A Qualitative Study of Pregnant Women’s Perspectives on Antibiotic Use for Mom and Child: Implications for Developing Tailored Health Education Interventions

 , , ,
, , , 
Abstract
:1. Introduction
2. Results
2.1. Participant Demographics
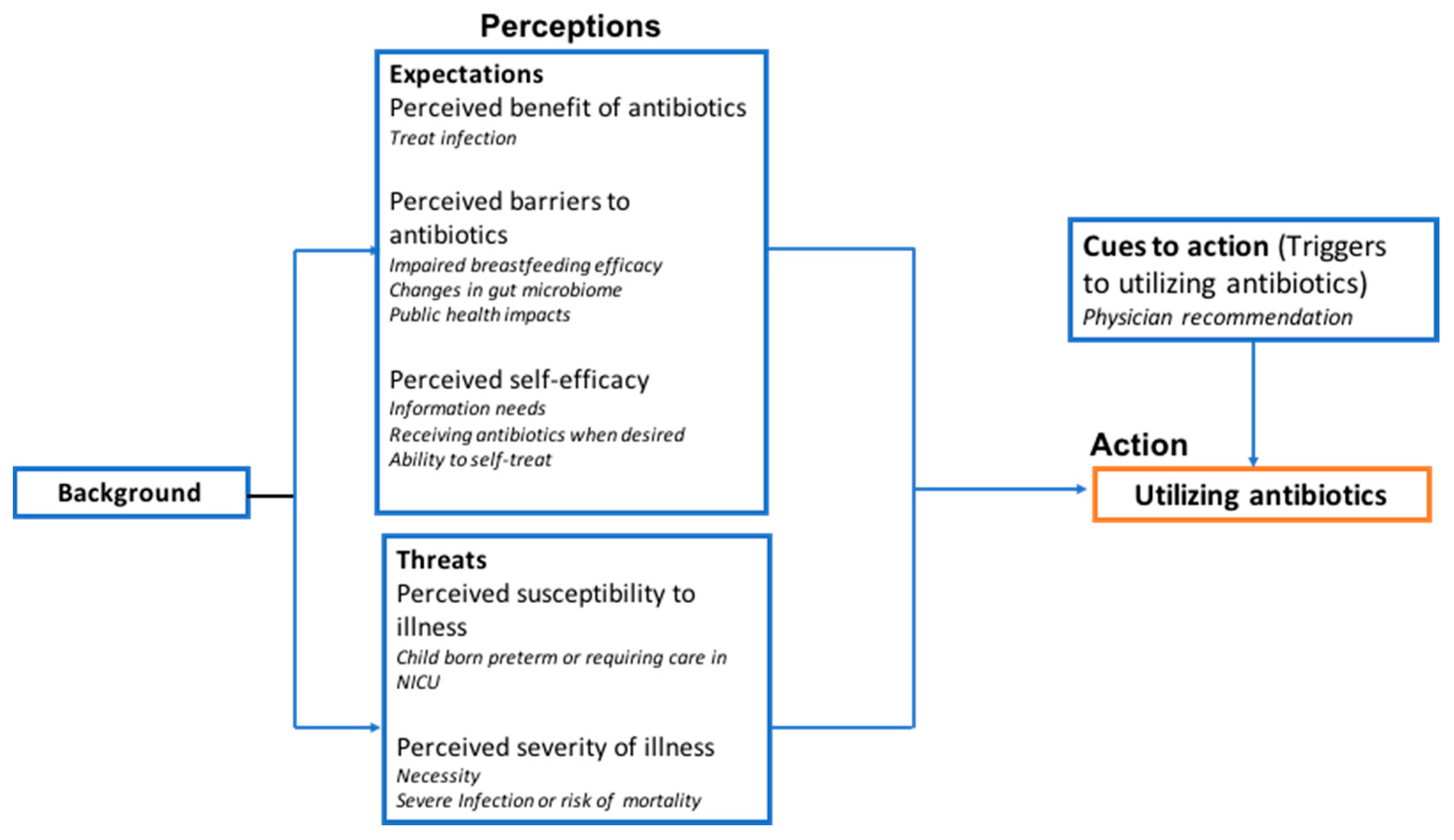
2.2. Factors Involved in Perceptions of Antibiotics and Decision-Making: The Health Belief Model
2.2.1. Expectations of Antibiotic Use: Perceived Benefits of Taking Antibiotics
“When I think of antibiotics, I think of like a way to get better from being sick.”—PRG005
“If you’re sick and you’re getting treated, yeah, it’s awesome, if you’ve got a reason to take them, which you know she’s like, “Okay, you’re not getting any better, it’s not viral, try the antibiotics and see if it’ll help.”—PRG018
“In general, I’m not a big fan of antibiotics and I try not to take them.”—PRG002
2.2.2. Expectations of Antibiotic Use: Perceived Barriers of Taking Antibiotics
“It could in the same way like with thrush in the mouth… I think in that sense, it could impact the breastfeeding goals.”—PRG016
“The way that antibiotics works is it kills bad—the bad bacteria, but it also kills the good bacteria as well. I think, it can impact the ability of—for the breastmilk to actually give the nutrients that it needs to the child.”—PRG013
“Antibiotics mess up your gut health, and that gives you like other issues and other ailments and other things. It’s just like a domino effect.”—PRG020
“I definitely want to know how [antibiotics] affect a baby’s health or digestion cuz I’m sure it’s not just like in the moment. It’s gonna show up later on.”—PRG007
“I just feel like they just prescribe something, because they learned how to do that. So, I think they’re overutilized. I think if you’re sick, instead of getting to the root of the problem, they’ll just be like, ‘Oh, take this antibiotic and cure that…’ and not cure the actual root of the issue.”—PRG020
“Well, and there’s all the resistance issues and everything which is why … I’m like, I’m gonna do my part to help with that by not taking it unless I absolutely need it.”—PRG018
2.2.3. Expectations of Antibiotic Use: Perceived Self-Efficacy Surrounding Antibiotic Use
“As long as I know what’s going on in my child’s body or my body, then I don’t think that I’d have an issue with anything. I want to know how it’s affecting me and know exactly what that antibiotic is going to do for me and my child. So as long as I know that information and I have both the negatives and positives, I don’t see why not.”—PRG005
“[I would like] some honest information about the benefits and risks, pros and cons, both, to be able to make it an informative decision.”—PRG011
“Because I think a lot of times moms are just like, we need something to get the baby to feel better.”—PRG004
“When your child is crying and in pain, you just want to do something.”—PRG002
“I’ll take antibiotics but if I can take like a ton of vitamin C and like get a lot of sleep, I would rather do that than affecting all the bio stuff in me.”—PRG007
“If it is preventive or unnecessary, then let me try to do—something different because there are other ways that you can heal the body other than antibiotics.”—PRG013
