

The Clinical Outcome of Early Periprosthetic Joint Infections Caused by Staphylococcus epidermidis and Managed by Surgical Debridement in an Era of Increasing Resistance
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design
2.2. Studied Population
2.3. Data Collection
2.4. Statistical Analysis
3. Results
3.1. Studied Population
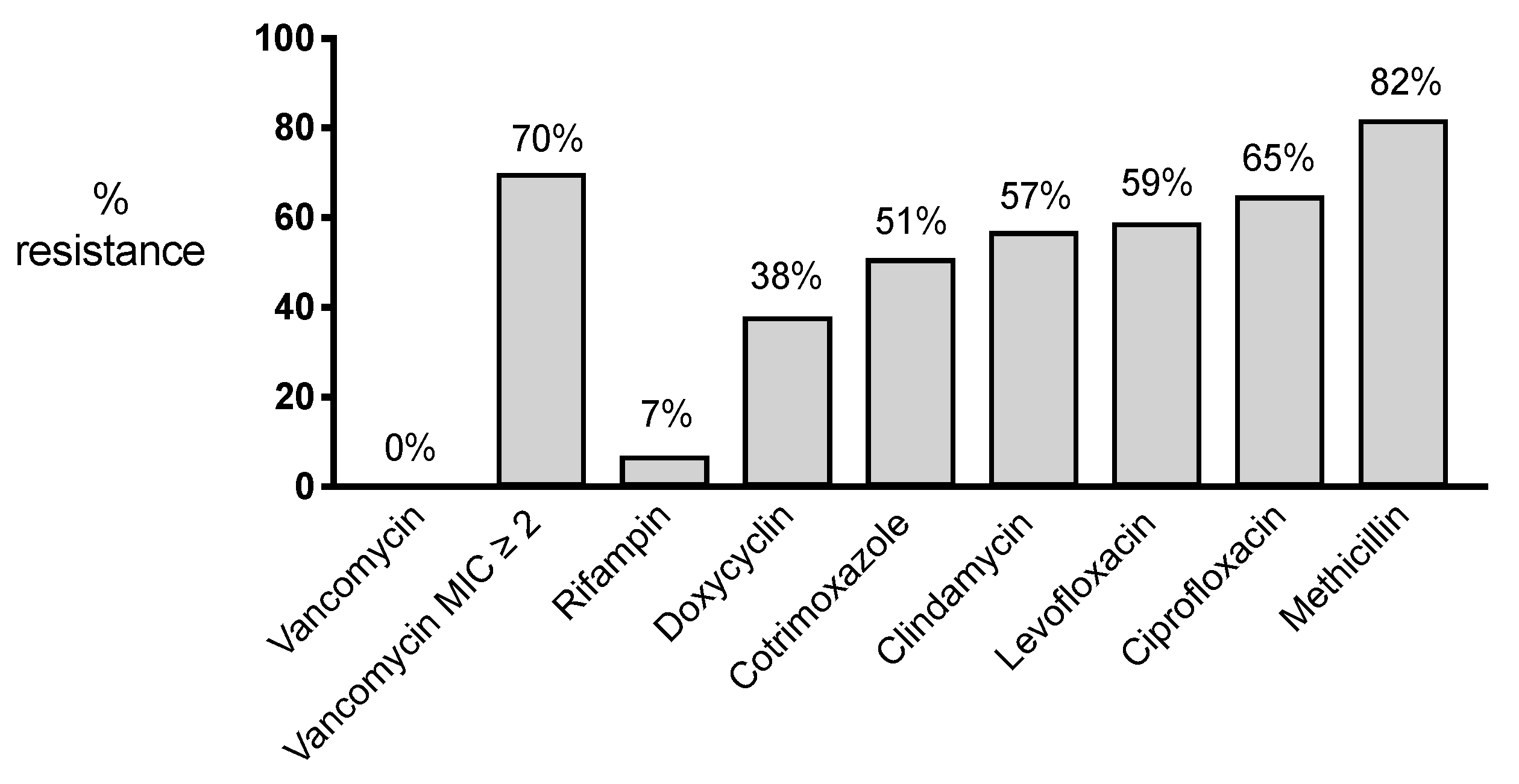
3.2. Resistance Profiles
3.3. Clinical Outcomes According to Resistance Profiles and Oral Antimicrobial Regimen
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferguson, R.J.; Palmer, A., Jr.; Taylor, A.; Porter, M.L.; Malchau, H.; Glyn-Jones, S. Hip replacement. Lancet 2018, 392, 1662–1671. [Google Scholar] [CrossRef] [PubMed]
- Price, A.J.; Alvand, A.; Troelsen, A.; Katz, J.N.; Hooper, G.; Gray, A.; Carr, A.; Beard, D. Knee replacement. Lancet 2018, 392, 1672–1682. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.; Whitehouse, M.; Blom, A.W.; Beswick, A.; Team, I. Patient-related risk factors for periprosthetic joint infection after total joint arthroplasty: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0150866. [Google Scholar] [CrossRef] [PubMed]
- Wildeman, P.; Rolfson, O.; Söderquist, B.; Wretenberg, P.; Lindgren, V. What are the long-term outcomes of mortality, quality of life, and hip function after prosthetic joint infection of the hip? A 10-year follow-up from Sweden. Clin. Orthop. Relat. Res. 2021, 479, 2203–2213. [Google Scholar] [CrossRef]
- Löwik, C.A.; Jutte, P.C.; Tornero, E.; Ploegmakers, J.J.; Knobben, B.A.; de Vries, A.J.; Zijlstra, W.P.; Dijkstra, B.; Soriano, A.; Wouthuyzen-Bakker, M. Predicting failure in early acute prosthetic joint infection treated with debridement, antibiotics and implant retention: External validation of the KLIC-score. J. Arthroplast. 2018, 33, 2582–2587. [Google Scholar] [CrossRef] [PubMed]
- Soriano, A.; García, S.; Bori, G.; Almela, M.; Gallart, X.; Macule, F.; Sierra, J.; Martínez, J.; Suso, S.; Mensa, J. Treatment of acute post-surgical infection of joint arthroplasty. Clin. Microbiol. Infect. 2006, 12, 930–933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodríguez-Pardo, D.; Pigrau, C.; Lora-Tamayo, J.; Soriano, A.; del Toro, M.; Cobo, J.; Palomino, J.; Euba, G.; Riera, M.; Sánchez-Somolinos, M.; et al. Gram-negative prosthetic joint infection: Outcome of a debridement, antibiotics and implant retention approach. A large multicentre study. Clin. Microbiol. Infect. 2014, 20, O911–O919. [Google Scholar] [CrossRef] [Green Version]
- Silva da, R.B.; Salles, M.J. Outcome and risk factors in prosthetic joint infections by multidrug-resistant Gram-negative bacteria: A retrospective cohort study. Antibiotics 2021, 10, 340. [Google Scholar] [CrossRef]
