
Effectiveness of a Selective Etching Technique in Reducing White Spots Formation around Lingual Brackets: A Prospective Cohort Clinical Study

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
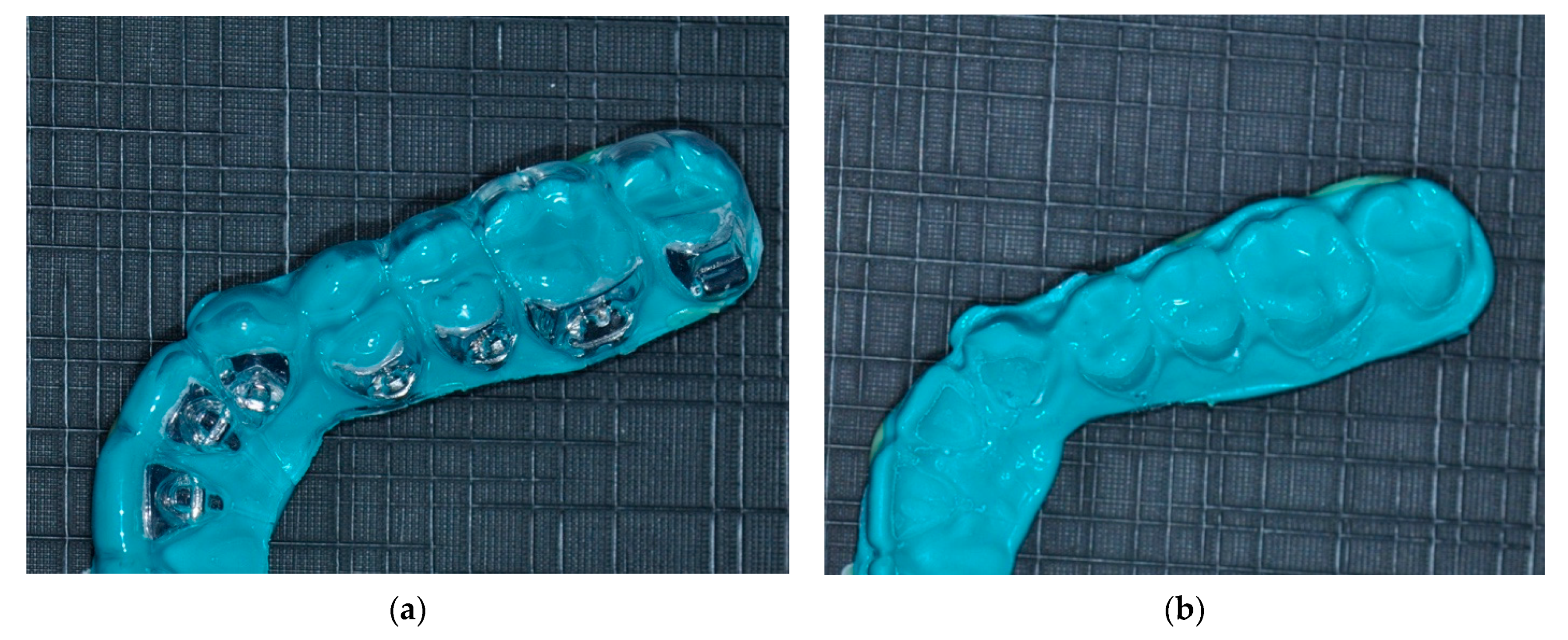
- A light-body (low viscosity) poly-vinyl siloxane (PVS) dental impression material (AcquasilTM Ultra LV, Dentsply Intl, York, PA, USA) was placed inside each indirect bonding transfer tray, paying attention to avoid the formation of any type of gap or air bubble, until filling it completely (Figure 1).
- After waiting the appropriate setting time, the PVS was removed, checked for impression precision, and an .STL file was generated using an intraoral scanner (CS3600, Carestream Dental, Atlanta, GA, USA).
- This .STL file was then printed in resin with a 3D printer (Formlabs Form 2), and it underwent vacuum thermoforming to thermoform a blue-colored polyethylene terephthalate (PET) thermoplastic sheet into an etching guide.
