

Design Characteristics and Recruitment Rates for Randomized Trials of Peri-Prosthetic Joint Infection Management: A Systematic Review

Abstract
:1. Introduction
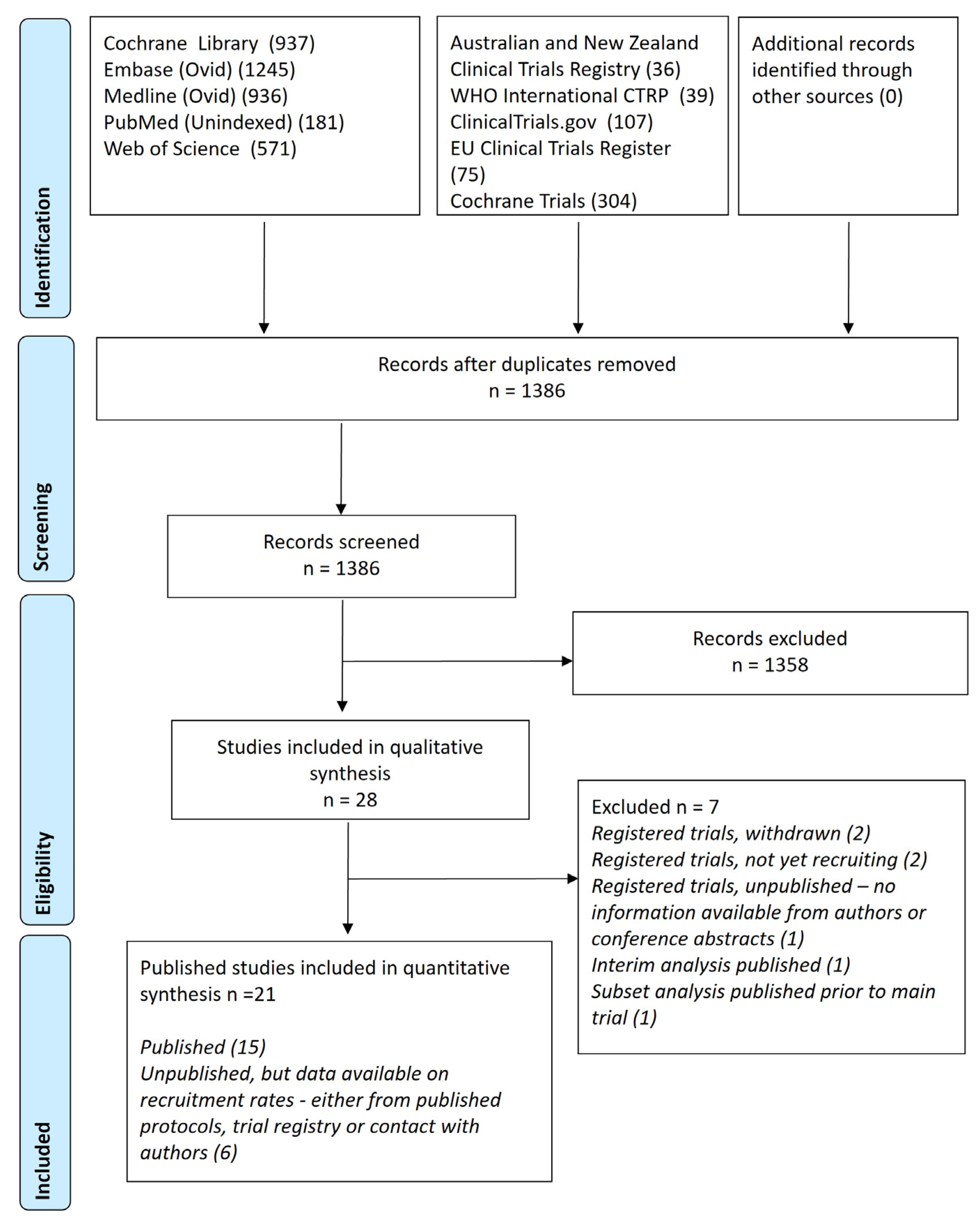
2. Results
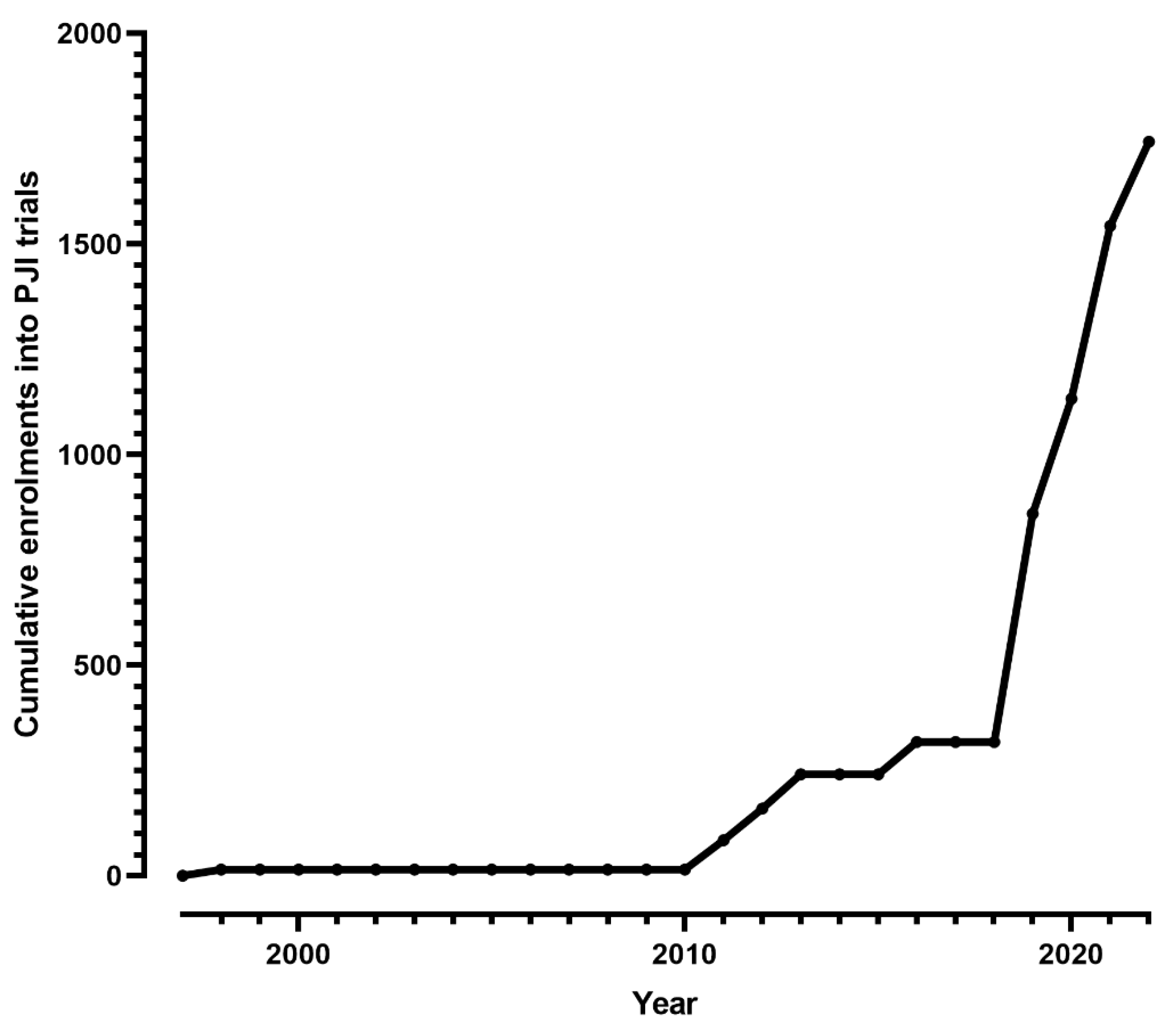
2.1. Recruitment Rates
2.2. Clinical Endpoints
2.3. Blinding Outcome Assessment and Randomization
2.4. Sample Size Calculations
3. Discussion
4. Materials and Methods
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ong, K.L.; Kurtz, S.M.; Lau, E.; Bozic, K.J.; Berry, D.J.; Parvizi, J. Prosthetic Joint Infection Risk After Total Hip Arthroplasty in the Medicare Population. J. Arthroplast. 2009, 24, 105–109. (In English) [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Ong, K.L.; Lau, E.; Bozic, K.J.; Berry, D.; Parvizi, J. Prosthetic Joint Infection Risk after TKA in the Medicare Population. Clin. Orthop. Relat. Res. 2010, 468, 52–56. (In English) [Google Scholar] [CrossRef] [PubMed]
- Manning, L.; Davis, J.S.; Robinson, O.; Clark, B.; Lorimer, M.; de Steiger, R.; Graves, S.E. High prevalence of older Australians with one or more joint replacements: Estimating the population at risk for late complications of arthroplasty. ANZ J. Surg. 2020, 90, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Manning, L.; Metcalf, S.; Clark, B.; Robinson, J.O.; Huggan, P.; Luey, C.; McBride, S.; Aboltins, C.; Nelson, R.; Campbell, D.; et al. Clinical Characteristics, Etiology, and Initial Management Strategy of Newly Diagnosed Periprosthetic Joint Infection: A Multicenter, Prospective Observational Cohort Study of 783 Patients. Open Forum Infect. Dis. 2020, 7, ofaa068. [Google Scholar] [CrossRef] [PubMed]
- Peel, T.; Dowsey, M.; Buising, K.; Liew, D.; Choong, P. Cost analysis of debridement and retention for management of prosthetic joint infection. Clin. Microbiol. Infect. 2013, 19, 181–186. [Google Scholar] [CrossRef]
- Del Pozo, J.L.; Patel, R. Infection Associated with Prosthetic Joints. N. Engl. J. Med. 2009, 361, 787–794. [Google Scholar] [CrossRef]
- Roberts, R.R.; Hota, B.; Ahmad, I.; Scott, R.D., II; Foster, S.D.; Abbasi, F.; Schabowski, S.; Kampe, L.M.; Ciavarella, G.G.; Supino, M.; et al. Hospital and Societal Costs of Antimicrobial-Resistant Infections in a Chicago Teaching Hospital: Implications for Antibiotic Stewardship. Clin. Infect. Dis. 2009, 49, 1175–1184. [Google Scholar] [CrossRef]
