Trends in Primary Antibiotic Resistance in H. pylori Strains Isolated in Italy between 2009 and 2019

 , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
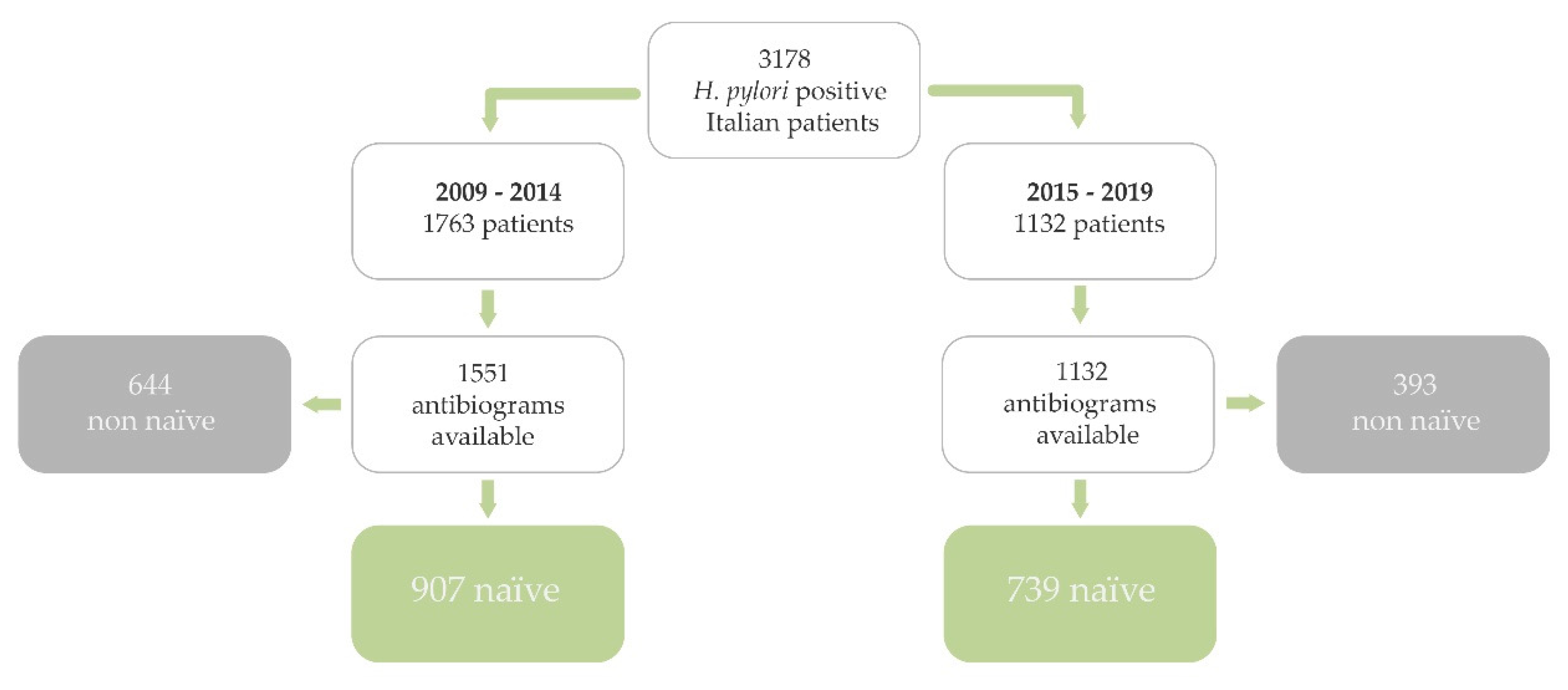
4.1. Patients
4.2. Endoscopy and H. pylori Assessment
4.3. Antibiotics Susceptibility Test for H. pylori
4.4. Chemotherapy for H. pylori
4.5. Potential Predictive Factors of Antibiotic Resistance
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- McColl, K.E. Clinical practice. Helicobacter pylori infection. N. Engl. J. Med. 2010, 362, 1597–1604. [Google Scholar] [CrossRef]
- Ailloud, F.; Didelot, X.; Woltemate, S.; Pfaffinger, G.; Overmann, J.; Bader, R.C.; Schulz, C.; Malfertheiner, P.; Suerbaum, S. Within-host evolution of Helicobacter pylori shaped by niche-specific adaptation, intragastric migrations and selective sweeps. Nat. Commun. 2019, 10, 2273. [Google Scholar] [CrossRef] [Green Version]
- De Francesco, V.; Zullo, A.; Hassan, C.; Giorgio, F.; Rosania, R.; Ierardi, E. Mechanisms of Helicobacter pylori antibiotic resistance: An updated appraisal. World J. Gastrointest. Pathophysiol. 2011, 2, 35–41. [Google Scholar] [CrossRef] [PubMed]
- De Francesco, V.; Zullo, A.; Giorgio, F.; Saracino, I.; Zaccaro, C.; Hassan, C.; Ierardi, E.; Di Leo, A.; Fiorini, G.; Castelli, V.; et al. Change of point mutations in Helicobacter pylori rRNA associated with clarithromycin resistance in Italy. J. Med. Microbiol. 2014, 63, 453–457. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Kim, N.; Kwon, Y.H.; Nam, R.H.; Kim, J.M.; Park, J.Y.; Lee, Y.S.; Lee, D.H. rdxA, frxA, and efflux pump in metronidazole-resistant Helicobacter pylori: Their relation to clinical outcomes. J. Gastroenterol. Hepatol. 2018, 33, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Rimbara, E.; Noguchi, N.; Kawai, T.; Sasatsu, M. Fluoroquinolone resistance in Helicobacter pylori: Role of mutations at position 87 and 91 of GyrA on the level of resistance and identification of a resistance conferring mutation in GyrB. Helicobacter 2012, 17, 36–42. [Google Scholar] [CrossRef]
- World Health Organization: List of Bacteria for Which New Antibiotics Are Urgently Needed. 2017. Available online: http://www.who.int/mediacentre/news/releases/2017/bacteria-antibiotics-needed/en/ (accessed on 18 November 2019).
