1. Introduction
Antimicrobial resistance (AMR) is a global, public, and individual health challenge affecting the delivery of safe, effective healthcare in all settings and all countries. The ability of microorganisms to become resistant to the effect of antimicrobials is an inevitable evolutionary process; however, misuse and over-use of antimicrobial agents hastens the development and spread [
1,
2].
AMR leads to increased mortality rates [
3] and duration and cost of patient care [
1]. This is of particular concern in low- and middle-income countries (LMICs) due to the reduced availability of appropriate equipment and/or appropriate diagnostic tools, as well as challenges with access to quality antimicrobials [
4,
5,
6,
7]. The rise in incidence of AMR has led to an increased global focus on antimicrobial stewardship (AMS). Surveillance of antimicrobial use and resistance are core to all AMS activities and understanding how antimicrobials are used allows for a review of current practices and highlights areas for improvement. Point prevalence surveys (PPSs) are a widely recognised surveillance method requiring limited resources to collect information on antimicrobial prescribing practices and other relevant factors in hospitalized patients [
8,
9,
10,
11].
PPS are a key resource when planning and supporting national and local stewardship interventions in a range of settings, offering a standardised method for comparing data on antimicrobial use across hospitals and countries. The Global Point Prevalence Survey of Antimicrobial Consumption and Resistance (G-PPS;
www.global-pps.com/, accessed on 15 May 2021) aims to assess the global prevalence of antimicrobial prescribing and resistance, with an emphasis on countries with low resources, support, and expertise and supports antimicrobial stewardship programs in order to enhance appropriate antimicrobial prescribing [
12].
Alongside the evaluation of antimicrobial prescribing practices in hospitals, PPS can identify targets for quality improvement of antimicrobial prescribing and implement and monitor the impact of interventions through repeated surveys. One of the main aims in strengthening global AMS is to reduce the use of antimicrobials that are in the World Health Organization’s (WHO) ‘Watch’ and ‘Reserve categories’ and ‘Not Recommended’ group of their AWaRe framework [
13,
14]. The framework recommends preferred antimicrobial choice for treating common infections—the ‘Access’ category, based on consideration of benefits versus risks to patients and the potential for resistance. An additional classification—‘Not recommended’ was added to the framework more recently to include fixed-dose combinations of broad-spectrum antibiotics for which use is not evidence-based [
15]. Similarly, the Anatomic Therapeutic Chemical (ATC) classification categorizes drugs active substances into different groups and subgroups according to their therapeutic, pharmacological and chemical properties. WHO endorses the ATC classification as the standard for drug utilization monitoring and research [
16].
The Commonwealth Partnerships for Antimicrobial Stewardship programme (CwPAMS), managed by the Commonwealth Pharmacists Association (CPA) and Tropical Health and Education Trust (THET), is a health partnerships programme funded by the UK Official Development Assistance (ODA), through the Department of Health and Social Care’s Fleming Fund to address AMR globally [
17]. The aim of the programme is to enhance the implementation of protocols and evidenced-based decision making to support antimicrobial prescribing and the capacity for surveillance of antimicrobial consumption and stewardship.
The CwPAMS programme included 12 partnerships between UK health institutions and counterparts in four African Commonwealth countries: Ghana (GH), Uganda (UG), Zambia (ZM), and Tanzania (TZ). The partnerships consisted of volunteer health workers and experts from the five countries who shared skills and knowledge to co-develop strategies to address AMR and AMS. As part of the fulfillment of the aims of the partnership, a Global Point Prevalence Study was used to obtain baseline data and measure the impact of the implementation of AMS programmes across partnership countries.
This paper aims to compare national data on antimicrobial use obtained from 12 hospitals across four countries (Ghana (6), Uganda (4), Zambia (1) and Tanzania (1)) and identify target points for improvement. As part of an additional collaboration, PPS data from a further four hospitals in Ghana and one additional hospital in Zambia (which collected data using the Global PPS platform during the same period as the CwPAMS programme), are also included in the study.