- The etching guide was completed making holes on the lingual/palatal teeth surface, exactly corresponding in shape, dimension, and position to the bracket base.
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Försch, M.; Krull, L.; Hechtner, M.; Rahimi, R.; Wriedt, S.; Wehrbein, H.; Jacobs, C.; Jacobs, C. Perception of esthetic orthodontic appliances: An eye tracking and cross-sectional study. Angle Orthod. 2020, 90, 109–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AlSeraidi, M.; Hansa, I.; Dhaval, F.; Ferguson, D.J.; Vaid, N.R. The effect of vestibular, lingual, and aligner appliances on the quality of life of adult patients during the initial stages of orthodontic treatment. Prog. Orthod. 2021, 22, 3. [Google Scholar] [CrossRef] [PubMed]
- Marañón-Vásquez, G.A.; Barreto, L.S.D.C.; Pithon, M.M.; Nojima, L.I.; Nojima, M.D.C.G.; Araújo, M.T.S.; Souza, M.M.G. Reasons influencing the preferences of prospective patients and orthodontists for different orthodontic appliances. Korean J. Orthod. 2021, 51, 115–125. [Google Scholar] [CrossRef] [PubMed]
- Antonio-Zancajo, L.; Montero, J.; Albaladejo, A.; Oteo-Calatayud, M.D.; Alvarado-Lorenzo, A. Pain and Oral-Health-Related Quality of Life in Orthodontic Patients During Initial Therapy with Conventional, Low-Friction, and Lingual Brackets and Aligners (Invisalign): A Prospective Clinical Study. J. Clin. Med. 2020, 9, 2088. [Google Scholar] [CrossRef]
- Massetti, F.; Dalessandri, D. Influence of attachment shape on rescanning accuracy in clear aligner therapy: An in vitro study. J. Align. Orth. in press.
- Knösel, M.; Klang, E.; Helms, H.J.; Wiechmann, D. Occurrence and severity of enamel decalcification adjacent to bracket bases and sub-bracket lesions during orthodontic treatment with two different lingual appliances. Eur. J. Orthod. 2016, 38, 485–492. [Google Scholar] [CrossRef] [Green Version]
- Silvestrini Biavati, A.; Gastaldo, L.; Dessì, M.; Silvestrini Biavati, F.; Migliorati, M. Manual orthodontic vs. oscillating-rotating electric toothbrush in orthodontic patients: A randomised clinical trial. Eur. J. Paediatr. Dent. 2010, 11, 200–202. [Google Scholar]
- Wiechmann, D.; Klang, E.; Helms, H.J.; Knösel, M. Lingual appliances reduce the incidence of white spot lesions during orthodontic multibracket treatment. Am. J. Orthod. Dentofac. Orthop. 2015, 148, 414–422. [Google Scholar] [CrossRef]
- Dalessandri, D.; Bindi, M.; Massetti, F.; Migliorati, M.; Isola, G.; Tonni, I.; Visconti, L.; Bonetti, S. Comparison of Gum® HydralTM Moisturizing gel and Biotene® Oral gel in dry mouth sensation reduction: A randomized clinical trial. BMC Oral Health. in press.