- Fallone, C.A.; Chiba, N.; van Zanten, S.V.; Fischbach, L.; Gisbert, J.P.; Hunt, R.H.; Jones, N.L.; Render, C.; Leontiadis, G.I.; Moayyedi, P.; et al. The Toronto consensus for the treatment of Helicobacter pylori infection in adults. Gastroenterology 2016, 151, 51–69. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Megraud, F.; O’morain, C.A.; Gisbert, J.P.; Kuipers, E.J.; Axon, A.T.; Bazzoli, F.; Gasbarrini, A.; Atherton, J.; Graham, D.Y.; et al. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thung, I.; Aramin, H.; Vavinskaya, V.; Gupta, S.; Park, J.Y.; Crowe, S.E.; Valasek, M.A. Review article: The global emergence of Helicobacter pylori antibiotic resistance. Aliment. Pharmacol. Ther. 2016, 43, 514–533. [Google Scholar] [CrossRef] [Green Version]
- Malfertheiner, P.; Bazzoli, F.; Delchier, J.C.; Celiñski, K.; Giguère, M.; Rivière, M.; Mégraud, F.; Pylera Study Group. Helicobacter pylori eradication with a capsule containing bismuth subcitrate potassium, metronidazole, and tetracycline given with omeprazole versus clarithromycin-based triple therapy: A randomised, open-label, non-inferiority, phase 3 trial. Lancet 2011, 377, 905–913. [Google Scholar] [CrossRef]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG clinical guideline: Treatment of Helicobacter pylori infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef] [PubMed]
- Megraud, F.; Coenen, S.; Versporten, A.; Kist, M.; Lopez-Brea, M.; Hirschl, A.M.; Andersen, L.P.; Goossens, H.; Glupczynski, Y. Helicobacter pylori resistance to antibiotics in Europe and its relationship to antibiotic consumption. Gut 2013, 62, 34–42. [Google Scholar] [CrossRef]
- Dang, B.N.; Graham, D.Y. Helicobacter pylori infection and antibiotic resistance: A WHO high priority? Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 383–384. [Google Scholar] [CrossRef] [PubMed]
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of antibiotic resistance in helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gatta, L.; Scarpignato, C.; Fiorini, G.; Belsey, J.; Saracino, I.M.; Ricci, C.; Vaira, D. Impact of primary antibiotic resistance on the effectiveness of sequential therapy for Helicobacter pylori infection: Lessons from a 5-year study on a large number of strains. Aliment. Pharmacol. Ther. 2018, 47, 1261–1269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zagari, R.M.; Romano, M.; Ojetti, V.; Stockbrugger, R.; Gullini, S.; Annibale, B.; Farinati, F.; Ierardi, E.; Maconi, G.; Rugge, M.; et al. Guidelines for the management of Helicobacter pylori infection in Italy: The III Working Group Consensus Report 2015. Dig. Liver Dis. 2015, 47, 903–912. [Google Scholar] [CrossRef]
- Vakil, N.; Megraud, F. Eradication therapy for Helicobacter pylori. Gastroenterology 2007, 133, 985–1001. [Google Scholar] [CrossRef]
