
Role of Neonatal Biomarkers of Exposure to Psychoactive Substances to Identify Maternal Socio-Demographic Determinants

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Neonatal Biomarkers Testing
2.2.1. Meconium Toxicology Testing for Analysis of Illicit Drugs
2.2.2. Meconium Toxicology Testing for Analysis of EtG
2.2.3. Urine and Hair Toxicology Testing for Analysis of Illicit Drugs
2.3. Data Collection
2.4. Data Analyses
3. Results
3.1. Neonatal Biomarkers Testing
3.2. Sociodemographic Profiles Associated with Prenatal Exposure to Psychoactive Substances
3.2.1. Age
3.2.2. Lack of Adequate Pregnancy Care
3.2.3. Previous Abortions
3.2.4. Single Mother
3.2.5. Academic Level
3.2.6. Self-Reported Tobacco Smoking and Licit Drug Use
3.2.7. Referral to Social Services and Custody withdrawal
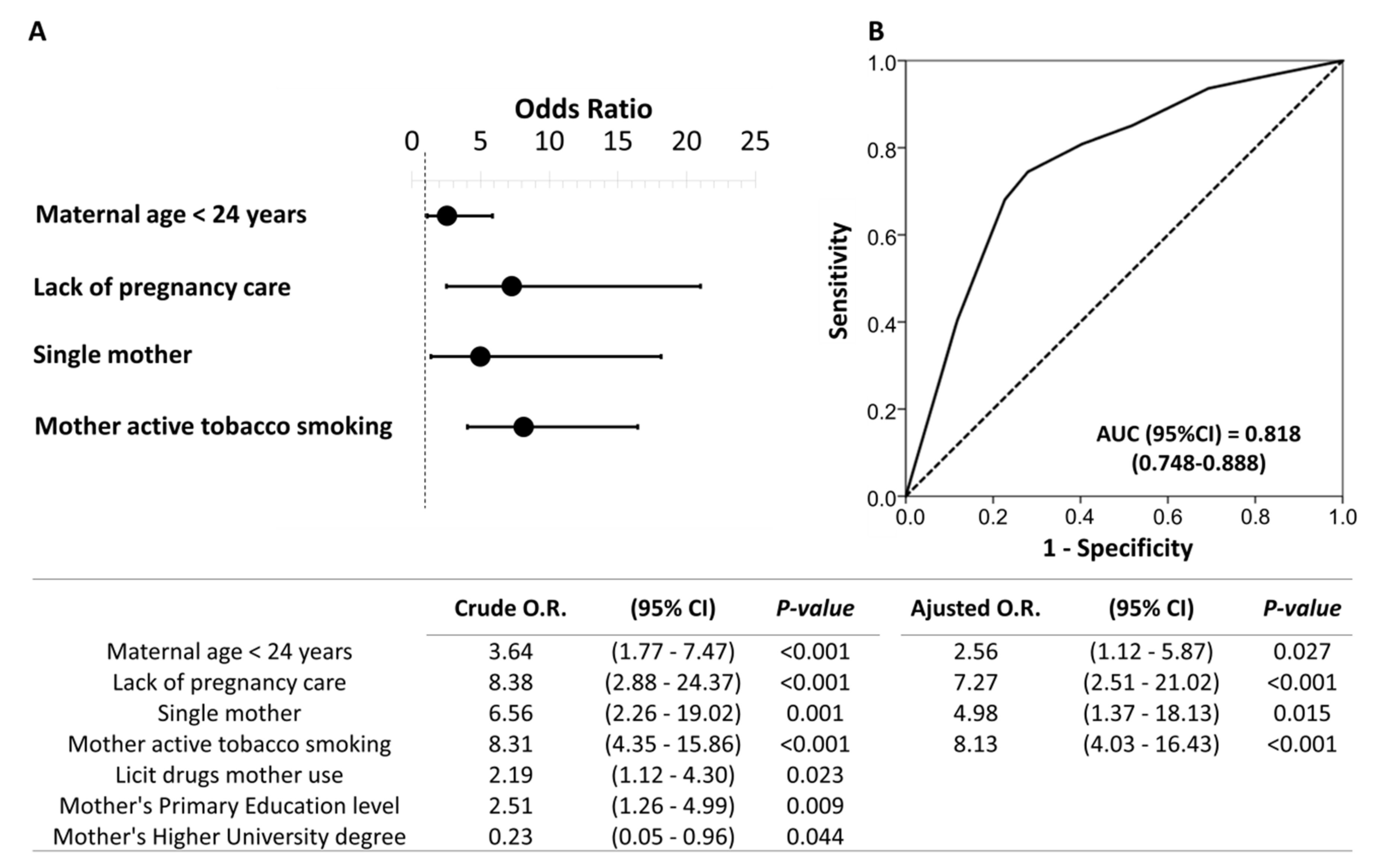
3.3. Independent Sociodemographic Risk Factors Associated with Prenatal Exposure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cook, J.L.; Green, C.R.; de la Ronde, S.; Dell, C.A.; Graves, L.; Ordean, A.; Ruiter, J.; Steeves, M.; Wong, S. Epidemiology and Effects of Substance Use in Pregnancy. J. Obstet. Gynaecol. Can. 2017, 39, 906–915. [Google Scholar] [CrossRef]
- Behnke, M.; Smith, V.C. Prenatal substance abuse: Short- and long-term effects on the exposed fetus. Pediatrics 2013, 131, e1009–e1024. [Google Scholar] [CrossRef] [Green Version]
