Delayed Antibiotic Prescription by General Practitioners in the UK: A Stated-Choice Study

 , ,
, ,  , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Results
2.1. Respondent Characteristics
2.2. Importance Ranking of the Attributes
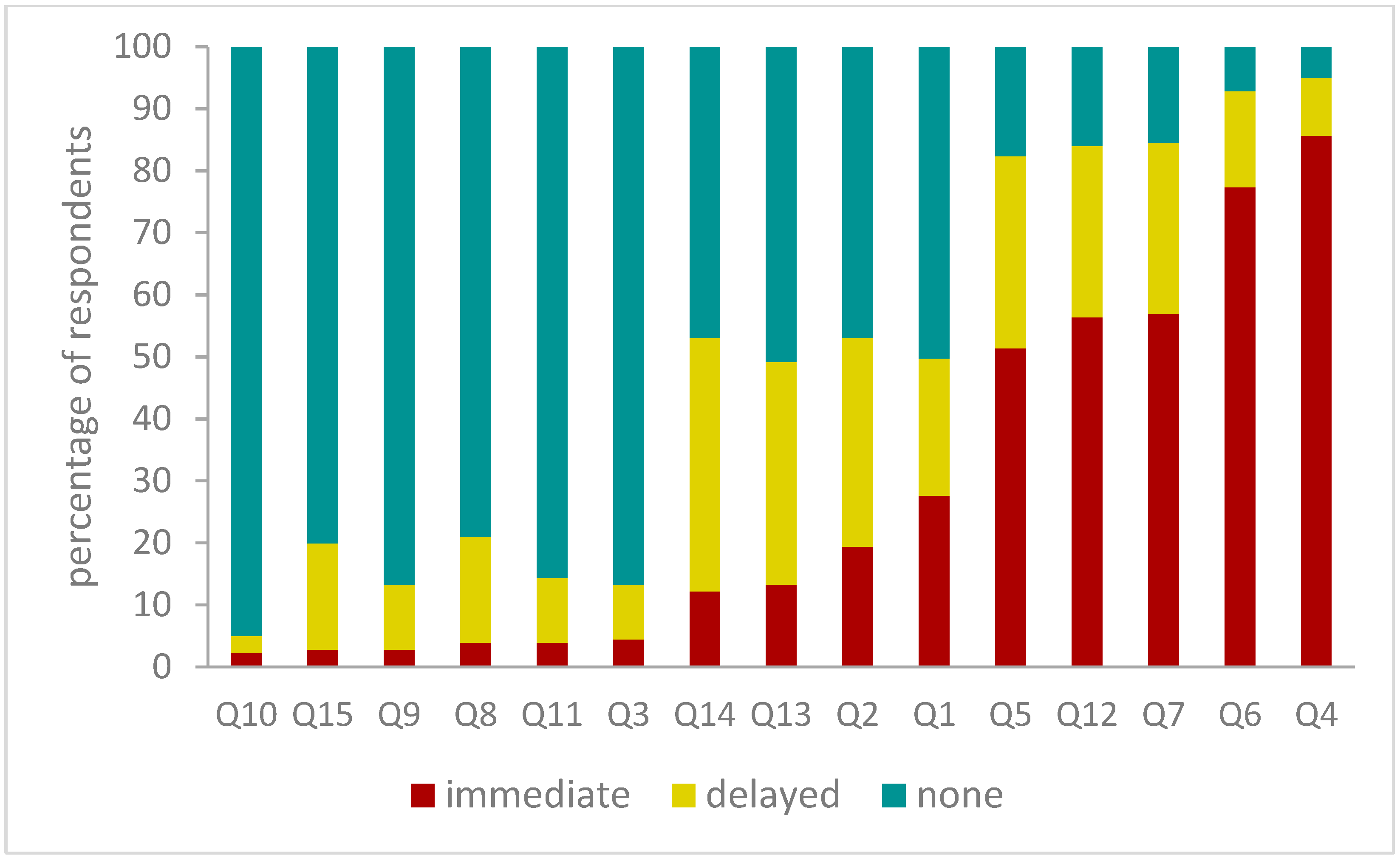
2.3. Choice Responses
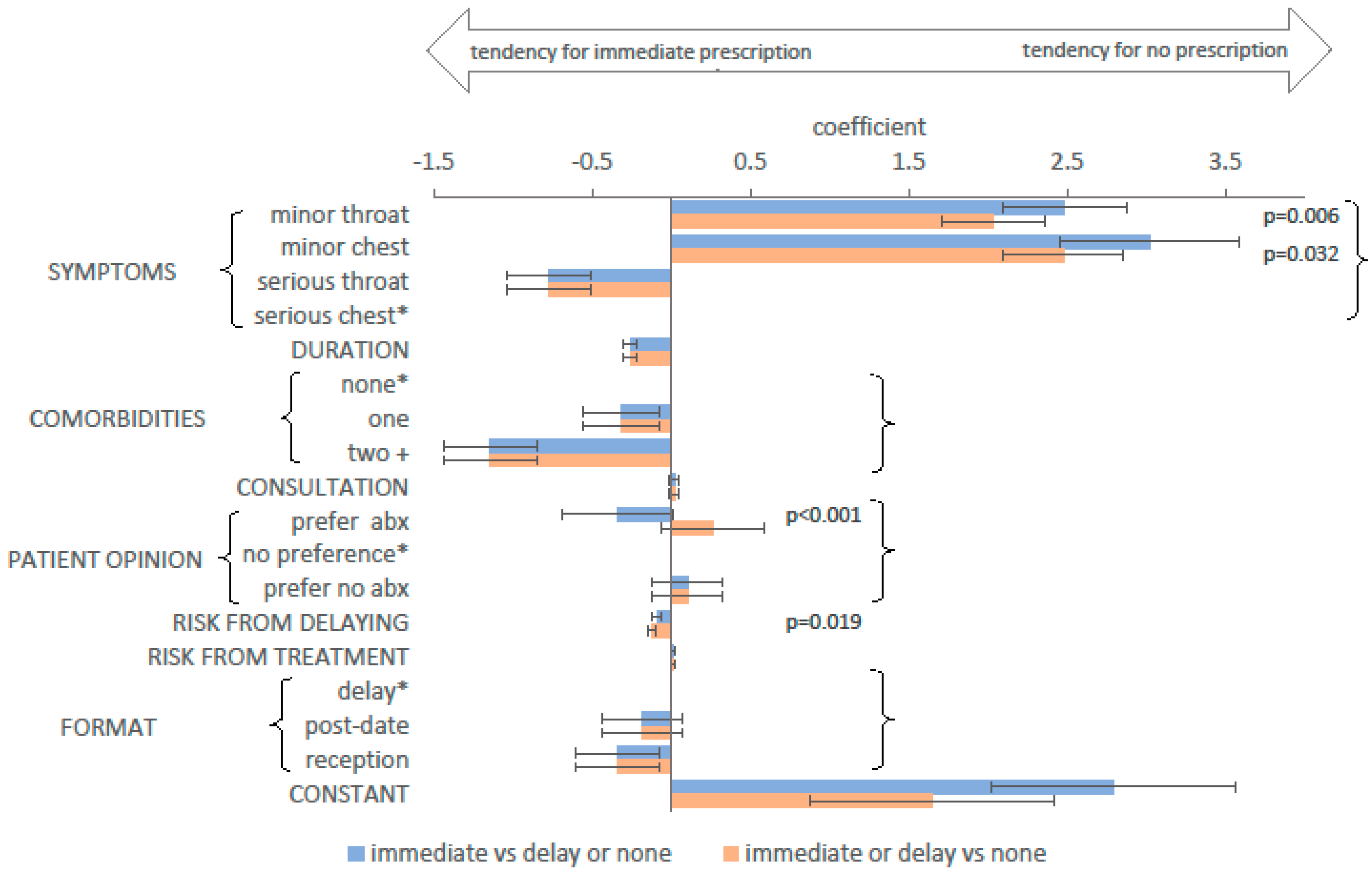
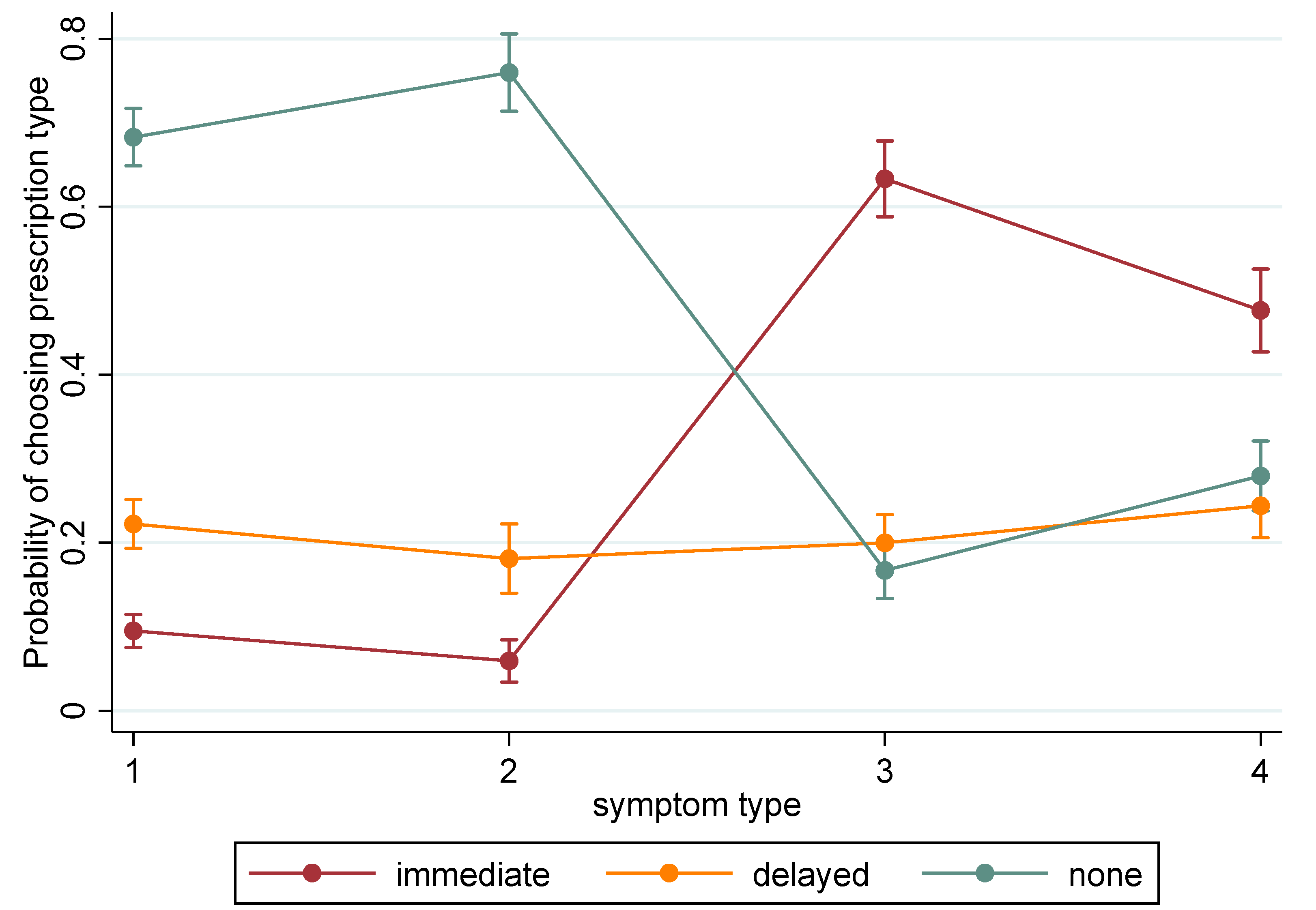
2.4. Choice Modelling
3. Discussion
Limitations
4. Methods
4.1. Defining Survey Attributes and Levels
4.2. Choice Questions
4.3. Survey and Experimental Design
4.4. Data Collection
4.5. Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| abx | antibiotics |
| GP | general practitioner |
| NHS | National Health Service |
| NICE | National Institute for Health and Care Excellence |
| RTI | respiratory tract infection |
References
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Available online: https://wellcomecollection.org/works/thvwsuba (accessed on 1 May 2019).
- Davies, S. Annual Report of the Chief Medical Officer 2011: Volume 2; Department of Health and Social Care: London, UK, 2013. [Google Scholar]
- Public Health England. English Surveillance Programme for Antimicrobial Utilisation and Resistance (ESPAUR): Report 2018–2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/843129/English_Surveillance_Programme_for_Antimicrobial_Utilisation_and_Resistance_2019.pdf (accessed on 20 February 2020).