- Zullo, A.; Perna, F.; Hassan, C.; Ricci, C.; Saracino, I.; Morini, S.; Vaira, D. Primary antibiotic resistance in Helicobacter pylori strains isolated in northern and central Italy. Aliment. Pharmacol. Ther. 2007, 25, 1429–1434. [Google Scholar] [CrossRef]
- Fiorini, G.; Zullo, A.; Saracino, I.M.; Gatta, L.; Pavoni, M.; Vaira, D. Pylera and sequential therapy for first-line Helicobacter pylori eradication: A culture-based study in real clinical practice. Eur. J. Gastroenterol. Hepatol. 2018, 30, 621–625. [Google Scholar] [CrossRef]
- Löfmark, S.; Edlund, C.; Nord, C.E. Carl Erik Nord. Metronidazole is still the drug of choice for treatment of anaerobic infections. Clin. Infect. Dis. 2010, 50, S16–S23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mcquiston Haslund, J.; Rosborg Dinesen, M.; Sternhagen Nielsen, A.B.; Llor, C.; Bjerrum, L. Different recommendations for empiric first-choice antibiotic treatment of uncomplicated urinary tract infections in Europe. Scand. J. Prim. Health Care 2013, 31, 235–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, Z.; Han, F.; Meng, F.; Tu, M.; Yang, N.; Zhang, J. The association of age and antibiotic resistance of Helicobacter pylori: A Study in Jiaxing City, Zhejiang Province, China. Medicine 2016, 95, e2831. [Google Scholar] [CrossRef] [PubMed]
- Camargo, M.C.; Piazuelo, M.B.; Mera, R.M.; Fontham, E.T.; Delgado, A.G.; Yepez, M.C.; Ceron, C.; Bravo, L.E.; Bravo, J.C.; Correa, P. Effect of smoking on failure of H. pylori therapy and gastric histology in a high gastric cancer risk area of Colombia. Acta Gastroenterol. Latinoam. 2007, 37, 238–245. [Google Scholar] [PubMed]
- Suzuki, T.; Matsuo, K.; Ito, H.; Sawaki, A.; Hirose, K.; Wakai, K.; Sato, S.; Nakamura, T.; Yamao, K.; Ueda, R.; et al. Smoking increases the treatment failure for Helicobacter pylori eradication. Am. J. Med. 2006, 119, 217–224. [Google Scholar] [CrossRef]
- ICH Steering Committee. Principles for clinical evaluation of new antihypertensive drugs: International Conference on Harmonisation of Technical Requirements for Registration of Pharmaceuticals for Human Use. Int. Dig. Health Legis 1997, 48, 231–234. [Google Scholar]
- World Medical Association. WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Available online: http://www.wma.net/en/30publications/10policies/b3 (accessed on 19 November 2019).
- Newcombe, R.G.; Altman, D.G. Proportion and Their Differences. In Statistics with Confidences, 2nd ed.; Altman, D.G., Machin, D., Trevor, N.B., Gardner, M.J., Eds.; BMJ Books: London, UK, 2000. [Google Scholar]
- Clinical Breakpoints-Breakpoints and Guidance. Available online: http://www.eucast.org/clinical_breakpoints (accessed on 18 November 2019).