- Ross, E.J.; Graham, D.L.; Money, K.M.; Stanwood, G.D. Developmental consequences of fetal exposure to drugs: What we know and what we still must learn. Neuropsychopharmacology 2015, 40, 61–87. [Google Scholar] [CrossRef] [PubMed]
- Luisa, M.; Navinés, R.; Gelabert, E.; Fonseca, F.; Gutierrez-zotes, A.; Guillamat, R.; Langohr, K.; Canellas, F.; Gornemann, I.; Costas, J.; et al. Substance use during pregnancy and personality dimensions [Consumo de substancias durante el embarazo y dimensiones de personalidad]. Adicciones 2020. Online ahead of print. [Google Scholar] [CrossRef]
- Lozano, J.; García-Algar, O.; Vall, O.; De La Torre, R.; Scaravelli, G.; Pichini, S. Biological matrices for the evaluation of in utero exposure to drugs of abuse. Ther. Drug Monit. 2007, 29, 711–734. [Google Scholar] [CrossRef]
- Hasin, D.S.; O’Brien, C.P.; Auriacombe, M.; Borges, G.; Bucholz, K.; Budney, A.; Compton, W.M.; Crowley, T.; Ling, W.; Petry, N.M.; et al. DSM-5 Criteria for Substance Use Disorders: Recommendations and Rationale. Am. J. Psychiatry 2013, 170, 834–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshaarawy, O.; Anthony, J.C. Cannabis use among women of reproductive age in the United States: 2002–2017. Addict. Behav. 2019, 99, 106082. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services; Substance Abuse and Mental Health Services Administration Center for Behavioral Health Statistics and Quality. Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings; NSDUH Series H-48; HHS Publication No. (SMA) 14-4863: Rockville, MD, USA, 2014.
