

Predictors of Vancomycin-Resistant Enterococcus spp. Intestinal Carriage among High-Risk Patients in University Hospitals in Serbia
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Sample Characteristics
2.2. Univariate Logistic Regression
2.3. Multivariate Logistic Regression
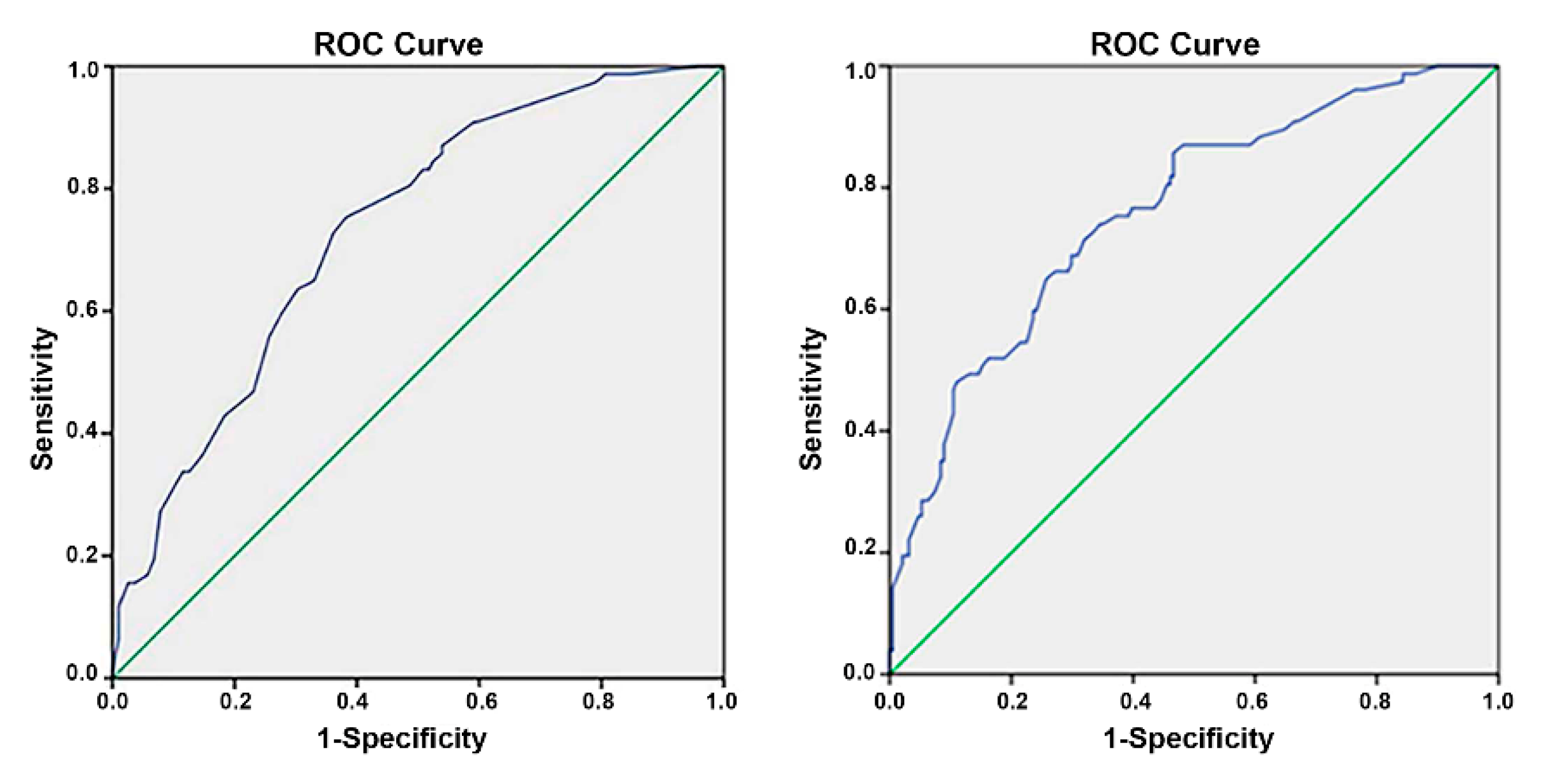
2.4. Evaluation of the Models
2.5. Validation of the Models
3. Discussion
4. Materials and Methods
4.1. Study Design, Setting, and Study Population
4.2. Sampling, Isolation, Identification, and Genotyping
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lebreton, F.; Willems, R.J.L.; Gilmore, M.S. Enterococcus Diversity, Origins in Nature, and Gut Colonization. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Gilmore, M.S., Clewell, D.B., Ike, Y., Shankar, N., Eds.; Eye and Ear Infirmary: Boston, MA, USA, 2014. [Google Scholar]
- European Centre for Disease Prevention and Control. Antimicrobial Resistance in the EU/EEA (EARS-Net). 2020. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2019 (accessed on 27 July 2022).