- Davis, J.S.; Metcalf, S.; Clark, B.; Robinson, J.O.; Huggan, P.; Luey, C.; McBride, S.; Aboltins, C.; Nelson, R.; Campbell, D.; et al. Predictors of Treatment Success After Periprosthetic Joint Infection: 24-Month Follow up From a Multicenter Prospective Observational Cohort Study of 653 Patients. Open Forum Infect. Dis. 2022, 9, ofac048. [Google Scholar] [CrossRef]
- Paterson, D.L. Determining research priorities for clinician-initiated trials in infectious diseases. Med. J. Aust. 2013, 198, 270–272. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Infectious Diseases Society of America. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef]
- Argenson, J.N.; Arndt, M.; Babis, G.; Battenberg, A.; Budhiparama, N.; Catani, F.; Chen, F.; de Beaubien, B.; Ebied, A.; Esposito, S.; et al. Hip and Knee Section, Treatment, Debridement and Retention of Implant: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2018, 34, S399–S419. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, T.; Parvizi, J. Proceedings of the International Consensus Meeting on Periprosthetic Joint Infection. J. Arthroplast. 2014, 29, 4. [Google Scholar] [CrossRef]
- Expert Group for Antibiotics. Bone and joint infections. In Therapeutic Guidelines: Antibiotics; Therapeutic Guidelines Limited: Melbourne, Australia, 2010; Volume 14. [Google Scholar]
- Zimmerli, W.; Widmer, A.F.; Blatter, M.; Frei, R.; Ochsner, P.E. Role of Rifampin for Treatment of Orthopedic Implant–Related Staphylococcal Infections A Randomized Controlled Trial. JAMA 1998, 279, 1537–1541. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, E.; Borgen, P.; Bragnes, B.; Figved, W.; Grøgaard, B.; Rydinge, J.; Sandberg, L.; Snorrason, F.; Wangen, H.; Witsøe, E.; et al. Rifampin combination therapy in staphylococcal prosthetic joint infections: A randomized controlled trial. J. Orthop. Surg. Res. 2020, 15, 1–9. [Google Scholar] [CrossRef]
- Aydın, O.; Ergen, P.; Ozturan, B.; Ozkan, K.; Arslan, F.; Vahaboglu, H. Rifampin-accompanied antibiotic regimens in the treatment of prosthetic joint infections: A frequentist and Bayesian meta-analysis of current evidence. Eur. J. Clin. Microbiol. Infect. Dis. 2020, 40, 665–671. [Google Scholar] [CrossRef]