- Memo, L.; Gnoato, E.; Caminiti, S.; Pichini, S.; Tarani, L. Fetal alcohol spectrum disorders and fetal alcohol syndrome: The state of the art and new diagnostic tools. Early Hum. Dev. 2013, 89, S40–S43. [Google Scholar] [CrossRef]
- Hoyme, H.E.; Kalberg, W.O.; Elliott, A.J.; Blankenship, J.; Buckley, D.; Marais, A.S.; Manning, M.A.; Robinson, L.K.; Adam, M.P.; Abdul-Rahman, O.; et al. Updated clinical guidelines for diagnosing fetal alcohol spectrum disorders. Pediatrics 2016, 138, e20154256. [Google Scholar] [CrossRef] [Green Version]
- Cook, J.L.; Green, C.R.; Lilley, C.M.; Anderson, S.M.; Baldwin, M.E.; Chudley, A.E.; Conry, J.L.; LeBlanc, N.; Loock, C.A.; Lutke, J.; et al. Fetal alcohol spectrum disorder: A guideline for diagnosis across the lifespan. CAMJ 2016, 188, 191–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pichini, S.; Puig, C.; Zuccaro, P.; Marchei, E.; Pellegrini, M.; Murillo, J.; Vall, O.; Pacifici, R.; García-Algar, O. Assessment of exposure to opiates and cocaine during pregnancy in a Mediterranean city: Preliminary results of the “Meconium Project”. Forensic Sci. Int. 2005, 153, 59–65. [Google Scholar] [CrossRef] [PubMed]
- García-Algar, O.; Vall Combelles, O.; Puig Sola, C.; Mur Sierra, A.; Scaravelli, G.; Pacifici, R.; Monleón Getino, T.; Pichini, S. Exposición prenatal a drogas de abuso a través del análisis de meconio en una población de bajo nivel socioeconómico en Barcelona. An. Pediatr. (Barc.) 2009, 70, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Lendoiro, E.; González-Colmenero, E.; Concheiro-Guisán, A.; de Castro, A.; Cruz, A.; López-Rivadulla, M.; Concheiro, M. Maternal Hair Analysis for the Detection of Illicit Drugs, Medicines, and Alcohol Exposure During Pregnancy. Ther. Drug Monit. 2013, 35, 296–304. [Google Scholar] [CrossRef]
- Garcia-Algar, O.; Kulaga, V.; Gareri, J.; Koren, G.; Vall, O.; Zuccaro, P.; Pacifici, R.; Pichini, S. Alarming Prevalence of Fetal Alcohol Exposure in a Mediterranean City. Ther. Drug Monit. 2008, 30, 249–254. [Google Scholar] [CrossRef]
- Pichini, S.; Pellegrini, M.; Gareri, J.; Koren, G.; Garcia-Algar, O.; Vall, O.; Vagnarelli, F.; Zuccaro, P.; Marchei, E. Liquid chromatography–tandem mass spectrometry for fatty acid ethyl esters in meconium: Assessment of prenatal exposure to alcohol in two European cohorts. J. Pharm. Biomed. Anal. 2008, 48, 927–933. [Google Scholar] [CrossRef] [PubMed]
- Consell de Mallorca. Pla Sobre Drogodependències i Altres Addiccions de Mallorca. 2015. Available online: https://www.imasmallorca.net/sites/default/files/2015-PlasobreDroguesiAltresAddiccionsdeMallorca%28aprovat%29_2.pdf (accessed on 31 January 2021).
- Perlman, N.C.; Cantonwine, D.E.; Smith, N.A. Toxicology Testing in Pregnancy. Obstet. Gynecol. 2020, 136, 607–609. [Google Scholar] [CrossRef] [PubMed]
- Ecker, J.; Abuhamad, A.; Hill, W.; Bailit, J.; Bateman, B.T.; Berghella, V.; Blake-Lamb, T.; Guille, C.; Landau, R.; Minkoff, H.; et al. Substance use disorders in pregnancy: Clinical, ethical, and research imperatives of the opioid epidemic: A report of a joint workshop of the Society for Maternal-Fetal Medicine, American College of Obstetricians and Gynecologists, and American Society of. Am. J. Obstet. Gynecol. 2019, 221, B5–B28. [Google Scholar] [CrossRef] [Green Version]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Guía de Práctica Clínica de Atención en el Embarazo y Puerperio; Agencia de Evaluación de Tecnologías Sanitarias de Andalucía: Madrid, Spain, 2014.
