
GPs’ Perspective on a Multimodal Intervention to Enhance Guideline-Adherence in Uncomplicated Urinary Tract Infections: A Qualitative Process Evaluation of the Multicentric RedAres Cluster-Randomised Controlled Trial
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participant Selection
2.3. Setting
2.4. Data Collection
2.5. Research Team and Reflexivity
2.6. Data Analysis
2.7. Ethics
3. Results
3.1. Determinants of Decision Making
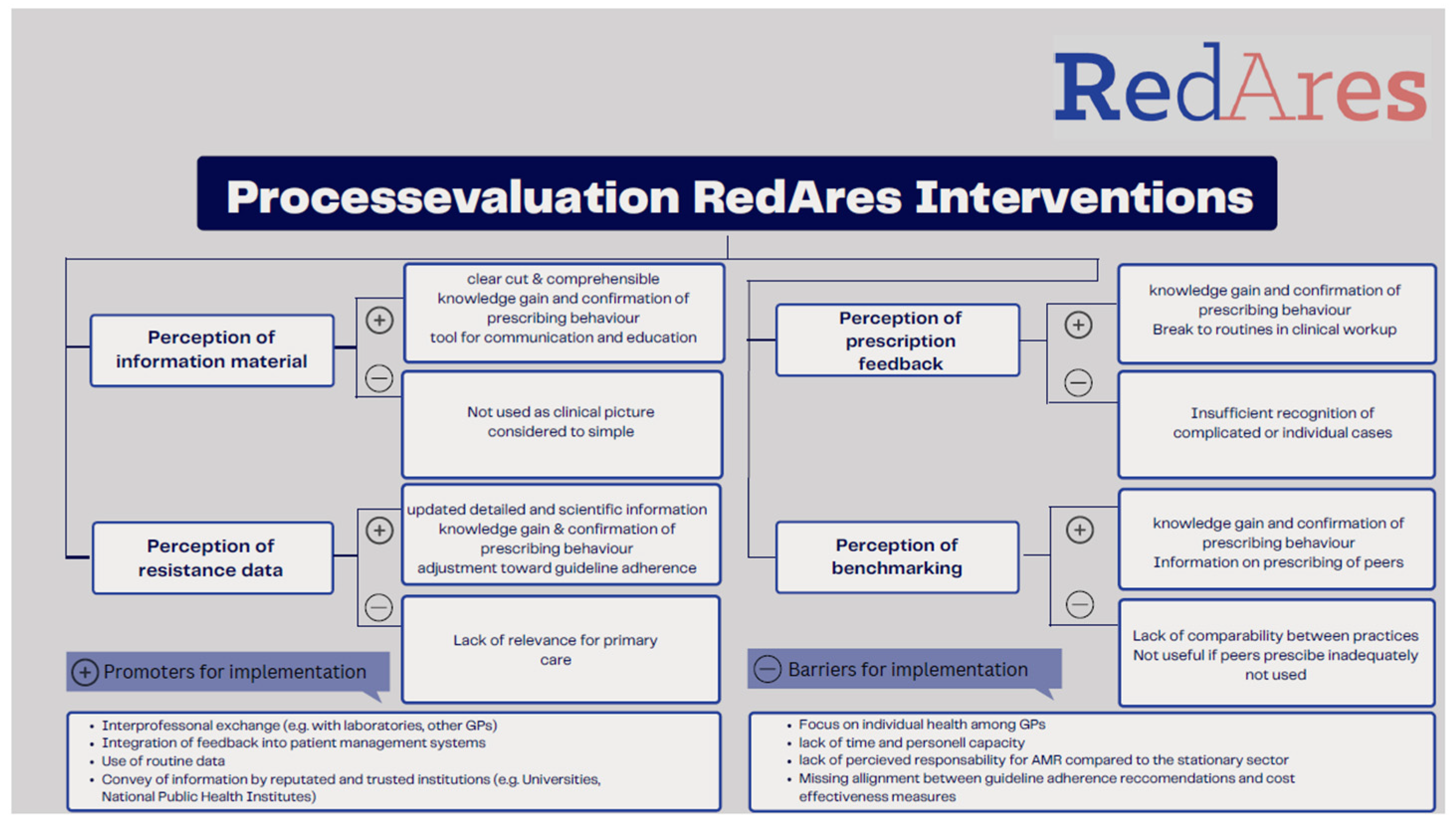
3.2. Perspectives on the RedAres Interventions
3.2.1. Information Material on Guideline Recommendations
3.2.2. Regional Resistance Data
3.2.3. Prescription Feedback
3.2.4. Benchmarking
3.2.5. Perception of the Intervention Format
3.3. Promoting Factors and Barriers for Implementation
4. Discussion
4.1. Potential Drivers for Implementation
4.2. Potential Barriers to Implementation
4.3. Including a Public Health Perspective in Clinical Decision Making
4.4. Strengths and Limitations
5. Conclusions
6. Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- General evaluation of the RedAres study
- Evaluation of content and usability
- Technical and organizational feasibility in the practice and for physician assistants
- Integration of physician assistants
- Determinants of decision-making
- Intervention materials
- Information material
- Evaluation of content and usability
- Evaluation of the format, suggestions for optimization
- RKI resistance data
- Evaluation of content and usability
- Evaluation of the format, suggestions for optimization
- Perspectives on implementation into regular practice
- Prescription feedback
- Evaluation of content and usability
- General evaluation
- Confirmation of prescription behavior, promoting treatment safety
- Gain in knowledge, refreshing contents
- Reflection and adaptation of prescribing behavior
- External experience with prescription feedback
- Evaluation of benchmarking
- General evaluation
- Confirmation of prescription behavior, promoting treatment safety
- Gain in knowledge, refreshing contents
- Reflection and adaptation of prescribing behavior
- External experience with prescription feedback
- Evaluation of the format, suggestions for optimization
- Perspectives on implementation into regular practice
- Attitude towards data protection
References
- Dicheva, S. Harnwegsinfekte bei Frauen. pp. 107–137. Available online: https://www.barmer.de/resource/blob/1026444/60143006d7108440f02512a6a80fcaea/barmer-gek-arzneimittel-report-2015-data.pdf (accessed on 23 December 2022).
