
Clindamycin Efficacy for Cutibacterium acnes Shoulder Device-Related Infections

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Population
2.2. Surgical Management of the Population
2.3. Microbiology Results and Resistance Profile
2.4. Antibiotic Therapy
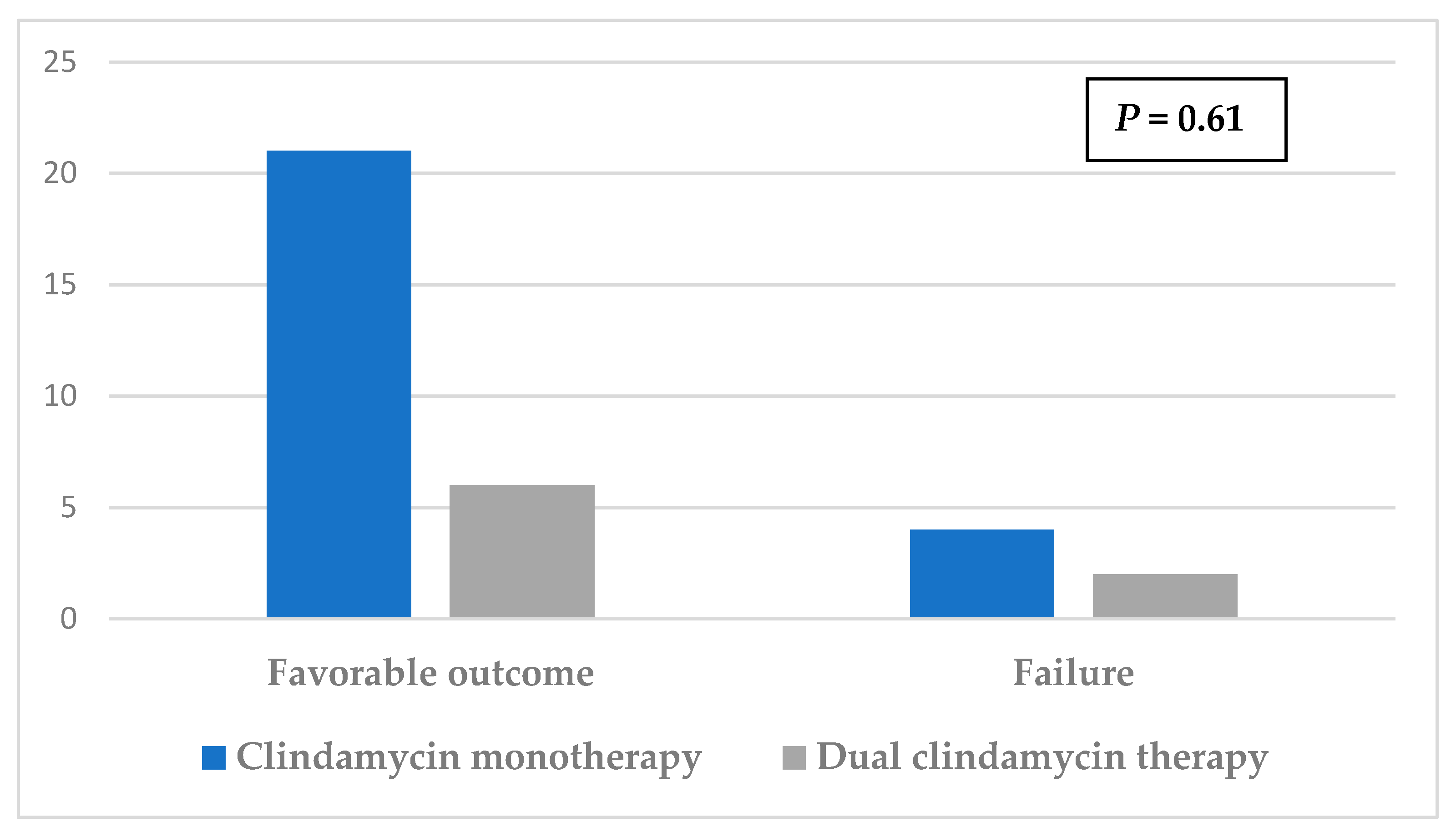
2.5. Treatment Outcome According to Clindamycin Use
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
- One shoulder surgical procedure (including arthroscopy) performed between 2011 and 2019 in patients with a history of shoulder implants RTSA, ATSA, hemiarthroplasties, and osteosyntheses;
- At least one intraoperative sample positive for C. acnes in culture. We excluded all other types of infection and primary surgery.