- Papadopoulos, A.; Ribera, A.; Mavrogenis, A.F.; Rodriguez-Pardo, D.; Bonnet, E.; Salles, M.J.; del Toro, M.D.; Nguyen, S.; Blanco-García, A.; Skaliczki, G.; et al. Multidrug-resistant and extensively drug-resistant Gram-negative prosthetic joint infections: Role of surgery and impact of colistin administration. Int. J. Antimicrob. Agents 2019, 53, 294–301. [Google Scholar] [CrossRef]
- Siljander, M.P.; Sobh, A.H.; Baker, K.C.; Baker, E.A.; Kaplan, L.M. Multidrug-resistant organisms in the setting of periprosthetic joint infection- diagnosis, prevention, and treatment. J. Arthroplast. 2018, 33, 185–194. [Google Scholar] [CrossRef]
- Tai, D.B.G.; Patel, R.; Abdel, M.P.; Berbari, E.F.; Tande, A.J. Microbiology of hip and knee periprosthetic joint infections: A database study. Clin. Microbiol. Infect. 2021, 28, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Benito, N.; Mur, I.; Ribera, A.; Soriano, A.; Rodríguez-Pardo, D.; Sorlí, L.; Cobo, J.; Fernández-Sampedro, M.; del Toro, M.D.; Guío, L.; et al. The Different Microbial Etiology of Prosthetic Joint Infections according to Route of Acquisition and Time after Prosthesis Implantation, Including the Role of Multidrug-Resistant Organisms. J. Clin. Med. 2019, 8, 673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.Y.H.; Monk, I.R.; Gonçalves da Silva, A.; Seemann, T.; Chua, K.Y.L.; Kearns, A.; Hill, R.; Woodford, N.; Bartels, M.D.; Strommenger, B.; et al. Global spread of three multidrug-resistant lineages of Staphylococcus epidermidis. Nat. Microbiol. 2018, 3, 1175–1185. [Google Scholar] [CrossRef] [PubMed]
- Beldman, M.; Löwik, C.; Soriano, A.; Albiach, L.; Zijlstra, W.P.; Knobben, B.A.S.; Jutte, P.; Sousa, R.; Carvalho, A.; Goswami, K.; et al. If, When, and How to Use Rifampin in Acute Staphylococcal Periprosthetic Joint Infections, a Multicentre Observational Study. Clin Infect Dis. 2021, 73, 1634–1641. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Lourtet-Hascoët, J.; Bicart-See, A.; Félicé, M.; Giordano, G.; Bonnet, E. Staphylococcus lugdunensis, a serious pathogen in periprosthetic joint infections: Comparison to Staphylococcus aureus and Staphylococcus epidermidis. Int. J. Infect. Dis. 2016, 51, 56–61. [Google Scholar] [CrossRef] [Green Version]
- Zeller, V.; Kerroumi, Y.; Meyssonnier, V.; Heym, B.; Metten, M.-A.; Desplaces, N.; Marmor, S. Analysis of postoperative and hematogenous prosthetic joint-infection microbiological patterns in a large cohort. J. Infect. 2018, 76, 328–334. [Google Scholar] [CrossRef]
