
Use of Dalbavancin in Skin, Bone and Joint Infections: A Real-Life Experience in an Italian Center

Abstract
:1. Introduction
2. Results
2.1. Patients’ Characteristics, Infection and Microorganisms
2.2. Treatment Characteristics
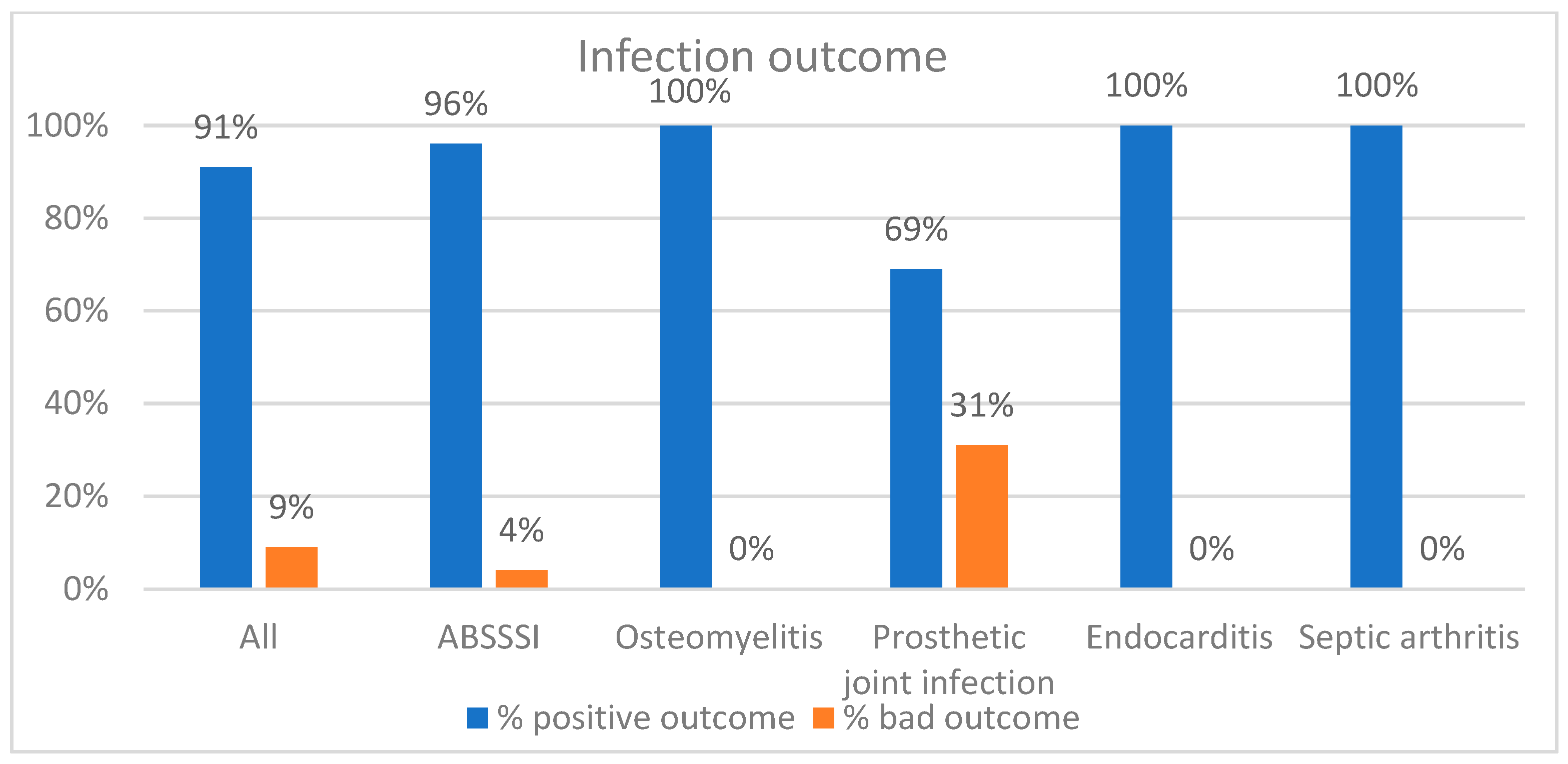
2.3. Outcome and Tolerability
2.4. Comparison between ABSSSI and Non-ABSSSI Patients
3. Discussion
4. Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Simonetti, O.; Rizzetto, G.; Molinelli, E.; Cirioni, O.; Offidani, A. Review: A Safety Profile of Dalbavancin for On- and Off-Label Utilization. Ther. Clin. Risk Manag. 2021, 17, 223–232. [Google Scholar] [CrossRef]
- Dunne, M.W.; Puttagunta, S.; Giordano, P.; Krievins, D.; Zelasky, M.; Baldassarre, J. A Randomized Clinical Trial of Single-Dose Versus Weekly Dalbavancin for Treatment of Acute Bacterial Skin and Skin Structure Infection. Clin. Infect. Dis. 2016, 62, 545–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, M.Z.; Dryden, M.; Gottlieb, T.; Tattevin, P.; Gould, I.M. Recently Approved Antibacterials for Methicillin-Resistant Staphylococcus Aureus (MRSA) and Other Gram-Positive Pathogens: The Shock of the New. Int. J. Antimicrob. Agents 2017, 50, 303–307. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, O.; Lucarini, G.; Morroni, G.; Orlando, F.; Lazzarini, R.; Zizzi, A.; Brescini, L.; Provinciali, M.; Giacometti, A.; Offidani, A.; et al. New Evidence and Insights on Dalbavancin and Wound Healing in a Mouse Model of Skin Infection. Antimicrob. Agents Chemother. 2020, 64, e02062-19, PMCID:PMC7179315. [Google Scholar] [CrossRef] [PubMed]
- Bassetti, M.; Peghin, M.; Carnelutti, A.; Righi, E. The Role of Dalbavancin in Skin and Soft Tissue Infections. Curr. Opin. Infect. Dis. 2018, 31, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.Y.; Zervos, M.J.; Vazquez, J.A. Dalbavancin: A Novel Antimicrobial. Int. J. Clin. Pract. 2007, 61, 853–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leighton, A.; Gottlieb, A.B.; Dorr, M.B.; Jabes, D.; Mosconi, G.; VanSaders, C.; Mroszczak, E.J.; Campbell, K.C.M.; Kelly, E. Tolerability, Pharmacokinetics, and Serum Bactericidal Activity of Intravenous Dalbavancin in Healthy Volunteers. Antimicrob. Agents Chemother. 2004, 48, 940–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunne, M.W.; Puttagunta, S.; Sprenger, C.R.; Rubino, C.; Van Wart, S.; Baldassarre, J. Extended-Duration Dosing and Distribution of Dalbavancin into Bone and Articular Tissue. Antimicrob. Agents Chemother. 2015, 59, 1849–1855. [Google Scholar] [CrossRef] [Green Version]
- Seltzer, E.; Dorr, M.B.; Goldstein, B.P.; Perry, M.; Dowell, J.A.; Henkel, T. Dalbavancin Skin and Soft-Tissue Infection Study Group Once-Weekly Dalbavancin versus Standard-of-Care Antimicrobial Regimens for Treatment of Skin and Soft-Tissue Infections. Clin. Infect. Dis. 2003, 37, 1298–1303. [Google Scholar] [CrossRef] [Green Version]
