Short- vs. Long-Course Antibiotic Treatment for Acute Streptococcal Pharyngitis: Systematic Review and Meta-Analysis of Randomized Controlled Trials



Abstract
:1. Introduction
2. Methods
2.1. Types of Studies
2.2. Types of Participants
2.3. Types of Interventions and Outcomes
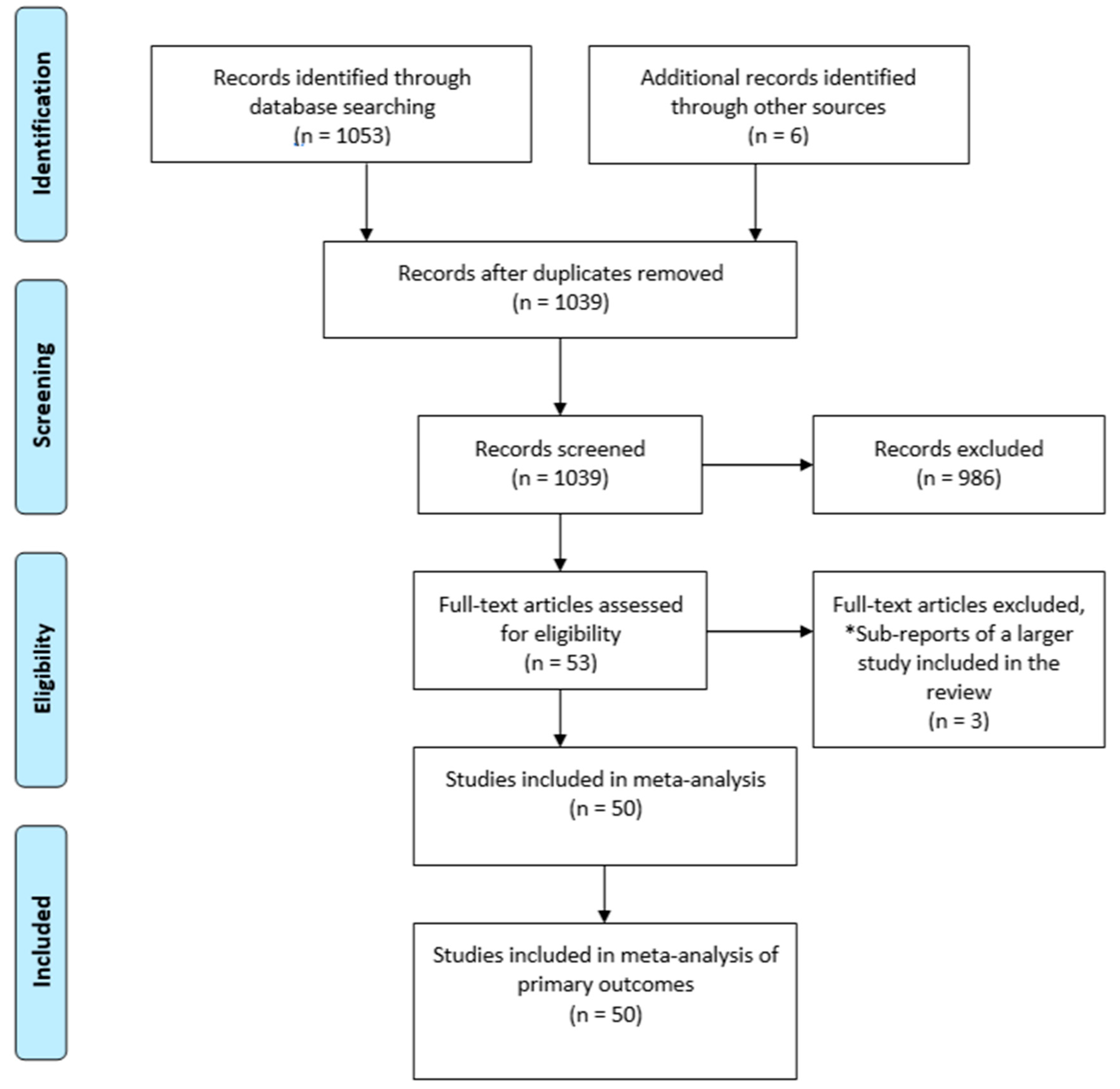
2.4. Search Strategy and Selection Criteria
3. Data Collection
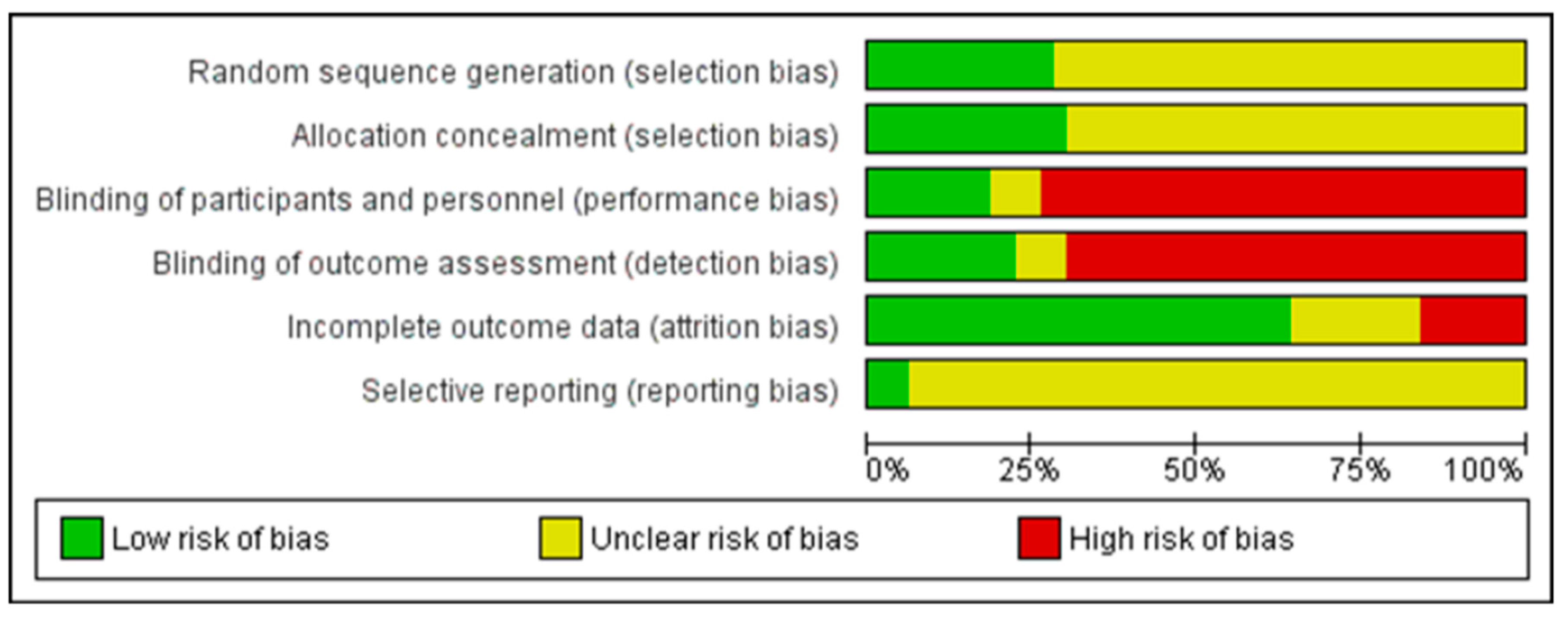
3.1. Risk of Bias
3.2. Analysis
4. Results
4.1. Characteristics of the Included Studies
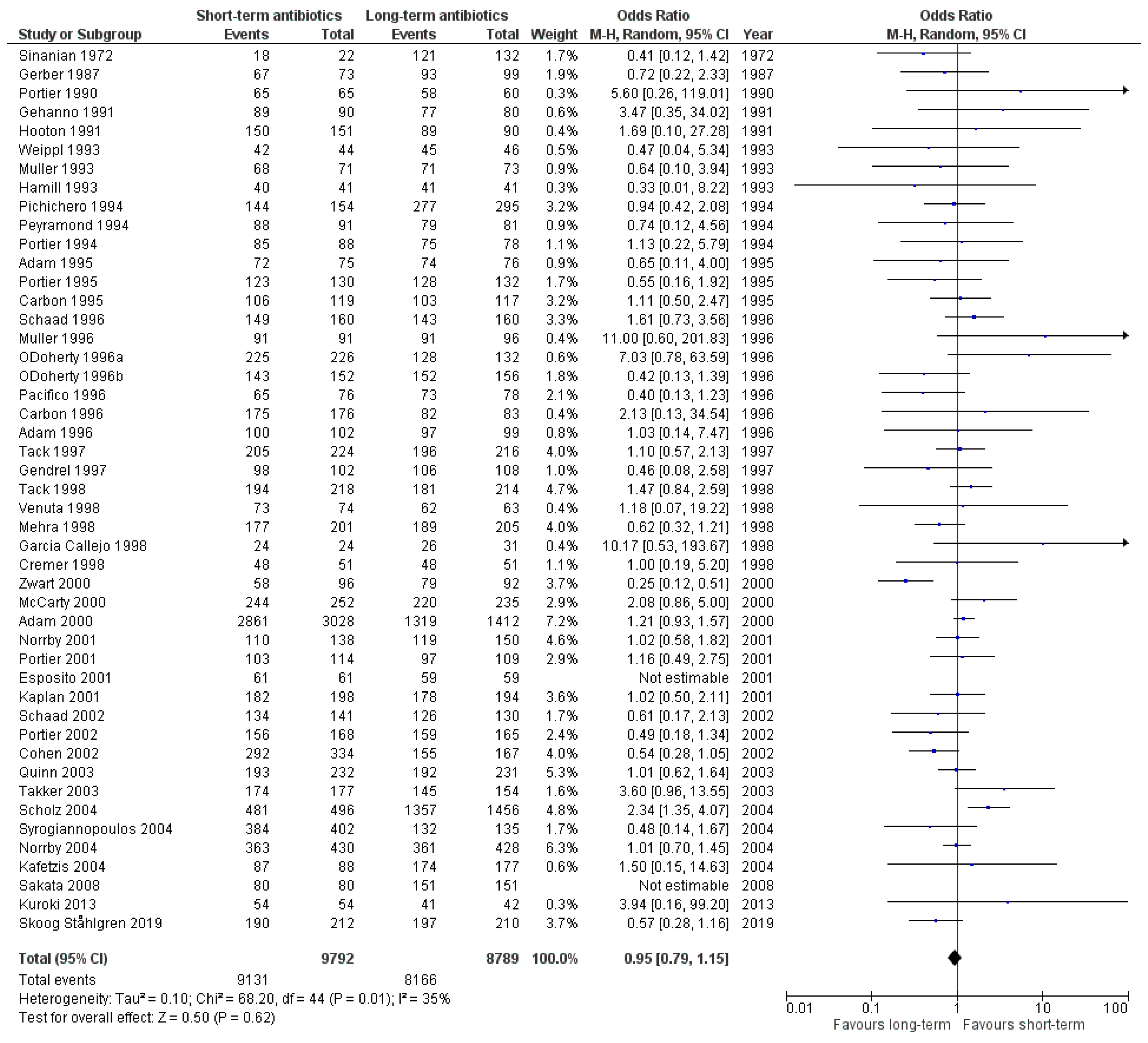
4.2. Effects of Intervention
5. Discussion
5.1. Summary of Main Results
5.2. Strengths and Weaknesses of Study
5.3. Comparison with Previous Studies
5.4. Relevance of the Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Schappert, S.M.; Rechtsteiner, E.A. Ambulatory medical care utilization estimates for 2006. Natl. Health Stat. Rep. 2008, 8, 1–29. [Google Scholar]
- Fleming-Dutra, K.E.; Hersh, A.L.; Shapiro, D.J.; Bartoces, M.; Enns, E.A.; File, T.M.; Finkelstein, J.A.; Gerber, J.S.; Hyun, D.Y.; Linder, J.A.; et al. Prevalence of Inappropriate Antibiotic Prescriptions among US Ambulatory Care Visits, 2010–2011. JAMA 2016, 315, 1864–1873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinks, A.; Glasziou, P.P.; Del Mar, C.B. Antibiotics for sore throat. Cochrane Database Syst. Rev. 2013, 2013, CD000023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shulman, S.T.; Bisno, A.L.; Clegg, H.W.; Gerber, M.A.; Kaplan, E.L.; Lee, G.; Martin, J.M.; van Beneden, C. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect. Dis. 2012, 55, 1279–1282. [Google Scholar] [CrossRef] [PubMed]
- Pelucchi, C.; Grigoryan, L.; Galeone, C.; Esposito, S.; Huovinen, P.; Little, P.; Verheij, T. Guideline for the management of acute sore throat. Clin. Microbiol. Infect. 2012, 18, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Spellberg, B.; Rice, L.B. Duration of Antibiotic Therapy: Shorter Is Better. Ann. Intern. Med. 2019, 171, 210–211. [Google Scholar] [CrossRef]