- OpenPrescribing.net, EBM DataLab, University of Oxford, Oxford. Available online: https://openprescribing.net/bnf/0501/ (accessed on 1 July 2020).
- Smieszek, T.; Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.M.; Hopkins, S.; Sharland, M.; Hay, A.D.; Moore, M.V.; Robotham, J.V. Potential for reducing inappropriate antibiotic prescribing in English primary care. J. Antimicrob. Chemother. 2018, 73, ii36–ii43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.R.M.; Dolk, F.C.K.; Pouwels, K.B.; Christie, M.; Robotham, J.V.; Smieszek, T. Defining the appropriateness and inappropriateness of antibiotic prescribing in primary care. J. Antimicrob. Chemother. 2018, 73, ii11–ii18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NICE. Quality Standard QS121: Antimicrobial Stewardship. Available online: https://www.nice.org.uk/guidance/qs121/chapter/Quality-statement-2-Back-up-delayed-prescribing (accessed on 20 January 2020).
- Spurling, G.K.; Del Mar, C.B.; Dooley, L.; Foxlee, R.; Farley, R. Delayed antibiotic prescriptions for respiratory infections. Cochrane Database Syst. Rev. 2017, 9, Cd004417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arroll, B.; Kenealy, T.; Kerse, N. Do delayed prescriptions reduce antibiotic use in respiratory tract infections? A systematic review. Br J Gen Pr. 2003, 53, 871–877. [Google Scholar]