- Butler, C.C.; Hawking, M.K.; Quigley, A.; McNulty, C.A. Incidence, severity, help seeking, and management of uncomplicated urinary tract infection: A population-based survey. Br. J. Gen. Pract. 2015, 65, e702–e707. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Chen, H.; Zheng, Y.; Qu, S.; Wang, H.; Yi, F. Disease burden and long-term trends of urinary tract infections: A worldwide report. Front. Public Health 2022, 10, 888205. [Google Scholar] [CrossRef] [PubMed]
- Schmiemann, G.; Hoffmann, F.; Hamprecht, A.; Jobski, K. Patterns and trends of antibacterial treatment in patients with urinary tract infections, 2015–2019: An analysis of health insurance data. BMC Prim. Care 2022, 23, 204. [Google Scholar] [CrossRef] [PubMed]
- Gágyor, I.; Strube-Plaschke, S.; Rentzsch, K.; Himmel, W. Management of urinary tract infections: What do doctors recommend and patients do? An observational study in German primary care. BMC Infect. Dis. 2020, 20, 813. [Google Scholar] [CrossRef]
- Mulder, M.; Baan, E.; Verbon, A.; Stricker, B.; Verhamme, K. Trends of prescribing antimicrobial drugs for urinary tract infections in primary care in the Netherlands: A population-based cohort study. BMJ Open 2019, 9, e027221. [Google Scholar] [CrossRef]
- Butler, C.C.; Francis, N.; Thomas-Jones, E.; Llor, C.; Bongard, E.; Moore, M.; Little, P.; Bates, J.; Lau, M.; Pickles, T.; et al. Variations in presentation, management, and patient outcomes of urinary tract infection: A prospective four-country primary care observational cohort study. Br. J. Gen. Pract. 2017, 67, e830–e841. [Google Scholar] [CrossRef]
- Petersen, I.; Hayward, A.C.; on behalf of the SACAR Surveillance Subgroup. Antibacterial prescribing in primary care. J. Antimicrob. Chemother. 2007, 60, i43–i47. [Google Scholar] [CrossRef]
- van Driel, A.A.; Mulder, M.; Stobberingh, E.E.; Verbon, A. Adherence to and usefulness of the national treatment guideline for urinary tract infections (UTI) in a risk area. BMC Prim. Care 2022, 23, 224. [Google Scholar] [CrossRef]
- Tempera, G.; Furneri, P.M.; Cianci, A.; Incognito, T.; Marano, M.R.; Drago, F. The Impact of Prulifloxacin on Vaginal Lactobacillus Microflora: An In Vivo Study. J. Chemother. 2009, 21, 646–650. [Google Scholar] [CrossRef]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef]
- Barosi, G. Strategies for dissemination and implementation of guidelines. Neurol. Sci. 2006, 27, s231–s234. [Google Scholar] [CrossRef] [PubMed]
- Deutsche Gesellschaft für Allgemeinmedizin und Familienmedizin (DEGAM) Brennen Beim Wasserlassen, S3-Leitlinie und Anwenderversion der S3-Leitlinie Harnwegsinfektion. 2018, p. 78. Available online: https://register.awmf.org/assets/guidelines/053-001k_S3_Brennen_beim_Wasserlassen_2018-08.pdf (accessed on 23 December 2022).
