do you know about the term “antimicrobial resistance”? | yes | 425 (85.7) | 121 (92.4) | 188 (82.8) | 116 (84.4) | 0.12 |
| no | 46 (9.3) | 5 (3.8) | 26 (11.5) | 15 (10.9) | ||
| maybe | 25 (5) | 5 (3.8) | 13 (5.7) | 7 (5.1) | ||
| Do you know poorly designed dosing regimens can contribute to antimicrobial resistance? | yes | 394 (79.4) | 118 (90.1) | 170 (74.9) | 106 (76.8) | 0.003 |
| no | 55 (11.1) | 9 (6.9) | 26 (11.5) | 20 (14.5) | ||
| maybe | 47 (9.5) | 4 (3.1) | 31 (13.7) | 12 (8.7) | ||
| Do you know the usage of broad-spectrum antibiotics promotes antimicrobial resistance? | yes | 433 (87.3) | 121 (92.4) | 194 (85.5) | 118 (85.5) | 0.09 |
| no | 27 (5.4) | 1 (0.8) | 17 (7.5) | 9 (6.5) | ||
| maybe | 36 (7.3) | 9 (6.9) | 16 (7) | 11 (8.0) | ||
| Do you know that antibiotics can kill viruses? | yes | 134 (27.1) | 21 (16.2) | 72 (31) | 41 (29.7) | 0.006 |
| no | 294 (59.4) | 95 (73.1) | 123 (54.2) | 76 (55.1) | ||
| maybe | 67 (13.5) | 14 (10.8) | 32 (14.1) | 21 (15.2) | ||
| Overall N (%) | Pharmaceutical Sciences | Veterinary Sciences | Biological Sciences | p-Value | ||
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||||
| Do you think irrational use of antibiotics can harm the patient? | yes | 433 (87.3) | 121 (92.4) | 194 (85.5) | 118 (85.5) | 0.09 |
| no | 27 (5.4) | 1 (0.8) | 17 (7.5) | 9 (6.5) | ||
| maybe | 36 (7.3) | 9 (6.9) | 16 (7.0) | 11 (8.0) | ||
| Do you think casual/common use of antibiotics in Pakistan is appropriate? | yes | 217 (43.8) | 48 (36.9) | 121 (53.3) | 48 (34.8) | <0.001 |
| no | 229 (46.3) | 78 (60) | 77 (33.9) | 74 (53.6) | ||
| maybe | 49 (9.9) | 4 (3.1) | 29 (12.8) | 16 (11.6) | ||
| Do you think broad-spectrum anti-bacterials are used unnecessarily when narrow-spectrum antibiotics are available? | yes | 330 (66.5) | 109 (83.2) | 137 (60.4) | 84 (60.9) | <0.001 |
| no | 77 (15.5) | 9 (6.9) | 47 (20.7) | 21 (15.2) | ||
| maybe | 89 (17.9) | 13 (9.9) | 43 (18.9) | 33 (23.9) | ||
| Do you think poor patient adherence to prescribed antibiotics can be a cause of AMR? | yes | 356 (71.9) | 110 (84.6) | 151 (66.5) | 95 (68.8) | 0.003 |
| no | 66 (13.3) | 9 (6.9) | 33 (14.5) | 24 (17.4) | ||
| maybe | 73 (14.7) | 11 (8.5) | 43 (18.9) | 19 (13.8) | ||
| It is important to follow the appropriate duration of antimicrobials to prevent the development of resistance? | yes | 417 (84.1) | 120 (91.6) | 183 (80.6) | 114 (82.6) | <0.001 |
| no | 35 (7.1) | 6 (4.6) | 19 (8.4) | 10 (7.2) | ||
| maybe | 44 (8.9) | 5 (3.8) | 25 (11.0) | 14 (10.1) | ||
| Do you think antibiotic use should be reduced? | yes | 379 (76.4) | 117 (89.3) | 153 (67.4) | 109 (79.0) | <0.001 |
| no | 69 (13.9) | 7 (5.3) | 40 (17.6) | 22 (15.9) | ||
| maybe | 48 (9.7) | 7 (5.3) | 34 (15.0) | 7 (5.1) | ||
| Overall N (%) | Pharmaceutical Sciences | Veterinary Sciences | Biological Sciences | p-Value | ||
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||||
| Do you know about AMS? | yes | 158 (31.9) | 49 (37.4) | 82 (36.1) | 27 (19.6) | <0.001 |
| no | 287 (57.9) | 64 (48.9) | 119 (52.4) | 104 (75.4) | ||
| maybe | 51 (10.3) | 18 (13.7) | 26 (11.5) | 7 (5.1) | ||
| AMS aims to optimize antimicrobial use. | yes | 427 (86.3) | 119 (91.5) | 186 (81.9) | 122 (88.4) | 0.006 |
| no | 37 (7.5) | 7 (5.4) | 21 (9.3) | 9 (6.5) | ||
| maybe | 31 (6.3) | 4 (3.1) | 20 (8.8) | 7 (5.1) | ||
| AMS is the key component of a multifaceted approach for preventing the emergence of antimicrobial resistance. | yes | 429 (86.5) | 126 (96.2) | 192 (84.6) | 111 (80.4) | 0.006 |
| no | 36 (7.3) | 1 (0.8) | 17 (7.5) | 18 (13) | ||
| maybe | 31 (6.3) | 4 (3.1) | 18 (7.9) | 9 (6.5) | ||
| Overall N (%) | Pharmaceutical Sciences | Veterinary Sciences | Biological Sciences | p-Value | ||