- Little, P.; Stuart, B.; Hobbs, F.D.R.; Butler, C.C.; Hay, A.D.; Delaney, B.; Campbell, J.; Broomfield, S.; Barratt, P.; Hood, K.; et al. Antibiotic prescription strategies for acute sore throat: A prospective observational cohort study. Lancet Infect. Dis. 2014, 14, 213–219. [Google Scholar] [CrossRef]
- Little, P.; Moore, M.; Kelly, J.; Williamson, I.; Leydon, G.; McDermott, L.; Mullee, M.; Stuart, B. Delayed antibiotic prescribing strategies for respiratory tract infections in primary care: Pragmatic, factorial, randomised controlled trial. BMJ 2014, 348, g1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Everitt, H.A.; Little, P.S.; Smith, P.W.F. A randomised controlled trial of management strategies for acute infective conjunctivitis in general practice. BMJ 2006, 333, 321. [Google Scholar] [CrossRef] [Green Version]
- Little, P.; Moore, M.V.; Turner, S.; Rumsby, K.; Warner, G.; Lowes, J.A.; Smith, H.; Hawke, C.; Leydon, G.; Arscott, A.; et al. Effectiveness of five different approaches in management of urinary tract infection: Randomised controlled trial. BMJ 2010, 340, c199. [Google Scholar] [CrossRef] [Green Version]
- NICE. Respiratory tract infections (self-limiting): Prescribing antibiotics. Clinical guideline (CG69). Available online: https://www.nice.org.uk/guidance/cg69 (accessed on 26 March 2018).