- Committee Opinion No. 633. Alcohol abuse and other substance use disorders: Ethical issues in obstetric and gynecologic practice. Obs. Gynecol. 2015, 125, 1529–1537. [CrossRef]
- Price, H.R.; Collier, A.C.; Wright, T.E. Screening Pregnant Women and Their Neonates for Illicit Drug Use: Consideration of the Integrated Technical, Medical, Ethical, Legal, and Social Issues. Front. Pharmacol. 2018, 9, 961. [Google Scholar] [CrossRef]
- Cotten, S.W. Drug Testing in the Neonate. Clin. Lab. Med. 2012, 32, 449–466. [Google Scholar] [CrossRef]
- Colby, J.M.; Cotton, S.W. Facing Challenges in Neonatal Drug Testing. How Laboratory Stewardship Enhances Care for a Vulnerable Population. Clinical Laboratory News AACC. 2018. Available online: https://www.aacc.org/cln/articles/2018/march/facing-challenges-in-neonatal-drug-testing (accessed on 31 January 2021).
- Jarque, P.; Marchei, E.; Roca, A.; Gomila, I.; Pichini, S.; Busardò, F.P.; Barceló, B. The importance of biomarkers of fetal exposure to alcohol and psychotropic drugs in early diagnosis: A case report. Drug Test. Anal. 2018, 10, 895–898. [Google Scholar] [CrossRef] [PubMed]
- ElSohly, M.A.; Stanford, D.F.; Murphy, T.P.; Lester, B.M.; Wright, L.L.; Smeriglio, V.L.; Verter, J.; Bauer, C.R.; Shankaran, S.; Bada, H.S.; et al. Immunoassay and GC-MS Procedures for the Analysis of Drugs of Abuse in Meconium. J. Anal. Toxicol. 1999, 23, 436–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jarque, P.; Roca, A.; Gomila, I.; Noce, V.; Barcelo, B.; Klein, J. Quantification of Methamphetamine «Shabu» in Biological Matrices to Detect Prenatal Exposure: A Case Report and a Literature Review. Curr. Pharm. Biotechnol. 2018, 19, 163–174. [Google Scholar] [CrossRef]
- Lopez, P.; Bermejo, A.M.; Tabernero, M.J.; Cabarcos, P.; Alvarez, I.; Fernandez, P. Cocaine and Opiates Use in Pregnancy: Detection of Drugs in Neonatal Meconium and Urine. J. Anal. Toxicol. 2009, 33, 351–355. [Google Scholar] [CrossRef] [Green Version]
- Tynon, M.; Porto, M.; Logan, B.K. Simplified Analysis of 11-Hydroxy-Delta-9-Tetrahydrocannabinol and 11-Carboxy-Delta-9-Tetrahydrocannabinol in Human Meconium: Method Development and Validation. J. Anal. Toxicol. 2015, 39, 35–40. [Google Scholar] [CrossRef] [Green Version]
- Malaca, S.; Marchei, E.; Barceló Martín, B.; Minutillo, A.; Pichini, S. Novel fast ultra-performance liquid chromatography–tandem mass spectrometry (UHPLC–MS/MS) and extraction of ethylglucuronide in meconium samples. Drug Test. Anal. 2019, 11, 1471–1475. [Google Scholar] [CrossRef]
- Himes, S.K.; Dukes, K.A.; Tripp, T.; Petersen, J.M.; Raffo, C.; Burd, L.; Odendaal, H.; Elliott, A.J.; Hereld, D.; Signore, C.; et al. Clinical sensitivity and specificity of meconium fatty acid ethyl ester, ethyl glucuronide, and ethyl sulfate for detecting maternal drinking during pregnancy. Clin. Chem. 2015, 61, 523–532. [Google Scholar] [CrossRef]
- Wasels, R.; Belleville, F. Gas chromatographic-mass spectrometric procedures used for the identification and determination of morphine, codeine and 6-monoacetylmorphine. J. Chromatogr. A 1994, 674, 225–234. [Google Scholar] [CrossRef]
