

Does Caffeine Supplementation Associated with Paralympic Powerlifting Training Interfere with Hemodynamic Indicators?

 ,
,  ,
,  , ,
, ,  , , , , ,
, , , , ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
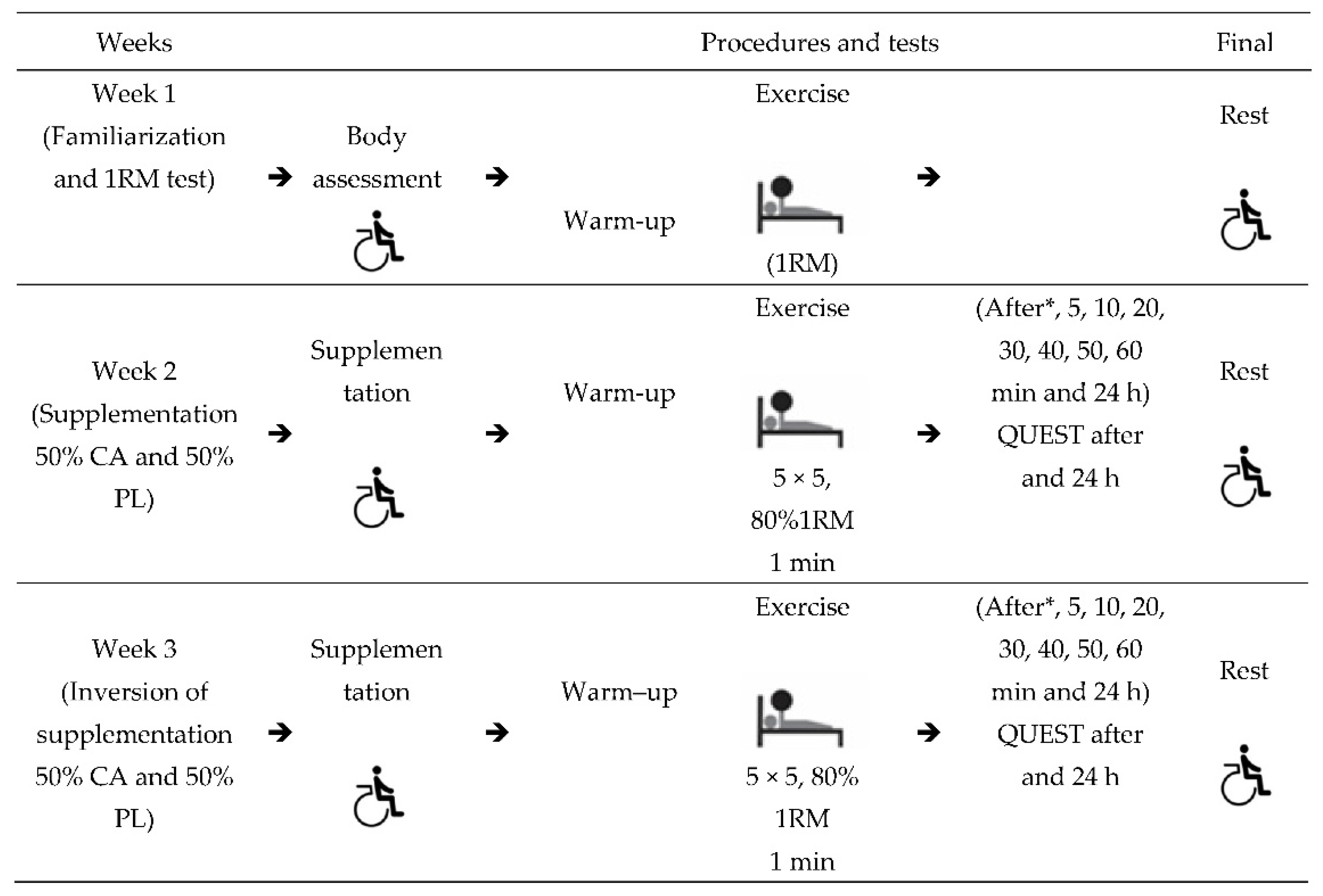
2.1. Study Design
2.2. Participants
2.3. Instruments
2.3.1. Caffeine Anhydrous (CA) and Placebo (PL)
2.3.2. Load Determination
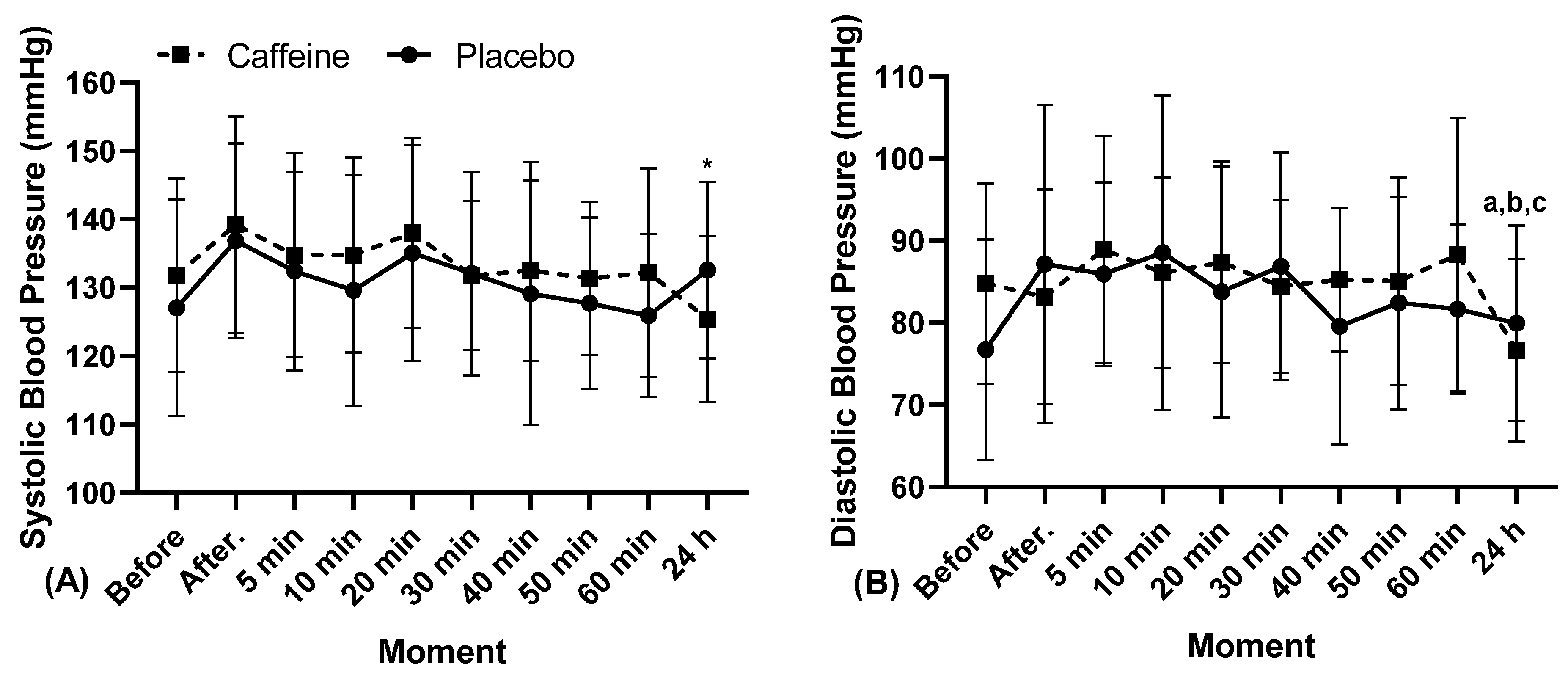
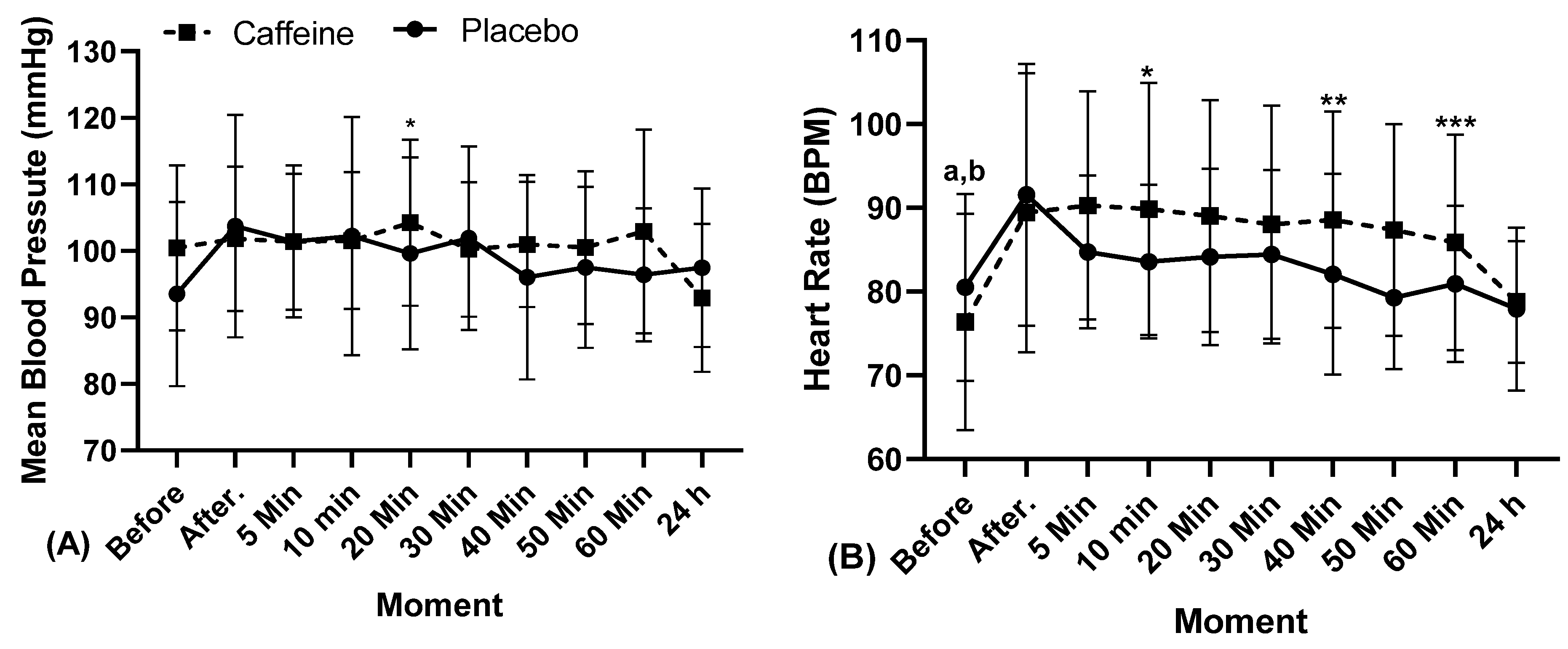
2.3.3. Blood Pressure and Heart Rate Measurement
2.3.4. Side Effects
2.4. Procedures
2.5. Statistical Analysis
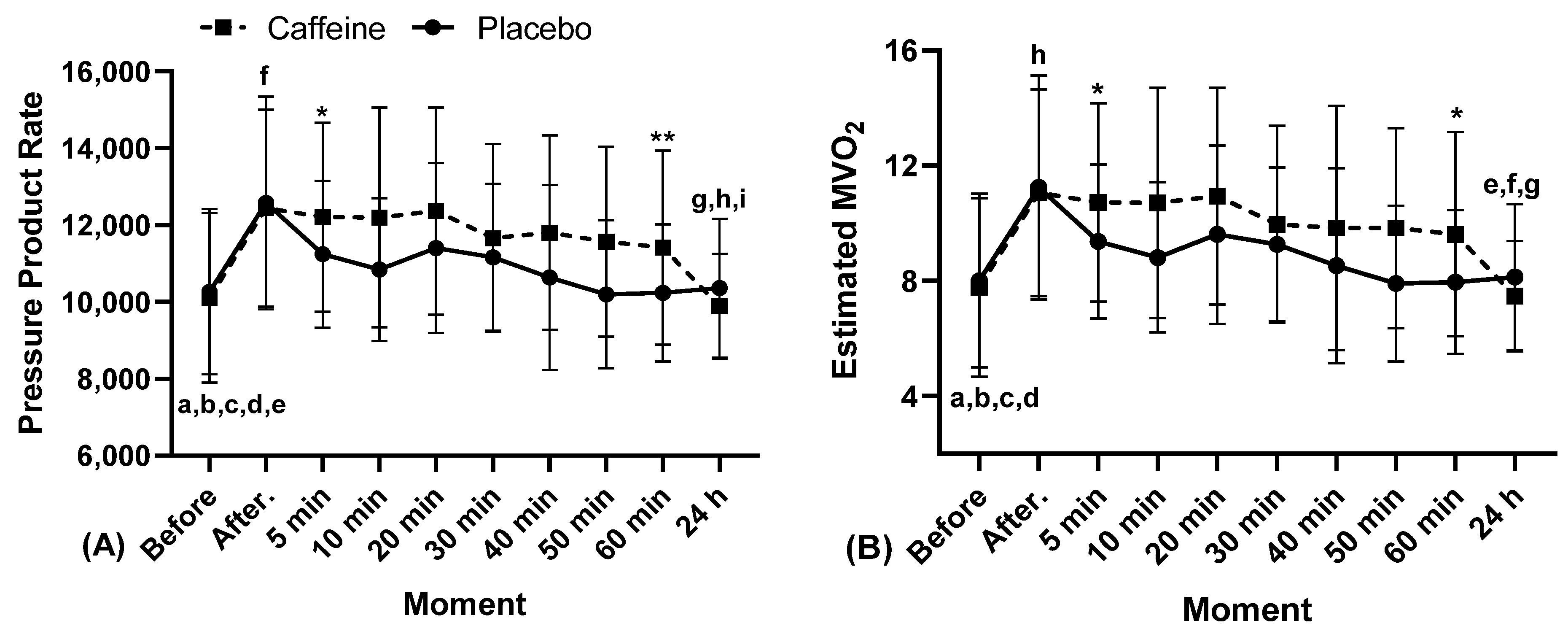
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benjamim, C.J.R.; Monteiro, L.R.L.; Pontes, Y.M.M. Caffeine slows heart rate autonomic recovery following strength exercise in healthy subjects. Rev. Port. Cardiol. 2021, 40, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Polito, M.; Farinatti, P.T.V. Heart-rate, blood pressure, and pressure product rateduring resistive exercises: A review of the literature. Port. J. Sport Sci. 2003, 3, 79–91. [Google Scholar]
- Aidar, F.J.; Paz, Â.; Gama, D.M.; de Souza, R.F.; Vieira Souza, L.M.; Santos, J.L.D.; Almeida-Neto, P.F.; Marçal, A.C.; Neves, E.B.; Moreira, O.C.; et al. Evaluation of the Post-Training Hypotensor Effect in Paralympic and Conventional Powerlifting. J. Funct. Morphol. Kinesiol. 2021, 6, 92. [Google Scholar] [CrossRef]
- Paz, Â.A.; Aidar, F.J.; De Matos, D.G.; De Souza, R.F.; Da Silva-Grigoletto, M.E.; Van den Tillaar, R.; Ramirez-Campillo, R.; Nakamura, F.Y.; Costa, M.; Nunes-Silva, A.; et al. Comparison of Post-Exercise Hypotension Responses in Paralympic Powerlifting Athletes after Completing Two Bench Press Training Intensities. Medicina 2020, 56, 156. [Google Scholar] [CrossRef] [Green Version]