- European Centre for Disease Prevention and Control. Surveillance of Antimicrobial Resistance in Europe. ECDC: Stockholm, Sweden. 2019. Available online: https://www.ecdc.europa.eu/en/publications-data/surveillance-antimicrobial-resistance-europe-2020 (accessed on 27 July 2022).
- Tacconelli, E.; Carrara, E.; Savoldi, A.; Harbarth, S.; Mendelson, M.; Monnet, D.L.; Pulcini, C.; Kahlmeter, G.; Kluytmans, J.; Carmeli, Y.; et al. Discovery, research, and development of new antibiotics: The WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect. Dis. 2018, 18, 318–327. [Google Scholar] [CrossRef]
- Tacconelli, E.; Margin, N. Global Priority List of Antibiotic-Resistant Bacteria to Guide Research, Discovery, and Development of new Antibiotics. World Haelth Organization: Geneva, Switzerland. 2017. Available online: http://www.cdc.gov/drugresistance/threat-report-2013 (accessed on 27 July 2022).
- Rice, L.B. Federal Funding for the Study of Antimicrobial Resistance in Nosocomial Pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Stosovic, B.; Stepanovic, S.; Donabedian, S.; Tosic, T.J.M. Vancomycin- resistant Enterococcus faecalis in Serbia. Emerg. Infect. Dis. 2004, 10, 157–158. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe/European Centre for Disease Prevention and Control. Antimicrobial Resistance Surveillance in Europe 2022–2020 data. WHO Regional Office for Europe: Copenhagen, Denmark. 2022. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/ECDC-WHO-AMR-report.pdf (accessed on 27 July 2022).
- Zhou, X.; Willems, R.J.L.; Friedrich, A.W.; Rossen, J.W.A.; Bathoorn, E. Enterococcus faecium: From microbiological insights to practical recommendations for infection control and diagnostics. Antimicrob. Resist. Infect. Control 2020, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Recommendations for Preventing the Spread of Vancomycin Resistance Recommendations of the Hospital Infection Control Practices Advisory Committee (HICPAC). Available online: https://www.cdc.gov/MMwr/preview/mmwrhtml/00039349.htm (accessed on 27 July 2022).
- Boeing, C.; Correa-Martinez, C.L.; Schuler, F.; Mellmann, A.; Karch, A.; Kampmeiera, S. Development and validation of a tool for the prediction of vancomycin-resistant enterococci colonization persistence—The PREVENT score. Microbiol Spectr. 2021, 9, 1–7. [Google Scholar] [CrossRef]
- Higuita, N.I.A.; Huycke, M.M. Enterococcal Disease, Epidemiology, and Implications for Treatment. In Enterococci: From Commensals to Leading Causes of Drug Resistant Infection; Gilmore, M.S., Clewell, D.B., Ike, Y., Shankar, N., Eds.; Eye and Ear Infirmary: Boston, MA, USA, 2014. [Google Scholar]
- Ahmed, M.O.; Baptiste, K.E. Vancomycin-Resistant Enterococci: A Review of Antimicrobial Resistance Mechanisms and Perspectives of Human and Animal Health. Microb. Drug Resist. 2018, 24, 590–606. [Google Scholar] [CrossRef]
- Zirakzadeh, A.; Patel, R. Vancomycin-resistant enterococci: Colonization, infection, detection, and treatment. Mayo Clin. Proc. 2006, 81, 529–536. [Google Scholar] [CrossRef]
- Pan, S.; Wang, J.; Chen, Y.; Chang, Y.; Chen, M.; Chang, C. Incidence of and Risk Factors for Infection or Colonization of Vancomycin-Resistant Enterococci in Patients in the Intensive Care Unit Acute renal failure. PLoS ONE 2012, 7, e47297. [Google Scholar] [CrossRef]
- Shaghaghian, S.; Pourabbas, B.; Alborzi, A.; Askarian, M.; Mardaneh, J. Vancomycin-Resistant Entrococci colonization in chronic hemodialysis patients and its risk factors in southern. Iran. Red Crescent Med. J. 2012, 14, 686–691. [Google Scholar]