- Gomila, I.; Barceló, B.; Rosell, A.; Avella, S.; Sahuquillo, L.; Dastis, M. Cross-Reactivity of Pantoprazole with Three Commercial Cannabinoids Immunoassays in Urine. J. Anal. Toxicol. 2017, 41, 760–764. [Google Scholar] [CrossRef]
- Marchei, E.; Colone, P.; Nastasi, G.G.; Calabrò, C.; Pellegrini, M.; Pacifici, R.; Zuccaro, P.; Pichini, S. On-site screening and GC–MS analysis of cocaine and heroin metabolites in body-packers urine. J. Pharm Biomed. Anal. 2008, 48, 383–387. [Google Scholar] [CrossRef]
- Cone, E.J.; Yousefnejad, D.; Darwin, W.D.; Maguire, T. Testing Human Hair for Drugs of Abuse. II. Identification of Unique Cocaine Metabolites in Hair of Drug Abusers and Evaluation of Decontamination Procedures. J. Anal. Toxicol. 1991, 15, 250–255. [Google Scholar] [CrossRef] [Green Version]
- Moore, C.; Guzaldo, F.; Donahue, T. The Determination of 11-nor- 9-Tetrahydrocannabinol-9-Carboxylic Acid (THC-COOH)in Hair using Negative Ion Gas Chromatography-Mass Spectrometry and High-Volume Injection. J. Anal. Toxicol. 2001, 25, 555–558. [Google Scholar] [CrossRef]
- Friguls, B.; Joya, X.; Garcia-Serra, J.; Gómez-Culebras, M.; Pichini, S.; Martinez, S.; Vall, O.; Garcia-Algar, O. Assessment of exposure to drugs of abuse during pregnancy by hair analysis in a Mediterranean island. Addiction 2012, 107, 1471–1479. [Google Scholar] [CrossRef]
- Hetea, A.; Cosconel, C.; Stanescu, A.A.M.; Simionescu, A.A. Alcohol and Psychoactive Drugs in Pregnancy. Maedica (Buchar) 2019, 14, 397–401. [Google Scholar] [CrossRef]
- European Monitoring Centre for Drugs and drug Addiction. Pregnancy, Childcare and the Family: Key Issues for Europes Response to Drugs [Internet]. 2012. Available online: http://www.emcdda.europa.eu/system/files/publications/671/TDSI12001ENC_396469.PDF (accessed on 31 January 2021).
- European Monitoring Centre for Drugs and Drug Addiction. Informe Sobre Drogas 2019: España. 2019. Available online: https://www.emcdda.europa.eu/system/files/publications/11364/20191724_TDAT19001ESN_PDF.pdf (accessed on 31 January 2021).
- Lozano, J.; García-Algar, O.; Marchei, E.; Vall, O.; Monleon, T.; Giovannandrea, R.D.; Pichin, S. Prevalence of gestational exposure to cannabis in a Mediterranean city by meconium analysis. Acta Paediatr. Int. J. Paediatr. 2007, 96, 1734–1737. [Google Scholar] [CrossRef] [PubMed]
- García-Serra, J.; Ramis, J.; Simó, S.; Joya, X.; Pichini, S.; Vall, O.; García-Algar, O. Matrices biológicas alternativas para detectar la exposición prenatal a drogas de abuso en el tercer trimestre de la gestación. An. Pediatr. (Barc.) 2012, 77, 323–328. [Google Scholar] [CrossRef]
- Gomez-Roig, M.D.; Marchei, E.; Sabra, S.; Busardò, F.P.; Mastrobattista, L.; Pichini, S.; Gratacós, E.; Garcia-Algar, O. Maternal hair testing to disclose self-misreporting in drinking and smoking behavior during pregnancy. Alcohol 2018, 67, 1–6. [Google Scholar] [CrossRef]