- João, G.A.; Bocalini, D.S.; Rodriguez, D.; Charro, M.A.; Ceschini, F.; Martins, A.; Figueira Junior, A. Powerlifting sessions promote significant post-exercise hypotension. Rev. Bras. Med. Esporte 2017, 23, 118–122. [Google Scholar] [CrossRef] [Green Version]
- Casonatto, J.; Goessler, K.F.; Cornelissen, V.A.; Cardoso, J.R.; Polito, M.D. The blood pressure-lowering effect of a single bout of resistance exercise: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Prev. Cardiol. 2016, 23, 1700–1714. [Google Scholar] [CrossRef]
- Da Nóbrega, T.K.S.; Junior, J.S.M.; Alves, N.F.B.; Santos, A.C.; Silva, A.S. The coffee intake leads to abolition of aerobic exercise induced hypotension: A pilot study. J. Phys. Educ. 2011, 22, 601–612. [Google Scholar] [CrossRef] [Green Version]
- Astorino, T.A.; Martin, B.J.; Schachtsiek, L.; Wong, K. Caffeine ingestion and intense resistance training minimize postexercise hypotension in normotensive and prehypertensive men. Res. Sports Med. 2013, 21, 52–65. [Google Scholar] [CrossRef]
- Da Nóbrega, T.K.S.; Brasileiro-Santos, M.S.; Dantas, F.F.O.D.; De Lima, P.F.M.; Da Silva, F.T.M.; Brito, A.F.; Santos, A.C. Effect of Caffeine on Hemodynamics and Autonomics Parameters in Hypertensive Women after Aerobic Exercise. Motricidade 2017, 13, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Santos, Y.W.T.d.; Pereira, B.B.; Vieira, S.C.R.; Alves, C.D.P.; Sousa, A.M.M.d.; Sampaio, A.M.C.T.; Junior, L.S.L.; Marques, A.d.A. Effect of caffeine on post-exercise hypotensive response: A literature review. Rev. Ciênc. 2017, 5, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Cazé, R.F.; Franco, G.A.M.; Porpino, S.K.P.; De Souza, A.A.; Padilhas, O.P.; Silva, A.S. Caffeine influence on blood pressure response to aerobic exercise in hypertensive subjects. Rev. Bras. Med. Esporte 2010, 16, 324–328. [Google Scholar] [CrossRef]