- Gudiol, C.; Ayats, J.; Camoez, M.; Domínguez, M.; García-Vidal, C.; Bodro, M.; Ardanuy, C.; Obed, M.; Arnan, M.; Antonio, M.; et al. Increase in Bloodstream Infection Due to Vancomycin- Susceptible Enterococcus faecium in Cancer Patients: Risk Factors, Molecular Epidemiology and Outcomes. PLoS ONE 2013, 8, e74734. [Google Scholar] [CrossRef]
- Ghanem, G.; Hachem, R.; Jiang, Y.; Chemaly, R.F.; Raad, I. Outcomes for and Risk Factors Associated With Vancomycin-Resistant Enterococcus faecalis and Vancomycin-Resistant Enterococcus faecium Bacteremia in Cancer Patients. Infect. Control Hosp. Epidemiol. 2007, 28, 1054–1059. [Google Scholar] [CrossRef] [PubMed]
- Mazuski, J.E. Vancomycin-resistant enterococcus: Risk factors, surveillance, infections, and treatment. Surg. Infect. 2008, 9, 567–571. [Google Scholar] [CrossRef] [PubMed]
- DeLisle, S.; Perl, T.M. Vancomycin-resistant enterococci: A road map on how to prevent the emergence and transmission of antimicrobial resistance. Chest 2003, 123, 504S–518S. [Google Scholar] [CrossRef]
- Faron, M.L.; Ledeboer, N.A.; Buchan, B.W. Resistance Mechanisms, Epidemiology, and Approaches to Screening. J. Clin. Microbiol. 2016, 54, 2436–2447. [Google Scholar] [CrossRef] [PubMed]
- The World Bank Group. Serbia. Available online: https://data.worldbank.org/country/serbia?view=chart (accessed on 27 July 2022).
- Janjusevic, A.; Markovic Denic, L.; Minic, R.; Grgurevic, A.; Cirkovic, I. Intestinal carriage of vancomycin-resistant Enterococcus spp. among high-risk patients in university hospitals in Serbia: First surveillance report. Ann. Clin. Microbiol. Antimicrob. 2021, 20, 18. [Google Scholar] [CrossRef]
- Karki, S.; Houston, L.; Land, G.; Bass, P.; Kehoe, R.; Borrell, S.; Watson, K.; Spelman, D.; Kennon, J.; Harrington, G.; et al. Prevalence and risk factors for VRE colonisation in a tertiary hospital in Melbourne, Australia: A cross sectional study. Antimicrob. Resist. Infect. Control 2012, 1, 1–6. [Google Scholar] [CrossRef]
- Djembi, L.F.; Hodille, E.; Chomat-Jaboulay, S.; Coudrais, S.; De Santis, N.; Gardes, S.; Mauranne, C.C.; Mourey, N.; Fredenucci, I.; Girard, R. Factors associated with Vancomycin-resistant Enterococcus acquisition during a large outbreak. J. Infect. Public Health 2017, 10, 185–190. [Google Scholar] [CrossRef]
- Toh, H.J.; Lim, Z.Y.; Yap, P.; Tang, T. Factors associated with prolonged length of stay in older patients. Singapore Med. J. 2017, 58, 134–138. [Google Scholar] [CrossRef]
- Ojeda Méndez, C.A.; Palomino Pacichana, D.S.; Bejarano Barragán, L.; Ocampo-Chaparro, J.M.; Reyes-Ortiz, C.A. Factores asociados con estancia hospitalaria prolongada en una unidad geriátrica de agudos. Acta Médica Colomb. 2020, 46, 7–13. [Google Scholar] [CrossRef]
- Poutanen, S.M.; Simor, A.E. Clostridium difficile-associated diarrhea in adults. CMAJ 2004, 171, 51–58. [Google Scholar] [CrossRef]
- Alevizakos, M.; Gaitanidis, A.; Nasioudis, D.; Tori, K.; Flokas, M.E.; Mylonakis, E. Colonization with vancomycin-resistant enterococci and risk for bloodstream infection among patients with malignancy: A systematic review and meta-analysis. Open Forum Infect. Dis. 2017, 4, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dahms, R.A.; Johnson, E.M.; Statz, C.L.; Lee, J.T.; Dunn, D.L.; Beilman, G.J. Third-generation cephalosporins and vancomycin as risk factors for postoperative vancomycin-resistant enterococcus infection. Arch. Surg. 1998, 133, 1343–1346. [Google Scholar] [CrossRef] [PubMed]
- Goossens, H.; Jabes, D.; Rossi, R.; Lammens, C.; Privitera, G.; Courvalin, P. European survey of vancomycin-resistant enterococci in at-risk hospital wards and in vitro susceptibility testing of ramoplanin against these isolates. J. Antimicrob. Chemother. 2003, 51, 5–12. [Google Scholar] [CrossRef]