- Leitlinienprogramm DGU, AWMF. Interdisziplinäre S3 Leitlinie: Epidemiologie, Diagnostik, Therapie, Prävention und Management Unkomplizierter, Bakterieller, Ambulant Erworbener Harnwegsinfektionen bei Erwachsenen Patienten. Kurzversion 1.1.-2. 2017 AWMF Registernummer: /044. Available online: https://register.awmf.org/assets/guidelines/043-044k_S3_Harnwegsinfektionen_2017-05.pdf (accessed on 30 January 2023).
- Kranz, J.; Schmidt, S.; Lebert, C.; Schneidewind, L.; Schmiemann, G.; Wagenlehner, F. Uncomplicated Bacterial Community-acquired Urinary Tract Infection in Adults. Dtsch. Ärztebl. Int. 2017, 114, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Rabanaque, G.; López, A.; Cots, J.M. The adherence of GPs to guidelines for the diagnosis and treatment of lower urinary tract infections in women is poor. Fam. Pract. 2011, 28, 294–299. [Google Scholar] [CrossRef] [PubMed]
- McIsaac, W.J.; Moineddin, R.; Ross, S. Validation of a Decision Aid to Assist Physicians in Reducing Unnecessary Antibiotic Drug Use for Acute Cystitis. Arch. Intern. Med. 2007, 167, 2201–2206. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Dunstan, F.; Heginbothom, M.; Mason, B.; Roberts, Z.; Hillier, S.; Howe, R.; Palmer, S.; Howard, A. Containing antibiotic resistance: Decreased antibiotic-resistant coliform urinary tract infections with reduction in antibiotic prescribing by general practices. Br. J. Gen. Pract. 2007, 57, 785–792. [Google Scholar]
- Petruschke, I.; Stichling, K.; Greser, A.; Gagyor, I.; Bleidorn, J. The general practitioner perspective of a multimodal intervention for the adequate use of antibiotics in urinary tract infection–A qualitative interview study. Z. Evidenz Fortbild. Qual. Im Gesundheitswesen 2022, 170, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Selbmann, H.-K.; Kopp, I. Implementierung von Leitlinien in den Versorgungsalltag. Die Psychiatr. 2005, 2, 33–38. [Google Scholar]
- Vellinga, A.; Galvin, S.; Duane, S.; Callan, A.; Bennett, K.; Cormican, M.; Domegan, C.; Murphy, A.W. Intervention to improve the quality of antimicrobial prescribing for urinary tract infection: A cluster randomized trial. CMAJ 2016, 188, 108–115. [Google Scholar] [CrossRef]
- Arnold, S.R.; Straus, S.E. Interventions to improve antibiotic prescribing practices in ambulatory care. Cochrane Database Syst. Rev. 2005, 2005, CD003539. [Google Scholar] [CrossRef]
- Petruschke, I.; Salm, F.; Kaufmann, M.; Freytag, A.; Gensichen, J.; Behnke, M.; Kramer, T.S.; Hanke, R.; Gastmeier, P.; Schneider, S.; et al. Evaluation of a multimodal intervention to promote rational antibiotic use in primary care. Antimicrob. Resist. Infect. Control 2021, 10, 66. [Google Scholar] [CrossRef]
- Bouchet, F.; Le Moing, V.; Dirand, D.; Cros, F.; Lienard, A.; Reynes, J.; Giraudon, L.; Morquin, D. Effectiveness and Acceptance of Multimodal Antibiotic Stewardship Program: Considering Progressive Implementation and Complementary Strategies. Antibiotics 2020, 9, 848. [Google Scholar] [CrossRef] [PubMed]
- Proctor, E.K.; Powell, B.J.; McMillen, J.C. Implementation strategies: Recommendations for specifying and reporting. Implement. Sci. 2013, 8, 139. [Google Scholar] [CrossRef] [PubMed]
- Sijbom, M.; Büchner, F.L.; Saadah, N.H.; Numans, M.E.; de Boer, M.G.J. Determinants of inappropriate antibiotic prescription in primary care in developed countries with general practitioners as gatekeepers: A systematic review and construction of a framework. BMJ Open 2023, 13, e065006. [Google Scholar] [CrossRef] [PubMed]
- Lugtenberg, M.; Zegers-van Schaick, J.M.; Westert, G.P.; Burgers, J.S. Why don’t physicians adhere to guideline recommendations in practice? An analysis of barriers among Dutch general practitioners. Implement. Sci. 2009, 4, 54. [Google Scholar] [CrossRef]