- Júnior, F.A.; Gomes, S.G.; da Silva, F.F.; Souza, P.M.; Oliveira, E.C.; Coelho, D.B.; Nascimento-Neto, R.M.; Lima, W.; Becker, L.K. The effects of aquatic and land exercise on resting blood pressure and post-exercise hypotension response in elderly hypertensives. Cardiovasc. J. Afr. 2020, 31, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sport 2015, 25, 1–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brito, A.F.; Alves, N.F.; Araújo, A.S.; Gonçalves, M.C.; Silva, A.S. Active intervals between sets of resistance exercises potentiate the magnitude of postexercise hypotension in elderly hypertensive women. J. Strength Cond. Res. 2011, 25, 3129–3136. [Google Scholar] [CrossRef]
- Mohammedi, K.; Potier, L.; Belhatem, N.; Matallah, N.; Hadjadj, S.; Roussel, R.; Marre, M.; Velho, G. Lower-extremity amputation as a marker for renal and cardiovascular events and mortality in patients with long standing type 1 diabetes. Cardiovasc. Diabetol. 2016, 15, 5. [Google Scholar] [CrossRef] [Green Version]
- International Paralympic Committee. Para Powerlifting Rules. Available online: www.paralympic.org/powerlifting/rules (accessed on 10 May 2022).
- Materko, W.; Santos, E.L. Acute effect of caffeine supplementation on performance of muscular strength and cardiovascular changes during resistance training. Motricidade 2011, 7, 29–36. [Google Scholar]
- Soares Freitas Sampaio, C.R.; Aidar, F.J.; Ferreira, A.R.P.; Santos, J.L.D.; Marçal, A.C.; Matos, D.G.; Souza, R.F.; Moreira, O.C.; Guerra, I.; Fernandes Filho, J.; et al. Can Creatine Supplementation Interfere with Muscle Strength and Fatigue in Brazilian National Level Paralympic Powerlifting? Nutrients 2020, 12, 2492. [Google Scholar] [CrossRef]