- Dalessandri, D. Reduction in incidence of white spot lesions with lingual appliances. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 7–8. [Google Scholar] [CrossRef] [Green Version]
- Dalessandri, D.; Lazzaroni, E.; Migliorati, M.; Piancino, M.G.; Tonni, I.; Bonetti, S. Self-ligating fully customized lingual appliance and chair-time reduction: A typodont study followed by a randomized clinical trial. Eur. J. Orthod. 2013, 35, 758–765. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Veen, M.H.; Attin, R.; Schwestka-Polly, R.; Wiechmann, D. Caries outcomes after orthodontic treatment with fixed appliances: Do lingual brackets make a difference? Eur. J. Oral. Sci. 2010, 118, 298–303. [Google Scholar] [CrossRef]
- Cozzani, M.; Menini, A.; Bertelli, A. Etching masks for precise indirect bonding. J. Clin. Orthod. 2010, 44, 326–330. [Google Scholar]
- Dalessandri, D.; Dalessandri, M.; Bonetti, S.; Visconti, L.; Paganelli, C. Effectiveness of an indirect bonding technique in reducing plaque accumulation around braces. Angle Orthod. 2012, 82, 313–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zotti, F.; Dalessandri, D.; Salgarello, S.; Piancino, M.; Bonetti, S.; Visconti, L.; Paganelli, C. Usefulness of an app in improving oral hygiene compliance in adolescent orthodontic patients. Angle Orthod. 2016, 86, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suresh, K. An overview of randomization techniques: An unbiased assessment of outcome in clinical research. J. Hum. Reprod. Sci. 2011, 4, 8–11. [Google Scholar] [CrossRef]
- Bruno, G.; De Stefani, A.; Pillan, M.; Balasso, P.; Mazzoleni, S.; Gracco, A.; Stellini, E. Vestibular and lingual orthodontics: Experimental study on plaque and blood indexes. Minerva Stomatol. 2019, 68, 285–290. [Google Scholar] [CrossRef]
- Migliorati, M.; Isaia, L.; Cassaro, A.; Rivetti, A.; Silvestrini-Biavati, F.; Gastaldo, L.; Piccardo, I.; Dalessandri, D.; Silvestrini-Biavati, A. Efficacy of professional hygiene and prophylaxis on preventing plaque increase in orthodontic patients with multibracket appliances: A systematic review. Eur. J. Orthod. 2015, 37, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Ay, Z.Y.; Sayin, M.O.; Ozat, Y.; Goster, T.; Atilla, A.O.; Bozkurt, F.Y. Appropriate oral hygiene motivation method for patients with fixed appliances. Angle Orthod. 2007, 77, 1085–1089. [Google Scholar] [CrossRef]