3. Discussion
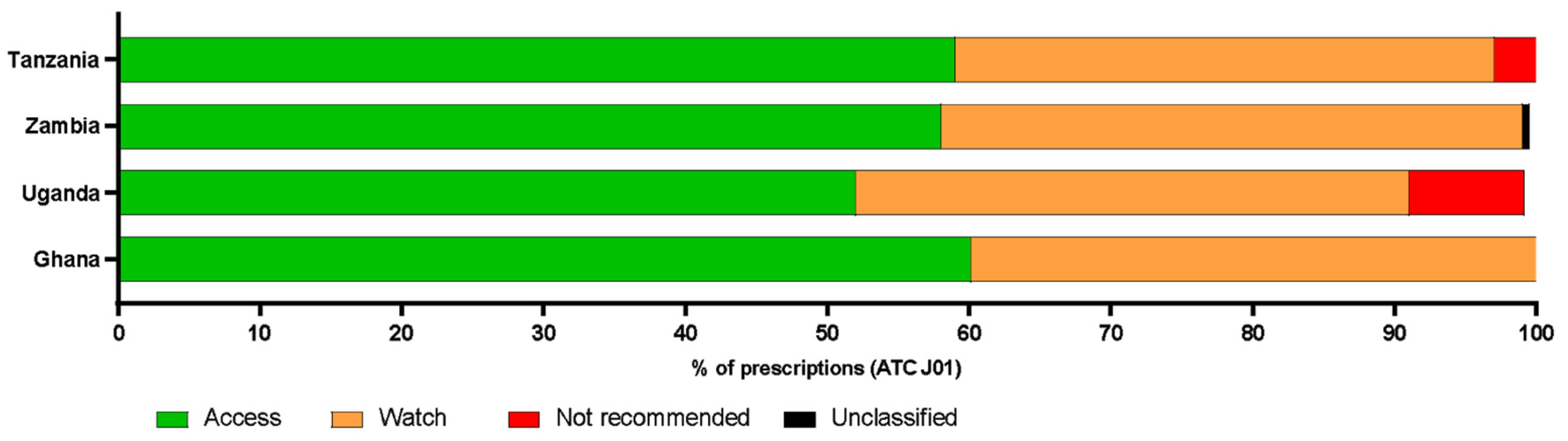
The Point Prevalence Surveys presented provide key insights into antibiotic prescribing in selected public or not-for-profit hospitals across Ghana, Tanzania, Uganda, and Zambia. The overall prevalence of antimicrobial use was 50% (30–57%), with most antibiotics prescribed belonging to the WHO ‘Access’ and ‘Watch’ groups. No ‘Reserve’ category antibiotics were prescribed across the study sites; however, there were some prescriptions of ‘Not Recommended’ antibiotic combinations. While this pattern of antibiotic use may partly be due to the prescriber’s consideration of optimality and potential for antimicrobial resistance, in line with WHO’s goal of improving antibiotic use through antimicrobial stewardship [
19], other authors suggest alternative reasoning [
20,
21].
Antibiotic prescribing patterns were significantly associated with accessibility and affordability, with broad-spectrum antibiotics in the Access category being more readily available and affordable than antibiotics in the Watch and Reserve categories and the ‘Not Recommended’ group [
20,
21]. A recent study on antibiotic availability and use in 20 low- and middle-income countries reported that the median proportion of facilities across countries with availability of Access category antibiotics was 89.5% [
22]. Pauwels et al. (2021) reported that low-income countries had the highest percentage of use of Access category antibiotics (63%), the lowest use of Watch category antibiotics (36%) and no Reserve category prescriptions on adult wards across 69 countries [
23]. A PPS conducted across six referral hospitals in Tanzania also supports data presented in the current study, reporting 62% of prescriptions for in-patients being from the Access group [
24]. In addition to availability and affordability, the similarity in prescription patterns across all four countries in the current study might be associated with the circulating bacterial strains and disease burden across low- and middle-income countries [
6,
7,
25]. The WHO proposes that the AWaRe classification should support monitoring of antibiotic prescribing and inform AMS programmes and has the target that by 2023 at least 60% of national antibiotic consumption should come from the Access category [
15]. In data presented here, 60% of the total of ATC J01 antibiotics prescribed in Ghana (1212/2071), 52% in Uganda (309/592), 58% in Zambia (201/347) and 59% in Tanzania (170/288) were in the Access category, demonstrating the hospitals’ alignment with the WHO target for national antibiotic consumption.