4.2. Follow-up and Treatment Outcome
4.3. Data Collection
4.4. Antibiotic Susceptibility Tests
4.5. Clindamycin Treatment
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chebili, F. Implants Articulaires D’épaule. HAS. 25 Mars 2014. Available online: https://www.has-sante.fr/upload/docs/application/pdf/2014-04/texte_court_du_rapport_devaluation_implants_articulaires_depaule.pdf (accessed on 17 March 2022).
- Del Pozo, J.L.; Patel, R. Clinical practice. Infection associated with prosthetic joints. N. Engl. J. Med. 2009, 361, 787–794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohsali, K.I.; Bois, A.J.; Wirth, M.A. Complications of Shoulder Arthroplasty. J. Bone Jt. Surg. Am. 2017, 99, 256–269. [Google Scholar] [CrossRef] [PubMed]
- Darouiche, R.O. Treatment of infections associated with surgical implants. N. Engl. J. Med. 2004, 350, 1422–1429. [Google Scholar] [CrossRef]
- Paxton, E.S.; Green, A.; Krueger, V.S. Periprosthetic Infections of the Shoulder: Diagnosis and Management. J. Am. Acad. Orthop. Surg. 2019, 27, e935–e944. [Google Scholar] [CrossRef] [PubMed]
- Nelson, G.N.; Davis, D.E.; Namdari, S. Outcomes in the treatment of periprosthetic joint infection after shoulder arthroplasty: A systematic review. J. Shoulder Elbow Surg. 2016, 25, 1337–1345. [Google Scholar] [CrossRef] [PubMed]
- Grice, E.A.; Kong, H.H.; Conlan, S.; Deming, C.B.; Davis, J.; Young, A.C.; NISC Comparative Sequencing Program; Bouffard, G.G.; Blakesley, R.W.; Murray, P.R.; et al. Topographical and temporal diversity of the human skin microbiome. Science 2009, 324, 1190–1192. [Google Scholar] [CrossRef] [Green Version]
- Piggott, D.A.; Higgins, Y.M.; Melia, M.T.; Ellis, B.; Carroll, K.C.; McFarland, E.G.; Auwaerter, P.G. Characteristics and Treatment Outcomes of Propionibacterium acnes Prosthetic Shoulder Infections in Adults. Open Forum Infect. Dis. 2016, 3, ofv191. [Google Scholar] [CrossRef] [Green Version]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Infectious Diseases Society of America Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [Green Version]
- De Velde, F.; de Winter, B.C.M.; Koch, B.C.P.; van Gelder, T.; Mouton, J.W.; COMBACTE-NET consortium. Non-linear absorption pharmacokinetics of amoxicillin: Consequences for dosing regimens and clinical breakpoints. J. Antimicrob. Chemother. 2016, 71, 2909–2917. [Google Scholar] [CrossRef] [Green Version]
- De Lastours, V.; Fantin, B. Impact of fluoroquinolones on human microbiota. Focus on the emergence of antibiotic resistance. Future Microbiol. 2015, 10, 1241–1255. [Google Scholar] [CrossRef]
- Landersdorfer, C.B.; Bulitta, J.B.; Kinzig, M.; Holzgrabe, U.; Sörgel, F. Penetration of antibacterials into bone: Pharmacokinetic, pharmacodynamic and bioanalytical considerations. Clin. Pharm. 2009, 48, 89–124. [Google Scholar] [CrossRef] [PubMed]
- Vollmer, N.J.; Rivera, C.G.; Stevens, R.W.; Oravec, C.P.; Mara, K.C.; Suh, G.A.; Osmon, D.R.; Beam, E.N.; Abdel, M.P.; Virk, A. Safety and Tolerability of Fluoroquinolones in Patients with Staphylococcal Periprosthetic Joint Infections. Clin. Infect. Dis. 2021, 73, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Trampuz, A.; Zimmerli, W. New strategies for the treatment of infections associated with prosthetic joints. Curr. Opin. Investig. Drugs 2005, 6, 185–190. [Google Scholar]