- Arici, S.; Alkan, A.; Arici, N. Comparison of different toothbrushing protocols in poor-toothbrushing orthodontic patients. Eur. J. Orthod. 2007, 29, 488–492. [Google Scholar] [CrossRef] [Green Version]
- Bock, N.C.; von Bremen, J.; Kraft, M.; Ruf, S. Plaque control effectiveness and handling of interdental brushes during multibracket treatment: A randomized clinical trial. Eur. J. Orthod. 2010, 32, 408–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, M.Y.; Busscher, H.J.; Evans, R.; Noar, J.; Pratten, J. Early biofilm formation and the effects of antimicrobial agents on orthodontic bonding materials in a parallel plate flow chamber. Eur. J. Orthod. 2006, 28, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Øgaard, B.; Alm, A.A.; Larsson, E.; Adolfsson, U. A prospective, randomized clinical study on the effects of an amine fluoride/stannous fluoride toothpaste/mouthrinse on plaque, gingivitis and initial caries lesion development in orthodontic patients. Eur. J. Orthod. 2006, 28, 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, P.E.; Pender, N.; Higham, S.M. Quantifying enamel demineralization from teeth with orthodontic brackets--a comparison of two methods. Part 1: Repeatability and agreement. Eur. J. Orthod. 2003, 25, 149–158. [Google Scholar] [CrossRef] [Green Version]
- Benson, P.E.; Pender, N.; Higham, S.M. Quantifying enamel demineralization from teeth with orthodontic brackets--a comparison of two methods. Part 2: Validity. Eur. J. Orthod. 2003, 25, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Livas, C.; Kuijpers-Jagtman, A.M.; Bronkhorst, E.; Derks, A.; Katsaros, C. Quantification of white spot lesions around orthodontic brackets with image analysis. Angle Orthod. 2008, 78, 585–590. [Google Scholar] [CrossRef] [Green Version]
- Tufekci, E.; Dixon, J.S.; Gunsolley, J.C.; Lindauer, S.J. Prevalence of white spot lesions during orthodontic treatment with fixed appliances. Angle Orthod. 2011, 81, 206–210. [Google Scholar] [CrossRef] [Green Version]
- Laffranchi, L.; Zotti, F.; Bonetti, S.; Dalessandri, D.; Fontana, P. Oral implications of the vegan diet: Observational study. Minerva Stomatol. 2010, 59, 583–591. [Google Scholar]