- Matthys, J.; De Meyere, M.; Van Driel, M.L.; De Sutter, A. Differences Among International Pharyngitis Guidelines: Not Just Academic. Ann. Fam. Med. 2007, 5, 436–443. [Google Scholar] [CrossRef] [Green Version]
- The European Committee on Antimicrobial Susceptibility Testing. Available online: https://www.eucast.org/ (accessed on 12 October 2020).
- Feder, H.M.; Gerber, M.A.; Randolph, M.F.; Stelmach, P.S.; Kaplan, E.L. Once-Daily Therapy for Streptococcal Pharyngitis with Amoxicillin. Pediatrics 1999, 103, 47–51. [Google Scholar] [CrossRef]
- Lennon, D.R.; Farrell, E.; Martin, D.R.; Stewart, J.M. Once-daily amoxicillin versus twice-daily penicillin V in group A beta-haemolytic streptococcal pharyngitis. Arch. Dis. Child. 2008, 93, 474–478. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Contopoulos-Ioannidis, D.G.; Chew, P.; Lau, J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for upper respiratory tract infections. J. Antimicrob. Chemother. 2001, 48, 677–689. [Google Scholar] [CrossRef] [Green Version]
- Casey, J.R.; Pichichero, M.E. Metaanalysis of Short Course Antibiotic Treatment for Group A Streptococcal Tonsillopharyngitis. Pediatr. Infect. Dis. J. 2005, 24, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Casey, J.R.; Pichichero, M.E. Higher Dosages of Azithromycin Are More Effective in Treatment of Group A Streptococcal Tonsillopharyngitis. Clin. Infect. Dis. 2005, 40, 1748–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pichichero, M.E.; Casey, J.R. Bacterial eradication rates with shortened courses of 2nd- and 3rd-generation cephalosporins versus 10 days of penicillin for treatment of group A streptococcal tonsillopharyngitis in adults. Diagn. Microbiol. Infect. Dis. 2007, 59, 127–130. [Google Scholar] [CrossRef] [PubMed]
- Altamimi, S.; Khalil, A.; Khalaiwi, K.A.; Milner, R.A.; Pusic, M.V.; Al Othman, M.A. Short-term late-generation antibiotics versus longer term penicillin for acute streptococcal pharyngitis in children. Cochrane Database Syst. Rev. 2012, 8, CD004872. [Google Scholar] [CrossRef] [Green Version]