- Concheiro, M.; Lendoiro, E.; de Castro, A.; Gónzalez-Colmenero, E.; Concheiro-Guisan, A.; Peñas-Silva, P.; Macias-Cortiña, M.; Cruz-Landeira, A.; López-Rivadulla, M. Bioanalysis for cocaine, opiates, methadone, and amphetamines exposure detection during pregnancy. Drug Test. Anal. 2017, 9, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Manich, A.; Velasco, M.; Joya, X.; García-Lara, N.R.; Pichini, S.; Vall, O.; García-Algar, O. Validity of a maternal alcohol consumption questionnaire in detecting prenatal exposure. An. Pediatr. 2012, 76, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Joya, X.; Gomez-Culebras, M.; Callejón, A.; Friguls, B.; Puig, C.; Ortigosa, S.; Morini, L.; Garcia-Algar, O.; Vall, O. Cocaine use during pregnancy assessed by hair analysis in a Canary Islands cohort. BMC Pregnancy Childbirth 2012, 12, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morini, L.; Marchei, E.; Vagnarelli, F.; Garcia Algar, O.; Groppi, A.; Mastrobattista, L.; Pichini, S. Ethyl glucuronide and ethyl sulfate in meconium and hair-potential biomarkers of intrauterine exposure to ethanol. Forensic Sci. Int. 2010, 196, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Joya, X.; Marchei, E.; Salat-Batlle, J.; García-Algar, O.; Calvaresi, V.; Pacifici, R.; Pichini, S. Fetal exposure to ethanol: Relationship between ethyl glucuronide in maternal hair during pregnancy and ethyl glucuronide in neonatal meconium. Clin. Chem. Lab. Med. 2016, 54, 427–435. [Google Scholar] [CrossRef]
- Jackson, M.A.; Baker, A.L.; McCarter, K.L.; Brown, A.L.; Gould, G.S.; Dunlop, A.J. Interventions for pregnant women who use tobacco and other substances: A systematic review protocol. BMJ Open 2019, 9, e032449. [Google Scholar] [CrossRef] [Green Version]
- Ryan, S.A.; Ammerman, S.D.; O’Connor, M.E.; Committee on Substance Use and Prevention and Section on Breastfeeding. Marijuana use during pregnancy and breastfeeding: Implications for neonatal and childhood outcomes. Pediatrics 2018, 142, e20181889. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koren, G.; Cohen, R. The use of cannabis for Hyperemesis Gravidarum (HG). J. Cannabis Res. 2020, 2, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberson, E.K.; Patrick, W.K.; Hurwitz, E.L. Marijuana use and maternal experiences of severe nausea during pregnancy in Hawai’i. Hawaii J. Med. Public Health 2014, 73, 283–287. [Google Scholar] [PubMed]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Plan de Acción Sobre Adicciones 2018–2020. Secretaría General Técnica. Centro de Publicaciones Delegación del Gobierno para el Plan Nacional sobre Drogas. Available online: https://pnsd.sanidad.gob.es/pnsd/planAccion/docs/PLAD_2018-2020_FINAL.pdf (accessed on 31 January 2021).
- Delano, K.; Koren, G. Emerging Biomarkers of Intrauterine Neonatal and Pediatric Exposures to Xenobiotics. Pediatr. Clin. N. Am. 2012, 59, 1059–1070. [Google Scholar] [CrossRef] [PubMed]
- Gómez Roig, M.D.; García-Algar, O. Crecimiento intrauterino restringido: ¿problema de definición o de contenido? An. Pediatr. 2011, 75, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Ostrea, E.M.; Knapp, D.K.; Tannenbaum, L.; Ostrea, A.R. Estimates of illicit drug use during pregnancy by maternal interview, hair analysis, and meconium analysis. J. Pediatr. 2001, 138, 344–348. [Google Scholar] [CrossRef] [PubMed]
- McQueen, K.; Murphy-Oikonen, J. Neonatal abstinence syndrome. N. Engl. J. Med. 2016, 375, 2468–2479. [Google Scholar] [CrossRef] [PubMed]