- NICE. Sore throat (acute): Antimicrobial prescribing. NICE guideline (NG84). Available online: https://www.nice.org.uk/guidance/ng84 (accessed on 20 May 2019).
- NICE. Cough (acute): Antimicrobial prescribing. NICE guideline (NG120). Available online: https://www.nice.org.uk/guidance/ng120/chapter/Recommendations#treatment (accessed on 1 February 2020).
- NICE. Urinary tract infection (lower): Antimicrobial prescribing. NICE guideline (NG109). Available online: https://www.nice.org.uk/guidance/ng109/chapter/Recommendations#treatment-for-women-with-lower-uti-who-are-not-pregnant (accessed on 1 February 2020).
- NICE. Clinical Knowledge Summary—Conjunctivitis (infective). Available online: https://cks.nice.org.uk/conjunctivitis-infective#!scenario:1 (accessed on 30 January 2020).
- Ryves, R.; Eyles, C.; Moore, M.; McDermott, L.; Little, P.; Leydon, G.M. Understanding the delayed prescribing of antibiotics for respiratory tract infection in primary care: A qualitative analysis. Bmj Open 2016, 6, e011882. [Google Scholar] [CrossRef] [Green Version]
- Leydon, G.M.; Turner, S.; Smith, H.; Little, P. Women’s views about management and cause of urinary tract infection: Qualitative interview study. BMJ 2010, 340, c279. [Google Scholar] [CrossRef] [Green Version]
- Little, P.; Stuart, B.; Smith, S.; Thompson, M.J.; Knox, K.; van den Bruel, A.; Lown, M.; Moore, M.; Mant, D. Antibiotic prescription strategies and adverse outcome for uncomplicated lower respiratory tract infections: Prospective cough complication cohort (3C) study. BMJ 2017, 357, j2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Little, P.; Hobbs, F.R.; Moore, M.; Mant, D.; Williamson, I.; McNulty, C.; Lasseter, G.; Cheng, M.E.; Leydon, G.; McDermott, L.; et al. PRImary care Streptococcal Management (PRISM) study: In vitro study, diagnostic cohorts and a pragmatic adaptive randomised controlled trial with nested qualitative study and cost-effectiveness study. Health Technol Assess 2014, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, S.; Rowbotham, S.; Chisholm, A.; Wearden, A.; Moschogianis, S.; Cordingley, L.; Baker, D.; Hyde, C.; Chew-Graham, C. Managing self-limiting respiratory tract infections: A qualitative study of the usefulness of the delayed prescribing strategy. Br J Gen Pr. 2011, 61, e579–e589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raft, C.F.; Bjerrum, L.; Arpi, M.; Jarlov, J.O.; Jensen, J.N. Delayed antibiotic prescription for upper respiratory tract infections in children under primary care: Physicians’ views. Eur. J. Gen. Pract. 2017, 23, 190–195. [Google Scholar] [CrossRef] [Green Version]
- Sargent, L.; McCullough, A.; Del Mar, C.; Lowe, J. Using theory to explore facilitators and barriers to delayed prescribing in Australia: A qualitative study using the Theoretical Domains Framework and the Behaviour Change Wheel. Bmc Fam Pr. 2017, 18, 20. [Google Scholar] [CrossRef]
- Lum, E.P.M.; Page, K.; Whitty, J.A.; Doust, J.; Graves, N. Antibiotic prescribing in primary healthcare: Dominant factors and trade-offs in decision-making. Infect. Dis. Health 2018, 23, 74–86. [Google Scholar] [CrossRef] [Green Version]
- Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.M.; Smieszek, T.; Robotham, J.V. Explaining variation in antibiotic prescribing between general practices in the UK. J. Antimicrob. Chemother. 2018, 73, ii27–ii35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolk, F.C.K.; Pouwels, K.B.; Smith, D.R.M.; Robotham, J.V.; Smieszek, T. Antibiotics in primary care in England: Which antibiotics are prescribed and for which conditions? J. Antimicrob. Chemother. 2018, 73, ii2–ii10. [Google Scholar] [CrossRef] [PubMed]