- Dawson-Hahn, E.E.; Mickan, S.; Onakpoya, I.; Roberts, N.; Kronman, M.; Butler, C.C.; Thompson, M.J. Short-course versus long-course oral antibiotic treatment for infections treated in outpatient settings: A review of systematic reviews. Fam. Pr. 2017, 34, 511–519. [Google Scholar] [CrossRef]
- Rojas-Ramírez, C.; Kramer-Urrutia, T.; Cifuentes, L.; Ram, R.-; Kramer-Urrutia, T. Is a short-course antibiotic treatment effective for streptococcal tonsillopharyngitis in children? Medwave 2017, 17, e6873. [Google Scholar] [CrossRef]
- Falagas, M.; Vouloumanou, E.K.; Matthaiou, D.K.; Kapaskelis, A.M.; Karageorgopoulos, D.E. Effectiveness and safety of short-course vs long-course antibiotic therapy for group a beta hemolytic streptococcal tonsillopharyngitis: A meta-analysis of randomized trials. Mayo Clin. Proc. 2008, 83, 880–889. [Google Scholar] [CrossRef]
- Ståhlgren, G.S.; Tyrstrup, M.; Edlund, C.; Giske, C.G.; Mölstad, S.; Norman, C.; Rystedt, K.; Sundvall, P.-D.; Hedin, K. Penicillin V four times daily for five days versus three times daily for 10 days in patients with pharyngotonsillitis caused by group A streptococci: Randomised controlled, open label, non-inferiority study. BMJ 2019, 367, l5337. [Google Scholar] [CrossRef] [Green Version]
- Montori, V.M.; Wilczynski, N.L.; Morgan, D.; Haynes, R.B. Optimal search strategies for retrieving systematic reviews from Medline: Analytical survey. BMJ 2004, 330, 68. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Kannan, S.; Gowri, S. Clinical trials in allied medical fields: A cross-sectional analysis of World Health Organization International Clinical Trial Registry Platform. J. Ayurveda Integr. Med. 2016, 7, 48–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Review Manager (RevMan) [Computer Program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration. 2014. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman (accessed on 12 October 2020).