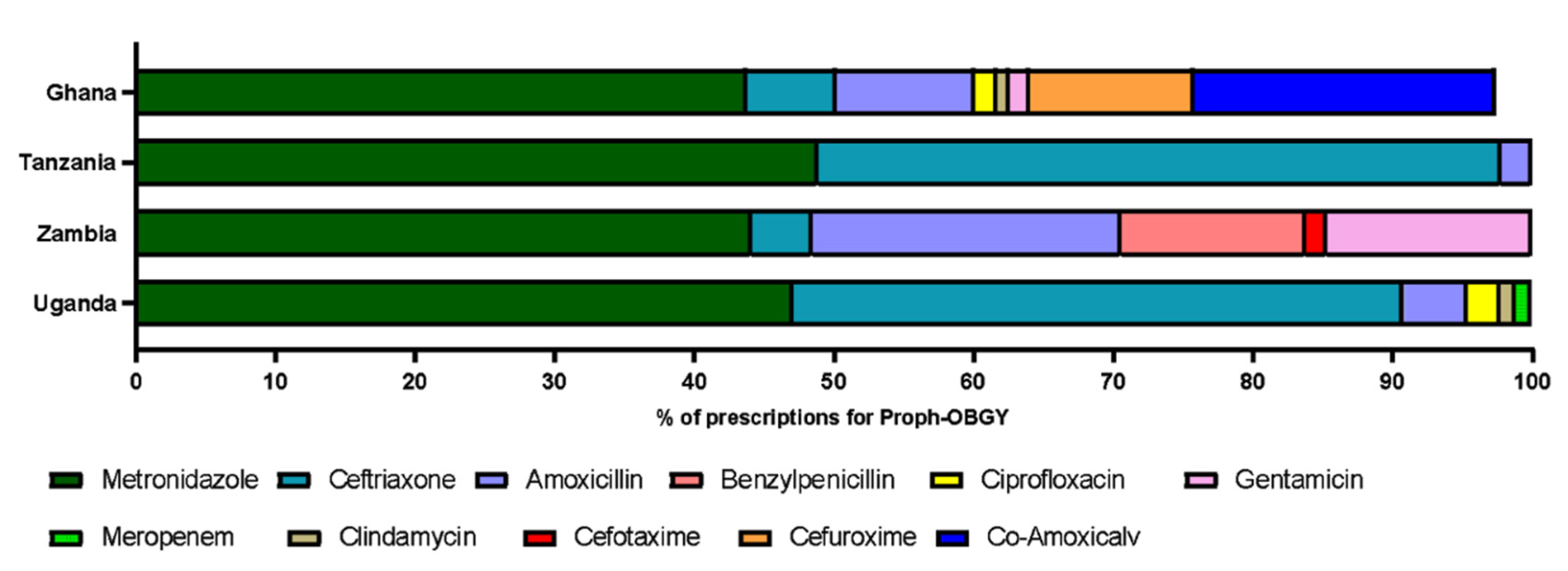
The antibiotics most commonly prescribed across hospitals in all four countries in the current study were metronidazole and ceftriaxone, with metronidazole being the most prescribed antibiotic across Ghanaian hospitals. These findings are supported by data from the Pauwels et al. study across 69 countries, where ceftriaxone was the most commonly used antibiotic for therapeutic use on adult wards worldwide. In the same study, up to 24% of prescriptions for surgical prophylaxis in sub-Saharan Africa were for metronidazole, followed by ceftriaxone (23%) [
23]. A PPS carried at the Korle-Bu Teaching Hospital in Ghana (2018) reported metronidazole as the most frequently prescribed antibiotic, followed by amoxicillin-clavulanic acid, cephalosporins (ceftriaxone, cefuroxime), and cloxacillin [
26]. A PPS in Kenya also recorded a higher use of nitroimidazoles compared to beta-lactam antibiotics [
27]. Furthermore, a PPS in three hospitals in north-eastern Tanzania reported ceftriaxone, metronidazole, and penicillin as the most prescribed antibiotics [
28].