- De Santis, M.; De Luca, C.; Mappa, I.; Quattrocchi, T.; Angelo, L.; Cesari, E. Smoking, alcohol consumption and illicit drug use in an Italian population of pregnant women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 159, 106–110. [Google Scholar] [CrossRef]
- Chiandetti, A.; Hernandez, G.; Mercadal-Hally, M.; Alvarez, A.; Andreu-Fernandez, V.; Navarro-Tapia, E.; Bastons-Compta, A.; Garcia-Algar, O. Prevalence of prenatal exposure to substances of abuse: Questionnaire versus biomarkers. Reprod. Health. 2017, 14, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Alonso, M.; González-Mesa, E.; Montes, M.G.; Bravo, I.L.; Galdón, F.M.; Campos, F.C.; Marín Schiaffino, G.; Pérez Torres, S.; Herrera Peral, J.; Bellido Estévez, I. Exposición a tabaco, alcohol y drogas de abuso en gestantes. Estudio de prevalencia en gestantes de Málaga (España). Adicciones 2015, 27, 99–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schempf, A.H.; Strobino, D.M. Drug use and limited prenatal care: An examination of responsible barriers. Am. J. Obs. Gynecol. 2009, 200, 412.e1–412.e10. [Google Scholar] [CrossRef] [PubMed]
- Ortigosa Gómez, S.; López-Vilchez, M.A.; Díaz Ledo, F.; Castejón Ponce, E.; Caballero Rabasco, A.; Carreras Collado, R.; Mur Sierra, A. Consumo de drogas durante la gestación y su repercusión neonatal. Análisis de los períodos 1982–1988 y 2002–2008. Med. Clin. 2011, 136, 423–430. [Google Scholar] [CrossRef]
- Oga, E.A.; Mark, K.; Coleman-Cowger, V. Cigarette Smoking Status and Substance Use in Pregnancy. Matern. Child. Health J. 2019, 22, 1477–1483. [Google Scholar] [CrossRef]
- Brown, R.A.; Dakkak, H.; Gilliland, J.; Seabrook, J.A. Predictors of drug use during pregnancy: The relative effects of socioeconomic, demographic, and mental health risk factors. J. Neonatal Perinat. Med. 2019, 12, 179–187. [Google Scholar] [CrossRef]
- Grywacheski, V.; Ali, J.; Baker, M.M.; Gheorghe, M.; Wong, S.L.; Orpana, H.M. Opioid and Cannabis Use During Pregnancy and Breastfeeding in Relation to Sociodemographics and Mental Health Status: A Descriptive Study. J. Obstet. Gynaecol. Can. 2020, 43, 329–336. [Google Scholar] [CrossRef]
- Garcia Garcia, J.; Campistol Mas, E.; López-Vilchez, M.Á.; Morcillo Buscato, M.J.; Mur Sierra, A. Análisis del maltrato prenatal en Cataluña entre los años 2011 y 2014. An. Pediatr. 2018, 88, 122–126. [Google Scholar] [CrossRef]
- Houston-Ludlam, A.N.; Bucholz, K.K.; Grant, J.D.; Waldron, M.; Madden, P.A.F.; Heath, A.C. The interaction of sociodemographic risk factors and measures of nicotine dependence in predicting maternal smoking during pregnancy. Drug Alcohol Depend. 2019, 198, 168–175. [Google Scholar] [CrossRef]
- Son, S.L.; Guiahi, M.; Heyborne, K.D. Historical and clinical factors associated with positive urine toxicology screening on labor and delivery. Eur J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Hans, S.L. Demographic and psychosocial characteristics of substance-abusing pregnant women. Clin. Perinatol. 1999, 26, 55–74. [Google Scholar] [CrossRef]


{kind=link}
| Variable [n (%)] | All Cases (n = 372) | Negative Toxicology (n = 323) | Positive Toxicology (n = 49) | Positive Only for Cannabis (n = 24) | Positive Only for EtG (n = 11) | Positive Only for Cocaine (n = 6) | Positive for More Than One Drug (n = 8) |