- Saeed, K.; McLaren, A.C.; Schwarz, E.M.; Antoci, V.; Arnold, W.V.; Chen, A.F.; Clauss, M.; Esteban, J.; Gant, V.; Hendershot, E.; et al. 2018 international consensus meeting on musculoskeletal infection: Summary from the biofilm workgroup and consensus on biofilm related musculoskeletal infections. J. Orthop. Res. 2019, 37, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- Courjon, J.; Demonchy, E.; Cua, E.; Bernard, E.; Roger, P.-M. Efficacy and safety of clindamycin-based treatment for bone and joint infections: A cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 2513–2518. [Google Scholar] [CrossRef]
- Schneider, P.; Visconti, J.A. Pharmacokinetics in drug therapy III: Clindamycin dosage regimens for treatment of chronic osteomyelitis. Am. J. Hosp. Pharm. 1977, 34, 980–983. [Google Scholar] [CrossRef]
- Zeller, V.; Ghorbani, A.; Strady, C.; Leonard, P.; Mamoudy, P.; Desplaces, N. Propionibacterium acnes: An agent of prosthetic joint infection and colonization. J. Infect. 2007, 55, 119–124. [Google Scholar] [CrossRef]
- Jacobs, A.M.E.; Hooff, M.L.V.; Meis, J.F.; Vos, F.; Goosen, J.H.M. Treatment of prosthetic joint infections due to Propionibacterium. Acta Orthop. 2016, 87, 60–66. [Google Scholar] [CrossRef] [Green Version]
- Levy, P.Y.; Fenollar, F.; Stein, A.; Borrione, F.; Cohen, E.; Lebail, B.; Raoult, D. Propionibacterium acnes postoperative shoulder arthritis: An emerging clinical entity. Clin. Infect. Dis. 2008, 46, 1884–1886. [Google Scholar] [CrossRef] [Green Version]
- Vilchez, H.H.; Escudero-Sanchez, R.; Fernandez-Sampedro, M.; Murillo, O.; Auñón, Á.; Rodríguez-Pardo, D.; Jover-Sáenz, A.; del Toro, M.D.; Rico, A.; Falgueras, L.; et al. Prosthetic Shoulder Joint Infection by Cutibacterium acnes: Does Rifampin Improve Prognosis? A Retrospective, Multicenter, Observational Study. Antibiotics 2021, 10, 475. [Google Scholar] [CrossRef]
- Rosi, E.; Pescitelli, L.; Ricceri, F.; Di Cesare, A.; Novelli, A.; Pimpinelli, N.; Prignano, F. Clindamycin as unique antibiotic choice in Hidradenitis Suppurativa. Dermatol. Ther. 2019, 32, e12792. [Google Scholar] [CrossRef] [PubMed]
- An, J.H.; Moon, S.J.; Shin, J.U.; Kim, D.H.; Yoon, M.S.; Lee, H.J. Clindamycin Mono-Therapy of Hidradenitis Suppurativa Patients: A Single-Center Retrospective Study. Ann. Dermatol. 2021, 33, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Zeller, V.; Dzeing-Ella, A.; Kitzis, M.-D.; Ziza, J.-M.; Mamoudy, P.; Desplaces, N. Continuous clindamycin infusion, an innovative approach to treating bone and joint infections. Antimicrob. Agents Chemother. 2010, 54, 88–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groupe bibliographique de la SPILF [Bone and joint infections: Risk of clindamycin low concentration when combined with rifampicin]. Med. Mal. Infect. 2015, 45, 343. [CrossRef]
- Pradier, M.; Suy, F.; Issartel, B.; Dehecq, C.; Loiez, C.; Senneville, E. Quel traitement pour les infections de prothèse d’épaule à Cutibacterium acnes? Méd. Mal. Infect. 2018, 48, S33. [Google Scholar] [CrossRef]