- Scheper, H.; Gerritsen, L.M.; Pijls, B.G.; A Van Asten, S.; Visser, L.G.; De Boer, M.G.J. Outcome of Debridement, Antibiotics, and Implant Retention for Staphylococcal Hip and Knee Prosthetic Joint Infections, Focused on Rifampicin Use: A Systematic Review and Meta-Analysis. Open Forum Infect. Dis. 2021, 8, ofab298. [Google Scholar] [CrossRef]
- Fillingham, Y.A.; Della Valle, C.J.; Suleiman, L.I.; Springer, B.D.; Gehrke, T.; Bini, S.A.; Segreti, J.; Chen, A.F.; Goswami, K.; Tan, T.L.; et al. Definition of Successful Infection Management and Guidelines for Reporting of Outcomes After Surgical Treatment of Periprosthetic Joint Infection. J. Bone Jt. Surg. 2019, 101, e69. [Google Scholar] [CrossRef]
- Johns, B.P.; Dewar, D.C.; Loewenthal, M.R.; Manning, L.A.; Atrey, A.; Atri, N.; Campbell, D.G.; Dunbar, M.; Kandel, C.; Khoshbin, A.; et al. A desirability of outcome ranking (DOOR) for periprosthetic joint infection—A Delphi analysis. J. Bone Jt. Infect. 2022, 7, 221–229. [Google Scholar] [CrossRef]
- Frank, J.M.; Kayupov, E.; Moric, M.; Segreti, J.; Hansen, E.; Hartman, C.; Okroj, K.; Belden, K.; Roslund, B.; Silibovsky, R.; et al. The Mark Coventry, MD, Award: Oral Antibiotics Reduce Reinfection After Two-Stage Exchange: A Multicenter, Randomized Controlled Trial. Clin. Orthop. Relat. Res. 2017, 475, 56–61. [Google Scholar] [CrossRef]
- Yang, J.; Parvizi, J.; Hansen, E.N.; Culvern, C.N.; Segreti, J.C.; Tan, T.; Hartman, C.W.; Sporer, S.M.; Della Valle, C.J.; The Knee Society Research Group. 2020 Mark Coventry Award: Microorganism-directed oral antibiotics reduce the rate of failure due to further infection after two-stage revision hip or knee arthroplasty for chronic infection: A multicentre randomized controlled trial at a minimum of two years. Bone Jt. J. 2020, 102–B, 3–9. [Google Scholar] [CrossRef]