- Warrick, K.; Althouse, S.K.; Rahrig, A.; Rupenthal, J.; Batra, S. Factors associated with a prolonged hospital stay during induction chemotherapy in newly diagnosed high risk pediatric acute lymphoblastic leukemia. Leuk. Res. 2018, 71, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Keng, M.K.; Sekeres, M.A. Febrile neutropenia in hematologic malignancies. Curr. Hematol. Malig. Rep. 2013, 8, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Heinz, W.J.; Buchheidt, D.; Christopeit, M.; von Lilienfeld-Toal, M.; Cornely, O.A.; Einsele, H.; Karthaus, M.; Link, H.; Mahlberg, R.; Neumann, S.; et al. Diagnosis and empirical treatment of fever of unknown origin (FUO) in adult neutropenic patients: Guidelines of the Infectious Diseases Working Party (AGIHO) of the German Society of Hematology and Medical Oncology (DGHO). Ann. Hematol. 2017, 96, 1775–1792. [Google Scholar] [CrossRef]
- Storms, A.D.; Chen, J.; Jackson, L.A.; Nordin, J.; Naleway, A.L.; Glanz, J.M.; Jacobsen, S.J.; Weintraub, E.S.; Klein, N.P.; Gargiullo, P.M.; et al. Rates and risk factors associated with hospitalization for pneumonia with ICU admission among adults. BMC Pulm. Med. 2017, 17, 1–9. [Google Scholar] [CrossRef]
- Ferreyro, B.L.; Scales, D.C.; Wunsch, H.; Cheung, M.C.; Gupta, V.; Saskin, R.; Thyagu, S.; Munshi, L. Critical illness in patients with hematologic malignancy: A population-based cohort study. Intensive Care Med. 2021, 47, 1104–1114. [Google Scholar] [CrossRef]
- Vijenthira, A.; Chiu, N.; Jacobson, D.; Freedman, Z.; Cheung, M.C.; Goddard, S.; Fowler, R.; Buckstein, R. Predictors of intensive care unit admission in patients with hematologic malignancy. Natureresearch 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Hawari, F.I.; Nazer, L.H.; Addassi, A.; Rimawi, D.; Jamal, K. Predictors of ICU Admission in Patients With Cancer and the Related Characteristics and Outcomes: A 5-Year Registry-Based Study. Crit. Care Med. 2016, 44, 548–553. [Google Scholar] [CrossRef]
- Tokars, J.I.; Gehr, T.; Jarvis, W.R.; Anderson, J.; Armistead, N.; Miller, E.R.; Parrish, J.; Qaiyumi, S.; Arduino, M.; Holt, S.C.; et al. Vancomycin-resistant enterococci colonization in patients at seven hemodialysis centers. Kidney Int. 2001, 60, 1511–1516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphreys, H. Controlling the spread of vancomycin-resistant enterococci. Is active screening worthwhile? J. Hosp. Infect. 2014, 88, 191–198. [Google Scholar] [CrossRef]
- Barbosa, D.; Lima, L.; Silbert, S.; Sader, H.; Cendoroglo, M.; Draibe, S.; Camargo, L.; Vianna, L.; Belasco, A.; Sesso, R. Evaluation of the prevalence and risk factors for colonization by vancomycin-resistant Enterococcus among patients on dialysis. Am. J. Kidney Dis. 2004, 44, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Zacharioudakis, I.M.; Zervou, F.N.; Ziakas, P.D.; Rice, L.B.; Mylonakis, E. Vancomycin-resistant enterococci colonization among dialysis patients: A meta-analysis of prevalence, risk factors, and significance. Am. J. Kidney Dis. 2015, 65, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Sakka, V.; Tsiodras, S.; Galani, L.; Antoniadou, A.; Souli, M.; Galani, I.; Pantelaki, M.; Siafakas, N.; Zerva, L.; Giamarellou, H. Risk-factors and predictors of mortality in patients colonised with vancomycin-resistant enterococci. Clin. Microbiol. Infect. 2008, 14, 14–21. [Google Scholar] [CrossRef]
- Metallidis, S.; Chatzidimitriou, M.; Tsona, A.; Bisiklis, A.; Lazaraki, G.; Koumentaki, E.; Gikas, A.; Alexiou-Daniel, S.; Nikolaidis, P. Vancomycin-Resistant Enterococci, Colonizing the Intestinal Tract of Patients in a University Hospital in Greece. Braz. J. Infect. Dis. 2006, 10, 179–184. [Google Scholar] [CrossRef]