{kind=link}
{kind=link}
| (a) | ||||||
|---|---|---|---|---|---|---|
| Population Features | 2009–2014 | % | 95% CI | 2015–2019 | % | 95% CI |
| Patients | 907 | 739 | ||||
| Male | 358 | 39.5 | 36.3–42.7 | 288 | 39.0 | 35.4–42.6 |
| Female | 549 | 60.0 | 57.3–63.7 | 451 | 61.0 | 57.4–64.6 |
| Age mean | 51.5 | 53 | ||||
| BMI mean | 24.3 | 25 | ||||
| Smokers | 205 | 22.6 | 19.9–25.5 | 158 | 21.4 | 18.5–24.5 |
| Alcohol | 135 | 14.9 | 12.6–17.4 | 99 | 13.4 | 11.0–16.1 |
| Cardioaspirin | 68 | 7.5 | 5.9–9.4 | 56 | 7.6 | 5.8–9.7 |
| Familiarity for gastric cancer | 118 | 13.0 | 10.9–15.4 | 89 | 12.0 | 9.8–14.6 |
| Compulsory education | 362 | 39.0 | 36.7–43.2 | 276 | 37.3 | 33.8–40.9 |
| High school | 362 | 39.9 | 36.7–43.2 | 311 | 42.1 | 38.5–45.7 |
| Graduation | 183 | 20.2 | 17.6–22.9 | 152 | 20.6 | 17.7–23.7 |
| Chief town | 397 | 43.8 | 40.5–47.1 | 284 | 38.4 | 34.9–42.0 |
| Emilia Romagna | 737 | 81.3 | 78.6–83.7 | 593 | 80.2 | 77.2–83.1 |
| (b) | |||
|---|---|---|---|
| Population Features | TOT | % | 95% CI |
| Patients | 1646 | ||
| Male | 646 | 39.2 | 36.9–41.7 |
| Female | 1000 | 60.8 | 58.3–63.1 |
| Age mean | 52.3 | ||
| BMI mean | 24.6 | ||
| Smokers | 363 | 22.1 | 20.1–24.1 |
| Alcohol | 234 | 14.2 | 12.6–16.0 |
| Cardioaspirin | 124 | 7.5 | 6.3–8.9 |
| Familiarity for gastric cancer | 207 | 12.6 | 11.0–14.3 |
| Compulsory education | 638 | 38.8 | 36.4–41.2 |
| High school | 673 | 40.9 | 38.5–43.3 |
| Graduation | 335 | 20.4 | 18.4–22.4 |
| Chief town | 681 | 41.4 | 39.0–43.8 |
| Emilia Romagna | 1330 | 80.8 | 78.8–82.7 |
| UGIE Reports (2009–2019) | No. | % | 95% CI |
|---|---|---|---|
| NUD | 1413 | 85.8 | 84.0–87.4 |
| PUD | 204 | 12.3 | 10.8–14.0 |
| MALT lymphoma | 20 | 1.2 | 0.7–1.8 |
| Gastric cancer | 9 | 0.5 | 0.2–1.0 |
| 907 Naïve | No. | % | 95% CI |
|---|---|---|---|
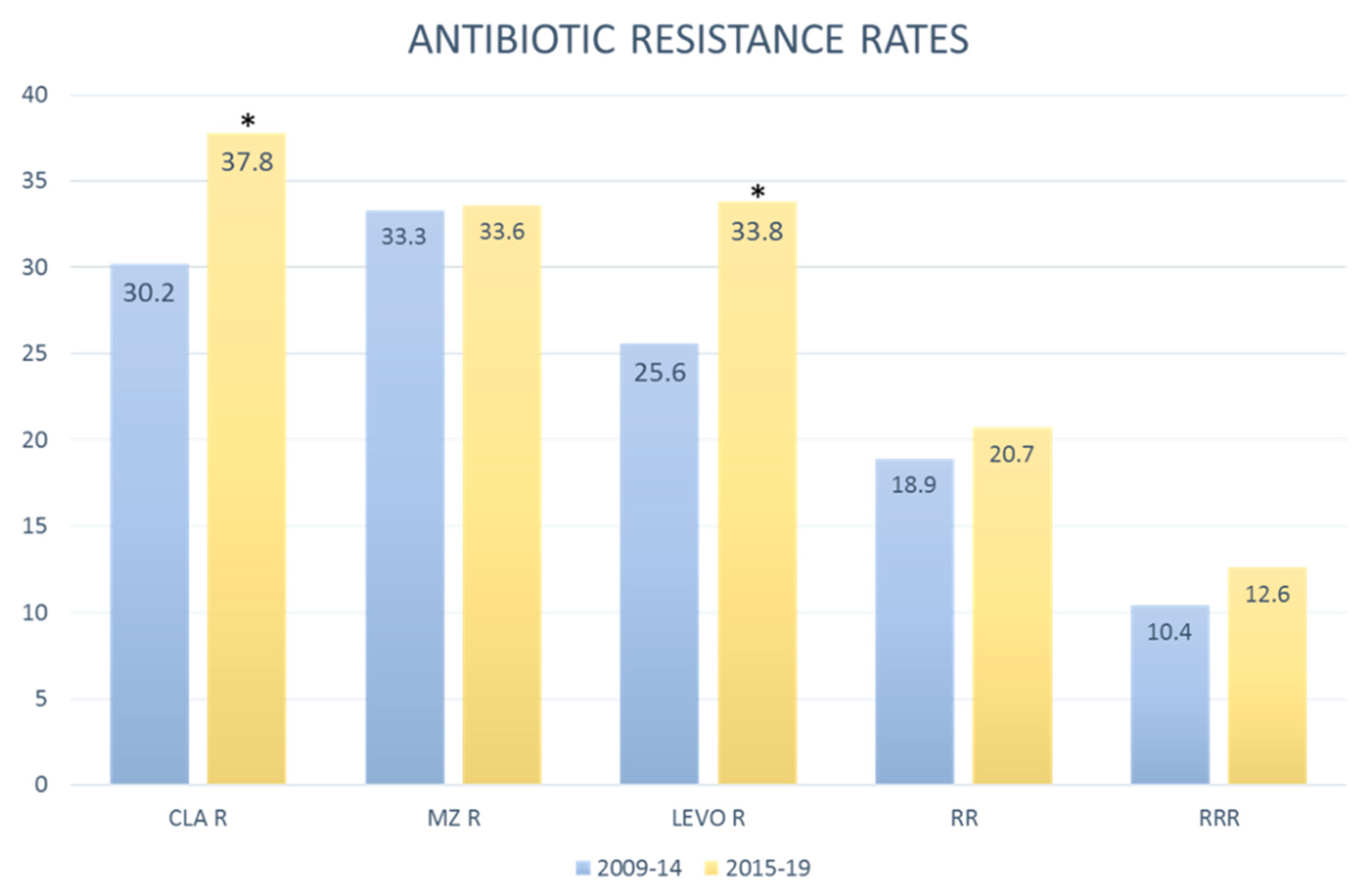
| ClaR, MzR, LevoR | 94 | 10.4 | 8.5–12.5 |
| ClaR, MzR, LevoS | 77 | 8.5 | 6.8–10.5 |