“I don’t think I would give my baby antibiotics if she’s sick or not because breastfeeding; you get all the nutrients you need, so you won’t get sick, so I probably won’t even like, “No. You can keep your medicine. I have got this.”—PRG006
2.2.4. Threats of Illness: Perceived Susceptibility of Illness
“I think a lot of my perspectives and my crazy crunchy remedies would change if I had a preemie. I’d be like, “Get me to the nearest hospital. Give me all the drugs.” So, I think it’s all a lot of your situation.”—PRG020
2.2.5. Threats of Illness: Perceived Severity of Illness
“I would want to know that there was no other way and that antibiotics are necessary for whatever issue.”—PRG009
“If there was some kind of fatal infection that needed antibiotics. There are times when a medical intervention is necessary, and the antibiotics are helpful.”—PRG013
2.2.6. Cues to Action
“I usually trust doctors that they know what they’re doing. That they’ve gone to medical school and I haven’t—and if they would consider [antibiotics] to be necessary.”—PRG001
“You know, like if your doctor says you need this, [you’re] gonna just do it. I wouldn’t ask any questions either, because it’s like your baby could die in there.”—PRG020
2.3. Preferences for Antibiotic Counseling
“I feel as soon as the mother knows she’s pregnant, they should start giving information about the different medicines.”—PRG006
“Taking antibiotic information and emailing it out would definitely have a greater impact on my life.”—PRG014
“Summary bullets points, these are the highlights.”—PRG018
“Probably electronically, like email, and consolidate like a brief of a research report.”—PRG014
3. Discussion
4. Materials and Methods
4.1. Design and Aims
4.2. Sample
4.3. Recruitment
4.4. Data Collection
4.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Andrade, S.E.; Gurwitz, J.H.; Davis, R.L.; Chan, K.A.; Finkelstein, J.A.; Fortman, K.; McPhillips, H.; Raebel, M.A.; Roblin, D.W.; Smith, D.H.; et al. Prescription drug use in pregnancy. Am. J. Obstet. Gynecol. 2004, 191, 398–407. [Google Scholar] [CrossRef] [PubMed]
- Chai, G.; Governale, L.; McMahon, A.W.; Trinidad, J.P.; Staffa, J.; Murphy, D. Trends of Outpatient Prescription Drug Utilization in US Children, 2002–2010. Pediatrics 2012, 130, 23–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, F.; Oraichi, D.; Bérard, A. Prevalence and predictors of anti-infective use during pregnancy. Pharmacoepidemiol. Drug Saf. 2010, 19, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Stokholm, J.; Schjørring, S.; Pedersen, L.; Bischoff, A.L.; Følsgaard, N.; Carson, C.G.; Chawes, B.L.K.; Bønnelykke, K.; Mølgaard, A.; Krogfelt, K.A.; et al. Prevalence and Predictors of Antibiotic Administration during Pregnancy and Birth. PLoS ONE 2013, 8, e82932. [Google Scholar] [CrossRef] [PubMed]
- De Jonge, L.; Bos, H.J.; Van Langen, I.M.; de Jong-van den Berg, L.T.W.; Bakker, M. Antibiotics prescribed before, during and after pregnancy in the Netherlands: A drug utilization study. Pharmacoepidemiol. Drug Saf. 2013, 23, 60–68. [Google Scholar] [CrossRef]