- Amberpet, R.; Sistla, S.; Parija, S.C.; Thabah, M.M. Screening for Intestinal Colonization with Vancomycin Resistant Enterococci and Associated Risk Factors among Patients Admitted to an Adult Intensive Care Unit of a Large Teaching Hospital. J. Clin. Diagn. Res. 2016, 10, 6–9. [Google Scholar] [CrossRef]
- McEvoy, S.P.; Plant, A.J.; Pearman, J.W.; Christiansen, K.J. Risk factors for the acquisition of vancomycin-resistant enterococci during a single-strain outbreak at a major Australian teaching hospital. J. Hosp. Infect. 2006, 62, 256–258. [Google Scholar] [CrossRef]
- Ostrowsky, B.E.; Venkataraman, L.; D’Agata, E.M.C.; Gold, H.S.; DeGirolami, P.C.; Samore, M.H. Vancomycin-resistant enterococci in intensive care units: High frequency of stool carriage during a non-outbreak period. Arch. Intern. Med. 1999, 159, 1467–1472. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Liew, D.; Mårtensson, J.; Jones, D. The Frequency of, and Factors Associated with Prolonged Hospitalization: A Multicentre Study in Victoria, Australia. J. Clin. Med. 2020, 9, 3055. [Google Scholar] [CrossRef]
- Manoukian, S.; Stewart, S.; Dancer, S.; Graves, N.; Mason, H.; McFarland, A.; Robertson, C.; Reilly, J. Estimating excess length of stay due to healthcare-associated infections: A systematic review and meta-analysis of statistical methodology. J. Hosp. Infect. 2018, 100, 222–235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dancer, S.J. The problem with cephalosporins. J. Antimicrob. Chemother. 2001, 48, 463–478. [Google Scholar] [CrossRef] [PubMed]
- Quale, J.; Landmah, D.; Saurina, G.; Atwood, E.; DiTore, V.; Patel, K. Manipulation of a hospital antimicrobial formulary to control an outbreak of vancomycin-resistant enterococci. Clin. Infect. Dis. 1996, 23, 1020–1025. [Google Scholar] [CrossRef]
- Malmros, K.; Huttner, B.D.; McNulty, C.; Rodríguez-Baño, J.; Pulcini, C.; Tängdén, T. Comparison of antibiotic treatment guidelines for urinary tract infections in 15 European countries: Results of an online survey. Int. J. Antimicrob. Agents 2019, 54, 478–486. [Google Scholar] [CrossRef]
- Stupka, J.E.; Mortensen, E.M.; Anzueto, A.; Restrepo, M.I. Community-acquired pneumonia in elderly patients. Aging Health 2009, 5, 763–774. [Google Scholar] [CrossRef]
- Karki, S.; Land, G.; Aitchison, S.; Kennon, J.; Johnson, P.D.R.; Ballard, S.A.; Leder, K.; Cheng, A.C. Long-Term Carriage of Vancomycin-Resistant Enterococci in Patients Discharged from Hospitals: A 12-Year Retrospective. J. Clin. Microbiol. 2013, 51, 3374–3379. [Google Scholar] [CrossRef]
- Van Boeckel, T.P.; Gandra, S.; Ashok, A.; Caudron, Q.; Grenfell, B.T.; Levin, S.; Laxminarayan, R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect. Dis. 2014, 14, 742–750. [Google Scholar] [CrossRef]
- Goossens, H. Antibiotic consumption and link to resistance. Clin. Microbiol. Infect. 2009, 15, 12–15. [Google Scholar] [CrossRef]
- Loeffler, J.M.; Garbino, J.; Lew, D.; Harbarth, S.; Rohner, P. Antibiotic consumption, bacterial resistance and their correlation in a swiss university hospital and its adult intensive care units. Scand. J. Infect. Dis. 2003, 35, 843–850. [Google Scholar] [CrossRef]
- Radonjić, V. Promet i Potrošnja Gotovih Lekova za Humanu Upotrebu u Republici Srbiji u 2013. godini; Skener Studio “Lazić”; Agencija za lekove i medicinska sredstva Srbije: Beograd, Serbia, 2014; p. 388.
- Radonjić, V. Promet i Potrošnja Gotovih Lekova za Humanu Upotrebu u Republici Srbiji u 2006. godini; Agencija za lekove i medicinska sredstva Srbije; Helicon Publishing: Beograd, Serbia, 2007; p. 286. [Google Scholar]
- Vukajlović, I.; Bogdanović, M. Promet i Potrošnja Gotovih Lekova za Humanu Upotrebu u Republici Srbiji u 2018. godini; Agencija za lekove i medicinska sredstva Srbije-ALIMS, P. Print: Beograd, Serbia, 2019; p. 408.