| ClaR, MzS, LevoR | 31 | 3.4 | 2.3–4.8 |
| ClaR, MzS, LevoS | 72 | 7.9 | 6.3–9.9 |
| ClaS, MzR, LevoR | 46 | 5.1 | 3.7–6.7 |
| ClaS, MzR, LevoS | 85 | 9.4 | 7.6–11.5 |
| ClaS, MzS, LevoR | 61 | 6.7 | 52.0–8.6 |
| ClaS, MzS, LevoS | 441 | 48.6 | 45.3–51.9 |
| Cla R tot | 274 | 30.2 | 27.2–33.3 |
| Cla S tot | 633 | 69.8 | 66.7–72.8 |
| Mz R tot | 302 | 33.3 | 30.2–36.5 |
| Mz S tot | 605 | 66.7 | 63.5–69.8 |
| Levo R tot | 232 | 25.6 | 22.8–28.5 |
| Levo S tot | 675 | 74.4 | 71.5–77.2 |
| ClaR, MzR tot | 171 | 18.9 | 16.4–21.6 |
| 739 Naive | No. | % | 95% CI |
|---|---|---|---|
| ClaR, MzR, LevoR | 93 | 12.6 | 10.3–15.2 |
| ClaR, MzR, LevoS | 60 | 8.1 | 6.3–10.3 |
| ClaR, MzS, LevoR | 46 | 6.2 | 4.6–8.2 |
| ClaR, MzS, LevoS | 80 | 10.8 | 8.7–13.3 |
| ClaS, MzR, LevoR | 46 | 6.2 | 4.6–8.2 |
| ClaS, MzR, LevoS | 49 | 6.6 | 4.9–8.7 |
| ClaS, MzS, LevoR | 65 | 8.8 | 6.9–11.1 |
| ClaS, MzS, LevoS | 300 | 40.6 | 37.0–44.2 |
| Cla R tot | 279 | 37.8 | 34.2–41.4 |
| Cla S tot | 460 | 62.2 | 58.6–65.8 |
| Mz R tot | 248 | 33.6 | 30.2–37.1 |
| Mz S tot | 491 | 66.4 | 62.9–69.8 |
| Levo R tot | 250 | 33.8 | 30.4–37.4 |
| Levo S tot | 489 | 66.2 | 62.6–69.6 |
| ClaR, MzR tot | 153 | 20.7 | 17.8–23.8 |
| (a) | |||
|---|---|---|---|
| Variables | Patterns of Resistance | OR | p Value |
| 2015–2019 | Cla R | 1.4 | 0.001 * |
| Mz R | 1.01 | 0.910 | |
| Levo R | 1.48 | 0.000 * | |
| ClaR, MzR | 1.23 | 0.348 | |
| ClaR, MzR, LevoR | 1.24 | 0.158 | |
| Sex female | Cla R | 1.22 | 0.069 |
| Mz R | 1.78 | 0.000 * | |
| Levo R | 0.99 | 0.927 | |
| ClaR, MzR | 1.47 | 0.003 * | |
| ClaR, MzR, LevoR | 1.18 | 0.309 | |
| Age > 50 years | Cla R | 0.79 | 0.027 ** |
| Mz R | 1 | 0.7054 | |
| Levo R | 1.38 | 0.003 * | |
| ClaR, MzR | 1 | 0.8291 | |
| ClaR, MzR, LevoR | 1.1 | 0.003 * | |
| BMI > 25 | Cla R | 0.9 | 0.367 |
| Mz R | 0.9 | 0.280 | |
| Levo R | 1.06 | 0.608 | |
| ClaR, MzR | 0.9 | 0.113 | |
| ClaR, MzR, LevoR | 0.88 | 0.401 | |
| Smokers | Cla R | 1.1 | 0.447 |
