A Mini-Review on Ceftaroline in Bacteremia Patients with Methicillin-Resistant Staphylococcus aureus (MRSA) Infections


Abstract
:1. Introduction
2. Data Sources
3. Chemistry/Mode of Action/Pharmacology
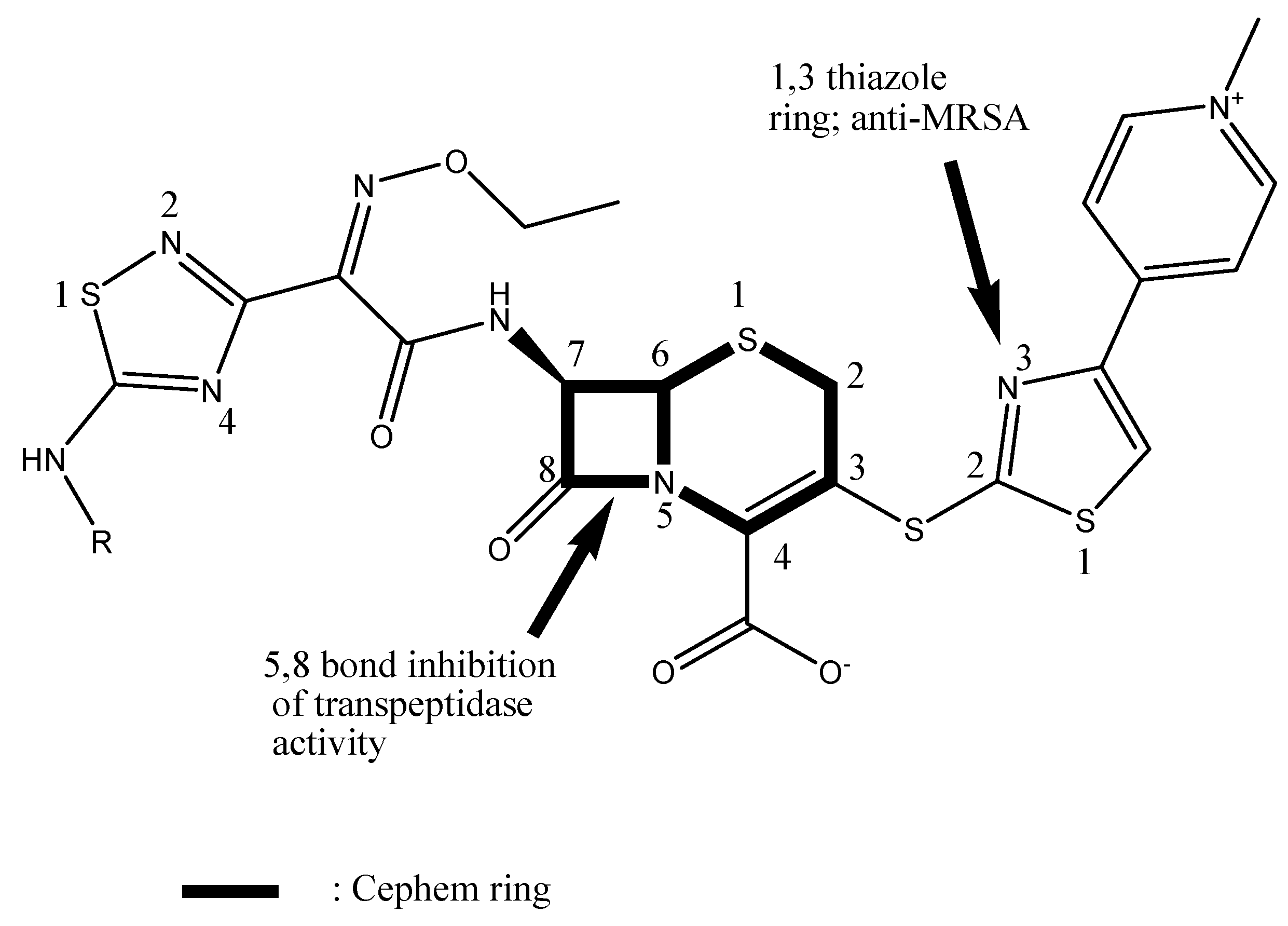
3.1. Chemistry and mode of action of ceftaroline
3.2. In Vitro Antimicrobial Activity of Ceftaroline against S. aureus
4. Specific Populations
4.1. Ceftaroline Use in Pediatrics MRSA
4.2. Adults MRSAB
5. Conclusions
- Some evidence in literature suggests that ceftaroline used for the treatment of MRSA has been shown to be successful in some cases in terms of clinical cure.