- Valenzuela, M.M.; Odum, S.M.; Griffin, W.L.; Springer, B.D.; Fehring, T.K.; Otero, J.E. High-Dose Antibiotic Cement Spacers Independently Increase the Risk of Acute Kidney Injury in Revision for Periprosthetic Joint Infection: A Prospective Randomized Controlled Clinical Trial. J. Arthroplast. 2022, 37, S321–S326. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Mahamud, E.; García, S.; Bori, G.; Martínez-Pastor, J.C.; Zumbado, J.A.; Riba, J.; Mensa, J.; Soriano, A. Comparison of a low-pressure and a high-pressure pulsatile lavage during débridement for orthopaedic implant infection. Arch. Orthop. Trauma Surg. 2011, 131, 1233–1238. [Google Scholar] [CrossRef] [PubMed]
- Byren, I.; Rege, S.; Campanaro, E.; Yankelev, S.; Anastasiou, D.; Kuropatkin, G.; Evans, R. Randomized Controlled Trial of the Safety and Efficacy of Daptomycin versus Standard-of-Care Therapy for Management of Patients with Osteomyelitis Associated with Prosthetic Devices Undergoing Two-Stage Revision Arthroplasty. Antimicrob. Agents Chemother. 2012, 56, 5626–5632. [Google Scholar] [CrossRef] [PubMed]
- Bruni, D.; Iacono, F.; Sharma, B.; Zaffagnini, S.; Marcacci, M. Tibial Tubercle Osteotomy or Quadriceps Snip in Two-stage Revision for Prosthetic Knee Infection? A Randomized Prospective Study. Clin. Orthop. Relat. Res. 2013, 471, 1305–1318. [Google Scholar] [CrossRef] [PubMed]
- Pushkin, R.; Iglesias-Ussel, M.D.; Keedy, K.; MacLauchlin, C.; Mould, D.R.; Berkowitz, R.; Kreuzer, S.; Darouiche, R.; Oldach, D.; Fernandes, P. A Randomized Study Evaluating Oral Fusidic Acid (CEM-102) in Combination With Oral Rifampin Compared With Standard-of-Care Antibiotics for Treatment of Prosthetic Joint Infections: A Newly Identified Drug–Drug Interaction. Clin. Infect. Dis. 2016, 63, 1599–1604. [Google Scholar] [CrossRef]
- Lora-Tamayo, J.; Euba, G.; Cobo, J.; Horcajada, J.P.; Soriano, A.; Sandoval, E.; Pigrau, C.; Benito, N.; Falgueras, L.; Palomino, J.; et al. Short- versus long-duration levofloxacin plus rifampicin for acute staphylococcal prosthetic joint infection managed with implant retention: A randomised clinical trial. Int. J. Antimicrob. Agents 2016, 48, 310–316. [Google Scholar] [CrossRef]
- Benkabouche, M.; Racloz, G.; Spechbach, H.; A Lipsky, B.; Gaspoz, J.-M.; Uçkay, I. Four versus six weeks of antibiotic therapy for osteoarticular infections after implant removal: A randomized trial. J. Antimicrob. Chemother. 2019, 74, 2394–2399. [Google Scholar] [CrossRef]