- Zotti, F.; Laffranchi, L.; Fontana, P.; Dalessandri, D.; Bonetti, S. Effects of fluorotherapy on oral changes caused by a vegan diet. Minerva Stomatol. 2014, 63, 179–188. [Google Scholar] [PubMed]
- Pender, N. Aspects of oral health in orthodontic patients. Br. J. Orthod. 1986, 13, 95–103. [Google Scholar] [CrossRef]
- O’Reilly, M.T.; De Jesús Viñas, J.; Hatch, J.P. Effectiveness of a sealant compared with no sealant in preventing enamel demineralization in patients with fixed orthodontic appliances: A prospective clinical trial. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 837–844. [Google Scholar] [CrossRef]
- Oz, A.Z.; Oz, A.A.; Yazicioglu, S.; Sancaktar, O. Effectiveness of an antibacterial primer used with adhesive-coated brackets on enamel demineralization around brackets: An in vivo study. Prog. Orthod. 2019, 20, 15. [Google Scholar] [CrossRef] [Green Version]
- Linjawi, A.I. Sealants and White Spot Lesions in Orthodontics: A Review. J. Contemp. Dent. Pract. 2020, 21, 808–814. [Google Scholar] [CrossRef] [PubMed]
- Ko-Adams, C.; Cioffi, I.; Dufour, D.; Nainar, S.M.H.; Lévesque, C.M.; Gong, S.G. Short-term effects of fixed orthodontic appliance on concentrations of mutans streptococci and persister cells in adolescents. Am. J. Orthod. Dentofac. Orthop. 2020, 157, 385–391. [Google Scholar] [CrossRef]
- Sheridan, J.J. The Readers’ Corner. 1. Do you use indirect bonding? J. Clin. Orthod. 2004, 38, 543–544. [Google Scholar]
- Kachoei, M.; Nourian, A.; Divband, B.; Kachoei, Z.; Shirazi, S. Zinc-oxide nanocoating for improvement of the antibacterial and frictional behavior of nickel-titanium alloy. Nanomedicine 2016, 11, 2511–2527. [Google Scholar] [CrossRef]
- Höchli, D.; Hersberger-Zurfluh, M.; Papageorgiou, S.N.; Eliades, T. Interventions for orthodontically induced white spot lesions: A systematic review and meta-analysis. Eur. J. Orthod. 2017, 39, 122–133. [Google Scholar] [CrossRef] [Green Version]
- Paula, A.B.; Fernandes, A.R.; Coelho, A.S.; Marto, C.M.; Ferreira, M.M.; Caramelo, F.; do Vale, F.; Carrilho, E. Therapies for white spot lesions—A systematic review. J. Evid. Based Dent. Pract. 2017, 17, 23–38. [Google Scholar] [CrossRef]