- Sinanian, R.; Ruoff, G.; Panzer, J.; Atkinson, W. Streptococcal pharyngitis: A comparison of the eradication of the organism by 5 and 10-day antibiotic therapy. Curr. Ther. Res. 1972, 14, 716–720. [Google Scholar]
- Gerber, M.A.; Randolph, M.F.; Chanatry, J.; Wright, L.L.; De Meo, K.; Kaplan, E.L. Five vs Ten Days of Penicillin V Therapy for Streptococcal Pharyngitis. Arch. Pediatr. Adolesc. Med. 1987, 141, 224–227. [Google Scholar] [CrossRef]
- Strömberg, A.; Schwan, A.; Cars, O. Five versus ten days treatment of group A streptococcal pharyngotonsillitis: A randomized controlled clinical trial with phenoxymethyl-penicillin and cefadroxil. Scand. J. Infect. Dis. 1988, 20, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Portier, H.; Chavanet, P.; Gouyon, J.B.; Guetat, F. Five day treatment of pharyngotonsillitis with cefpodoxime proxetil. J. Antimicrob. Chemother. 1990, 26, 79–85. [Google Scholar] [CrossRef]
- Gehanno, P.; Chiche, D. Traitement des angines à streptocoque bêta hémolytique du groupe A par le céfuroxime axétil pendant 4 jours: Étude comparative à la pénicilline V pendant 10 jours. Méd. Mal. Infect. 1991, 21, 66–70. [Google Scholar] [CrossRef]
- Hooton, T.M. A comparison of azithromycin and penicillin V for the treatment of streptococcal pharyngitis. Am. J. Med. 1991, 91, S23–S26. [Google Scholar] [CrossRef]
- Milatovic, D. Evaluation of cefadroxil, penicillin and erythromycin in the treatment of streptococcal tonsillopharyngitis. Pediatr. Infect. Dis. J. 1991, 10, S61–S63. [Google Scholar] [CrossRef]
- Hamill, J. Multicentre evaluation of azithromycin and penicillin V in the treatment of acute streptococcal pharyngitis and tonsillitis in children. J. Antimicrob. Chemother. 1993, 31, 89–94. [Google Scholar] [CrossRef]
- Müller, O. Comparison of azithromycin versus clarithromycin in the treatment of patients with upper respiratory tract infections. J. Antimicrob. Chemother. 1993, 31, 137–146. [Google Scholar] [CrossRef]
- Weippl, G. Multicentre comparison of azithromycin versus erythromycin in the treatment of paediatric pharyngitis or tonsillitis caused by group A streptococci. J. Antimicrob. Chemother. 1993, 31, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Peyramond, D.; Tigaud, S.; Bremard-Oury, C.; Scheimberg, A. Multicenter comparative trial of cefixime and phenoxymethylpenicillin for group a beta-hemolytic streptococcal tonsillitis. Curr. Ther. Res. 1994, 55, 14–21. [Google Scholar] [CrossRef]
- Pichichero, M.E.; Gooch, W.M.; Rodriguez, M.; Blumer, J.L.; Aronoff, S.C.; Jacobs, R.F.; Musser, J.M. Effective short-course treatment of acute group A beta-hemolytic streptococcal tonsillopharyngitis. Arch. Pediatr. Adolesc. Med. 1994, 148, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Portier, H.; Chavanet, P.; Waldner-Combernoux, A.; Kisterman, J.P.; Grey, P.C.; Ichou, F.; Safran, C. Five versus Ten Days Treatment of Streptococcal Pharyngotonsillitis: A Randomized Controlled Trial Comparing Cefpodoxime Proxetil and Phenoxymethyl Penicillin. Scand. J. Infect. Dis. 1994, 26, 59–66. [Google Scholar] [CrossRef]
- Adam, D.; Hostalk, U.; Troster, K. Five-day cefixime therapy for bacterial pharyngitis and/or tonsillitis: Comparison with 10-day penicillin V therapy. Infection 1995, 23 (Suppl. S2), S83–S86. [Google Scholar] [CrossRef] [PubMed]
- Carbon, C.; Chatelin, A.; Bingen, E.; Zuck, P.; Rio, Y.; Guetat, F.; Orvain, J. A double-blind randomized trial comparing the efficacy and safety of a 5-day course of cefotiam hexetil with that of a 10-day course of penicillin V in adult patients with pharyngitis caused by group A beta-haemolytic streptococci. J. Antimicrob. Chemother. 1995, 35, 843–854. [Google Scholar] [CrossRef] [PubMed]
- Portier, H.; Lucht, F.; Lescale, O.; Kazmierczak, A.; Ros, A.; Scheimberg, A. Josamycine 5 jours versus penicilline V 10 jours dans le traitement des angines aigues a streptocoque β-hemolytique du groupe A. Med. Mal. Infect. 1995, 25, 1005–1010. [Google Scholar] [CrossRef]
- Adam, D.; Scholz, H.; Aspe, C.; Berzel, H.G.; Bulle, D.; Fritz, H.P.; Grosse, V.; Hartmann, W.; Heil, R.P.; Hirschbrunn, P.; et al. Five days of erythromycin estolate versus ten days of penicillin V in the treatment of group a streptococcal tonsillopharyngitis in children. Eur. J. Clin. Microbiol. Infect. Dis. 1996, 15, 712–717. [Google Scholar] [CrossRef]