- Gulliford, M.C.; Dregan, A.; Moore, M.V.; Ashworth, M.; Staa, T.v.; McCann, G.; Charlton, J.; Yardley, L.; Little, P.; McDermott, L. Continued high rates of antibiotic prescribing to adults with respiratory tract infection: Survey of 568 UK general practices. Bmj Open 2014, 4, e006245. [Google Scholar] [CrossRef]
- Pouwels, K.B.; Dolk, F.C.K.; Smith, D.R.M.; Robotham, J.V.; Smieszek, T. Actual versus ‘ideal’ antibiotic prescribing for common conditions in English primary care. J. Antimicrob. Chemother. 2018, 73, 19–26. [Google Scholar] [CrossRef]
- Macfarlane, J.; Holmes, W.; Gard, P.; Macfarlane, R.; Rose, D.; Weston, V.; Leinonen, M.; Saikku, P.; Myint, S. Prospective study of the incidence, aetiology and outcome of adult lower respiratory tract illness in the community. Thorax 2001, 56, 109–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, J.; Wordsworth, S.; Schuh, A. Patients’ Preferences for Genomic Diagnostic Testing in Chronic Lymphocytic Leukaemia: A Discrete Choice Experiment. Patient Patient Cent. Outcomes Res. 2016, 9, 525–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rowen, D.; Brazier, J.; Mukuria, C.; Keetharuth, A.; Risa Hole, A.; Tsuchiya, A.; Whyte, S.; Shackley, P. Eliciting Societal Preferences for Weighting QALYs for Burden of Illness and End of Life. Med Decis Mak. 2016, 36, 210–222. [Google Scholar] [CrossRef] [PubMed]
- Regier, D.A.; Diorio, C.; Ethier, M.-C.; Alli, A.; Alexander, S.; Boydell, K.M.; Gassas, A.; Taylor, J.; Kellow, C.; Mills, D.; et al. Discrete Choice Experiment to Evaluate Factors That Influence Preferences for Antibiotic Prophylaxis in Pediatric Oncology. PLoS ONE 2012, 7, e47470. [Google Scholar] [CrossRef] [PubMed]
- Little, P.; Hobbs, F.D.R.; Moore, M.; Mant, D.; Williamson, I.; McNulty, C.; Cheng, Y.E.; Leydon, G.; McManus, R.; Kelly, J.; et al. Clinical score and rapid antigen detection test to guide antibiotic use for sore throats: Randomised controlled trial of PRISM (primary care streptococcal management). BMJ 2013, 347, f5806. [Google Scholar] [CrossRef] [Green Version]
- Royal College of General Practitioners. TARGET Antibiotic Toolkit. Available online: https://www.rcgp.org.uk/clinical-and-research/resources/toolkits/target-antibiotic-toolkit.aspx (accessed on 20 May 2019).
- Fletcher-Lartey, S.; Yee, M.; Gaarslev, C.; Khan, R. Why do general practitioners prescribe antibiotics for upper respiratory tract infections to meet patient expectations: A mixed methods study. Bmj Open 2016, 6, e012244. [Google Scholar] [CrossRef] [Green Version]
- Arroll, B.; Kenealy, T.; Kerse, N. Do delayed prescriptions reduce the use of antibiotics for the common cold? A single-blind controlled trial. J. Fam. Pract. 2002, 51, 324–328. [Google Scholar] [PubMed]
- Little, P.; Rumsby, K.; Kelly, J.; Watson, L.; Moore, M.; Warner, G.; Fahey, T.; Williamson, I. Information Leaflet and Antibiotic Prescribing Strategies for Acute Lower Respiratory Tract InfectionA Randomized Controlled Trial. JAMA 2005, 293, 3029–3035. [Google Scholar] [CrossRef] [Green Version]
- Little, P.; Stuart, B.; Hobbs, F.D.R.; Butler, C.C.; Hay, A.D.; Campbell, J.; Delaney, B.; Broomfield, S.; Barratt, P.; Hood, K.; et al. Predictors of suppurative complications for acute sore throat in primary care: Prospective clinical cohort study. Bmj Br. Med. J. 2013, 347, f6867. [Google Scholar] [CrossRef] [Green Version]
- Smith, S.M.; Fahey, T.; Smucny, J.; Becker, L.A. Antibiotics for acute bronchitis. Cochrane Database Syst. Rev. 2017, 6, CD000245. [Google Scholar] [CrossRef]
- NHS England. Side effects—Antibiotics. Available online: https://www.nhs.uk/conditions/antibiotics/side-effects/ (accessed on 11 June 2019).