- Li, H.-K.; Rombach, I.; Zambellas, R.; Walker, A.S.; McNally, M.A.; Atkins, B.L.; Lipsky, B.A.; Hughes, H.C.; Bose, D.; Kümin, M.; et al. Oral versus Intravenous Antibiotics for Bone and Joint Infection. N. Engl. J. Med. 2019, 380, 425–436. [Google Scholar] [CrossRef]
- Xu, C.; Jia, C.-Q.; Kuo, F.-C.; Chai, W.; Zhang, M.-H.; Chen, J.-Y. Does the use of a closed-suction drain reduce the effectiveness of an antibiotic-loaded spacer in two-stage exchange Arthroplasty for Periprosthetic hip infection? A prospective, randomized, controlled study. BMC Musculoskelet. Disord. 2019, 20, 583. [Google Scholar] [CrossRef]
- Nahhas, C.R.; Chalmers, P.N.; Parvizi, J.; Sporer, S.M.; Berend, K.R.; Moric, M.; Chen, A.F.; Austin, M.S.; Deirmengian, G.K.; Morris, M.J.; et al. A Randomized Trial of Static and Articulating Spacers for the Treatment of Infection Following Total Knee Arthroplasty. J. Bone Jt. Surg. 2020, 102, 778–787. [Google Scholar] [CrossRef]
- Bernard, L.; Arvieux, C.; Brunschweiler, B.; Touchais, S.; Ansart, S.; Bru, J.-P.; Oziol, E.; Boeri, C.; Gras, G.; Druon, J.; et al. Antibiotic Therapy for 6 or 12 Weeks for Prosthetic Joint Infection. N. Engl. J. Med. 2021, 384, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Manning, L.; Metcalf, S.; Dymock, M.; Robinson, O.; Clark, B.; Nelson, R.; Paterson, D.L.; Yates, P.; Loewenthal, M.; Dewar, D.; et al. Short- versus standard-course intravenous antibiotics for peri-prosthetic joint infections managed with debridement and implant retention: A randomised pilot trial using a desirability of outcome ranking (DOOR) endpoint. Int. J. Antimicrob. Agents 2022, 60, 106598. [Google Scholar] [CrossRef] [PubMed]
- Blom, A.W.; Lenguerrand, E.; Strange, S.; Noble, S.M.; Beswick, A.D.; Burston, A.; Garfield, K.; Gooberman-Hill, R.; Harris, S.R.S.; Kunutsor, S.K.; et al. Clinical and cost effectiveness of single stage compared with two stage revision for hip prosthetic joint infection (INFORM): Pragmatic, parallel group, open label, randomised controlled trial. BMJ 2022, 379, e071281. [Google Scholar] [CrossRef] [PubMed]
- Cancer Council Queensland. Australian Cancer Atlas Queensland University of Technology. Available online: https://atlas.cancer.org.au (accessed on 4 June 2023).