- Heikkilä, A.M. Antibiotics in Pregnancy A Prospective Cohort Study on the Policy of Antibiotic Prescription. Ann. Med. 1993, 25, 467–471. [Google Scholar] [CrossRef]
- Nahum, G.G.; Uhl, K.; Kennedy, D.L. Antibiotic Use in Pregnancy and Lactation. Obstet. Gynecol. 2006, 107, 1120–1138. [Google Scholar] [CrossRef]
- Content and Format of Labeling for Human Prescription Drug and Biological Products. Requirements for Pregnancy and Lactation Labeling. Final Rule; Food and Drug Administration (FDA), Department of Health and Human Services (HHS): Washington, DC, USA, 2014.
- Kuperman, A.A.; Koren, O. Antibiotic use during pregnancy: How bad is it? BMC Med. 2016, 14, 91. [Google Scholar] [CrossRef] [Green Version]
- Mathew, J.L. Effect of maternal antibiotics on breast feeding infants. Postgrad. Med. J. 2004, 80, 196–200. [Google Scholar] [CrossRef]
- Mueller, N.T.; Whyatt, R.; Hoepner, L.; Oberfield, S.; Dominguez-Bello, M.G.; Widen, E.M.; Hassoun, A.; Perera, F.; Rundle, A. Prenatal exposure to antibiotics, cesarean section and risk of childhood obesity. Int. J. Obes. 2014, 39, 665–670. [Google Scholar] [CrossRef] [Green Version]
- Lapin, B.; Piorkowski, J.; Ownby, D.; Freels, S.; Chavez, N.; Hernandez, E.; Wagner-Cassanova, C.; Pelzel, D.; Vergara, C.; Persky, V. Relationship between prenatal antibiotic use and asthma in at-risk children. Ann. Allergy Asthma Immunol. 2015, 114, 203–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stensballe, L.G.; Simonsen, J.; Jensen, S.M.; Bønnelykke, K.; Bisgaard, H. Use of Antibiotics during Pregnancy Increases the Risk of Asthma in Early Childhood. J. Pediatrics 2013, 162, 832–838.e3. [Google Scholar] [CrossRef] [PubMed]
- Butler, C.C.; Kinnersley, P.; Prout, H.; Rollnick, S.; Edwards, A.; Elwyn, G. Antibiotics and shared decision-making in primary care. J. Antimicrob. Chemother. 2001, 48, 435–440. [Google Scholar] [CrossRef] [Green Version]
- McDonald, K.; Amir, L.H.; Davey, M.-A. Maternal bodies and medicines: A commentary on risk and decision-making of pregnant and breastfeeding women and health professionals. BMC Public Health 2011, 11 (Suppl. S5), 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glanz, K.; Rimer, B.K.; Viswanath, K. Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A Decade Later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoramabadi, M.; Dolatian, M.; Hajian, S.; Zamanian, M.; Taheripanah, R.; Sheikhan, Z.; Mahmoodi, Z.; Seyedi-Moghadam, A. Effects of Education Based on Health Belief Model on Dietary Behaviors of Iranian Pregnant Women. Glob. J. Health Sci. 2015, 8, 230–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- French, B.N.; Kurczynski, T.W.; Weaver, M.T.; Pituch, M.J. Evaluation of the Health Belief Model and Decision Making Regarding Amniocentesis in Women of Advanced Maternal Age. Health Educ. Q. 1992, 19, 177–186. [Google Scholar] [CrossRef]
- Loke, A.Y.; Davies, L.; Li, S.-F. Factors influencing the decision that women make on their mode of delivery: The Health Belief Model. BMC Health Serv. Res. 2015, 15, 274. [Google Scholar] [CrossRef] [Green Version]