- Saliba-Gustafsson, E.A.; Roing, M.; Borg, M.A.; Rosales-Klintz, S.; Lundborg, C.S. General practitioners’ perceptions of delayed antibiotic prescription for respiratory tract infections: A phenomenographic study. PLoS ONE 2019, 14, e0225506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Poza Abad, M.; Mas Dalmau, G.; Gich Saladich, I.; Martínez García, L.; Llor, C.; Alonso-Coello, P. Use of delayed antibiotic prescription in primary care: A cross-sectional study. Bmc Fam. Pract. 2019, 20, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guy, R.; Williams, C.; Irvine, N.; Reynolds, A.; Coelho, J.; Saliba, V.; Thomas, D.; Doherty, L.; Chalker, V.; von Wissmann, B.; et al. Increase in scarlet fever notifications in the United Kingdom, 2013/2014. Eurosurveillance 2014, 19, 20749. [Google Scholar] [CrossRef] [PubMed]
- Lamagni, T.; Guy, R.; Chand, M.; Henderson, K.L.; Chalker, V.; Lewis, J.; Saliba, V.; Elliot, A.J.; Smith, G.E.; Rushton, S.; et al. Resurgence of scarlet fever in England, 2014–16: A population-based surveillance study. Lancet Infect. Dis. 2018, 18, 180–187. [Google Scholar] [CrossRef] [Green Version]
- Francis, N.A.; Gillespie, D.; Nuttall, J.; Hood, K.; Little, P.; Verheij, T.; Goossens, H.; Coenen, S.; Butler, C.C. Delayed antibiotic prescribing and associated antibiotic consumption in adults with acute cough. Br J Gen Pr. 2012, 62, e639–e646. [Google Scholar] [CrossRef] [Green Version]
- Macfarlane, J.; Holmes, W.; Macfarlane, R.; Britten, N. Influence of patients’ expectations on antibiotic management of acute lower respiratory tract illness in general practice: Questionnaire study. BMJ 1997, 315, 1211–1214. [Google Scholar] [CrossRef] [Green Version]
- Butler, C.C.; Rollnick, S.; Pill, R.; Maggs-Rapport, F.; Stott, N. Understanding the culture of prescribing: Qualitative study of general practitioners’ and patients’ perceptions of antibiotics for sore throats. Bmj 1998, 317, 637–642. [Google Scholar] [CrossRef] [Green Version]
- Linder, J.A.; Singer, D.E. Desire for antibiotics and antibiotic prescribing for adults with upper respiratory tract infections. J. Gen. Intern. Med. 2003, 18, 795–801. [Google Scholar] [CrossRef] [Green Version]
- Hoye, S.; Frich, J.C.; Lindbaek, M. Use and feasibility of delayed prescribing for respiratory tract infections: A questionnaire survey. Bmc Fam Pr. 2011, 12, 34. [Google Scholar] [CrossRef] [Green Version]
- Rowe, T.A.; Linder, J.A. Delayed Antibiotic Prescriptions in Ambulatory Care: Reconsidering a Problematic Practice. JAMA 2020. [Google Scholar] [CrossRef] [Green Version]
- Erdem, S.; Thompson, C. Prioritising health service innovation investments using public preferences: A discrete choice experiment. Bmc Health Serv. Res. 2014, 14, 360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rose, J.M.; Bliemer, M.C.J. Constructing Efficient Stated Choice Experimental Designs. Transp. Rev. 2009, 29, 587–617. [Google Scholar] [CrossRef]
- Hayhoe, B.; Greenfield, G.; Majeed, A. Is it getting easier to obtain antibiotics in the UK? Br J Gen Pr. 2019, 69, 54–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bridges, J.F.P.; Hauber, A.B.; Marshall, D.; Lloyd, A.; Prosser, L.A.; Regier, D.A.; Johnson, F.R.; Mauskopf, J. Conjoint Analysis Applications in Health—A Checklist: A Report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health 2011, 14, 403–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenealy, T.; Arroll, B. Antibiotics for the common cold and acute purulent rhinitis. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed]
- Spinks, A.; Glasziou, P.P.; Del Mar, C.B. Antibiotics for sore throat. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [Green Version]
- DeShazo, J.R.; Fermo, G. Designing Choice Sets for Stated Preference Methods: The Effects of Complexity on Choice Consistency. J. Environ. Econ. Manag. 2002, 44, 123–143. [Google Scholar] [CrossRef]
- McNulty, C.; Hawking, M.; Lecky, D.; Jones, L.; Owens, R.; Charlett, A.; Butler, C.; Moore, P.; Francis, N. Effects of primary care antimicrobial stewardship outreach on antibiotic use by general practice staff: Pragmatic randomized controlled trial of the TARGET antibiotics workshop. J. Antimicrob. Chemother. 2018, 73, 1423–1432. [Google Scholar] [CrossRef]
- Skedgel, C.; Wailoo, A.; Akehurst, R. Societal preferences for distributive justice in the allocation of health care resources: A latent class discrete choice experiment. Med Decis Mak. 2015, 35, 94–105. [Google Scholar] [CrossRef] [PubMed]