- A combination of ceftaroline and daptomycin has shown to be successful in treating patients with MRSA infections in both adult and pediatric populations.
- A synergy mechanism was observed in vitro when ceftaroline was added to daptomycin therapy. Clinical evidence of the benefits of the combination of the two drugs still needs to be thoroughly studied.
- There is still limited data to date regarding the efficacy of ceftaroline alone or when compared to other antibiotics for the treatment of MRSA like quinupristin-dalfopristin, trimethoprim-sulfamethoxazole, linezolid, and telavancin.
- Evidence suggests that ceftaroline has been shown to be safe when administered in both adults and pediatrics.
Author Contributions
Funding
Conflicts of Interest
References
- Scott, L.J. Ceftaroline fosamil: A review in complicated skin and soft tissue infections and community-acquired pneumonia. Drugs 2016, 76, 1659–1674. [Google Scholar] [CrossRef] [PubMed]
- File, T.M., Jr.; Low, D.E.; Eckburg, P.B.; Talbot, G.H.; Friedland, H.D.; Lee, J.; Llorens, L.; Critchley, I.A.; Thye, D.A.; Focus 1 Investigators. FOCUS1: A randomized, double blinded, multicenter, Phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftaroline in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Low, D.E.; File, T.M., Jr.; Eckburg, P.B.; Talbot, G.H.; Friedland, H.D.; Lee, J.; Llorens, L.; Crichley, I.A.; Thye, D.A.; Focus 2 Investigators. FOCUS 2: A randomized, double blinded, multicenter, phase III trial of the efficacy and safety of ceftaroline fosamil versus ceftriaxone in community-acquired pneumonia. J. Antimicrob. Chemother. 2011, 66, 33–44. [Google Scholar] [CrossRef] [PubMed]
- File, T.M., Jr.; Wilcox, M.H.; Stein, G.E. Summary of ceftaroline fosamil clinical trial studies and clinical safety. Clin. Infect. Dis. 2012, 55, 173–180. [Google Scholar] [CrossRef]
- Kollef, M.H. New antimicrobial agents for methicillin-resistant Staphylococcus aureus. Crit. Care Resusc. 2009, 11, 282–286. [Google Scholar] [PubMed]
- Ishikawa, T.; Matsunaga, N.; Tawada, H.; Kuroda, N.; Nakayama, Y.; Ishibashi, Y.; Tomimoto, M.; Ikeda, Y.; Tagawa, Y.; Iizawa, Y.; et al. Tak-599, a novel N-phosphono type prodrug of anti-MRSA cephalosporin T-01825: Synthesis, physicochemical and pharmacological properties. Bioorg. Med. Chem. 2003, 11, 2427–2437. [Google Scholar] [CrossRef]
- Zapun, A.; Contreras-Martel, C.; Vernet, T. Penicillin-binding proteins and beta-lactam resistance. FEMS Microbiol. Rev. 2008, 32, 361–385. [Google Scholar] [CrossRef] [PubMed]
- Kosowska-Shick, K.; McGhee, P.L.; Appelbaum, P.C. Affinity of ceftaroline and other beta-lactams for penicillin-binding proteins from Staphylococcus aureus and Streptococcus pneumoniae. Antimicrob. Agents Chemother. 2010, 54, 1670–1677. [Google Scholar] [CrossRef]
- Llarull, L.I.; Fisher, J.F.; Mobashery, S. Molecular basis and phenotype of methicillin resistance in Staphylococcus aureus and insights into new beta-lactams that meet the challenge. Antimicrob. Agents Chemother. 2009, 53, 4051–4063. [Google Scholar] [CrossRef] [PubMed]
- Zhanel, G.G.; Sniezek, G.; Schweizer, F.; Zelenitsky, S.; Lagacé-Wiens, P.R.; Rubinstein, E.; Gin, A.S.; Hoban, D.J.; Karlowsky, J.A. Ceftaroline: A novel broad-spectrum cephalosporin with activity against methicillin-resistant Staphylococcus aureus. Drugs 2009, 69, 809–831. [Google Scholar] [CrossRef] [PubMed]