- Heid, C.; Knobloch, M.J.; Schulz, L.T.; Safdar, N. Use of the Health Belief Model to Study Patient Perceptions of Antimicrobial Stewardship in the Acute Care Setting. Infect. Control. Hosp. Epidemiol. 2016, 37, 576–582. [Google Scholar] [CrossRef] [Green Version]
- Ancillotti, M.; Eriksson, S.; Veldwijk, J.; Fahlquist, J.N.; Andersson, D.I.; Godskesen, T. Public awareness and individual responsibility needed for judicious use of antibiotics: A qualitative study of public beliefs and perceptions. BMC Public Health 2018, 18, 1153. [Google Scholar] [CrossRef]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- Nordeng, H.; Ystrøm, E.; Einarson, A. Perception of risk regarding the use of medications and other exposures during pregnancy. Eur. J. Clin. Pharmacol. 2009, 66, 207–214. [Google Scholar] [CrossRef]
- Sanz, E.J.; Gómez-López, T.; Martínez-Quintas, M.J. Perception of teratogenic risk of common medicines. Eur. J. Obstet. Gynecol. Reprod. Biol. 2001, 95, 127–131. [Google Scholar] [CrossRef]
- Lynch, M.; Squiers, L.; Kosa, K.M.; Dolina, S.; Read, J.G.; Broussard, C.S.; Frey, M.T.; Polen, K.N.; Lind, J.N.; Gilboa, S.M.; et al. Making Decisions About Medication Use During Pregnancy: Implications for Communication Strategies. Matern. Child Health J. 2017, 22, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Attanasio, L.B.; Kozhimannil, K.B.; Kjerulff, K.H. Factors influencing women’s perceptions of shared decision making during labor and delivery: Results from a large-scale cohort study of first childbirth. Patient Educ. Couns. 2018, 101, 1130–1136. [Google Scholar] [CrossRef]
- Santucci, A.K.; Gold, M.A.; Akers, A.Y.; Borrero, S.; Schwarz, E.B. Women’s perspectives on counseling about risks for medication-induced birth defects. Birth Defects Res. Part A Clin. Mol. Teratol. 2009, 88, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Adam, M.P.; Polifka, J.E.; Friedman, J. Evolving knowledge of the teratogenicity of medications in human pregnancy. Am. J. Med. Genet. Part C Semin. Med. Genet. 2011, 157, 175–182. [Google Scholar] [CrossRef]
- Kilfoyle, K.A.; Vitko, M.; O’Conor, R.; Bailey, S.C. Health Literacy and Women’s Reproductive Health: A Systematic Review. J. Women’s Health 2016, 25, 1237–1255. [Google Scholar] [CrossRef] [PubMed]
- Patnode, C.D.; Henderson, J.T.; Thompson, J.H.; Senger, C.A.; Fortmann, S.P.; Whitlock, E.P. Behavioral Counseling and Pharmacotherapy Interventions for Tobacco Cessation in Adults, Including Pregnant Women: A Review of Reviews for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2015, 163, 608–621. [Google Scholar] [CrossRef] [Green Version]
- Bertz, F.; Brekke, H.K.; Ellegård, L.; Rasmussen, K.M.; Wennergren, M.; Winkvist, A.; Ellegård, L. Diet and exercise weight-loss trial in lactating overweight and obese women. Am. J. Clin. Nutr. 2012, 96, 698–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Wulp, N.Y.; Hoving, C.; Eijmael, K.; Candel, M.J.J.M.; Van Dalen, W.; De Vries, H.; Johnson, N.; Haug, S. Reducing Alcohol Use During Pregnancy Via Health Counseling by Midwives and Internet-Based Computer-Tailored Feedback: A Cluster Randomized Trial. J. Med. Internet Res. 2014, 16, e274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García, D.; Vassena, R.; Prat, A.; Vernaeve, V. Increasing fertility knowledge and awareness by tailored education: A randomized controlled trial. Reprod. Biomed. Online 2016, 32, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Bookstaver, P.B.; Bland, C.M.; Griffin, B.; Stover, K.R.; Eiland, L.S.; McLaughlin, M. A Review of Antibiotic Use in Pregnancy. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2015, 35, 1052–1062. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.A.; Cragan, J.D.; Goldenberg, R.L.; Rasmussen, S.A.; Schulkin, J. Obstetrician—Gynaecologist knowledge of and access to information about the risks of medication use during pregnancy. J. Matern. Neonatal Med. 2010, 23, 1143–1150. [Google Scholar] [CrossRef] [PubMed]
- Heitmann, K.; Schjøtt, J. SafeMotherMedicine: Aiming to Increase Women’s Empowerment in Use of Medications during Pregnancy and Breastfeeding. Matern. Child Health J. 2020, 24, 531–536. [Google Scholar] [CrossRef] [Green Version]
- Dugas, M.; Shorten, A.; Dubé, E.; Wassef, M.; Bujold, E.; Chaillet, N. Decision aid tools to support women’s decision making in pregnancy and birth: A systematic review and meta-analysis. Soc. Sci. Med. 2012, 74, 1968–1978. [Google Scholar] [CrossRef]
- Lynch, M.M.; Amoozegar, J.B.; McClure, E.M.; Squiers, L.B.; Broussard, C.S.; Lind, J.N.; Polen, K.N.; Frey, M.T.; Gilboa, S.M.; Biermann, J. Improving Safe Use of Medications During Pregnancy: The Roles of Patients, Physicians, and Pharmacists. Qual. Health Res. 2017, 27, 2071–2080. [Google Scholar] [CrossRef]
- Bonari, L.; Koren, G.; Einarson, T.R.; Jasper, J.D.; Taddio, A.; Einarson, A. Use of antidepressants by pregnant women: Evaluation of perception of risk, efficacy of evidence based counseling and determinants of decision making. Arch. Women’s Ment. Health 2005, 8, 214–220. [Google Scholar] [CrossRef]
- Maher, J.; Saugeres, L. To be or not to be a mother? J. Sociol. 2007, 43, 5–21. [Google Scholar] [CrossRef]
- Nygaard, L.; Rossen, C.B.; Buus, N. Balancing Risk: A Grounded Theory Study of Pregnant Women’s Decisions to (Dis)Continue Antidepressant Therapy. Issues Ment. Health Nurs. 2015, 36, 485–492. [Google Scholar] [CrossRef]
- Sinclair, M.; Lagan, B.; Dolk, H.; McCullough, J.E.M. An assessment of pregnant women’s knowledge and use of the Internet for medication safety information and purchase. J. Adv. Nurs. 2017, 74, 137–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denton, L.; Creeley, C.E.; Stavola, B.; Hall, K.; Foltz, B.D. An analysis of online pregnancy message boards: Mother-to-mother advice on medication use. Women Birth 2020, 33, e48–e58. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.L.; Lind, J.N.; Humphrey, J.R.; Friedman, J.M.; Honein, M.A.; Tassinari, M.S.; Moore, C.A.; Mathis, L.L.; Broussard, C.S. Safe lists for medications in pregnancy: Inadequate evidence base and inconsistent guidance from Web-based information, 2011. Pharmacoepidemiol. Drug Saf. 2013, 22, 324–328. [Google Scholar] [CrossRef] [PubMed]
- QSR International Pty Ltd. NVivo. 2020. Available online: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home (accessed on 15 March 2020).