- Bouza, E.; Valerio, M.; Soriano, A.; Morata, L.; Carus, E.G.; Rodríguez-González, C.; Hidalgo-Tenorio, M.C.; Plata, A.; Muñoz, P.; Vena, A.; et al. Dalbavancin in the Treatment of Different Gram-Positive Infections: A Real-Life Experience. Int. J. Antimicrob. Agents 2018, 51, 571–577. [Google Scholar] [CrossRef]
- Rappo, U.; Puttagunta, S.; Shevchenko, V.; Shevchenko, A.; Jandourek, A.; Gonzalez, P.L.; Suen, A.; Mas Casullo, V.; Melnick, D.; Miceli, R.; et al. Dalbavancin for the Treatment of Osteomyelitis in Adult Patients: A Randomized Clinical Trial of Efficacy and Safety. Open Forum Infect. Dis. 2019, 6, ofy331. [Google Scholar] [CrossRef]
- Tobudic, S.; Forstner, C.; Burgmann, H.; Lagler, H.; Steininger, C.; Traby, L.; Vossen, M.G.; Winkler, S.; Thalhammer, F. Real-World Experience with Dalbavancin Therapy in Gram-Positive Skin and Soft Tissue Infection, Bone and Joint Infection. Infection 2019, 47, 1013–1020. [Google Scholar] [CrossRef] [Green Version]
- Wunsch, S.; Krause, R.; Valentin, T.; Prattes, J.; Janata, O.; Lenger, A.; Bellmann-Weiler, R.; Weiss, G.; Zollner-Schwetz, I. Multicenter Clinical Experience of Real Life Dalbavancin Use in Gram-Positive Infections. Int. J. Infect. Dis. 2019, 81, 210–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krsak, M.; Morrisette, T.; Miller, M.; Molina, K.; Huang, M.; Damioli, L.; Pisney, L.; Wong, M.; Poeschla, E. Advantages of Outpatient Treatment with Long-Acting Lipoglycopeptides for Serious Gram-Positive Infections: A Review. Pharmacotherapy 2020, 40, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Morata, L.; Cobo, J.; Fernández-Sampedro, M.; Guisado Vasco, P.; Ruano, E.; Lora-Tamayo, J.; Sánchez Somolinos, M.; González Ruano, P.; Rico Nieto, A.; Arnaiz, A.; et al. Safety and Efficacy of Prolonged Use of Dalbavancin in Bone and Joint Infections. Antimicrob. Agents Chemother. 2019, 63, e02280-18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrisette, T.; Miller, M.A.; Montague, B.T.; Barber, G.R.; McQueen, R.B.; Krsak, M. On- and off-label utilization of dalbavancin and oritavancin for Gram-positive infections. J. Antimicrob. Chemother. 2019, 74, 2405–2416. [Google Scholar] [CrossRef]
- Bork, J.T.; Heil, E.L.; Berry, S.; Lopes, E. Dalbavancin Use in Vulnerable Patients Receiving Outpatient Parenteral Antibiotic Therapy for Invasive Gram-Positive Infections. Infect. Dis. Ther. 2019, 8, 171–184. [Google Scholar] [CrossRef] [Green Version]
- Dinh, A.; Duran, C.; Pavese, P.; Khatchatourian, L.; Monnin, B.; Bleibtreu, A.; Denis, E.; Etienne, C.; Rouanes, N.; Mahieu, R.; et al. French National Cohort of First Use of Dalbavancin: A High Proportion of off-Label Use. Int. J. Antimicrob. Agents 2019, 54, 668–672. [Google Scholar] [CrossRef]
- Bai, F.; Aldieri, C.; Cattelan, A.; Raumer, F.; Di Meco, E.; Moioli, M.C.; Tordato, F.; Morelli, P.; Borghi, F.; Rizzi, M.; et al. Efficacy and Safety of Dalbavancin in the Treatment of Acute Bacterial Skin and Skin Structure Infections (ABSSSIs) and Other Infections in a Real-Life Setting: Data from an Italian Observational Multicentric Study (DALBITA Study). Expert Rev. Anti-Infect. Ther. 2020, 18, 1271–1279. [Google Scholar] [CrossRef]