Metronidazole is effective in the treatment of a broad range of anaerobic infections which may be more common in African countries [
29]. Metronidazole was used in addition to co-amoxiclav, so this could perhaps be an area to target to reduce use if anaerobic infections are covered by use of other antibiotics. This highlights that it might be useful to increase the awareness and understanding of antibiotic sensitivity. The findings presented here show that metronidazole was primarily prescribed for prophylaxis for obstetrics and gynaecology. Published data demonstrate a similarity between the most commonly prescribed antibiotics in PPSs carried out in other low-income countries. This could be explained by the affordability, availability, and the spectrum of activity of metronidazole and ceftriaxone, as well as their suitability for prophylaxis in certain obstetric and gynaecological procedures [
30]. However, the broad-spectrum activity of some antibiotics, particularly cephalosporins, can lead to the over-growth of other bacteria that are resistant to their activity, for example
Clostridiodies difficile, methicillin-resistant
Staphylococcus aureus (MRSA), and vancomycin-resistant enterococci (VRE) [
31,
32]. The use of cephalosporins, in particular, and third-generation drugs such as ceftriaxone, are linked to the rise in incidence of extended-spectrum beta-lactamase (ESBLs)-producing bacteria, leading to a reduction of effective antibiotics [
33,
34]. Therefore, there remains a need to evaluate prescriber’s choices and the frequent prescription of ceftriaxone, which falls within the Watch group of antibiotics in the WHO AWaRe categories.
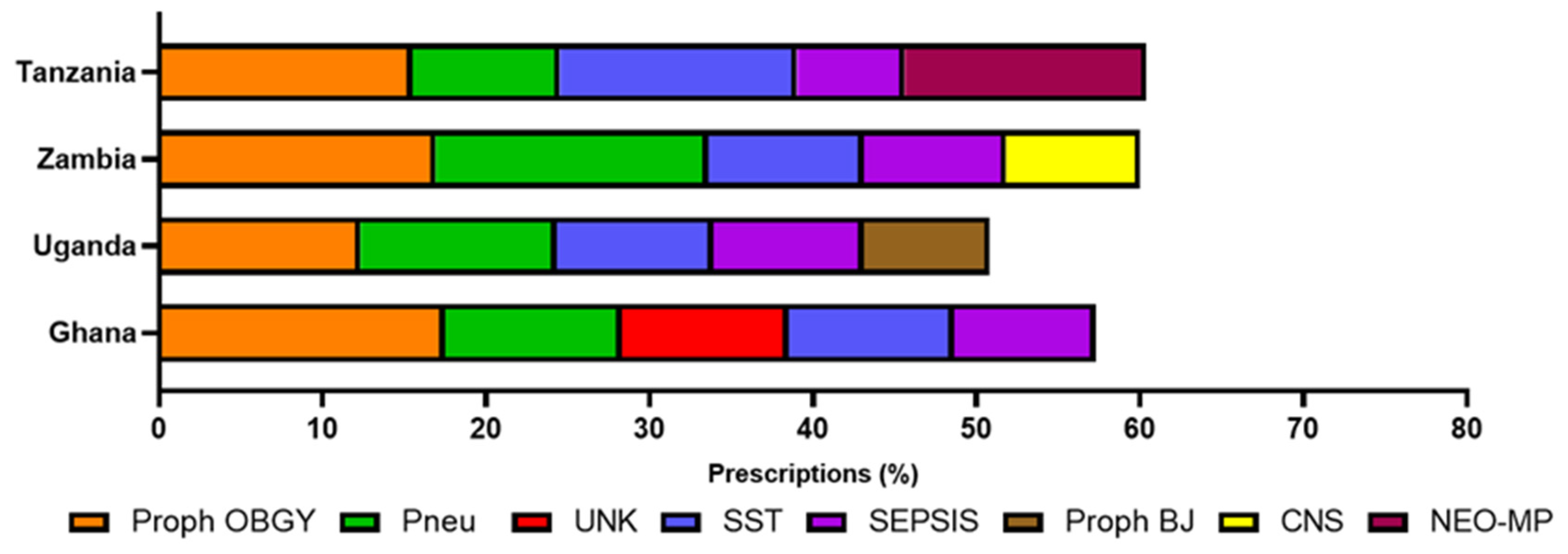
Reasons for antimicrobial prescribing in other published studies demonstrate a similar pattern to the current study, with lower respiratory tract infections and medical and surgical prophylaxis presented as common reasons for prescribing [
24,
25]. Prophylaxis for obstetric or gynaecological surgery was the most frequent reason for prescribing in the current study. Although the reasons for antimicrobial prescribing were similar across all four countries, Uganda had the highest prescription rates for antimalarials, drugs for the treatment of tuberculosis (TB). The WHO Global Tuberculosis Report (2020) reported Zambia having the highest incidence of TB (of the four countries included here) in 2019 (300–499 incidences per 100,000 population per year), followed by Tanzania (200–299 incidences per 100,000 population per year) and Ghana and Uganda having similar, lower rates (10–99 incidences per 100,000 population per year) [
35]. It is possible that there were localised TB and malaria outbreaks in the regions where the Ugandan hospitals were, but data are not available to confirm or deny this. This data may also be influenced by the time of year the PPS was carried out. If the PPS was conducted in the rainy season, then prescriptions for antimalarials might be higher than if the PPS was done in the dry seasons. The reason for this could also be that TB detection methods may be more robust in Uganda, which may explain the lower prevalence of disease but higher use of drugs. Further analysis and PPS would be required to explain the higher observed rates for unclassified antimicrobials and drugs used in the treatment of TB and malaria seen in Uganda. Antimicrobials were often prescribed when indication was documented (
Figure 2). There is a need to improve diagnostic capacity as diagnostic uncertainty might lead to the increase of antimicrobial prescribing [