- Shah, K.K.; Tsuchiya, A.; Wailoo, A.J. Valuing health at the end of life: A stated preference discrete choice experiment. Soc Sci Med 2015, 124, 48–56. [Google Scholar] [CrossRef] [Green Version]
- ChoiceMetrics. Ngene 1.1.1 User Manual & Reference Guide; ChoiceMetrics: St Leonards, Australia, 2012. [Google Scholar]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LP: College Station, TX, USA, 2017. [Google Scholar]
- McKelvey, R.D.; Zavoina, W. A statistical model for the analysis of ordinal level dependent variables. J. Math. Sociol. 1975, 4, 103–120. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Attribute a | Levels | Basis |
|---|---|---|
| Symptoms the patient is experiencing b | 1: Sore and red throat, and swollen lymph nodes in the neck 2: Productive cough and runny nose 3: Sore throat, swollen lymph nodes in the neck, pyrexia and purulent tonsils 4: Productive cough, pyrexia and pain on breathing | Two upper respiratory tract symptoms, and two lower, to allow exploration of differences in perception of ‘throat’ and ‘chest’ infections. Clinical guidelines [14,15], diagnostic criteria (such as FeverPAIN [35]) and practising clinicians were consulted to identify two plausible levels of severity for each, identified as ‘minor’ (1 and 2) and ‘serious’ (3 and 4) throughout this paper. |
| How long the person has had the symptoms when they see the primary care physician | 3 days 7 days 10 days | Durations identified from literature [8], to cover a wide yet realistic range for RTIs. |
| Relevant comorbidities of the patient b | 1. None 2. One 3. Two or more | Reflects clinical guideline CG69 [14], which identifies comorbidities as a risk factor for developing complications, and particularly for acute cough, increasing risk with additional comorbidities or other patient factors. |
| Length of the consultation with the primary care physician | 5 min 10 min 15 min | Proxy for quality of information exchange between primary care physician and patient. Levels represent plausible consultation durations; the longest consultation is intended to allow for use of tools such as TARGET patient leaflets [36] to explain treatment. |
| Patient opinion on taking antibiotics b | 1. Preference to have antibiotics 2. No preference expressed 3. Preference not to have antibiotics | Patient opinion can influence clinician choices [19,37]. Levels allow for patient preference in either direction, or neutral. |
| Risk of harm from not having antibiotic treatment straight away | 1% 10% 20% | The GP’s judgement of the risk of harm, explained as symptom persistence or recurrence, or complications. Shown as a percentage, as a graphic, and also described in words (‘In 1 case out of every 100 like this, the patient would…’). Levels identified from literature. Rates of complications typically range from <1% to 2% for RTIs in primary care studies without antibiotics [11,38,39,40]. Symptom persistence at follow-up in the case of acute bronchitis ranges from 18% to 35% in meta-analyses depending on the measure [41], with a reconsultation rate of ~20% for non-resolution for RTIs [10,21], without antibiotics. |
| Risk of an adverse effect from taking antibiotics | 1% 10% 20% | The GP’s judgement of the risk of adverse effect, explained as allergy, side effects, or future resistance. Shown in three formats, as above. Levels identified from literature and public information on rates of side effects and allergy [8,42]. |
| How a delayed prescription would be provided b | 1: prescription plus advice to delay collection of antibiotics 2: post-dated prescription 3: collect prescription from the practice reception at a later date | Policy relevance: these formats have been tested in clinical trials [11] and referred to in guidelines [14], but there are no quantitative data on clinician preferences. |
| Respondent Characteristic | N (Percentage) | Quota (%) # | |
|---|---|---|---|
| Sex | Male | 98 (54%) | 56 |
| Age (years) | 39 and under | 40 (22%) | 26 |
| 40–49 | 76 (42%) | 41 | |
| 50–59 | 50 (28%) | 24 | |
| 60 or over | 15 (8%) | 10 | |
| Median age | 46 | ||
| Country | England | 152 (84%) | 83 |
| Scotland | 17 (9%) | 10 | |
| Wales | 9 (5%) | 4.5 | |
| Northern Ireland | 3 (2%) | 2.5 | |
| Practice size | 1–2500 patients | 5 (3%) | 4 |
| 2501–5000 | 28 (15%) | 15 | |
| 5001–7500 | 40 (22%) | 20 | |
| 7501–10,000 | 35 (19%) | 20 | |
| 10,001–12,500 | 32 (18%) | 41 | |
| 12,501–15,000 | 14 (8%) | ||
| More than 15,000 patients | 27 (15%) | ||
| Role in practice | Partner | 96 (53%) | |