- Delleli, S.; Ouergui, I.; Messaoudi, H.; Trabelsi, K.; Ammar, A.; Glenn, J.M.; Chtourou, H. Acute Effects of Caffeine Supplementation on Physical Performance, Physiological Responses, Perceived Exertion, and Technical-Tactical Skills in Combat Sports: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 2996. [Google Scholar] [CrossRef]
- Chtourou, H.; Trabelsi, K.; Ammar, A.; Shephard, R.J.; Bragazzi, N.L. Acute Effects of an “Energy Drink” on Short-Term Maximal Performance, Reaction Times, Psychological and Physiological Parameters: Insights from a Randomized Double-Blind, Placebo-Controlled, Counterbalanced Crossover Trial. Nutrients 2019, 11, 992. [Google Scholar] [CrossRef] [Green Version]
- França, V.F.; Malfatti, C.R.M.; Silva, L.A.; Wietzikoski, E.C.; Osiecki, A.; Osiecki, R. Effect of acute caffeine supplementation in biochemical response during endurance exercise in rats. Rev. Bras. Med. Esporte 2015, 21, 372–375. [Google Scholar] [CrossRef] [Green Version]
- De Almeida, D.V.P.; Pereira, N.K.; Moreira, D.A.R. Cardiovascular EffectsofCaffeine: Literature Review. Rev. Ciênc. Saúde 2013, 3, 5–7. [Google Scholar]
- Sampaio-Jorge, F.; Morales, A.P.; Pereira, R.; Barth, T.; Ribeiro, B.G. Caffeine increases performance and leads to a cardioprotective effect during intense exercise in cyclists. Sci. Rep. 2021, 11, 24327. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, R.; Goessler, K.; Rissardi, L.; Araújo, A.; Polito, M. Caffeine Intake and Cardiovascular Responses after Resistance Exercise Session. Rev. Bras. Cardiol. 2011, 24, 112–115. [Google Scholar]