- Holmberg, A.; Lood, R.; Mörgelin, M.; Söderquist, B.; Holst, E.; Collin, M.; Christensson, B.; Rasmussen, M. Biofilm formation by Propionibacterium acnes is a characteristic of invasive isolates. Clin. Microbiol. Infect. 2009, 15, 787–795. [Google Scholar] [CrossRef] [Green Version]
- Bayston, R.; Ashraf, W.; Barker-Davies, R.; Tucker, E.; Clement, R.; Clayton, J.; Freeman, B.J.C.; Nuradeen, B. Biofilm formation by Propionibacterium acnes on biomaterials in vitro and in vivo: Impact on diagnosis and treatment. J. Biomed. Mater. Res. A 2007, 81, 705–709. [Google Scholar] [CrossRef]
- Furustrand Tafin, U.; Corvec, S.; Betrisey, B.; Zimmerli, W.; Trampuz, A. Role of rifampin against Propionibacterium acnes biofilm in vitro and in an experimental foreign-body infection model. Antimicrob. Agents Chemother. 2012, 56, 1885–1891. [Google Scholar] [CrossRef] [Green Version]
- Bayston, R.; Nuradeen, B.; Ashraf, W.; Freeman, B.J.C. Antibiotics for the eradication of Propionibacterium acnes biofilms in surgical infection. J. Antimicrob. Chemother. 2007, 60, 1298–1301. [Google Scholar] [CrossRef] [Green Version]
- Kusejko, K.; Auñón, Á.; Jost, B.; Natividad, B.; Strahm, C.; Thurnheer, C.; Pablo-Marcos, D.; Slama, D.; Scanferla, G.; Uckay, I.; et al. The Impact of Surgical Strategy and Rifampin on Treatment Outcome in Cutibacterium Periprosthetic Joint Infections. Clin. Infect. Dis. 2021, 72, e1064–e1073. [Google Scholar] [CrossRef]
- Falstie-Jensen, T.; Daugaard, H.; Søballe, K.; Ovesen, J.; Arveschoug, A.K.; Lange, J. ROSA study group Labeled white blood cell/bone marrow single-photon emission computed tomography with computed tomography fails in diagnosing chronic periprosthetic shoulder joint infection. J. Shoulder Elbow Surg. 2019, 28, 1040–1048. [Google Scholar] [CrossRef] [PubMed]
- Boisrenoult, P. Cutibacterium acnes prosthetic joint infection: Diagnosis and treatment. Orthop. Traumatol. Surg. Res. 2018, 104, S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Ollivier, M.; Senneville, E.; Drancourt, M.; Argenson, J.N.; Migaud, H. Potential changes to French recommendations about peri-prosthetic infections based on the international consensus meeting (ICMPJI). Orthop. Traumatol. Surg. Res. 2014, 100, 583–587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parvizi, J. Reply to the Letter to the Editor: New Definition for Periprosthetic Joint Infection: From the Workgroup of the Musculoskeletal Infection Society. Clin. Orthop. Relat. Res. 2017, 475, 291. [Google Scholar] [CrossRef] [Green Version]
- Renz, N.; Mudrovcic, S.; Perka, C.; Trampuz, A. Orthopedic implant-associated infections caused by Cutibacterium spp.—A remaining diagnostic challenge. PLoS ONE 2018, 13, e0202639. [Google Scholar] [CrossRef]
- Beekman, P.D.A.; Katusic, D.; Berghs, B.M.; Karelse, A.; De Wilde, L. One-stage revision for patients with a chronically infected reverse total shoulder replacement. J. Bone Jt. Surg. Br. 2010, 92, 817–822. [Google Scholar] [CrossRef]
- Figueiredo, S. Infections de Prothèses Ostéo-Articulaires. Available online: https://www.mapar.org/article/1/Communication%20MAPAR/j3idw3b7/Infections%20de%20proth%c3%a8ses%20ost%c3%a9o-articulaires.pdf (accessed on 17 March 2022).