- Löwik, C.A.M.; Parvizi, J.; Jutte, P.C.; Zijlstra, W.P.; Knobben, B.A.S.; Xu, C.; Goswami, K.; A Belden, K.; Sousa, R.; Carvalho, A.; et al. Debridement, antibiotics and implant retention is a viable treatment option for early periprosthetic joint infection presenting more than 4 weeks after index arthroplasty. Clin. Infect. Dis. 2020, 71, 630–636. [Google Scholar] [CrossRef]
- Hischebeth, G.T.; Randau, T.M.; Ploeger, M.M.; Friedrich, M.J.; Kaup, E.; Jacobs, C.; Molitor, E.; Hoerauf, A.; Gravius, S.; Wimmer, M.D. Staphylococcus epidermidis in periprosthetic joint infection—Outcome analysis of methicillin-resistant versus methicillin-susceptible strains. Diagn. Microbiol. Infect. Dis. 2019, 93, 125–130. [Google Scholar] [CrossRef]
- Lora-Tamayo, J.; Murillo, O.; Iribarren, J.A.; Soriano, A.; Sánchez-Somolinos, M.; Baraia-Etxaburu, J.M.; Rico, A.; Palomino, J.; Rodríguez-Pardo, D.; Horcajada, J.P.; et al. A large multicenter study of methicillin-susceptible and methicillin-resistant Staphylococcus aureus prosthetic joint infections managed with implant retention. Clin. Infect. Dis. 2013, 56, 182–194. [Google Scholar] [CrossRef]
- Zimmerli, W.; Widmer, A.F.; Blatter, M.; Frei, R.; Ochsner, P.E.; for the Foreign-Body Infection (FBI) Study Group. Role of rifampin for treatment of orthopedic implant-related staphylococcal infections: A randomized controlled trial. J. Am. Med. Assoc. 1998, 279, 1537–1541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishaq, H.; Tariq, W.; Talha, K.M.; Palraj, B.R.V.; Sohail, M.R.; Baddour, L.M.; Mahmood, M. Association between high vancomycin minimum inhibitory concentration and clinical outcomes in patients with methicillin-resistant Staphylococcus aureus bacteremia: A meta-analysis. Infection 2021, 49, 803–811. [Google Scholar] [CrossRef] [PubMed]
- Soriano, A.; Marco, F.; Martínez, J.A.; Pisos, E.; Almela, M.; Dimova, V.P.; Alamo, D.; Ortega, M.; Lopez, J.; Mensa, J. Influence of vancomycin minimum inhibitory concentration on the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Clin. Infect. Dis. 2008, 46, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Maor, Y.; Hagin, M.; Belausov, N.; Keller, N.; Ben-David, D.; Rahav, G. Clinical features of heteroresistant vancomycin-intermediate Staphylococcus aureus bacteremia versus those of methicillin-resistant S. aureus bacteremia. J. Infect. Dis. 2009, 199, 619–624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, H.-J.; Chen, C.-C.; Cheng, K.-C.; Wu, K.-Y.; Lin, Y.-C.; Zhang, C.-C.; Weng, T.-C.; Yu, W.-L.; Chiu, Y.-H.; Toh, H.-S.; et al. In Vitro efficacies and resistance profiles of rifampin-based combination regimens for biofilm-embedded methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 2013, 57, 5717–5720. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Univariate Binary Regression Analysis | Multivariate Binary Regression Analysis | ||||