| Mz R | 1.87 | 0.000 * | |
| Levo R | 1.01 | 0.927 | |
| ClaR, MzR | 0.97 | 0.828 | |
| ClaR, MzR, LevoR | 0.96 | 0.816 | |
| (b) | |||
|---|---|---|---|
| Variables | Patterns of Resistance | OR | p Value |
| Daily alcohol consumption | Cla R | 1.01 | 0.954 |
| Mz R | 0.84 | 0.282 | |
| Levo R | 1.06 | 0.701 | |
| ClaR, MzR | 0.94 | 0.715 | |
| ClaR, MzR, LevoR | 1.02 | 0.725 | |
| Familiarity for gastric cancer | Cla R | 0.94 | 0.689 |
| Mz R | 0.95 | 0.733 | |
| Levo R | 0.93 | 0.699 | |
| ClaR, MzR | 0.94 | 0.744 | |
| ClaR, MzR, LevoR | 0.87 | 0.556 | |
| Level of education (till middle school) | Cla R | 0.86 | 0.153 |
| Mz R | 0.99 | 0.899 | |
| Levo R | 1.04 | 0.724 | |
| ClaR, MzR | 0.96 | 0.742 | |
| ClaR, MzR, LevoR | 1.04 | 0.809 | |
| Residence (main city) | Cla R | 0.92 | 0.409 |
| Mz R | 1 | 0.637 | |
| Levo R | 1.08 | 0.469 | |
| ClaR, MzR | 0.89 | 0.375 | |
| ClaR, MzR, LevoR | 1.04 | 0.797 | |
| PUD | Cla R | 0.8 | 0.070 |
| Mz R | 0.77 | 0.120 | |
| Levo R | 0.85 | 0.350 | |
| ClaR, MzR | 0.74 | 0.157 | |
| ClaR, MzR, LevoR | 0.78 | 0.380 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saracino, I.M.; Fiorini, G.; Zullo, A.; Pavoni, M.; Saccomanno, L.; Vaira, D. Trends in Primary Antibiotic Resistance in H. pylori Strains Isolated in Italy between 2009 and 2019. Antibiotics 2020, 9, 26. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9010026
Saracino IM, Fiorini G, Zullo A, Pavoni M, Saccomanno L, Vaira D. Trends in Primary Antibiotic Resistance in H. pylori Strains Isolated in Italy between 2009 and 2019. Antibiotics. 2020; 9(1):26. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9010026
Chicago/Turabian StyleSaracino, Ilaria Maria, Giulia Fiorini, Angelo Zullo, Matteo Pavoni, Laura Saccomanno, and Dino Vaira. 2020. "Trends in Primary Antibiotic Resistance in H. pylori Strains Isolated in Italy between 2009 and 2019" Antibiotics 9, no. 1: 26. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9010026