- McDowell, A.; Barnard, E.; Nagy, I.; Gao, A.; Tomida, S.; Li, H.; Eady, A.; Cove, J.; Nord, C.E.; Patrick, S. An expanded multilocus sequence typing scheme for propionibacterium acnes: Investigation of “pathogenic”, “commensal” and antibiotic resistant strains. PLoS ONE 2012, 7, e41480. [Google Scholar] [CrossRef] [Green Version]
- El Sayed, F.; Roux, A.-L.; Sapriel, G.; Salomon, E.; Bauer, T.; Gaillard, J.-L.; Rottman, M. Molecular Typing of Multiple Isolates Is Essential to Diagnose Cutibacterium acnes Orthopedic Device-related Infection. Clin. Infect. Dis. 2019, 68, 1942–1945. [Google Scholar] [CrossRef]
- Trecourt, A.; Brevet, M.; Champagnac, A.; Conrad, A.; Josse, J.; Dupieux-Chabert, C.; Valour, F.; Ferry, T. Plasma Cell Infiltration on Histopathological Samples of Chronic Bone and Joint Infections due to Cutibacterium acnes: A series of 21 Cases. J. Bone Jt. Infect. 2020, 5, 205–211. [Google Scholar] [CrossRef]
- Ferry, T.; Seng, P.; Mainard, D.; Jenny, J.-Y.; Laurent, F.; Senneville, E.; Grare, M.; Jolivet-Gougeon, A.; Bernard, L.; Marmor, S. The CRIOAc healthcare network in France: A nationwide Health Ministry program to improve the management of bone and joint infection. Orthop. Traumatol.: Surg. Res. 2019, 105, 185–190. [Google Scholar] [CrossRef]
- Achermann, Y.; Goldstein, E.J.C.; Coenye, T.; Shirtliff, M.E. Propionibacterium acnes: From commensal to opportunistic biofilm-associated implant pathogen. Clin. Microbiol. Rev. 2014, 27, 419–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | n = 48 |
|---|---|
| Age, years | 67 (12) |
| Male | 36 (75%) |
| Diabetic | 14 (29%) |
| Obesity IMC > 30 kg/m2 | 1 (2%) |
| Coronaropathy | 6 (13%) |
| Cirrhosis | 1 (2%) |
| Rhumatoid polyarthrites | 1 (2%) |
| Anticoagulant | 3 (6%) |
| Corticotherapy | 1 (2%) |
| RTSA | 30 (63%) |
| ATSA | 8 (17%) |
| Osteosynthesis | 5 (10%) |
| Hemiarthroplasty | 5 (10%) |
| Time since index arthroplasty, months | 24 (49.5) |
| Number of previous interventions, mean a | 1 |
| History of BJI at the same site | 6 (13%) |
| Local inflammation | 7 (15%) |
| Shoulder pain | 42 (88%) |
| C-reactive protein [mg/L] | 22.59 |
| Leucocytes [G/L] | 7.99 |
| Polymorphonuclear neutrophiles [G/L] | 5.71 |
| Antimicrobial Agent | Rate of Susceptible Strains (%) * |
|---|---|
| Beta-lactam + beta lactam inhibitor | 48/48 (100) |
| Moxifloxacin | 40/40 (100) |
| Rifampicin | 8/8 (100) |
| clindamycin | 47/48 (98) |
| Tetracycline | 48/48 (100) |
| Linezolid | 44/44 (100) |
| Medical and Surgical Treatment | Rate of Favorable Outcome (%) |
|---|---|
| Monotherapy + 2-stage surgery | 10/12 (83) |
| Dual therapy + 2-stage surgery | 4/5 (80) |
| Monotherapy + 1-stage surgery | 11/11 (100) |
| Dual therapy + DAIR | 2/3 (67) |
| Monotherapy + Abscess drainage | 0/1 (0) |
| Monotherapy + Absence of revision | 0/1 (0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Courdurié, A.; Lotte, R.; Ruimy, R.; Cauhape, V.; Carles, M.; Gauci, M.-O.; Boileau, P.; Courjon, J. Clindamycin Efficacy for Cutibacterium acnes Shoulder Device-Related Infections. Antibiotics 2022, 11, 608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050608
Courdurié A, Lotte R, Ruimy R, Cauhape V, Carles M, Gauci M-O, Boileau P, Courjon J. Clindamycin Efficacy for Cutibacterium acnes Shoulder Device-Related Infections. Antibiotics. 2022; 11(5):608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050608
Chicago/Turabian StyleCourdurié, Audrey, Romain Lotte, Raymond Ruimy, Vincent Cauhape, Michel Carles, Marc-Olivier Gauci, Pascal Boileau, and Johan Courjon. 2022. "Clindamycin Efficacy for Cutibacterium acnes Shoulder Device-Related Infections" Antibiotics 11, no. 5: 608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11050608