- Murillo, Ó.; El-Haj, C. Analysis of dalbavancin in animal models. Enferm. Infecc. Microbiol. Clin. 2017, 35 (Suppl. 1), 28–32. [Google Scholar] [CrossRef]
- Barnea, Y.; Lerner, A.; Aizic, A.; Navon-Venezia, S.; Rachi, E.; Dunne, M.W.; Puttagunta, S.; Carmeli, Y. Efficacy of Dalbavancin in the Treatment of MRSA Rat Sternal Osteomyelitis with Mediastinitis. J. Antimicrob. Chemother. 2016, 71, 460–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buzón-Martín, L.; Zollner-Schwetz, I.; Tobudic, S.; Cercenado, E.; Lora-Tamayo, J. Dalbavancin for the Treatment of Prosthetic Joint Infections: A Narrative Review. Antibiotics 2021, 10, 656. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | N |
|---|---|
| Age, years, median (IQR) | 61 (52–73) |
| Gender | |
| Male | 34 (62%) |
| Female | 21 (38%) |
| Department | |
| Medical | 47 (85%) |
| ICU | 0 (0) |
| Surgical | 8 (15%) |
| Underlying diseases | |
| Diabetes mellitus | 9 (16%) |
| Cardiovascular disease | 34 (62%) |
| COPD | 6 (11%) |
| Neurological disease | 6 (11%) |
| Solid-organ malignancy | 6 (11%) |
| Gastrointestinal disease | 0 (0) |
| Hematologic malignancy | 9 (16%) |
| Chronic renal failure | 5 (9%) |
| Liver disease | 6 (11%) |
| Chemotherapy | 3 (5%) |
| Immunosuppressive therapy | 3 (5%) |
| Steroid therapy | 6 (11%) |
| Solid-organ transplant | 0 (0) |
| Bone marrow transplant | 2 (4%) |
| Acute comorbidity | 0 (0) |
| Charlson comorbidity index (median IQR) | 3 (2–5) |
| Infection type | |
| Prosthetic joint infection | 13 (24%) |
| ABSSSI | 28 (51%) |
| Osteomyelitis | 8 (14%) |
| Endocarditis | 1 (2%) |
| Septic arthritis | 5 (9%) |
| Pathogens | |
| MSSA | 1 (2%) |
| MRSA | 9 (16%) |
| Enterococcus faecalis | 2 (4%) |
| Enterococcus faecium | 0 (0) |
| S. epidermidis | 3 (5%) |
| MRSE | 1 (2%) |
| Polimicrobial infection a | 6 (11%) |
| Other species b | 8 (15%) |
| Empirical | 25 (45%) |
| Previous Antibiotic Treatment | N |
|---|---|
| N (%) patients who had received previous antibiotic treatment | 53 (96%) |
| N antibiotics received before dalbavancin therapy, median (IQR) | 1 (1–2) |
| Days of antibiotic treatment before dalbavancin therapy, median (IQR) | 7 (1–13) |
| Total n days of previous antibiotic treatment, median (IQR) | 14 (7–30) |
| Reasons for dalbavancin use | |
| N (%) clinical and/or microbiological failure of previous antibiotic therapy | 25 (45%) |
| N (%) side effects of previous antibiotic therapy | 1 (2%) |
| N (%) multidrug bacterials | 2 (4%) |
| N (%) poor compliance/early discharge | 27 (49%) |
| Dalbavancin therapy | |
| N (%) 1 × 1500 mg | 29 (53%) |
| N (%) 1 × 1500 mg d1 + d8 | 3 (5%) |
| N (%) 1 × 1500 mg d1 + d14 | 10 (18%) |
| N (%) other regimens (multiple administrations) | 13 (24%) |