- Ge, Y.; Redman, R.; Floren, L.; Liao, S.; Wikler, M. The pharmacokinetics and safety of ceftaroline (PPI-0903) in healthy subjects receiving multiple-dose intravenous infusions. In Proceedings of the 46th Interscience Conference on Antimicrobial Agents and Chemotherapy, San Francisco, CA, USA, 27–30 September 2006. [Google Scholar]
- Ikeda, Y.; Ban, J.; Ishikawa, T.; Hashiguchi, S.; Urayama, S.; Horibe, H. Stability and stabilization studies of TAK-599 (ceftaroline fosamil) a novel N-phosphono type prodrug of anti-methicillin resistant Staphylococcus aureus cephalosporin T-91825. Chem. Pharm. Bull. 2008, 56, 1406–1411. [Google Scholar] [CrossRef] [PubMed]
- Korczowski, B.; Antadze, T.; Giorgobiani, M.; Stryjewski, M.E.; Jandourek, A.; Smith, A.; O’Neal, T.; Bradley, J.S. A multicenter, randomized, observer-blinded, active-controlled study to evaluate the safety and efficacy of ceftaroline versus comparator in pediatric patients with acute bacterial skin and skin structure infection. Pediatr. Infect. Dis. J. 2016, 35, 239–247. [Google Scholar] [CrossRef]
- Sader, H.S.; Mendes, R.E.; Farrell, D.J.; Flamm, R.K.; Jones, R.N. Ceftaroline activity tested against bacterial isolates from pediatric patients: Results from the assessing worldwide antimicrobial resistance and evaluation program for the United States (2011–2012). Pediatr. Infect. Dis. J. 2014, 33, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Dukic, V.M.; Lauderdale, D.S.; Wilder, J.; Daum, R.S.; David, M.Z. Epidemics of community associated methicillin-resistant Staphylococcus aureus in the United States; a meta-analysis. PLoS ONE 2013, 8, e52722. [Google Scholar] [CrossRef] [PubMed]
- Blumer, J.; Ghonghazde, T.; Cannavino, C.; O’Neal, T.; Jandourek, A.; Friedland, H.D.; Bradley, J.S. A multicenter, randomized, observer-blinded, active-controlled study evaluating the safety and effectiveness of ceftaroline compared with ceftriaxone plus vancomycin in pediatric patients with complicated community acquired bacterial pneumonia. Pediatr. Infect. Dis. J. 2016, 35, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.M.; McTigue, S.M. Ceftaroline Plus Daptomycin for Refractory Methicillin-Resistant Staphylococcus aureus Bacteremia in a Child. J. Pediatr. Pharmacol. Ther. 2018, 23, 490–493. [Google Scholar] [CrossRef] [PubMed]
- Fowler, V.G., Jr.; Boucher, H.W.; Corey, G.R.; Abrutyn, E.; Karchmer, A.W.; Rupp, M.E.; Levine, D.P.; Chambers, H.F.; Tally, F.P.; Vigliani, G.A.; et al. Daptomycin versus standard therapy for bacteremia and endocarditis by Staphylococcus aureus. N. Eng. J. Med. 2006, 355, 653–665. [Google Scholar] [CrossRef]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the infectious diseases society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef]
- Ho, T.T.; Cadena, J.; Childs, L.M.; Gonzalez-Velez, M.; Lewis, J.S., 2nd. Methicillin resistant Staphylococcus aureus bacteremia and endocarditis treated with ceftaroline salvage therapy. J. Antimicrob. Chemother. 2012, 67, 1267–1270. [Google Scholar]
- Casapao, A.M.; Davis, S.L.; Barr, V.O.; Klinker, K.P.; Goff, D.A.; Barber, K.E.; Kaye, K.S.; Mynatt, R.P.; Molloy, L.M.; Pogue, J.M.; et al. Large retrospective evaluation of the effectiveness and safety of ceftaroline fosamil therapy. Antimicrob. Agents Chemother. 2014, 58, 2541–2546. [Google Scholar] [CrossRef]