- Ruiz, R.; Ramos, S.P.; Pinge, M.M.; Moraes, S.F.; Polito, M. Caffeine and physical training: Effects on cardiac morphology and cardiovascular response. Rev. Assoc. Med. Bras. 2014, 60, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Bunsawat, K.; White, D.W.; Kappus, R.M.; Baynard, T. Caffeine delays autonomic recovery following acute exercise. Eur. J. Prev. Cardiol. 2015, 22, 1473–1479. [Google Scholar] [CrossRef]
- Buchanan, S.R.; Karabulut, M. A caffeine containing weight loss supplement augments hemodynamic responses after exercise. Int. J. Cardiol. 2018, 253, 133–137. [Google Scholar] [CrossRef]
- Austin, D.; Mann, B. Powerlifting: The Complete Guide to Technique, Training, and Competition; Human Kinetics: Champaign, IL, USA, 2012; ISBN 9781492598800. [Google Scholar]
- Durkalec-Michalski, K.; Nowaczyk, P.M.; Główka, N.; Grygiel, A. Dose-dependent effect of caffeine supplementation on judo-specific performance and training activity: A randomized placebo-controlled crossover trial. J. Int. Soc. Sports Nutr. 2019, 16, 38. [Google Scholar] [CrossRef] [Green Version]
- Topouchian, J.A.; El Assaad, M.A.; Orobinskaia, L.V.; El Feghali, R.N.; Asmar, R.G. Validation of two devices for self-measurement of brachial blood pressure according to the International Protocol of the European Society of Hypertension: The SEINEX SE-9400 and the Microlife BP 3AC1-1. Blood Press. Monit. 2005, 10, 325–331. [Google Scholar] [CrossRef]
- Wilk, M.; Filip, A.; Krzysztofik, M.; Maszczyk, A.; Zajac, A. The Acute Effect of Various Doses of Caffeine on Power Output and Velocity during the Bench Press Exercise among Athletes Habitually Using Caffeine. Nutrients 2019, 11, 1465. [Google Scholar] [CrossRef] [Green Version]
- Pallarés, J.G.; Fernández-Elías, V.E.; Ortega, J.F.; Muñoz, G.; Muñoz-Guerra, J.; Mora-Rodríguez, R. Neuromuscular Responses to Incremental Caffeine Doses: Performance and Side Effects. Med. Sci. Sports Exerc. 2013, 45, 2184–2192. [Google Scholar] [CrossRef]