- Dalessandri, D.; Sangalli, L.; Tonni, I.; Laffranchi, L.; Bonetti, S.; Visconti, L.; Signoroni, A.; Paganelli, C. Attitude towards Telemonitoring in Orthodontists and Orthodontic Patients. Dent. J. 2021, 9, 47. [Google Scholar] [CrossRef]
- Bianco, A.; Dalessandri, D.; Oliva, B.; Isola, G.; Tonni, I.; Bonetti, S.; Visconti, L.; Paganelli, C. COVID-19 and Orthodontics: An approach for monitoring patients at home. Open Dent. J. 2021, 15, 87–96. [Google Scholar] [CrossRef]
- Chapman, J.A.; Roberts, W.E.; Eckert, G.J.; Kula, K.S.; González-Cabezas, C. Risk factors for incidence and severity of white spot lesions during treatment with fixed orthodontic appliances. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Degrazia, F.W.; Genari, B.; Leitune, V.C.B.; Arthur, R.A.; Luxan, S.A.; Samuel, S.M.W.; Collares, F.M.; Sauro, S. Polymerisation, antibacterial and bioactivity properties of experimental orthodontic adhesives containing triclosan-loaded halloysite nanotubes. J. Dent. 2018, 69, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Altmann, A.S.; Collares, F.M.; Leitune, V.C.; Samuel, S.M. The effect of antimicrobial agents on bond strength of orthodontic adhesives: A meta-analysis of in vitro studies. Orthod. Craniofac. Res. 2016, 19, 1–9. [Google Scholar] [CrossRef]
- Robles-Ruíz, J.J.; Ciamponi, A.L.; Medeiros, I.S.; Kanashiro, L.K. Effect of lingual enamel sandblasting with aluminum oxide of different particle sizes in combination with phosphoric acid etching on indirect bonding of lingual brackets. Angle Orthod. 2014, 84, 1068–1073. [Google Scholar] [CrossRef]
- Wiechmann, D. Lingual orthodontics (Part 3): Intraoral sandblasting and indirect bonding. J. Orofac. Orthop. 2000, 61, 280–291. [Google Scholar] [CrossRef]
- Baumgartner, S.; Koletsi, D.; Verna, C.; Eliades, T. The effect of enamel sandblasting on enhancing bond strength of orthodontic brackets: A systematic review and meta-analysis. J. Adhes Dent. 2017, 19, 463–473. [Google Scholar] [PubMed]
- Robles-Ruíz, J.J.; Arana-Chavez, V.E.; Ciamponi, A.L.; Abrão, J.; Kanashiro, L.K. Effects of sandblasting before orthophosphoric acid etching on lingual enamel: In-vitro roughness assessment. Am. J. Orthod. Dentofac. Orthop. 2015, 147, S76–S81. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Clinical Presentation |
|---|---|
| 0 | No plaque |