- Müller, O. An open comparative study of azithromycin and roxithromycin in the treatment of acute upper respiratory tract infections. J. Antimicrob. Chemother. 1996, 37, 83–92. [Google Scholar] [CrossRef]
- O’Doherty, B.; Pilfors, G.; Quinn, P.T.; Howard, A.; Bradbury, F.; Scully, M.; Clarke, O.; Kiernan, J.; Ryan, M.F.; O’Kelly, P.; et al. Azithromycin versus penicillin V in the treatment of paediatric patients with acute streptococcal pharyngitis/tonsillitis. Eur. J. Clin. Microbiol. Infect. Dis. 1996, 15, 718–724. [Google Scholar] [CrossRef]
- O’Doherty, B. An open comparative study of azithromycin versus cefaclor in the treatment of patients with upper respiratory tract infections. J. Antimicrob. Chemother. 1996, 37, 71–81. [Google Scholar] [CrossRef] [PubMed]
- Pacifico, L.; Scopetti, F.; Ranucci, A.; Pataracchia, M.; Savignoni, F.; Chiesa, C. Comparative efficacy and safety of 3-day azithromycin and 10-day penicillin V treatment of group A beta-hemolytic streptococcal pharyngitis in children. Antimicrob. Agents Chemother. 1996, 40, 1005–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaad, U.; Heynen, G. Evaluation of the efficacy, safety and toleration of azithromycin vs penicillin V in the treatment of acute streptococcal pharyngitis in children: Results of multicenter, open comparative study. The Swiss Tonsillopharyngitis Study Group. Pediatr. Infect. Dis. J. 1996, 15, 791–795. [Google Scholar] [CrossRef]
- Gendrel, D.; Bourrillon, A.; Touron, D.; Lilienthal, F.; Gendrel, D.; Bingen, E.; Raymond, J. Five-Day Spiramycin vs Seven-Day Penicillin V in the Treatment of Streptococcal Tonsillitis in Children. Clin. Drug Investig. 1997, 13, 338–344. [Google Scholar] [CrossRef]
- Tack, K.J.; Hedrick, J.A.; Rothstein, E.; Nemeth, M.A.; Keyserling, C.; Pichichero, M.E. A Study of 5-Day Cefdinir Treatment for Streptococcal Pharyngitis in Children. Arch. Pediatr. Adolesc. Med. 1997, 151, 45. [Google Scholar] [CrossRef]
- Cremer, J.; Wallrauch, C.; Milatovic, D.; Braveny, I. Azithromycin versus cefaclor in the treatment of pediatric patients with acute group A beta-hemolytic streptococcal tonsillopharyngitis. Eur. J. Clin. Microbiol. Infect. Dis. 1998, 17, 235–239. [Google Scholar] [CrossRef]
- García Callejo, F.J.; Velert Vila, M.M.; Orts Alborch, M.H.; Pardo Mateu, L.; Esparcia Navarro, M. Comparación de azitromicina, amoxicilina/ácido clavulánico y cefaclor en el tratamiento de la infección aguda otorrinolaringológica. Acta Otorrinolaringol. Esp. 1998, 49, 306–312. [Google Scholar]
- Mehra, S.; Van Moerkerke, M.; Welck, J.; Sverrisson, G.; Sirotiakova, J.; Marr, C.; Staley, H. Short course therapy with cefuroxime axetil for group A streptococcal tonsillopharyngitis in children. Pediatr. Infect. Dis. J. 1998, 17, 452–457. [Google Scholar] [CrossRef]
- Tack, K.J.; Henry, D.C.; Gooch, W.M.; Brink, D.N.; Keyserling, C.H. The Cefdinir Pharyngitis Study Group Five-Day Cefdinir Treatment for Streptococcal Pharyngitis. Antimicrob. Agents Chemother. 1998, 42, 1073–1075. [Google Scholar] [CrossRef] [Green Version]
- Venuta, A.; Laudizi, L.; Beverelli, A.; Bettelli, F.; Milioli, S.; Garetti, E. Azithromycin Compared with Clarithromycin for the Treatment of Streptococcal Pharyngitis in Children. J. Int. Med Res. 1998, 26, 152–158. [Google Scholar] [CrossRef]
- Adam, D.; Scholz, H.; Helmerking, M. Short-Course Antibiotic Treatment of 4782 Culture-Proven Cases of Group A Streptococcal Tonsillopharyngitis and Incidence of Poststreptococcal Sequelae. J. Infect. Dis. 2000, 182, 509–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mccarty, J.; Hedrick, J.A.; Gooch, W.M. Clarithromycin suspension vs penicillin V suspension in children with streptococcal pharyngitis. Adv. Ther. 2000, 17, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Zwart, S.; Sachs, A.P.E.; Ruijs, G.J.H.M.; Gubbels, J.W.; Hoes, A.W.; De Melker, R.A. Penicillin for acute sore throat: Randomised double blind trial of seven days versus three days treatment or placebo in adults. BMJ 2000, 320, 150–154. [Google Scholar] [CrossRef] [Green Version]