{kind=link}
| Variables | VRE Status | p-Value * | |||
|---|---|---|---|---|---|
| Positive | Negative | ||||
| N (77) | % | N (191) | % | ||
| Gender | 0.471 | ||||
| Males | 39 | 50.6 | 106 | 55.5 | |
| Females | 38 | 49.4 | 85 | 44.5 | |
| Age group (years) | 0.057 | ||||
| <65 | 54 | 70.1 | 110 | 57.6 | |
| ≥65 | 23 | 29.9 | 81 | 42.4 | |
| Hospitals | 0.549 | ||||
| Zemun University Medical Centre | 27 | 35.1 | 74 | 38.7 | |
| Zvezdara University Medical Centre | 23 | 29.8 | 63 | 33.0 | |
| University Clinical Centre of Serbia | 27 | 35.1 | 54 | 28.3 | |
| Departments | 0.004 | ||||
| Geriatrics | 23 | 29.9 | 31 | 16.2 | |
| Intensive care units | 16 | 20.8 | 24 | 12.6 | |
| Hemato-oncology | 22 | 28.6 | 57 | 29.8 | |
| Infectious diseases | 10 | 12.9 | 34 | 17.8 | |
| Hemodialysis | 6 | 7.8 | 45 | 23.6 | |
| Comorbidities | |||||
| Diabetes mellitus | 14 | 18.2 | 63 | 32.9 | 0.978 |
| Hypertension | 44 | 57.1 | 33 | 42.9 | 0.387 |
| Ischemic heart disease | 14 | 18.2 | 28 | 14.7 | 0.473 |
| Heart failure | 6 | 7.8 | 12 | 6.3 | 0.655 |
| Cerebrovascular disease | 15 | 19.5 | 21 | 11.0 | 0.065 |
| Chronic pulmonary disease | 8 | 10.4 | 11 | 5.8 | 0.181 |
| Transfer from another institution | |||||
| Yes | 5 | 6.5 | 9 | 4.7 | 0.553 |
| Hospital length of stay before sampling | 0.008 | ||||
| ≤48 h | 3 | 3.9 | 37 | 19.4 | |
| 3–7 days | 23 | 29.9 | 52 | 27.2 | |
| 8–15 days | 23 | 29.9 | 37 | 19.4 | |
| ≥16 days | 28 | 36.4 | 65 | 34 | |
| Previous hospital admission | 0.544 | ||||
| No | 18 | 23.4 | 29 | 15.2 | |
| Yes, during the last 3 months | 38 | 49.4 | 98 | 51.3 | |
| Yes, during the previous 3–6 months | 2 | 2.6 | 9 | 4.7 | |
| Yes, during the previous 6–12 months | 3 | 3.9 | 9 | 4.7 | |
| Yes, more than a year ago | 16 | 20.8 | 46 | 24.1 | |
| Surgical intervention during the current admission | 0.023 | ||||
| Yes | 9 | 11.7 | 8 | 4.2 | |
| Surgical intervention in the period of 3 months prior to the current admission | 6 | 7.6 | 15 | 7.9 | 0.987 |
| Yes | |||||
| Antibiotics treatment during the current admission | <0.001 | ||||
| No | 26 | 33.8 | 115 | 60.2 | |
| Yes, one antimicrobial drug | 38 | 49.4 | 57 | 29.8 | |
| Yes, ≥2 antimicrobial drugs | 13 | 16.9 | 19 | 9.9 | |
| Groups of antimicrobial drugs used during the current admission | |||||
| Beta-lactams without cephalosporins | 9 | 11.7 | 28 | 14.7 | 0.523 |
| Cephalosporins | 27 | 35.1 | 30 | 15.7 | <0.001 |
| Fluoroquinolones | 19 | 24.7 | 25 | 13.1 | 0.021 |
| Aminoglycosides | 7 | 9.1 | 12 | 6.3 | 0.418 |
| Vancomycin | 10 | 13.0 | 17 | 8.9 | 0.315 |
| Macrolides and Lincosamides | 9 | 11.7 | 12 | 6.3 | 0.136 |
| Metronidazole | 18 | 23.4 | 28 | 14.7 | 0.087 |
| Other antimicrobial drugs | 5 | 6.5 | 12 | 6.3 | 0.949 |
| Antibiotic treatment in the period of 6 months prior to current admission | |||||
| Yes | 14 | 18.2 | 42 | 22.1 | 0.476 |
| Diagnostic–Therapeutic Procedures | |||||
| Oncology therapy | 22 | 28.6 | 57 | 29.8 | 0.836 |
| Corticosteroid therapy | 17 | 22.1 | 20 | 10.5 | 0.683 |
| Transfusion | 21 | 27.3 | 52 | 27.2 | 0.756 |
| Urinary catheter | 9 | 11.7 | 17 | 8.9 | 0.485 |
| Central venous catheter | 3 | 3.9 | 14 | 7.3 | 0.297 |