|---|---|---|---|---|---|
| Variable | Non-Failures (n = 93) | Failures (n = 64) | p Value | Adjusted OR (95% CI) | p Value |
| Baseline characteristics Male sex | 37.6% | 45.3% | 0.34 | ||
| Age > 70 | 66.7% | 82.8% | 0.03 * | 0.97 (0.24–2.05) | 0.97 |
| BMI > 30 | 59.1% | 70.3% | 0.15 * | 0.71 (0.25–3.90) | 0.53 |
| ASA (≥3) | 44.1% | 54.7% | 0.19 * | 1.03 (0.35–3.05) | 0.96 |
| Comorbidities Arterial hypertension | 67.7% | 67.2% | 0.94 | ||
| Heart failure | 9.7% | 9.4% | 0.95 | ||
| Coronary heart disease | 15.1% | 20.3% | 0.39 | ||
| Diabetes mellitus | 20.4% | 23.4% | 0.65 | ||
| Chronic renal failure | 7.5% | 17.2% | 0.06 * | 1.48 (0.31–7.22) | 0.63 |
| COPD | 19.4% | 14.1% | 0.39 | ||
| Liver cirrhosis | 2.2% | 1.6% | 0.79 | ||
| Rheumatoid arthritis | 7.5% | 4.7% | 0.47 | ||
| Characteristics implant Hip | 72.0% | 70.3% | 0.81 | ||
| Fracture Cemented | 10.8% 74.2% | 18.8% 82.8% | 0.16 * 0.20 * | 2.20 (0.59–8.23) 3.23 (0.49–21.39) | 0.24 0.23 |
| Microorganism Polymicrobial | 61.2% | 62.7% | 0.85 | ||
| Resistance profile Methicillin resistance Fluoroquinolone resistance Cotrimoxazole resistance Clindamycin resistance Doxycycline resistance Rifampin resistance Vancomycin MIC ≥ 2 | 76.3% 49.2% 42.1% 49.2% 39.0% 3.4% 64.4% | 93.3% 83.9% 66.7% 73.3% 37.5% 12.9% 70.8% | 0.05 ** 0.001 * 0.03 ** 0.03 ** 0.90 0.09 * 0.59 | 5.45 (1.67–17.83) 5.69 (0.61–52.75) | 0.005 0.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shabana, N.S.; Seeber, G.; Soriano, A.; Jutte, P.C.; Westermann, S.; Mithoe, G.; Pirii, L.; Siebers, T.; Have, B.t.; Zijlstra, W.; et al. The Clinical Outcome of Early Periprosthetic Joint Infections Caused by Staphylococcus epidermidis and Managed by Surgical Debridement in an Era of Increasing Resistance. Antibiotics 2023, 12, 40. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12010040
Shabana NS, Seeber G, Soriano A, Jutte PC, Westermann S, Mithoe G, Pirii L, Siebers T, Have Bt, Zijlstra W, et al. The Clinical Outcome of Early Periprosthetic Joint Infections Caused by Staphylococcus epidermidis and Managed by Surgical Debridement in an Era of Increasing Resistance. Antibiotics. 2023; 12(1):40. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12010040
Chicago/Turabian StyleShabana, Nada S., Gesine Seeber, Alex Soriano, Paul C. Jutte, Silvia Westermann, Glenn Mithoe, Loredana Pirii, Théke Siebers, Bas ten Have, Wierd Zijlstra, and et al. 2023. "The Clinical Outcome of Early Periprosthetic Joint Infections Caused by Staphylococcus epidermidis and Managed by Surgical Debridement in an Era of Increasing Resistance" Antibiotics 12, no. 1: 40. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12010040