- Esposito, S.; Noviello, S.; Ianniello, F.; D’Errico, G. Short-course therapy with cefaclor for treatment of streptococcal pharyngotonsillitis. Int. J. Antimicrob. Agents 2001, 18, 341–345. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Gooch, W.M.; Notario, G.F.; Craft, J.C. Macrolide Therapy of Group A Streptococcal Pharyngitis: 10 Days of Macrolide Therapy (Clarithromycin) Is More Effective in Streptococcal Eradication than 5 Days (Azithromycin). Clin. Infect. Dis. 2001, 32, 1798–1802. [Google Scholar] [CrossRef] [Green Version]
- Norrby, S.R.; Rabie, W.J.; Bacart, P.; Mueller, O.; Leroy, B.; Rangaraju, M.; Butticaz-Iroudayassamy, E. Efficacy of Short-course Therapy with the Ketolide Telithromycin Compared with 10 Days of Penicillin V for the Treatment of Pharyngitis/Tonsillitis. Scand. J. Infect. Dis. 2001, 33, 883–890. [Google Scholar] [CrossRef]
- Portier, H.; Bourrillon, A.; Lucht, F.; Choutet, P.; Gehanno, P.; Meziane, L.; Bingen, E. Traitement des angines aiguës à streptocoque β-hémolytique du groupe A chez l’enfant par la josamycine pendant cinq jours. Arch. Pédiatr. 2001, 8, 700–706. [Google Scholar] [CrossRef]
- Cohen, R.; Reinert, P.; De La Rocque, F.; Levy, C.; Boucherat, M.; Robert, M.; Navel, M.; Brahimi, N.; Deforche, D.; Palestro, B.; et al. Comparison of two dosages of azithromycin for three days versus penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatr. Infect. Dis. J. 2002, 21, 297–303. [Google Scholar] [CrossRef]
- Portier, H.; Filipecki, J.; Weber, F.; Goldfarb, G.; Lethuaire, D.; Chauvin, J.P. Five day clarithromycin modified release versus 10 day penicillin V for group A streptococcal pharyngitis: A multi-centre, open-label, randomized study. J. Antimicrob. Chemother. 2002, 49, 337–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaad, U.B.; Kellerhals, P.; Altwegg, M. Azithromycin versus penicillin V for treatment of acute group A streptococcal pharyngitis. Pediatr. Infect. Dis. J. 2002, 21, 304–308. [Google Scholar] [CrossRef] [PubMed]
- Quinn, J.; Ruoff, G.E.; Ziter, P.S. Efficacy and tolerability of 5-day, once-daily telithromycin compared with 10-day, twice-daily clarithromycin for the treatment of group A beta-hemolytic streptococcal tonsillitis/pharyngitis: A multicenter, randomized, double-blind, parallel-group study. Clin. Ther. 2003, 25, 422–443. [Google Scholar] [CrossRef]
- Takker, U.; Dzyublyk, O.; Busman, T.; Notario, G.F. Comparison of 5 days of extended-release clarithromycin versus 10 days of penicillin V for the treatment of streptococcal pharyngitis/tonsillitis: Results of a multicenter, double-blind, randomized study in adolescent and adult patients. Curr. Med Res. Opin. 2003, 19, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Zwart, S.; Rovers, M.M.; A De Melker, R.; Hoes, A.W. Penicillin for acute sore throat in children: Randomised, double blind trial. BMJ 2003, 327, 1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kafetzis, D.; Liapi, G.; Tsolia, M.; Aoudi, H.; Mathioudakis, J.; Paraskakis, I.; Bairamis, T. Failure to eradicate Group A beta-haemolytic streptococci (GABHS) from the upper respiratory tract after antibiotic treatment. Int. J. Antimicrob. Agents 2004, 23, 67–71. [Google Scholar] [CrossRef]
- Norrby, S.R.; Quinn, J.; Rangaraju, M.; Leroy, B. Evaluation of 5-day therapy with telithromycin, a novel ketolide antibacterial, for the treatment of tonsillopharyngitis. Clin. Microbiol. Infect. 2004, 10, 615–623. [Google Scholar] [CrossRef] [Green Version]
- Scholz, H. Streptococcal-A Tonsillopharyngitis: A 5-Day Course of Cefuroxime Axetil versus a 10-Day Course of Penicillin V. Chemotherapy 2004, 50, 51–54. [Google Scholar] [CrossRef]
- Syrogiannopoulos, G.A.; Bozdogan, B.; Grivea, I.N.; Ednie, L.M.; Kritikou, D.I.; Katopodis, G.D.; Beratis, N.G.; Appelbaum, P.C. Hellenic Antibiotic-Resistant Respiratory Pathogens Study Group. Two dosages of clarithromycin for five days, amoxicillin/clavulanate for five days or penicillin V for ten days in acute group A streptococcal tonsillopharyngitis. Pediatr. Infect. Dis. J. 2004, 23, 857–865. [Google Scholar] [CrossRef]
- Sakata, H. Comparative study of 5-day cefcapene-pivoxil and 10-day amoxicillin or cefcapene-pivoxil for treatment of group A streptococcal pharyngitis in children. J. Infect. Chemother. 2008, 14, 208–212. [Google Scholar] [CrossRef]