| Hematology procedures | 11 | 14.3 | 18 | 9.4 | 0.246 |
| Intensive care unit procedures without central venous catheter | 9 | 11.7 | 9 | 4.7 | 0.039 |
| Endoscopic procedures | 9 | 11.7 | 27 | 14.1 | 0.595 |
| Miscellaneous | |||||
| Proton-pump inhibitors treatment | 20 | 26.0 | 42 | 22.0 | 0.484 |
| Probiotics | 17 | 22.1 | 39 | 20.4 | 0.762 |
| Clostridioides difficile infection | 3 | 3.9 | 3 | 1.6 | 0.244 |
| Viral infection | 6 | 7.8 | 18 | 9.4 | 0.672 |
| Neutropenia | 11 | 14.3 | 22 | 11.5 | 0.533 |
| Hypoalbuminemia | 45 | 58.4 | 88 | 46.1 | 0.067 |
| Antifungal treatment | 2 | 2.6 | 3 | 1.6 | 0.574 |
| Variables | Univariate Logistic Regression | |
|---|---|---|
| RR (95% CI) | p value | |
| Gender | 0.471 | |
| Males | 0.8 (0.484–1.398) | |
| Females | 1.2 (0.715–2.065) | |
| Age group (years) | ||
| ≥65 | 1.7 (0.981–3.045) | 0.058 |
| Hospitals | ||
| Zemun University Medical Centre | 0.73 (0.385–1.382) | 0.353 |
| Zvezdara University Medical Centre | 0.73 (0.376–1.419) | 0.354 |
| University Clinical Centre of Serbia (ref) | / | |
| Departments | ||
| Geriatrics | 5.5 (2.030–15.251) | 0.001 |
| Hemato-oncology | 2.9 (1.082–7.741) | 0.034 |
| Infectious diseases | 2.2 (0.730–6.665) | 0.161 |
| Intensive care units | 5.0 (1.731–14.447) | 0.003 |
| Hemodialysis (ref) | / | |
| Comorbidities | ||
| Diabetes mellitus | 0.9 (0.499–1.966) | 0.978 |
| Hypertension | 1.2 (0.742–2.156) | 0.387 |
| Ischemic heart disease | 1.2 (0.640–2.616) | 0.474 |
| Heart failure | 1.2 (0.456–3.488) | 0.656 |
| Cerebrovascular disease | 1.9 (0.950–4.038) | 0.069 |
| Chronic pulmonary disease | 1.8 (0.732–4.916) | 0.187 |
| Transfer from another institution | ||
| Yes | 1.4 (0.455–4.333) | 0.555 |
| Hospital length of stay before sampling | ||
| ≤48 h (ref) | / | |
| 3–7 days | 5.4 (1.525–19.516) | 0.009 |
| 8–15 days | 7.6 (2.118–27.755) | 0.002 |
| ≥16 days | 5.3 (1.511–18.678) | 0.009 |
| Previous hospital admission | ||
| No (ref) | / | |
| Yes, during the last 3 m | 0.6 (0.311–1.255) | 0.186 |
| Yes, during the previous 3–6 m | 0.3 (0.069–1.848) | 0.22 |
| Yes, during the previous 6–12 m | 0.5 (0.128–2.251) | 0.395 |
| Yes, more than a year ago | 0.5 (0.247–1.270) | 0.165 |
| Surgical intervention during the current admission | ||
| Yes | 3.0 (1.122–8.166) | 0.029 |
| Surgical intervention in the period of 3 months prior to the current admission | ||
| Yes | 0.9 (0.370–2.658) | 0.987 |
| Antibiotics treatment during the current admission | ||
| No (ref) | / | |
| 1 | 2.9 (1.632–5.326) | 0.001 |
| ≥2 | 3.0 (1.328–6.898) | 0.008 |
| Groups of antimicrobial drugs used during the current admission | ||
| Beta-lactams without cephalosporins | 0.7 (0.345–1.719) | 0.524 |
| Cephalosporins | 2.8 (1.576–5.329) | 0.001 |
| Fluoroquinolones | 2.1 (1.116–4.239) | 0.022 |
| Aminoglycosides | 1.4 (0.564–3.944) | 0.420 |
| Vancomycin | 1.5 (0.666–3.505) | 0.317 |
| Macrolides and Lincosamides | 1.9 (0.796–4.896) | 0.142 |
| Metronidazole | 1.7 (0.915–3.446) | 0.089 |
| Other antimicrobial drugs | 1.0 (0.352–3.046) | 0.949 |
| Antibiotic treatment in the period of 6 months prior to the current admission | ||
| Yes | 0.7 (0.400–1.535) | 0.476 |
| Diagnostic–therapeutic procedures | ||