- Cranney, M.; Warren, E.; Barton, S.; Gardner, K.; Walley, T. Why do GPs not implement evidence-based guidelines? A descriptive study. Fam. Pract. 2001, 18, 359–363. [Google Scholar] [CrossRef] [PubMed]
- Harbin, N.J.; Lindbæk, M.; Romøren, M. Barriers and facilitators of appropriate antibiotic use in primary care institutions after an antibiotic quality improvement program—A nested qualitative study. BMC Geriatr. 2022, 22, 458. [Google Scholar] [CrossRef]
- Rocha, V.; Estrela, M.; Neto, V.; Roque, F.; Figueiras, A.; Herdeiro, M.T. Educational Interventions to Reduce Prescription and Dispensing of Antibiotics in Primary Care: A Systematic Review of Economic Impact. Antibiotics 2022, 11, 1186. [Google Scholar] [CrossRef]
- Mentzel, A.; Maun, A. Ambulantes Verordnungsverhalten von Antibiotika und Einstellung zum Verordnungsfeedback. Z. Allg. 2023, 99, 21–27. [Google Scholar] [CrossRef]
- Schmiemann, G.; Greser, A.; Maun, A.; Bleidorn, J.; Schuster, A.; Miljukov, O.; Rücker, V.; Klingeberg, A.; Mentzel, A.; Minin, V.; et al. Effects of a multimodal intervention in primary care to reduce second line antibiotic prescriptions for urinary tract infections in women: Parallel, cluster randomised, controlled trial. BMJ 2023, 383, e076305. [Google Scholar] [CrossRef]
- Gágyor, I.; Greser, A.; Heuschmann, P.; Rücker, V.; Maun, A.; Bleidorn, J.; Heintze, C.; Jede, F.; Eckmanns, T.; Klingeberg, A.; et al. REDuction of Antibiotic RESistance (REDARES) in urinary tract infections using treatments according to national clinical guidelines: Study protocol for a pragmatic randomized controlled trial with a multimodal intervention in primary care. BMC Infect. Dis. 2021, 21, 990. [Google Scholar] [CrossRef] [PubMed]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Mayring, P.; Fenzl, T. Qualitative Inhaltsanalyse. In Handbuch Methoden der Empirischen Sozialforschung; Baur, N., Blasius, J., Eds.; Springer Fachmedien: Wiesbaden, Germany, 2019; pp. 633–648. [Google Scholar] [CrossRef]
- Mayring, P. Qualitative Content Analysis: Theoretical Foundation, Basic Procedures and Software Solution; Beltz: Klagenfurt, Austria, 2014; 143p. [Google Scholar]
- Butler, C.C.; Simpson, S.A.; Dunstan, F.; Rollnick, S.; Cohen, D.; Gillespie, D.; Evans, M.R.; Alam, M.F.; Bekkers, M.-J.; Evans, J.; et al. Effectiveness of multifaceted educational programme to reduce antibiotic dispensing in primary care: Practice based randomised controlled trial. BMJ 2012, 344, d8173. [Google Scholar] [CrossRef] [PubMed]
- Vervloet, M.; Meulepas, M.A.; Cals, J.W.L.; Eimers, M.; van der Hoek, L.S.; van Dijk, L. Reducing antibiotic prescriptions for respiratory tract infections in family practice: Results of a cluster randomized controlled trial evaluating a multifaceted peer-group-based intervention. NPJ Prim. Care Respir. Med. 2016, 26, 15083. [Google Scholar] [CrossRef] [PubMed]
- Robertson, N.; Baker, R.; Hearnshaw, H. Changing the clinical behavior of doctors: A psychological framework. Qual. Health Care QHC 1996, 5, 51–54. [Google Scholar] [CrossRef]
- Bandura, A. Perceived self-efficacy in the exercise of personal agency. J. Appl. Sport Psychol. 1990, 2, 128–163. [Google Scholar] [CrossRef]
- Biezen, R.; Ciavarella, S.; Manski-Nankervis, J.-A.; Monaghan, T.; Buising, K. Addressing Antimicrobial Stewardship in Primary Care-Developing Patient Information Sheets Using Co-Design Methodology. Antibiotics 2023, 12, 458. [Google Scholar] [CrossRef]
- UK Health Security Agency. GOV.UK. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR) Report 2021 to 2022. Available online: https://www.gov.uk/government/publications/english-surveillance-programme-antimicrobial-utilisation-and-resistance-espaur-report (accessed on 30 January 2023).