- Kuroki, H.; Ishiwada, N.; Inoue, N.; Ishikawa, N.; Suzuki, H.; Himi, K.; Kurosaki, T. Comparison of clinical efficacy between 3-day combined clavulanate/amoxicillin preparation treatment and 10-day amoxicillin treatment in children with pharyngolaryngitis or tonsillitis. J. Infect. Chemother. 2013, 19, 12–19. [Google Scholar] [CrossRef]
- Centor, R.M.; Witherspoon, J.M.; Dalton, H.P.; Brody, C.E.; Link, K. The Diagnosis of Strep Throat in Adults in the Emergency Room. Med. Decis. Mak. 1981, 1, 239–246. [Google Scholar] [CrossRef]
- Turnidge, J.D. The pharmacodynamics of beta-lactams. Clin. Infect. Dis. 1998, 27, 10–22. [Google Scholar] [CrossRef]
- Peyramond, D.; Portier, H.; Geslin, P.; Cohen, R. 6-day amoxicillin versus 10-day penicillin V for group A beta-haemolytic streptococcal acute tonsillitis in adults: A French multicentre, open-label, randomized study. The French Study Group Clamorange. Scand. J. Infect. Dis. 1996, 28, 497–501. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Levy, C.; Doit, C.; De La Rocque, F.; Boucherat, M.; Fitoussi, F.; Langue, J.; Bingen, E. Six-day amoxicillin vs. ten-day penicillin V therapy for group A streptococcal tonsillopharyngitis. Pediatr. Infect. Dis. J. 1996, 15, 678–682. [Google Scholar] [CrossRef]
- Carapetis, J.R.; Steer, A.C.; Mulholland, E.K.; Weber, M. The global burden of group A streptococcal diseases. Lancet Infect. Dis. 2005, 5, 685–694. [Google Scholar] [CrossRef]
- Van Driel, M.L.; De Sutter, A.I.; Habraken, H.; Thorning, S.; Christiaens, T. Different antibiotic treatments for group A streptococcal pharyngitis. Cochrane Database Syst. Rev. 2016, 2016, CD004406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Critically Important Antimicrobials for Human Medicine; 6th Revision; World Health Organization: Geneva, Switzerland, 2019; License: CC BY-NC-SA 3.0 IGO; Available online: https://apps.who.int/iris/bitstream/handle/10665/312266/9789241515528-eng.pdf?ua=1. (accessed on 12 October 2020).
- Hsia, Y.; Lee, B.R.; Versporten, A.; Yang, Y.; Bielicki, J.; Jackson, C.; Newland, J.; Goossens, H.; Magrini, N.; Sharland, M. Use of the WHO Access Watch, and Reserve classification to define patterns of hospital antibiotic use (AWaRe): An analysis of paediatric survey data from 56 countries. Lancet Glob. Health 2019, 7, e861–e871. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | No of Patients | Population: Age Range | Short-Term Antibiotic Therapy | Long-Term Antibiotic Therapy | Inclusion Based on Centor Criteria [72] (Yes/No) | Sponsorship |
|---|---|---|---|---|---|---|
| Sinanian, 1972 | 154 | NA | Clindamycin 5d | Clindamycin 10d, Penicillin V 10d | No | The Upjohn Company, Michigan |
| Gerber, 1987 | 172 | 3–25 | Penicillin V 5d | Penicillin V 10d | No | No mention of sponsor |
| Strömberg, 1988 | 203 | 7–70 | Penicillin V 5d | Penicillin V 10d, Cefadroxil 10d | No | Bristol-Myers AB. Sweden and Leo AB Sweden |
| Portier, 1990 | 125 | 15–79 | Cefpodoxime 5d | Penicillin V 10d | No | No mention of sponsor |
| Gehanno, 1991 | 170 | 5–70 | Cefuroxime 4d | Penicillin V 10d | No | Glaxo |
| Hooton, 1991 | 241 | NA (only included ≥16 year) | Azithromycin 4d | Penicillin V 10d | No | Pfizer Central Research Groton, Connecticut |
| Milatovic, 1991 | 209 | NA (only included children) | Cefadroxil 5d | Penicillin V 10d | No | No mention of sponsor |
| Hamill, 1993 | 82 | 2–12 | Azithromycin 3d | Penicillin V 10d | No | No mention of sponsor |
| Muller, 1993 | 144 | NA (only included ≥12 year) | Azithromycin 3d | Clarithromycin 10d | No | No mention of sponsor |
| Weippl, 1993 | 90 | 2–12 | Azithromycin 3d | Erythromycin 10d | No | No mention of sponsor |
| Peyramond, 1994 | 172 | 8–25 | Cefixime 4d | Penicillin V 10d | No | No mention of sponsor |
| Pichichero, 1994 | 449 | 2–17 | Cefpodoxime 5d | Cefpodoxime 10d, Penicillin V 10d | No | The Upjohn Company, Michigan |
| Portier, 1994 | 166 | 11–82 | Cefpodoxime 5d | Penicillin V 10d | No | Roussel-Uclaf |
| Adam, 1995 | 151 | 1–12 | Cefixime 5d | Penicillin V 10d | No | No mention of sponsor |
| Carbon, 1995 | 190 | 15–79 | Cefotiam 5d | Penicillin V 10d | No | Roussel-Uclaf |
| Portier, 1995 | 262 | 8–30 | Josamycin 5d | Penicillin V 10d | No | No mention of sponsor |
| Adam, 1996 | 201 | 3–17 | Erythromycin 5d | Penicillin V 10d | No | Infectopharm Arzneimittel GmbH, Germany |
| Carbon, 1996 | 259 | 18–65 | Azithromycin 3 and 5d | Roxithromycin 10d | No | Pfizer France |