- Vazquez, J.; Maggiore, C.R.; Cole, P.; Smith, A.; Jandourek, A.; Friedland, H.D. Ceftaroline fosamil for the treatment of Staphylococcus aureus bacteremia secondary to acute bacterial skin and skin structure infections or community acquired bacterial pneumonia. Inf. Dis. Clin. Pract. 2015, 23, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.C.; Aung, G.; Thomas, A.; Jahng, M.; Johns, S.; Fierer, J. The use of ceftaroline fosamil in methicillin resistant Staphylococcus aureus endocarditis and deep-seated MRSA infections: A restrospective case series of 10 patients. J. Infect. Chemother. 2013, 19, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Polenakovik, H.M.; Pleiman, C.M. Ceftaroline for methicillin resistant Staphylococcus aureus bacteremia: Case series and review of the literature. Int. J. Antimicrob. Agents 2013, 42, 450–455. [Google Scholar] [CrossRef] [PubMed]
- Sakoulas, G.; Moise, P.A.; Casapao, A.M.; Nonejuie, P.; Olson, J.; Okumura, C.Y.; Rybak, M.J.; Kullar, R.; Dhand, A.; Rose, W.E.; et al. Antimicrobial salvage therapy for persistent staphylococcal bacteremia using daptomycin plus ceftaroline. Clin. Ther. 2014, 10, 1317–1333. [Google Scholar] [CrossRef] [PubMed]
- Santos, P.D.; Davis, A.; Jandourek, A.; Smith, A.; Friedland, H.D. Ceftaroline fosamil and treatment of acute bacterial skin and skin structure infections: CAPTURE study experience. J. Chemother. 2013, 25, 341–346. [Google Scholar] [CrossRef]
- Sotgiu, G.; Aliberti, S.; Gramegna, A.; Mantero, M.; Di Pasquale, M.; Trogu, F.; Saderi, L.; Blasi, F. Efficacy and effectiveness of ceftaroline fosamil in patients with pneumonia: A systematic review and meta-analysis. Respir. Res. 2018, 19, 205. [Google Scholar] [CrossRef]
- Johnson, L.B.; Ramani, A.; Guervil, D. Use of ceftaroline fosamil in osteomyelitis: CAPTURE study experience. BMC Infect. Dis. 2019, 19, 183. [Google Scholar] [CrossRef]
- Destache, C.J.; Guervil, D.J.; Kaye, K.S. Ceftaroline fosamil for the treatment of Gram-positive endocarditis: CAPTURE study experience. Int. J. Antimicrob. Agents 2019. [Google Scholar] [CrossRef]
- Shafiq, I.; Bulman, Z.P.; Spitznogle, S.L.; Osorio, J.E.; Reilly, I.S.; Lesse, A.J.; Parameswaran, G.I.; Mergenhagen, K.A.; Tsuji, B.T. A combination of ceftaroline and daptomycin has synergistic and bacterial activity in vitro against daptomycin nonsusceptible methicillin-resistant Staphylococcus aureus (MRSA). Infect. Dis. 2017, 49, 410–416. [Google Scholar] [CrossRef]
- Rose, W.E.; Schulz, L.T.; Andes, D.; Striker, R.; Berti, A.D.; Hutson, P.R.; Shukla, S.K. Addition of ceftaroline to daptomycin after emergence of daptomycin-nonsusceptible Staphylococcus aureus during therapy improves antibacterial activity. Antimicrob. Agents Chemother. 2012, 56, 5296–5302. [Google Scholar] [CrossRef]
- Werth, B.J.; Sakoulas, G.; Rose, W.E.; Pogliano, J.; Tewhey, R.; Rybak, M.J. Ceftaroline increases membrane binding and enhances the activity of daptomycin against daptomycin-nonsusceptible vancomycin-intermediate Staphylococcus aureus in a pharmacokinetic/pharmacodynamic model. Antimicrob. Agents Chemother. 2013, 57, 66–73. [Google Scholar] [CrossRef] [PubMed]