|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | ||||
| Do you think strong knowledge and awareness about correct anti-microbial use is important for better patient care? | yes | 369 (74.4) | 106 (80.9) | 171 (75.3) | 92 (66.7) | 0.10 |
| no | 45 (9.1) | 5 (3.8) | 19 (8.4) | 21 (15.2) | ||
| maybe | 82 (16.5) | 20 (15.3) | 37 (16.3) | 25 (18.1) | ||
| Do you think pharmacists can play a role in awareness of correct antimicrobial usage? | yes | 429 (86.5) | 117 (89.3) | 192 (84.6) | 120 (87) | 0.001 |
| no | 24 (4.8) | 3 (2.3) | 15 (6.6) | 6 (4.3) | ||
| maybe | 43 (8.7) | 11 (8.4) | 20 (8.8) | 12 (8.7) | ||
| AMS should be incorporated into the healthcare system. | yes | 369 (74.4) | 106 (80.9) | 171 (75.3) | 92 (66.7) | 0.001 |
| no | 45 (9.1) | 5 (3.8) | 19 (8.4) | 21 (15.2) | ||
| maybe | 82 (16.5) | 20 (15.3) | 37 (16.3) | 25 (18.1) | ||
| Do you think hospital pharmacist is an essential element of AMS? | yes | 399 (80.4) | 117 (89.3) | 173 (76.2) | 109 (79) | 0.47 |
| no | 41 (8.3) | 7 (5.3) | 21 (9.3) | 13 (9.4) | ||
| maybe | 56 (11.3) | 7 (5.3) | 33 (14.5) | 16 (11.6) | ||
| Implementation of AMS can ensure therapeutic efficacy of antibiotics and reduce antimicrobial resistance? | yes | 274 (55.2) | 56 (42.7) | 148 (65.2) | 70 (50.7) | <0.001 |
| no | 92 (18.5) | 40 (30.5) | 20 (8.8) | 32 (23.2) | ||
| maybe | 130 (26.2) | 35 (26.7) | 59 (26) | 36 (26.1) | ||
| AMR Knowledge | p-Value | AMS Knowledge | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Poor | Good | Poor | Good | ||||
| N (%) | N (%) | N (%) | N (%) | ||||
| Age | 18–23 | 85 (60.3) | 179 (50.9) | 0.05 | 197 (54.1) | 67 (51.9) | 0.66 |
| >23 | 56 (39.7) | 173 (49.9) | 167 (45.9) | 62 (48.1) | |||
| Department | Pharmaceutical sciences | 19 (53.2) | 112 (31.5) | <0.001 | 87 (23.8) | 44 (33.8) | 0.002 |
| Veterinary sciences | 75 (33.3) | 152 (42.8) | 162 (44.3) | 65 (50) | |||
| Biological sciences | 47 (33.3) | 91 (25.6) | 117 (32) | 21 (16.2) | |||
| Gender | Male | 89 (63.1) | 194 (54.6) | 0.01 | 203 (55.5) | 80 (61.5) | 0.33 |
| Female | 50 (35.5) | 161 (45.4) | 162 (44.3) | 49 (37.7) | |||
| Marial status | Single | 136 (96.5) | 344 (96.9) | 0.79 | 355 (97) | 125 (96.2) | 0.64 |
| Married | 5 (3.5) | 11 (3.1) | 11 (3.0) | 5 (3.8) | |||
| Education level | Undergraduate | 135 (95.7) | 314 (88.5) | 0.01 | 330 (90.2) | 119 (91.5) | 0.64 |
| Postgraduate | 6 (4.3) | 41 (11.5) | 36 (9.8) | 11 (8.5) | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussain, I.; Yousaf, N.; Haider, S.; Jalil, P.; Saleem, M.U.; Imran, I.; Majeed, A.; Rehman, A.u.; Uzair, M.; Rasool, M.F.; et al. Assessing Knowledge and Perception Regarding Antimicrobial Stewardship and Antimicrobial Resistance in University Students of Pakistan: Findings and Implications. Antibiotics 2021, 10, 866. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070866
Hussain I, Yousaf N, Haider S, Jalil P, Saleem MU, Imran I, Majeed A, Rehman Au, Uzair M, Rasool MF, et al. Assessing Knowledge and Perception Regarding Antimicrobial Stewardship and Antimicrobial Resistance in University Students of Pakistan: Findings and Implications. Antibiotics. 2021; 10(7):866. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070866
Chicago/Turabian StyleHussain, Iltaf, Nisa Yousaf, Sana Haider, Pervisha Jalil, Muhammad Usman Saleem, Imran Imran, Abdul Majeed, Anees ur Rehman, Muhammad Uzair, Muhammad Fawad Rasool, and et al. 2021. "Assessing Knowledge and Perception Regarding Antimicrobial Stewardship and Antimicrobial Resistance in University Students of Pakistan: Findings and Implications" Antibiotics 10, no. 7: 866. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10070866