- Swedres-Svarm Consumption of Antibiotics and Occurence of Antibiotic Resistance in Sweden 2014; Solna/Uppsala. 2015. Report No.: ISSN 1650-6332. Available online: https://www.sva.se/media/e5mpndxz/rapport_swedres-svarm_2014.pdf (accessed on 30 January 2023).
- Goossens, H.; Ferech, M.; Vander Stichele, R.; Elseviers, M.; ESAC Project Group. Outpatient antibiotic use in Europe and association with resistance: A cross-national database study. Lancet 2005, 365, 579–587. [Google Scholar] [CrossRef]
- Wood, F.; Phillips, C.; Brookes-Howell, L.; Hood, K.; Verheij, T.; Coenen, S.; Little, P.; Melbye, H.; Godycki-Cwirko, M.; Jakobsen, K.; et al. Primary care clinicians’ perceptions of antibiotic resistance: A multi-country qualitative interview study. J. Antimicrob. Chemother. 2013, 68, 237–243. [Google Scholar] [CrossRef]
- Bollig, E.R.; Hirsch, E.B.; Bueno, I.; Lynfield, R.; Granick, J.L.; Gens, K.D.; Rashid, A.; Harris, K.; Boeser, K.; Beaudoin, A.L. Minnesota One Health Antibiotic Stewardship Collaborative: A Reproducible Approach to Facilitate Antimicrobial Stewardship Progress. Open Forum Infect. Dis. 2022, 9, ofac602. [Google Scholar] [CrossRef]
- Reeves, S.; Pelone, F.; Harrison, R.; Goldman, J.; Zwarenstein, M. Interprofessional collaboration to improve professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2017, 6, CD000072. [Google Scholar] [CrossRef]
- Davis, D.A.; Thomson, M.A.; Oxman, A.D.; Haynes, R.B. Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA 1995, 274, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Kuehlein, T.; Goetz, K.; Laux, G.; Gutscher, A.; Szecsenyi, J.; Joos, S. Antibiotics in urinary-tract infections. Sustained change in prescribing habits by practice test and self-reflection: A mixed methods before-after study. BMJ Qual. Saf. 2011, 20, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.O.; Diclemente, C.C. Toward a Comprehensive Model of Change. In Treating Addictive Behaviors: Processes of Change; Miller, W.R., Heather, N., Eds.; Applied Clinical Psychology; Springer: Boston, MA, USA, 1986; pp. 3–27. ISBN 978-1-4613-2191-0. [Google Scholar] [CrossRef]
- Marwick, C.A.; Hossain, A.; Nogueira, R.; Sneddon, J.; Kavanagh, K.; Bennie, M.; Seaton, R.A.; Guthrie, B.; Malcolm, W. Feedback of Antibiotic Prescribing in Primary Care (FAPPC) trial: Results of a real-world cluster randomized controlled trial in Scotland, UK. J. Antimicrob. Chemother. 2022, 77, 3291–3300. [Google Scholar] [CrossRef] [PubMed]
- Molstad, S.; Cars, O.; Struwe, J. Strama—A Swedish working model for containment of antibiotic resistance. Eurosurveillance 2008, 13, 19041. [Google Scholar] [CrossRef] [PubMed]
- Hallsworth, M.; Chadborn, T.; Sallis, A.; Sanders, M.; Berry, D.; Greaves, F.; Clements, L.; Davies, S.C. Provision of social norm feedback to high prescribers of antibiotics in general practice: A pragmatic national randomised controlled trial. Lancet 2016, 387, 1743–1752. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health and Aged Care. Nudge vs. Superbugs: A Report into a Behavioural Economics Trial to Reduce the Overprescribing of Antibiotics; Australian Government Department of Health and Aged Care: Canberra, Australia, 2021. Available online: https://www.health.gov.au/resources/publications/nudge-vs-superbugs?language=en (accessed on 30 January 2023).