|---|---|---|---|---|---|---|---|
| Maternal age (years, mean ± SD) | 32.4 ± 6.3 | 32.8 ± 6.2 | 29.7 ± 6.6 * | 27.0 ± 5.7 *ab | 33.3 ± 7.6 | 33.2 ± 6.5 | 30.0 ± 5.0 |
| Paternal age (years, mean ± SD) | 35.1 ± 6.8 | 35.3 ± 6.7 | 33.7 ± 7.2 | 30.9 ± 7.3 *b | 35.8 ± 8.1 | 39.0 ± 4.4 | 33.8 ± 3.3 |
| Adequate pregnancy care | 351 (94.4) | 313 (96.9) | 38 (77.6) * | 22 (91.7) b | 10 (90.9) | 3 (50.0) * | 3 (37.5) * |
| Previous abortions | 146 (39.2) | 122 (37.8) | 24 (49.0) | 7 (29.2) | 6 (54.5) | 4 (66.7) | 7 (87.5) * |
| Self-reported mother’s use | |||||||
| Tobacco | 77 (20.7) | 48 (14.9) | 29 (59.2) * | 16 (66.7) * | 4 (36.4) | 2 (33.3) | 7 (87.5) * |
| Licit drugs | 69 (18.5) | 54 (16.8) | 15 (30.6) * | 5 (20.8) | 4 (36.4) | 1 (16.7) | 5 (62.5) * |
| Self-reported father’s use | |||||||
| Tobacco | 108 (29.0) | 83 (26.5) | 25 (59.5) * | 16 (80.0) * | 2 (18.2) | 3 (60.0) | 4 (66.7) * |
| Single mother | 15 (4.0) | 8 (2.5) | 7 (14.3) * | 4 (16.7) * | 0 (0) | 1 (16.7) | 2 (25.0) * |
| Mother’s academic level | |||||||
| Primary education | 215 (57.8) | 178 (55.1) | 37 (75.5) * | 22 (91.7) *a | 4 (36.4) | 5 (83.3) | 6 (75.0) |
| Vocational education and training | 52 (14.0) | 46 (14.2) | 6 (12.2) | 2 (8.3) | 2 (18.2) | 0 (0) | 2 (25.0) |
| Bachelor’s degree | 52 (14.0) | 48 (14.9) | 4 (8.2) | 0 (0.0) a | 3 (27.3) | 1 (16.7) | 0 (0) |
| Higher university degree | 53 (14.2) | 51 (15.8) | 2 (4.1) * | 0 (0.0) * | 2 (18.2) | 0 (0) | 0 (0) |
| Father’s academic level | |||||||
| Primary education | 210 (56.5) | 182 (57.8) | 28 (66.7) | 17 (85.0) *a | 3 (27.3) | 3 (60.0) | 5 (83.3) |
| Vocational education and training | 93 (25.0) | 84 (26.7) | 9 (21.4) | 3 (15.0) | 4 (36.4) | 1 (20.0) | 1 (16.7) |
| Bachelor’s degree | 27 (7.3) | 23 (7.3) | 4 (9.5) | 0 (0) a | 3 (27.3) * | 1 (20.0) | 0 (0) |
| Higher university degree | 30 (8.1) | 29 (9.2) | 1 (2.4) | 0 (0) | 1 (9.1) | 0 (0) | 0 (0) |
| Referral to Social Services | 37 (9.9) | 6 (1.9) | 31 (63.3) * | 19 (79.2) *a | 0 (0) c | 5 (83.3) * | 7 (87.5) * |
| Custody withdrawal | 7 (1.9) | 1 (0.3) | 6 (12.2) * | 3 (12.5) * | 0 (0) | 1 (16.7) * | 2 (25.0) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarque, P.; Roca, A.; Gomila, I.; Marchei, E.; Tittarelli, R.; Elorza, M.Á.; Sanchís, P.; Barceló, B. Role of Neonatal Biomarkers of Exposure to Psychoactive Substances to Identify Maternal Socio-Demographic Determinants. Biology 2021, 10, 296. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10040296
Jarque P, Roca A, Gomila I, Marchei E, Tittarelli R, Elorza MÁ, Sanchís P, Barceló B. Role of Neonatal Biomarkers of Exposure to Psychoactive Substances to Identify Maternal Socio-Demographic Determinants. Biology. 2021; 10(4):296. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10040296
Chicago/Turabian StyleJarque, Pilar, Antonia Roca, Isabel Gomila, Emilia Marchei, Roberta Tittarelli, Miguel Ángel Elorza, Pilar Sanchís, and Bernardino Barceló. 2021. "Role of Neonatal Biomarkers of Exposure to Psychoactive Substances to Identify Maternal Socio-Demographic Determinants" Biology 10, no. 4: 296. https://0-doi-org.brum.beds.ac.uk/10.3390/biology10040296