36].
From the 4376 admitted inpatients across the 4 countries, 5.4% were treated with antibiotics for systemic use for at least one healthcare-associated infection (HCAI). Out of all therapeutic prescribing, community acquired infections were the most common reason for antimicrobial use. The rates of HCAI were similar to a large study conducted across acute care facilities in 28 countries in the EU/EAA, where 6.5% of patients had at least one HCAI [
37]. Although the European study was conducted over a much larger sample group, the data show a trend towards similar rates of HCAI in the data presented in this study.
The chi-squared test of association revealed significant associations between age, gender, countries, and AWaRe categories. Although the exact nature of the relationship between variables is uncertain, the summary statistics
(Supplementary Material: Tables S3–S5) provide more insight into these associations. As observed from descriptive analysis, reasons for antibiotic prescribing differ across populations with some age-specific indications such as ‘medical prophylaxis for new-born risk factors’ mostly observed in Tanzania and Uganda and gender-specific indications such as ‘prophylaxis for obstetric or gynaecological surgery’ observed across all countries. While these partly explain significant associations between antibiotic prescribing, gender, and age in specific countries and the general population, our results reflect country-specific trends worthy of further investigation.
Through the Global PPS programme and CwPAMS (for the participating hospitals), all partnerships and additional hospitals in Ghana and Zambia have demonstrated the strengthening of their healthcare workforce knowledge and capacity (
Table 7) in the areas of antimicrobial use surveillance and AMS. Prior to the programme, although other hospitals had collated antimicrobial use data through PPS methodology, only one hospital in the four countries had previously conducted data collection to the scale of the Global PPS.
Translating PPS findings into contextualised interventions can be challenging but all CwPAMS health partnerships and hospitals involved have provided information regarding key AMS interventions taken as a result of the Global PPS undertaken at their institutions. These are summarised in
Table 7 (for the full text, see
Supplementary Data). In an evaluation of the impact of the Global-PPS on local AMS programmes, prolonged surgical antibiotic prophylaxis was the most common target for improvement identified [
38]. This study also highlights the need to focus on prolonged surgical antibiotic prophylaxis considering that prescriptions for more than one day for surgical prophylaxis were common. However, antibiotics are only one component that can be used to reduce SSI. The inability to ensure a sterile environment and optimal IPC conditions may result in overuse or antibiotics.
Variations in quality indicators were observed across countries. Consistent with this study, the PPS in 6 reference hospitals in Tanzania observed an 84% adherence of antibiotic prescriptions to the National Standard Treatment Guideline [
24]. Similarly, a multi-centre PPS in Ghana also recorded a level of non-compliance to national antimicrobial standard treatment guidelines [
39]. The variations observed could be influenced by varying national antimicrobial prescribing policies, hospital protocols and the effectiveness of antimicrobial stewardship intervention programs in study centres across all four countries.