| 1 | Plaque accumulation on one bracket base margin |
| 2 | Plaque accumulation on two bracket base margins |
| 3 | Plaque accumulation on three bracket base margins |
| 4 | Plaque accumulation on four bracket base margins |
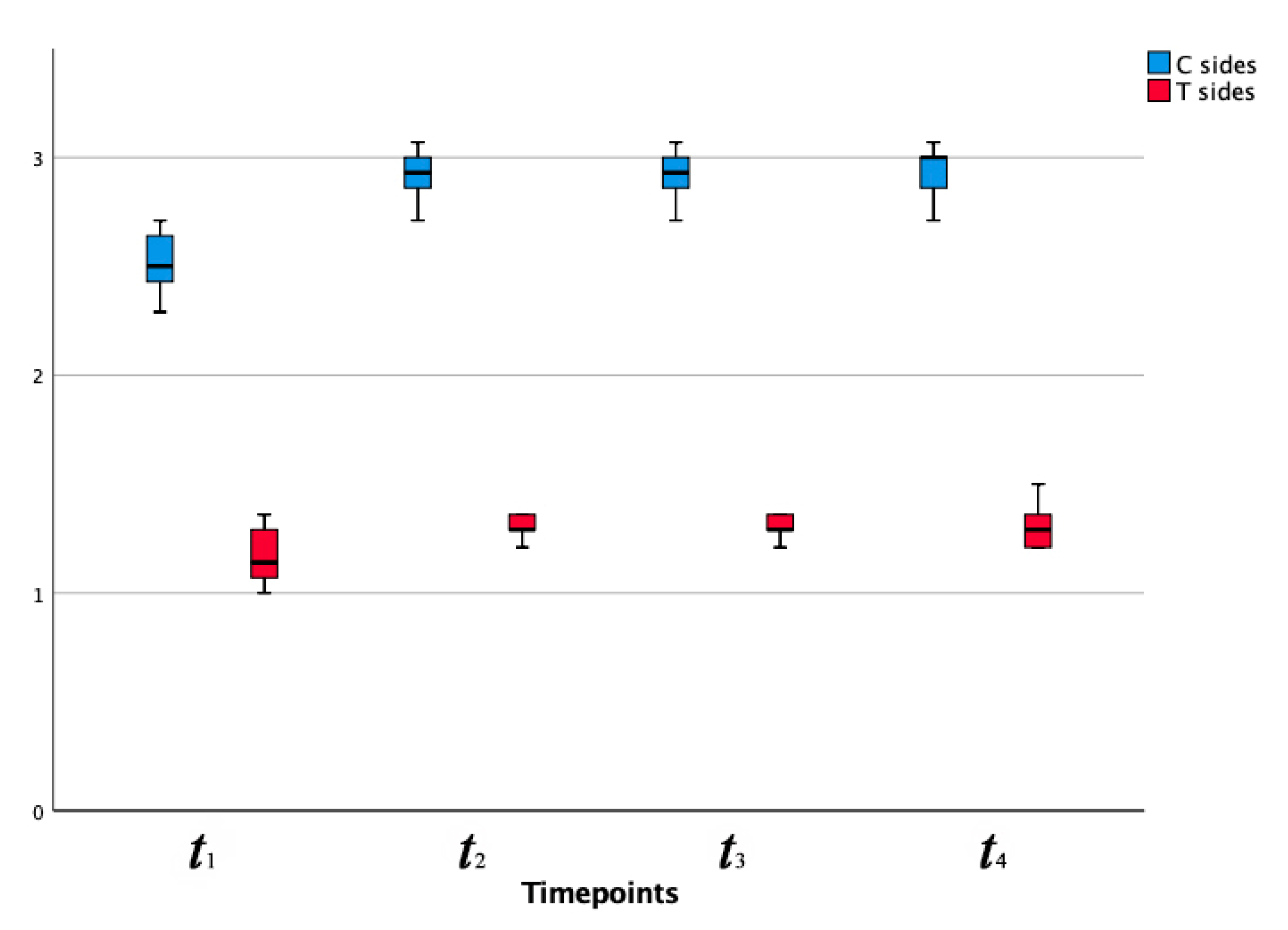
| Timepoint | C | T | p Value C vs. T |
|---|---|---|---|
| t1 | 2.51 (0.14) | 1.17 (0.13) | 0.00 **** |
| t2 | 2.92 (0.13) | 1.30 (0.06) | 0.00 **** |
| t3 | 2.93 (0.13) | 1.30 (0.05) | 0.00 **** |
| t4 | 2.93 (0.12) | 1.31 (0.07) | 0.00 **** |
| C | p value t1 vs. t2 | p value t2 vs. t3 | p value t3 vs. t4 |
| 0.00 **** | 0.16 | 0.08 | |
| T | p value t1 vs. t2 | p value t2 vs. t3 | p value t3 vs. t4 |
| 0.01 ** | 0.56 | 0.16 |
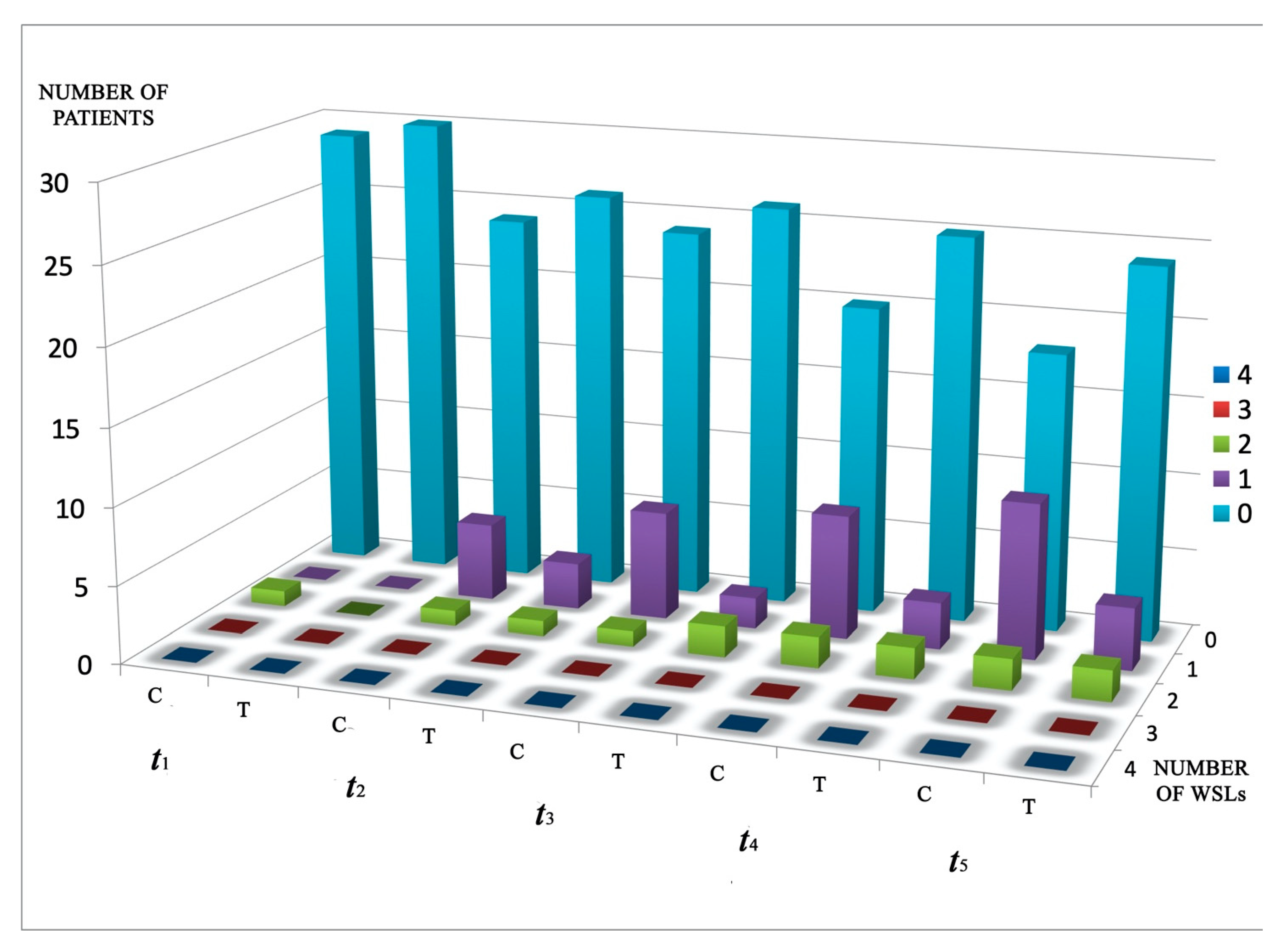
| Timepoint | C | T | p Value C vs. T |
|---|---|---|---|
| t1 | 1 | 0 | 0.31 |
| t2 | 6 | 4 | 0.49 |
| t3 | 8 | 4 | 0.20 |
| t4 | 10 | 5 | 0.14 |
| t5 | 12 | 6 | 0.02 * |
| C | |||
| p value t1 vs. t2 0.06 | p value t1 vs. t3 | p value t1 vs. t4 | p value t1 vs. t5 |
| 0.02 * | 0.00 ** | 0.00 *** | |
| T | |||
| p value t1 vs. t2 0.00 **** | p value t2 vs. t3 | p value t2 vs. t4 | p value t2 vs. t5 |
| 1 | 1 | 0.50 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dalessandri, D.; Bindi, M.; Massetti, F.; Isola, G.; Migliorati, M.; Visconti, L.; Paganelli, C.; Bonetti, S. Effectiveness of a Selective Etching Technique in Reducing White Spots Formation around Lingual Brackets: A Prospective Cohort Clinical Study. Coatings 2021, 11, 572. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings11050572
Dalessandri D, Bindi M, Massetti F, Isola G, Migliorati M, Visconti L, Paganelli C, Bonetti S. Effectiveness of a Selective Etching Technique in Reducing White Spots Formation around Lingual Brackets: A Prospective Cohort Clinical Study. Coatings. 2021; 11(5):572. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings11050572
Chicago/Turabian StyleDalessandri, Domenico, Marino Bindi, Francesca Massetti, Gaetano Isola, Marco Migliorati, Luca Visconti, Corrado Paganelli, and Stefano Bonetti. 2021. "Effectiveness of a Selective Etching Technique in Reducing White Spots Formation around Lingual Brackets: A Prospective Cohort Clinical Study" Coatings 11, no. 5: 572. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings11050572