| Muller, 1996 | 187 | 15–86 | Azithromycin 3d | Roxithromycin 10d | No | No mention of sponsor |
| O’Doherty, 1996a | 358 | 2–13 | Azithromycin 3d (2 doses) | Penicillin V 10d | No | No mention of sponsor |
| O’Doherty, 1996b | 308 | NA (only included ≥12 year) | Azithromycin 3d | Cefaclor 10d | No | No mention of sponsor |
| Pacifico, 1996 | 154 | 3–12 | Azithromycin 3d | Penicillin V 10d | No | Funded publicly |
| Schaad, 1996 | 320 | 1–14 | Azithromycin 3d | Penicillin V 10d | No | No mention of sponsor |
| Gendrel, 1997 | 210 | 1–14 | Spiramycin 5d | Penicillin V 7d | No | Rhone-Poulenc Rorer |
| Tack, 1997 | 440 | 1–18 | Cefdinir 5d | Penicillin V 10d | No | Parke-Davis Pharmaceutical Research |
| Cremer, 1998 | 102 | 1–12 | Azithromycin 3d | Cefaclor 10d | No | No mention of sponsor |
| Garcia Callejo, 1998 | 55 | 3–6 | Azithromycin 3d | Amox/clav+Cefaclor 7-14d | No | No mention of sponsor |
| Mehra, 1998 | 396 | 3–13 | Cefuroxime 5d | Cefuroxime 10d | No | No mention of sponsor |
| Tack, 1998 | 432 | 13–76 | Cefdinir 5d | Penicillin V 10d | No | Parke-Davis pharmaceutical research |
| Venuta, 1998 | 137 | 4–12 | Azithromycin 3d | Clarithromycin 10d | No | No mention of sponsor |
| Adam, 2000 | 4440 | 1–18 | Ceftibuten 5d, Erythromycin 5d, Cefuroxime 5d, Clarithromycin 5d, Loracarbef 5d, Amox/clav 5d | Penicillin V 10d | No | Cascan, Essex Pharma, Glaxo Wellcome, Infectopharm Arzneimittel und Consilium, Lilly Deutschland, and Smith Kline Beecham Pharma |
| McCarty, 2000 | 487 | 1–12 | Clarithromycin 5d | Penicillin V 10d | No | No mention of sponsor |
| Zwart, 2000 | 186 | 15–60 | Penicillin V 3d | Penicillin V 7d | Yes | Funded publicly |
| Esposito, 2001 | 120 | 3–12 | Cefaclor 5d | Cefaclor 10d | No | No mention of sponsor |
| Kaplan, 2001 | 392 | 12–61 | Azithromycin 5d | Clarithromycin 10d | No | Abbott laboratories |
| Norrby, 2001 | 288 | 15–74 | Telithromycin 5d | Penicillin V 10d | No | Aventis pharma |
| Portier, 2001 | 223 | 3–12 | Josamycin 5d | Penicillin V 10d | No | Aventis Pharma |
| Cohen, 2002 | 501 | 2–12 | Azithromycin 3d (2 doses) | Penicillin V 10d | No | Pfizer France |
| Portier, 2002 | 333 | 12–40 | Clarithromycin 5d | Penicillin V 10d | No | Abbott France (Rungis, France) and Sanofi-Synthelabo |
| Schaad, 2002 | 271 | 2–12 | Azithromycin 3d | Penicillin V 10d | No | Pfizer AG (PK) |
| Quinn, 2003 | 463 | 13–81 | Telithromycin 5d | Clarithromycin 10d | No | Aventis Pharma |
| Takker, 2003 | 331 | 12–75 | Clarithromycin 5d | Penicillin V 10d | No | Abbott Laboratories |
| Zwart, 2003 | 69 | 4–15 | Penicillin V 3d | Penicillin V 7d | Yes | Funded publicly |
| Kafetzis, 2004 | 265 | 3–13 | Cefprozil 5d | Penicillin V 10d, Clarithromycin 10d | No | No mention of sponsor |
| Norrby, 2004 | 858 | NA (only included ≥13 year) | Telithromycin 5d | Penicillin V 10d, Clarithromycin 10d | No | Aventis Pharma |
| Scholz, 2004 | 1952 | 1–17 | Cefuroxime 5d | Penicillin V 10d | No | No mention of sponsor |
| Syrogiannopoulos, 2004 | 537 | 2–16 | Clarithromycin 5d (2 doses), Amox/clav 5d | Penicillin V 10d | No | Abbott Laboratories |
| Sakata, 2008 | 231 | 1–16 | Cefcapene 5d | Cefcapene 10d, Amoxicillin 10d | No | No mention of sponsor |
| Kuroki, 2013 | 96 | 1–13 | Amox/clav 3d | Amoxicillin 10d | No | Glaxo-SmithKline K.K. |
| Skoog Ståhlgren, 2019 | 422 | 3–67 | Penicillin V 5d | Penicillin V 10d | Yes | Funded publicly |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holm, A.E.; Llor, C.; Bjerrum, L.; Cordoba, G. Short- vs. Long-Course Antibiotic Treatment for Acute Streptococcal Pharyngitis: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antibiotics 2020, 9, 733. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110733
Holm AE, Llor C, Bjerrum L, Cordoba G. Short- vs. Long-Course Antibiotic Treatment for Acute Streptococcal Pharyngitis: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antibiotics. 2020; 9(11):733. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110733
Chicago/Turabian StyleHolm, Anna Engell, Carl Llor, Lars Bjerrum, and Gloria Cordoba. 2020. "Short- vs. Long-Course Antibiotic Treatment for Acute Streptococcal Pharyngitis: Systematic Review and Meta-Analysis of Randomized Controlled Trials" Antibiotics 9, no. 11: 733. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9110733