The consistency of data collection via the G-PPS methodology adds rigor and validity to the data presented here. The study demonstrates inclusivity with data obtained from 17 hospitals across four countries in 3 African regions, coupled with a good representation of gender, age groups, and hospital sections. In addition, data were collected by trained health professionals working, for the most part, as part of the Commonwealth Partnerships for Antimicrobial Stewardship.
4. Materials and Methods
Training on the collection of surveillance data for the G-PPS reported in this paper was provided to the CwPAMS health partnerships by the Global PPS team and the CPA, supporting the development of evidence-based standards, guidelines, protocols and the development of a mentorship programme to support sustainability. UK volunteers who had experience of PPS also provided mentorship and in-country support during their visits to Ghana, Uganda, Zambia, and Tanzania. Data collection was carried out by volunteers from individual health partnerships. PPS were conducted between May and December 2019, using the G-PPS methodology as described elsewhere [
18]. Data from 17 hospitals across four countries: ten in Ghana, four in Uganda, two in Zambia and one in Tanzania were collected and analysed. Follow-up data were collected in a second PPS for two hospitals but only the data from the first survey are included here.
Age of patients were defined as: adult (≥18 years) Child (>1 month–≤17 years) or neonate (≤1 month). Gender, age, diagnosis (reason for prescribing), indication (therapeutic versus prophylactic prescribing), routes of administration, prescribed antimicrobials dosing regimen, and causative microorganisms were all recorded. Data collection also included a set of prescription-related quality indicators; Prescriptions with a documented stop/review date, prescriptions with a documented indication, prescriptions that were guideline compliant and prescriptions for which no guidelines were available. The G-PPS data collection form is available via:
https://www.global-pps.com/documents/ (accessed on 15 September 2021).
Hospitals were classified as primary, secondary, or tertiary care hospitals. All inpatients admitted at 8 a.m. on the day of the PPS were included and data were analysed by country and ward type. The included wards were neonatal medical and intensive-care units, paediatric medical, surgical or haematology-oncology ward and intensive-care units and adult medical, pneumology, surgical, haematology-oncology wards, and intensive-care units.
Prescribed antimicrobials were divided into four main categories using the WHO AWaRe classification [
14] and further grouped using the 2021 WHO ATC code classification system [
20]. AWaRe groups were Access, Watch, Reserve and Not Recommended. Those that were not included in the classification were recorded as unclassified. Antimicrobials were grouped into therapeutic subgroups (ATC 2 level) following the WHO ATC classification system [
20]. The therapeutic subgroups were antibacterials for systemic use (J01), antimycotics and antifungals for systemic use (J02 and D01BA including griseofulvin and terbinafine), drugs for treatment of tuberculosis (J04A), antibiotics used as intestinal anti-infectives (A07AA), antiprotozoals used as antibacterial agents, nitroimidazole derivatives (P01AB), antivirals for systemic use (J05) and antimalarials (P01B).
Antimicrobial stewardship interventions as a result of PPS data: leads of all hospitals were asked to provide a short summary of AMS interventions, detailing the actions taken and any follow up data as a result of the PPS.
Data analysis: The results were analyzed descriptively and analytically using the R software (version 4.1.0) and Microsoft Excel (2016). Antimicrobial use prevalence rates were reported by calculating the number of patients on at least one antimicrobial relative to the number of admitted patients at the time of the PPS using Microsoft Excel (2016). The chi-squared test of association was conducted to compare national data on antimicrobial use and identify associations between dependent and independent variables within the dataset using the R software. The tests investigated the association between countries, gender, age groups, and antibiotic prescription across the AWaRe categories. Age was split into three categories namely: neonates (>1 month), children (1 month–17 years), and adults (18 years and above). Statistical significance was set at p < 0.05.
Ethics: Formal ethics approval was not required at any hospital as there was no direct patient contact and all data were anonymized. All sites obtained approval from their respective hospital administration. Ethics review and approval was sought and obtained in Uganda and administrative clearance by the participating hospitals was also given. For the four additional sites in Ghana, formal ethical approval was received.


 ,
, 





{kind=link}
{kind=link}
{kind=link}