| Salaried GP | 57 (31%) | ||
| Locum | 28 (15%) | ||
| Level of local deprivation * | High | 49 (27%) | |
| Medium | 72 (40%) | ||
| Low | 56 (31%) | ||
| Practice’s level of antibiotic | Very low/Low | 36 (20%) | |
| prescribing compared to | Average | 100 (55%) | |
| similar practices * | Very high/high | 35 (19%) | |
| Usual format of delayed prescription * | Standard prescription with recommendation to wait | 145 (80%) | |
| Post-dated prescription | 23 (13%) | ||
| Electronic post-dated prescription | 7 (4%) | ||
| Prescription available from practice at future date | 4 (2%) | ||
| Other | 2 (1%) | ||
| RTI prescribing *: mean | An immediate antibiotic prescription (range) | 31% (1 to 90%) | |
| percentage of patients | A delayed antibiotic prescription (range) | 17% (0 to 85%) | |
| who leave with… | No antibiotic prescription (range) | 52% (0 to 95%) | |
| Found the survey * | Very easy/easy/quite easy | 90 (50%) | |
| Neither easy nor difficult | 52 (29%) | ||
| Very difficult/difficult/quite difficult | 39 (21%) | ||
| Attribute/Level | 1. Attributes Only | 2. Respondent Characteristics | |||
|---|---|---|---|---|---|
| Coefficient | 95% CI | Coefficient | 95% CI | ||
| Symptoms | Sore and red throat, and swollen lymph nodes in the neck (‘minor throat’) | 3.17 | 2.48 to 3.86 p < 0.001 | 3.17 | 2.48 to 3.86 p < 0.001 |
| Productive cough and runny nose (‘minor chest’) | 3.47 | 2.79 to 4.14 p < 0.001 | 3.47 | 2.79 to 4.14 p < 0.001 | |
| Sore throat, swollen lymph nodes in the neck, pyrexia and purulent tonsils (‘serious throat’) | −0.90 | −1.31 to −0.49 p < 0.001 | −0.90 | −1.31 to −0.49 p < 0.001 | |
| Productive cough, pyrexia and pain on breathing (‘serious chest’) a | 0 | - | 0 | - | |
| Symptom duration | Per day longer | −0.33 | −0.43 to −0.23 p < 0.001 | −0.33 | −0.43 to −0.23 p < 0.001 |
| Relevant comorbidities | None a | 0 | - | 0 | - |
| One | 0.05 | −0.31 to 0.42 p = 0.769 | 0.06 | −0.31 to 0.42 p = 0.762 | |
| Two or more | −1.18 | −1.64 to −0.72 p < 0.001 | −1.18 | −1.64 to −0.72 p < 0.001 | |
| Consultation length | Per minute longer | 0.05 | 0.02 to 0.09 p = 0.003 | 0.05 | 0.02 to 0.09 p = 0.003 |
| Patient opinion | Preference to have antibiotics | 0.39 | −0.72 to −0.05 p = 0.022 | −0.39 | −0.72 to −0.05 p = 0.023 |
| No preference expressed a | 0 | - | 0 | - | |
| Preference not to have antibiotics | 0.33 | 0.05 to 0.60 p = 0.020 | 0.33 | 0.05 to 0.60 p = 0.020 | |
| Risk of harm from not starting antibiotics | Per 1% higher | −0.13 | −0.17 to −0.10 p < 0.001 | −0.13 | −0.17 to −0.10 p < 0.001 |
| Risk of adverse effect from taking antibiotics | Per 1% higher | 0.03 | 0.01 to 0.05 p = 0.001 | 0.03 | 0.01 to 0.05 p = 0.001 |
| Format of the delayed prescription | Advice to delay a | 0 | - | 0 | - |
| Post-dated prescription | −0.03 | −0.37 to 0.31 p = 0.872 | −0.03 | −0.37 to 0.31 p = 0.872 | |
| Collect from practice | −0.43 | −0.82 to −0.08 p = 0.016 | −0.45 | −0.82 to −0.08 p = 0.016 | |
| Self-reported prescribing behaviour: percent immediate prescriptions for RTI | −0.02 | −0.04 to −0.01 p = 0.002 | |||
| Intercept | 2.23 | 1.49 to 2.97 p < 0.001 | 3.44 | 2.46 to 4.42 p < 0.001 | |
| Var(intercept) b | 1.57 | 0.96 to 2.57 | 1.41 | 0.88 to 2.28 | |
| Pseudo R2: attributes only | 0.61 | 0.62 | |||
| Pseudo R2: attributes and respondent-level effect | 0.65 | 0.66 | |||
| Akaike Information Criterion | 1955 | 1943 | |||
| Bayesian Information Criterion | 2043 | 2037 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morrell, L.; Buchanan, J.; Roope, L.S.J.; Pouwels, K.B.; Butler, C.C.; Hayhoe, B.; Moore, M.V.; Tonkin-Crine, S.; McLeod, M.; Robotham, J.V.; et al. Delayed Antibiotic Prescription by General Practitioners in the UK: A Stated-Choice Study. Antibiotics 2020, 9, 608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090608
Morrell L, Buchanan J, Roope LSJ, Pouwels KB, Butler CC, Hayhoe B, Moore MV, Tonkin-Crine S, McLeod M, Robotham JV, et al. Delayed Antibiotic Prescription by General Practitioners in the UK: A Stated-Choice Study. Antibiotics. 2020; 9(9):608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090608
Chicago/Turabian StyleMorrell, Liz, James Buchanan, Laurence S. J. Roope, Koen B. Pouwels, Christopher C. Butler, Benedict Hayhoe, Michael V. Moore, Sarah Tonkin-Crine, Monsey McLeod, Julie V. Robotham, and et al. 2020. "Delayed Antibiotic Prescription by General Practitioners in the UK: A Stated-Choice Study" Antibiotics 9, no. 9: 608. https://0-doi-org.brum.beds.ac.uk/10.3390/antibiotics9090608