- Wang, K.Y.; Seed, P.; Schofield, P.; Ibrahim, S.; Ashworth, M. Which practices are high antibiotic prescribers? A cross-sectional analysis. Br. J. Gen. Pract. 2009, 59, e315–e320. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Cui, Z.; Liao, X.; He, X.; Wang, L.; Wei, D.; Wu, S.; Chang, Y. Effects of a feedback intervention on antibiotic prescription control in primary care institutions based on a Health Information System: A cluster randomized cross-over controlled trial. J. Glob. Antimicrob. Resist. 2023, 33, 51–60. [Google Scholar] [CrossRef]
- Gastmeier, P.; Bleidorn, J.; Salm, F.; Kramer, T.; Remschmidt, C.; Wiese-Posselt, M.; Schneider, S.; mooc.house. Rationale Antibiotikatherapie in der Hausärztlichen Versorgung. 2020. Available online: https://mooc.house/courses/rai1-3 (accessed on 30 January 2023).
- Armstrong, D.; Reyburn, H.; Jones, R. A study of general practitioners’ reasons for changing their prescribing behaviour. BMJ 1996, 312, 949–952. [Google Scholar] [CrossRef]
- Klingeberg, A.; Noll, I.; Willrich, N.; Feig, M.; Emrich, D.; Zill, E.; Krenz-Weinreich, A.; Kalka-Moll, W.; Oberdorfer, K.; Schmiemann, G.; et al. Antibiotic-Resistant E. coli in Uncomplicated Community-Acquired Urinary Tract Infection. Dtsch. Arzteblatt Int. 2018, 115, 494–500. [Google Scholar] [CrossRef]
- Spurling, G.K.; Mansfield, P.R.; Montgomery, B.D.; Lexchin, J.; Doust, J.; Othman, N.; Vitry, A.I. Information from pharmaceutical companies and the quality, quantity, and cost of physicians’ prescribing: A systematic review. PLoS Med. 2010, 7, e1000352. [Google Scholar] [CrossRef]
- Klerings, I.; Weinhandl, A.S.; Thaler, K.J. Information overload in healthcare: Too much of a good thing? Z. Evidenz Fortbild. Qual. Im Gesundheitswesen 2015, 109, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Greer, S.L.; Wismar, M.; Figueras, J.; European Observatory on Health Systems and Policies (Eds.) Strengthening Health System Governance: Better Policies, Stronger Performance; European Observatory on Health Systems and Policies Series; Open University Press: Maidenhead, UK, 2016; 272p. [Google Scholar]
- Rogers Van Katwyk, S.; Grimshaw, J.M.; Nkangu, M.; Nagi, R.; Mendelson, M.; Taljaard, M.; Hoffman, S.J. Government policy interventions to reduce human antimicrobial use: A systematic review and evidence map. PLoS Med. 2019, 16, e1002819. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.; Hsiung, C.A.; Yu, H.-T.; Chi, C.-L.; Chang, H.-J. Changes before and after a policy to restrict antimicrobial usage in upper respiratory infections in Taiwan. Int. J. Antimicrob. Agents 2004, 23, 438–445. [Google Scholar] [CrossRef] [PubMed]
- Ellegård, L.M.; Dietrichson, J.; Anell, A. Can pay-for-performance to primary care providers stimulate appropriate use of antibiotics? Health Econ. 2018, 27, e39–e54. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, Y.; Feldhaus, I.; Özçelik, E.; Hashiguchi, T.C.O.; Cecchini, M. Financial strategies targeting healthcare providers to promote the prudent use of antibiotics: A systematic review of the evidence. Int. J. Antimicrob. Agents 2021, 58, 106446. [Google Scholar] [CrossRef]
- Raupach, T.; de Temple, I.; Middeke, A.; Anders, S.; Morton, C.; Schuelper, N. Effectiveness of a serious game addressing guideline adherence: Cohort study with 1.5-year follow-up. BMC Med. Educ. 2021, 21, 189. [Google Scholar] [CrossRef] [PubMed]
- Simpson, S.A.; Wood, F.; Butler, C.C. General practitioners’ perceptions of antimicrobial resistance: A qualitative study. J. Antimicrob. Chemother. 2007, 59, 292–296. [Google Scholar] [CrossRef]
- Gutscher, A.; Szecsenyi, J.; Götz, K.; Joos, S.; Hermann, K. Qualitative Ergebnisse einer Mixed-Methods-Studie zur Verordnung von Antibiotika bei Harnwegsinfekten-Gemeinwohl versus Wohl des Einzelnen... Habe ich Noch nie Drüber Nachgedacht“-Online ZFA. 17 October 2012. Available online: https://www.online-zfa.de/archiv/ausgabe/artikel/zfa-10-2012/47963-103238-zfa20120401-0407-gemeinwohl-versus-wohl-des-einzelnen-habe-ich-noch-nie-drueber/ (accessed on 30 January 2023).