- Sinagra, Z.P.; Davis, J.S.; Lorimer, M.; de Steiger, R.N.; Graves, S.E.; Yates, P.; Manning, L. The accuracy of reporting of periprosthetic joint infection to the Australian Orthopaedic Association National Joint Replacement Registry. Bone Jt. Open 2022, 3, 367–374. [Google Scholar] [CrossRef]
- Imber, B.S.; Yahalom, J.M. Radiotherapy for Non-Hodgkin Lymphomas. Cancer J. 2020, 26, 217–230. [Google Scholar] [CrossRef]
- Davis, J.S.; Kang, L.X.; Manning, L.; Dewar, D. Clinician-driven research priorities in bone and joint infection: Perspectives of orthopaedic surgeons and infectious diseases physicians. ANZ J. Surg. 2022, 92, 2790–2792. [Google Scholar] [CrossRef]
- Cooper, C.; Varley-Campbell, J.; Carter, P. Established search filters may miss studies when identifying randomized controlled trials. J. Clin. Epidemiol. 2019, 112, 12–19. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author, Year [Ref] | Trial Registration | Inclusion Criteria | Intervention (s) | Comparator | Primary Outcome | Time Point for Primary Outcome | Sample Size Justification | Target Recruitment (N) | Actual Recruitment (N; Patients with PJI) | Recruitment Period. Sites, N |
|---|---|---|---|---|---|---|---|---|---|---|
| Zimmerli, 1998 [14] | Not registered | Implant infection (stable implant, short duration) | Rifampicin | Placebo | Cure = no clinical signs, CRP < 5 and no radiology | 24 months | Superiority, cure 20% in SOC, 75% in intervention; attrition 20% | 30 | 33 (15 with PJI) | May 1992–1995, 2 centers |
| Munoz-Mahamud, 2011 [23] | Not registered | Implant infection requiring open debridement | High-pressure lavage | Low-pressure lavage | Remission = no symptoms of infection, prosthesis retained, and CRP < 10 | 12 months | Not stated | NA | 79 (70 with PJI) | January 2008–August 2009, single center |
| Byren, 2012 [24] | NCT00428844 | hip or knee PJI undergoing 2-stage revision | Daptomycin 6 mg/kg Daptomycin 8 mg/k | Vancomycin, teicoplanin, or beta-lactam therapy | Creatinine kinase (CK) >500 IU/mL | Up to 7 days following daptomycin cessation | 92% chance of observing at least one occurrence of elevated CK with a true rate of 10% | 72 (24 in each arm) | 75 (73 evaluable) | June 2007–June 2010, 22 sites |
| Bruni, 2013 [25] | Not registered | Patients at second stage of 2-stage revision for PJI of knee | Tibial tuberosity osteotomy | Quadriceps Snip | Knee society score (KSS) | Assessments made 8–15 years after procedure | A 20-point difference in the KSS, power of 80%, attrition 15–20%. | 90 | 81 evaluable | 1997–2004, single center |
| Pushkin, 2016 [26] | NCT01756924 | Hip and knee PJI (or spacer infection) | Rifampicin and fusidic acid | Standard of care | Success = no evidence of infection, antibiotics not changed | 12 weeks for 2-stage, 3–6 months | Not stated | 50 | 14 | April 2013–April 2014. 6 centers |
| Lora-Tamayo, 2016 [27] | ISRCTN35285839 | PJI patients managed with DAIR | Short course levofloxacin and rifampicin (8 weeks) | Long course (3 or 6 months) | Cure = retained prosthesis, no clinical signs of infection were resolved, progressive decrease in CRP | 12 months | Non-inferiority (NI), 75% expected, NI margin 15% | 195 | 63 | April 2009–April 2013, 17 sites |
| Benkabouche, 2019 [28] | NCT03602209 | Implant infections | 4 weeks antibiotic | 6 weeks antibiotic | Remission of infection at the operative site. | 12 months | NI, success rates of 95%, NI margin of 10%. | 120 | 123 (38 with PJI) | 1 March 2015 to 10 March 2018, single-center |
| Li, 2019 [29] | ISRCTN91566927 | Bone and joint infections | Short course IV | Long course IV | Definite treatment failure (clinical, micro, histo) | 12 months | NI, 5% treatment failure, NI margin 5% (increased to 7.5% during trial) | 1050 | 1054 (472 with PJI)) | June 2010–October 2015 recruited, 26 sites |
| Xu, 2019 [30] | ChiCTR-INR-17014162. | Hip PJI, 2-stage revision with a vanc + mero spacer | Closed suction drain | Non- closed suction drain | Antibacterial activity against MSSA, MRSA, and Escherichia. coli during the first five days following spacer implantation. | 5 days | NI, >95% antibacterial Activity, difference 20%, power of 80%, | 32 | 32 | January–November 2018, Single center |