- Ingram, J.; Cabral, C.; Hay, A.D.; Lucas, P.J.; Horwood, J. Parents’ information needs, self-efficacy and influences on consulting for childhood respiratory tract infections: A qualitative study. BMC Fam. Pract. 2013, 14, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemas, D.J.; Mack, J.A.; Schoch, J.J.; Cacho, N.; Plasencia, E.; Rhoton-Vlasak, A.S.; Neu, J.; Thompson, L.; Francois, M.; Patel, K.; et al. Postnatal pediatric systemic antibiotic episodes during the first three years of life are not associated with mode of delivery. PLoS ONE 2020, 15, e0229861. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristic | Frequency (n) | Percent (%) |
|---|---|---|
| Maternal age | ||
| 20–30 years | 8 | 44 |
| 31–40 years | 10 | 56 |
| Previous children | ||
| Yes | 7 | 39 |
| No | 11 | 61 |
| Highest level of education | ||
| Professional/Graduate degree | 9 | 50 |
| College degree | 5 | 28 |
| Associate/Technical/Vocational degree | 3 | 17 |
| High school degree | 1 | 5 |
| Antibiotics during pregnancy | ||
| Did not receive | 12 | 67 |
| Received during current and/or previous pregnancy | 5 | 28 |
| Missing | 1 | 6 |
| Antibiotic counseling during pregnancy | ||
| Received some counseling | 2 | 11 |
| Received counseling | 5 | 28 |
| Did not receive counseling | 9 | 50 |
| Missing | 2 | 11 |
| Previous experience |
|
| Opinions of antibiotics |
|
| Concerns/risks |
|
| Antibiotics counseling |
|
| Category | Construct | Description |
|---|---|---|
| Perceived Expectations | Perceived benefits | The belief that antibiotics will successfully reduce the risk and severity of infection/illness. |
| Perceived barriers | Perceived negative effects and costs of antibiotics. | |
| Perceived self-efficacy | The conviction that one can take action and/or make a decision about taking antibiotics. | |
| Perceived Threats | Perceived susceptibility | Beliefs about the susceptibility of the mother or infant to an infection or disease that requires antibiotics. |
| Perceived severity | Perceived severity of a condition and its clinical sequela. | |
| Cues to Action | Events that trigger one to take antibiotics. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, L.Y.; Flood-Grady, E.; Hentschel, A.; Wright, L.; Mkuu, R.; Young, A.; Francois, M.; Neu, J.; Parker, L.A.; Shenkman, E.; et al. A Qualitative Study of Pregnant Women’s Perspectives on Antibiotic Use for Mom and Child: Implications for Developing Tailored Health Education Interventions. Antibiotics 2020, 9, 704. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100704
Chen LY, Flood-Grady E, Hentschel A, Wright L, Mkuu R, Young A, Francois M, Neu J, Parker LA, Shenkman E, et al. A Qualitative Study of Pregnant Women’s Perspectives on Antibiotic Use for Mom and Child: Implications for Developing Tailored Health Education Interventions. Antibiotics. 2020; 9(10):704. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100704
Chicago/Turabian StyleChen, Lynn Y., Elizabeth Flood-Grady, Austen Hentschel, Lauren Wright, Rahma Mkuu, Alyson Young, Magda Francois, Josef Neu, Leslie A. Parker, Elizabeth Shenkman, and et al. 2020. "A Qualitative Study of Pregnant Women’s Perspectives on Antibiotic Use for Mom and Child: Implications for Developing Tailored Health Education Interventions" Antibiotics 9, no. 10: 704. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9100704