- Borek, A.J.; Santillo, M.; Wanat, M.; Butler, C.C.; Tonkin-Crine, S. How can behavioural science contribute to qualitative research on antimicrobial stewardship in primary care? JAC-Antimicrob. Resist. 2022, 4, dlac007. [Google Scholar] [CrossRef]
- Janis, I.L. Groupthink: Psychological Studies of Policy Decisions and Fiascoes; Houghton Mifflin: Boston, MA, USA, 1982; 374p, Available online: https://archive.org/details/groupthinkpsycho00jani/page/n7/mode/2up (accessed on 30 January 2023).
- Latané, B. The psychology of social impact. Am. Psychol. 1981, 36, 343–356. [Google Scholar] [CrossRef]
- Grimm, P. Social Desirability Bias. In Wiley International Encyclopedia of Marketing; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2010; Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1002/9781444316568.wiem02057 (accessed on 30 January 2023).


{kind=link}
| Subcategory | Citation |
|---|---|
| Perceived competence | “Basically, I need a lot of routine and then I feel safe.” (10-by_int_63: 29) “Sometimes you feel insecure there […] confidence comes when you have evidence-based guidelines, where you can say, okay, this helps and I’m doing everything right.” (17-by_int_09: 28) |
| Collegial exchange | “We are lucky enough to have such a round table of further education in our region. […] There’s a relatively large amount of exchange in collegial discussions, and […] questions like these [about antibiotic prescriptions] also come up in the round afterwards” (4-ber_int_25: 31) |
| Time constraints | “If I treated all my patients according to the guidelines, they would be busy with medicine all day. So [...] you can read through it, that’s what we do, but I can’t really sign off on treating patients absolutely according to guidelines.” (5-bw_int_49: 21) |
| Quality of information | “With some recommendations, one has nevertheless somewhat the hidden suspicion if there are industrial interests [...] behind it. One will then perhaps sometimes be a little more defensive.” (11-bw_int_60: 37) “You also get a lot of information that is almost too much [...], then you can get quite lost in all this stuff [...].” (15-th_int_34: 42) |
| Category | Subcategory | Citation |
|---|---|---|
| Information material | Knowledge and confirmation | “Yes, it was a good refresher for me.” (15-th_int_34: 18) “some drugs like [...] Pivmecillinam were unknown to me.” (9-by_int_10: 35) |
| Education and patient communication | “I also gave [the information material] to the training assistants and talked to them. And that was also good feedback for both of us.” (2-ber_int_05: 15) “Materials for patients are also important. Particularly when they are faced with unfamiliar therapeutic decisions [...] it is nice to have an argumentation paper with the stamp of the [university clinic] or a larger institution.” (2-ber_int_05: 25) | |
| Regional resistance data | Knowledge and confirmation, breaking routines | “That was an eye-opener. [...] I was very grateful for this information, because I really wouldn’t have gone to the Robert Koch Institute website on my own.” (14-bw_int_57: 25) “What came from the Robert Koch Institute is also well in line with our practice”. (13-by_int_69: 51) “Especially with uncomplicated infections, you don’t think too much about what you prescribed, what you prescribed last time. [...]. But it’s interesting to have that presented to you and to see, oh, you took this (decision) once, which you actually didn’t want to take anymore.” (4-ber_int_25: 51) |
| Relevance for practice | “Resistance avoidance is a relevant point [...] I just think that the regional resistance data do not influence every decision.” (16-bw_int_56: 38) “I think it’s more relevant in the stationary setting, because we often don’t have these decisions that require antibiotic stewardship [...] I think we must set other priorities” (16-bw_int_56: 34) | |
| Prescription feedback | Knowledge and confirmation | “You think: Well, we’re doing everything right, and so on. But it’s nice to see it again in print and then finally quoted in some kind of diagram.” (2-ber_int_05: 65) “that’s what makes reflection possible in the first place [...] it [...] provides an opportunity for discussion and reflection.” (12-th_int_36: 65) |
| Experiences and hurdles | “I prescribe [antibiotics] and say: [...] the urinary tract infection is so strong you have to take it now. [...] or they just get it as a backup for the next time.” (5-bw_int_49: 49–53) “We get feedback [from the Association of Statutory health insurance Physicians], not about the resistances and the right antibiotic, but about [economic] prescribing behaviour.” (17-by_int_09: 54) | |