| Nahhas, 2020 [31] | NCT01373112 | knee PJI undergoing 2-stage revision | Articulating spacer | Static | ROM in degrees | At least 2 years | Superiority, 13 degree difference, power 80% alpha 0.05 | 68 | 49 evaluable | July 2011–May 2016, 4 centers |
| Yang, 2020 [21] | NCT01760863 | hip or knee PJI undergoing 2-stage revision | Additional 3 months after 2nd stage | No antibiotics | reinfection as determined by meeting MSIS criteria | “minimum of 2 years” | Superiority; reduction in infection recurrence from 16% to 4%, power 80%, alpha 0.05 | 200 | 185 | 2011–2016, 7 centers |
| Karlsen, 2020 [15] | NCT00423982 | Early or acute Staphylococcal PJI | Rifampicin | Mono | Cure defined as a lack of clinical, biochemical, or radiological signs | 24 | Superiority; SOC group 70%, intervention 90%, power 80% | 200 | 65 (48 evaluable) | January 2007–June 2013, 8 centers |
| Bernard, 2021 [32] | NCT01816009 | PJI—hip and knee (all) | 6 weeks antibiotics | 12 weeks antibiotic | The primary endpoint—persistent infection (same organisms) within 2 years | 24 | NI; expected failure 15%, NI margin 10% | 410 | 410 | November 2011–January 2015, 28 centers |
| Manning, 2022 [33] | ACTRN12617000127303 | Acute PJI managed with DAIR | 2-weeks IV | 6-weeks IV | Seven-level ordinal outcome: Clinical cure will be defined as no clinical or microbiological evidence of infection; original prosthesis still present; and no use of ongoing antibiotic therapy for the index joint | 12 | Explicitly ‘pilot study’ | 60 | 60 | June 2017–30 September 2019, 6 centers |
| Blom, 2022 [34] | ISRCTN10956306 | Hip PJI | 1-stage | 2-stage | Patient-reported WOMAC index | 18 months | Difference of 10 points (0.5 SD) 2-sided type 1 error 0.05 | 148 | 140 | March 2015–December 2018, 15 centers |
| Study | Timing of Outcome Ascertainment | Terminology | C-Reactive protein (mg/L) | Clinical Features | Radiological Features | Microbiological | Destination Prosthesis | Antibiotic Use/Change |
|---|---|---|---|---|---|---|---|---|
| Zimmerli, 1998 [14] | 24 months | Cure | CRP < 5 | No clinical signs or symptoms of infection | No evidence of loosening or pseudoarthrosis | |||
| Munoz-Mahamud, 2011 [23] | 12 months | Remission | CRP < 10 | No symptoms of infection/inflammatory signs | Retained | |||
| Pushkin, 2016 [26] | 3 months (hip) 6 months (knee) | Clinical success | No clinical signs of infection at re-implantation | Negative cultures obtained at re-implantation | Antibiotics not changed | |||
| Lora-Tamayo, 2016 [27] | 12 months | Cure | Progressive decline in CRP | No clinical signs of infection, PJI-related death | Retained | |||
| Benkabouche, 2019 [28] | 12 months | Remission of infection at the infection site | ||||||
| Li, 2019 [29] | 12 months | Definite treatment failure | Sinus | Isolation of identical organisms, histological | ||||
| Yang, 2020 [21] | Minimum of 24 months | Reinfection (MSIS criteria) | Clinical signs | Micro (MSIS) | ||||
| Karlsen, 2020 [15] | 24 months | Cure | CRP < 10 | Lack of clinical signs (e.g., sinus) | No loosening | Retained | ||
| Bernard, 2021 [32] | 24 months | Definite or probable infection (persistent or new) | CRP > 10 | clinical signs of infection (sinus) | Micro |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manning, L.; Allen, B.; Davis, J.S. Design Characteristics and Recruitment Rates for Randomized Trials of Peri-Prosthetic Joint Infection Management: A Systematic Review. Antibiotics 2023, 12, 1486. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12101486
Manning L, Allen B, Davis JS. Design Characteristics and Recruitment Rates for Randomized Trials of Peri-Prosthetic Joint Infection Management: A Systematic Review. Antibiotics. 2023; 12(10):1486. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12101486
Chicago/Turabian StyleManning, Laurens, Bethwyn Allen, and Joshua S. Davis. 2023. "Design Characteristics and Recruitment Rates for Randomized Trials of Peri-Prosthetic Joint Infection Management: A Systematic Review" Antibiotics 12, no. 10: 1486. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12101486