| N dalbavancin administrations, median (IQR) | 1 (1–2) |
| N (%) concomitant antibiotic therapy | 11 (20%) |
| N (%) Adverse events | 1 (2%) |
| Outcome | |
| N (%) successful clinical outcome | 50 (91%) |
| N (%) treatment failure | 5 (9%) |
| Age (Years) | Type of Infection | Microorganism | Number of Administrations | Concomitant Antibiotics | Description |
|---|---|---|---|---|---|
| 72 | PJI | Undetermined | 2 | No | Knee replacement R |
| 68 | PJI | MRSA | 1 | No | Hip replacement L |
| 59 | PJI | Mixed | 3 | Yes | Hip replacement R |
| 65 | PJI | Mixed | 9 | Yes | Hip replacement R |
| 59 | ABSSSI | Mixed | 1 | Yes | Sternal post-operative wound following myocardial revascularization with Y graft |
| ABSSSI (n = 28) | Other Sites of Infection (n = 27) | p-Value | |
|---|---|---|---|
| Age, Years, Median (IQR) | 56 (52–73) | 67 (52–73) | 0.04 |
| Gender (male) | 16 (57%) | 18 (67%) | 0.47 |
| Charlson Comorbidity Index ≥ 3 | 18 (64%) | 22 (81%) | 0.15 |
| WBC, ×109/L, median (IQR) | 8050 (5610–9197) | 6220 (5645–9147) | 0.02 |
| CRP, mg/L, median (IQR) | 3 (1.2–5.17) | 3 (1.07–5.12) | 0.46 |
| Ward Surgical Medical ICU | 8 (29%) 20 (71%) | 0 (0%) 27 (100%) | 0.007 |
| Length of hospital stay, days (median IQR) | 15.5 (10–38.5) | 24 (10–38) | 0.87 |
| Previous antibiotic therapies | 27 (96%) | 26 (96%) | 0.97 |
| N of days of previous antibiotic therapies | 10 (8–30) | 15 (7.5–30) | 0.18 |
| N of days of antibiotics before start of dalbavancin therapy (median IQR) | 5.5 (1–12) | 10 (1–13) | 0.39 |
| N of dalbavancin administrations (median) | 1 (1–2) | 2 (1–2) | 0.0002 |
| Concomitant antibiotic therapy | 5 (18%) | 6 (22%) | 0.78 |
| Outcome Successful clinical outcome Treatment failure | 27 (96%) 1 (4%) | 23 (85%) 4 (15%) | 0.96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brescini, L.; Della Martera, F.; Morroni, G.; Mazzanti, S.; Di Pietrantonio, M.; Mantini, P.; Candelaresi, B.; Pallotta, F.; Olivieri, S.; Iencinella, V.; et al. Use of Dalbavancin in Skin, Bone and Joint Infections: A Real-Life Experience in an Italian Center. Antibiotics 2021, 10, 1129. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091129
Brescini L, Della Martera F, Morroni G, Mazzanti S, Di Pietrantonio M, Mantini P, Candelaresi B, Pallotta F, Olivieri S, Iencinella V, et al. Use of Dalbavancin in Skin, Bone and Joint Infections: A Real-Life Experience in an Italian Center. Antibiotics. 2021; 10(9):1129. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091129
Chicago/Turabian StyleBrescini, Lucia, Filippo Della Martera, Gianluca Morroni, Sara Mazzanti, Maria Di Pietrantonio, Paolo Mantini, Bianca Candelaresi, Francesco Pallotta, Silvia Olivieri, Valentina Iencinella, and et al. 2021. "Use of Dalbavancin in Skin, Bone and Joint Infections: A Real-Life Experience in an Italian Center" Antibiotics 10, no. 9: 1129. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics10091129