| Benchmarking | Knowledge and confirmation | “Actually, I think that’s quite good, because you actually compare yourself a bit. [...] So if I were completely off the mark, I would ask myself: What am I doing differently? (6-th_int_44: 73) “The comparison has somehow also shown that we have actually done quite well [...] encouraging me to continue in this way.” (19-by_int_65: 73) |
| Experiences and hurdles | “And I think that’s problematic in part because you can’t compare the practices with each other”. (17-by_int_09: 54)“I don’t necessarily always have to compare myself with others.” (14-bw_int_57: 45) | |
| Intervention format | Experiences and hurdles | “I need a clear recommendation from which I can derive a clear recommendation for the individual case. [...] I also don’t need a lot of justifications or [...] references to studies. Basically, I need a mini guideline that I can use.” (10-by_int_63: 29) |
| Category | Subcategory | Citation |
|---|---|---|
| Promoting factors | Information streams | “So [with] local resistance situations [...] I would hope that it would be mirrored more often in the future via the laboratory.” (19-by_int_65: 61) |
| Presentation of information | “Generally, I think that this feedback is very useful. Especially if [...] coupled with [...] information that is short and [...] that considers essential aspects of recent developments or guidelines.” (18-ber_int_19: 74) “You can do this anonymously and simply say: [...] we have observed in your region that it is like this and like that [...]. Now, if someone points the finger at a particular colleague and says: “You did this and that wrong”, then, of course, it’s not comfortable on a personal level.” (4-ber_int_25: 83) | |
| Use of routine data | “So, more transparency and more [...] data collection. [...] We need the routine data, [...] how else are we really going to make serious scientific progress”. (18-ber_int_19: 98–100) “I mean, in the end you have to say that if you take the individual data into account, you can of course subdivide them a bit more precisely [...].” (3-by_int_66: 65) | |
| Barriers | Comparability | Therefore, I find it relatively difficult to compare the practices with each other [...] So I wouldn’t draw any information from it if it said that I prescribed something completely different than all the other practices.” (4-ber_int_25: 65) |
| Data misuse | So [the possibility to access the data] should really only be available to independent research institutions [...]. As soon as there are any possibilities that this could drift into pharmaceutical companies [...] then of course it is very problematic.” (12-th_int_36: 81) | |
| Financial penalties | “We always get the information from the Association of Statutory Health Insurance Physicians about which drugs we prescribe too much. But there, it is always associated with severe penalties [...]. Of course, I don’t think that’s such a good thing.” (10-by_int_63: 75) | |
| Conflict of interests | “If you always [...] list drugs that are not in discount contracts or that are not among the cheaper ones, then we get audit problems because we are required to meet certain targets for those in primary care.” (9-by_int_10: 17) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schuster, A.; Tigges, P.; Grune, J.; Kraft, J.; Greser, A.; Gágyor, I.; Boehme, M.; Eckmanns, T.; Klingeberg, A.; Maun, A.; et al. GPs’ Perspective on a Multimodal Intervention to Enhance Guideline-Adherence in Uncomplicated Urinary Tract Infections: A Qualitative Process Evaluation of the Multicentric RedAres Cluster-Randomised Controlled Trial. Antibiotics 2023, 12, 1657. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12121657
Schuster A, Tigges P, Grune J, Kraft J, Greser A, Gágyor I, Boehme M, Eckmanns T, Klingeberg A, Maun A, et al. GPs’ Perspective on a Multimodal Intervention to Enhance Guideline-Adherence in Uncomplicated Urinary Tract Infections: A Qualitative Process Evaluation of the Multicentric RedAres Cluster-Randomised Controlled Trial. Antibiotics. 2023; 12(12):1657. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12121657
Chicago/Turabian StyleSchuster, Angela, Paula Tigges, Julianna Grune, Judith Kraft, Alexandra Greser, Ildikó Gágyor, Mandy Boehme, Tim Eckmanns, Anja Klingeberg, Andy Maun, and et al. 2023. "GPs’ Perspective on a Multimodal Intervention to Enhance Guideline-Adherence in Uncomplicated Urinary Tract Infections: A Qualitative Process Evaluation of the Multicentric RedAres Cluster-Randomised Controlled Trial" Antibiotics 12, no. 12: 1657. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics12121657