- Cortes-Penfield, N.; Oliver, N.T.; Hunter, A.; Rodriguez-Barradas, M. Daptomycin and combination daptomycin-ceftaroline as salvage therapy for persistent methicillin-resistant Staphylococcus aureus bacteremia. Infect. Dis. 2018, 50, 643–647. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | MIC 50/90 of Ceftaroline for MRSA |
|---|---|
| Multicenter, randomized, observer-blinded, active-controlled in pediatrics [13] | MRSA = 0.5/1 mg/L |
| AWARE study in pediatrics [14] | MRSA = 0.5/1 mg/L |
| Criteria | Korczowski et al. [13] | Blumer et al. [16] |
|---|---|---|
| Total number of patients included, n | 159 | 5 |
| Patients with MRSA, n (%) | 18 (11%) | 1 |
| Patients who received antibiotics prior to ceftaroline | 9 | 1 |
| Duration of treatment with ceftaroline, median (range) | 3 days to 10 days | - |
| Clinical success of MRSA patients, n (%) | 16/18 (89%) | 1 |
| Safety outcome | 8% diarrhea 8% rash 7% vomiting 1% pruritis Serious adverse effects reported: 1 patient experienced hypersensitivity and another clostridium difficile colitis No death reported | Anemia, pruritus and vomiting |
| Criteria | Ho et al. [20] | Casapao et al. [21] | Vazquez et al. [22] | Lin et al. [23] | Polenakovitch et al. [24] | Sakoulas et al. [25] | Santos et al. [26] |
|---|---|---|---|---|---|---|---|
| Total number of patients who received ceftaroline, n | 6 | 630 | 48 (27 with ABSSSI and 21 with CABP) | 10 | 31 | 26 | 647 |
| Patients with MRSA, n (%) | 6 (100%) | 241 (38%) | 16 (59%) with ABSSSI and 16 (76%) with CABP | 10 (100%) | 31 (100%) | 20 (76%) | 191 (29%) |
| Patients who received antibiotics prior to ceftaroline | 6 | 422 | 14 with ABSSSI and 13 with SAB | 10 | 31 | 26 | 515 |
| Duration of treatment with ceftaroline, median (range) | Varies per case | 6 days | 5.8 days for ABSSSI and 7 days for CABP | Varies per case | 5 days | 16 days | 6 days |
| Number of patients that were treated with ceftaroline as monotherapy | 6 | 447 | 22 in ABSSSI and 10 in CABP | - | - | none | 114 |
| Clinical success of MRSA patients, n (%) | 5 (83%) | 426/484 (88%) | 8/16 (50%) with ABSSSI And 10/16 (63%) with CABP | 6 (60%) | 23 (74%) | 23 (88%) | 144/178 (81%) |
| Safety outcome | GI bleeding and death reported in one patient | 8% hospital mortality 0.9% diarrhea 0.6% vomiting 1.1% renal failure | - | Rash, eosinophilia, pruritis and clostridium difficile infection | Eosinophilic pneumonia, rash and diarrhea | - | - |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lounsbury, N.; Reeber, M.G.; Mina, G.; Chbib, C. A Mini-Review on Ceftaroline in Bacteremia Patients with Methicillin-Resistant Staphylococcus aureus (MRSA) Infections. Antibiotics 2019, 8, 30. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8010030
Lounsbury N, Reeber MG, Mina G, Chbib C. A Mini-Review on Ceftaroline in Bacteremia Patients with Methicillin-Resistant Staphylococcus aureus (MRSA) Infections. Antibiotics. 2019; 8(1):30. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8010030
Chicago/Turabian StyleLounsbury, Nicole, Mary G. Reeber, Georges Mina, and Christiane Chbib. 2019. "A Mini-Review on Ceftaroline in Bacteremia Patients with Methicillin-Resistant Staphylococcus aureus (MRSA) Infections" Antibiotics 8, no. 1: 30. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics8010030