| Oncology therapy | 0.9 (0.525–1.685) | 0.836 |
| Corticosteroid therapy | 0.9 (0.534–1.711) | 0.683 0.756 |
| Transfusion | 0.9 (0.551–1.807) | |
| Urinary catheter | 0.7 (0.314–1.736) | 0.487 |
| Central venous catheter | 1.9 (0.545–6.990) | 0.305 |
| Hematology procedures | 1.6 (0.718–3.572) | 0.249 |
| Intensive care unit procedures without a central venous catheter | 2.6 (1.020–7.025) | 0.046 |
| Endoscopic procedures | 0.8 (1.359–1.799) | 1.595 |
| Miscellaneous | ||
| Proton-pump inhibitors treatment | 1.2 (1.674–2.200) | 1.484 |
| Probiotics | 1.1 (1.580–2.101) | 1.762 |
| Clostridioides difficile infection | 2.5 (1.501–12.873) | 1.260 |
| Viral infection | 0.8 (1.310–2.130) | 1.672 |
| Neutropenia | 1.2 (1.588–2.786) | 1.533 |
| Hypoalbuminemia | 1.6 (1.964–2.811) | 1.068 |
| Antifungal treatment | 1.6 (1.274–11.202) | 1.578 |
| Variables | Model 1 | Model 2 | ||
|---|---|---|---|---|
| RR (95% CI) | p value | RR (95% CI) | p value | |
| Age group (years) | ||||
| ≥65 | 2.3 (1.039–4.930) | 0.040 | ||
| Hospitals | ||||
| Zemun University Medical Centre | 0.26 (0.096–0.706) | 0.008 | ||
| Zvezdara University Medical Centre | 0.25 (0.094–0.685) | 0.007 | ||
| University Clinical Centre of Serbia (ref) | / | |||
| Departments | ||||
| Geriatrics | 6.5 (2.185–19.747) | 0.001 | 7.6 (2.272–25.523) | 0.001 |
| Hemato-oncology | 4.7 (1.599–14.204) | 0.005 | 5.5 (1.697–18.042) | 0.005 |
| Infectious diseases | 2.0 (0.580–7.308) | 0.264 | 1.03 (0.244–4.318) | 0.972 |
| Intensive care units | 5.0 (1.523–16.491) | 0.008 | 5.4(1.538–18.853) | 0.008 |
| Hemodialysis (ref) | / | |||
| Hospital length of stay before sampling | ||||
| ≤48 h (ref) | / | / | ||
| 3–7 days | 5.5 (1.519–20.388) | 0.010 | 5.0 (1.322–18.983) | 0.018 |
| 8–15 days | 5.4 (1.450–20.655) | 0.012 | 4.7 (1.215–18.128) | 0.025 |
| ≥16 days | 8.4 (2.236–31.529) | 0.002 | 6.6 (1.687–26.118) | 0.007 |
| Cephalosporins | 2.2 (1.093–4.351) | 0.027 | 2.2 (1.114–4.594) | 0.024 |
| Fluoroquinolones | 1.8 (0.865–4.066) | 0.111 | 1.9 (0.846–4.315) | 0.119 |
| Nagelkerke R2 | 0.206 | 0.253 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janjusevic, A.; Cirkovic, I.; Minic, R.; Stevanovic, G.; Soldatovic, I.; Mihaljevic, B.; Vidovic, A.; Markovic Denic, L. Predictors of Vancomycin-Resistant Enterococcus spp. Intestinal Carriage among High-Risk Patients in University Hospitals in Serbia. Antibiotics 2022, 11, 1228. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11091228
Janjusevic A, Cirkovic I, Minic R, Stevanovic G, Soldatovic I, Mihaljevic B, Vidovic A, Markovic Denic L. Predictors of Vancomycin-Resistant Enterococcus spp. Intestinal Carriage among High-Risk Patients in University Hospitals in Serbia. Antibiotics. 2022; 11(9):1228. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11091228
Chicago/Turabian StyleJanjusevic, Ana, Ivana Cirkovic, Rajna Minic, Goran Stevanovic, Ivan Soldatovic, Biljana Mihaljevic, Ana Vidovic, and Ljiljana Markovic Denic. 2022. "Predictors of Vancomycin-Resistant Enterococcus spp. Intestinal Carriage among High-Risk Patients in University Hospitals in Serbia" Antibiotics 11, no. 9: 1228. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics11091228