- Fleck, S.J.; Kraemer, W.J. Projetando Programas de Treinamento de Resistência, 4th ed.; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Hellerstein, H.K.; Wenger, N.K. Rehabilitation of the Coronary Patients; John Wiley and Sons: New York, NY, USA, 1978. [Google Scholar]
- Barroso, W.K.S.; Rodrigues, C.I.S.; Bortolotto, L.A.; Mota-Gomes, M.A.; Brandão, A.A.; de Magalhães Feitosa, A.D.; Machado, C.A.; Poli-de-Figueiredo, C.E.; Amodeo, C.; Mion Júnior, D.; et al. Diretrizes Brasileiras de Hipertensão Arterial—2020. Arq. Bras. Cardiol. 2021, 116, 516–658. [Google Scholar] [CrossRef] [PubMed]
- Simões, C.B.; Gomes, P.L.C.; Silva, R.A.D.; Fonseca, I.C.S.; Fonseca, M.; Cruz, V.M.; Drummond, M.D.M. Acute caffeine and capsaicin supplementation and performance in resistance training. Mot. Rev. Educ. Física 2022, 28, e1021010121. [Google Scholar] [CrossRef]
- Cohen, J. Statistics a power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Gonzaga, L.A.; Vanderlei, L.C.M.; Gomes, R.L.; Valenti, V.E. Caffeine affects autonomic control of heart rate and blood pressure recovery after aerobic exercise in young adults: A crossover study. Sci. Rep. 2017, 7, 14091. [Google Scholar] [CrossRef]
- Wikoff, D.; Welsh, B.T.; Henderson, R.; Brorby, G.P.; Britt, J.; Myers, E.; Goldberger, J.; Lieberman, H.R.; O’Brien, C.; Peck, J.; et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem. Toxicol. 2017, 109, 585–648. [Google Scholar] [CrossRef] [PubMed]
- Barcelos, R.P.; Lima, F.D.; Carvalho, N.R.; Bresciani, G.; Royes, L.F. Caffeine effects on systemic metabolism, oxidative-inflammatory pathways, and exercise performance. Nutr. Res. 2020, 80, 1–17. [Google Scholar] [CrossRef]
- Sarshin, A.; Naderi, A.; da Cruz, C.J.G.; Feizolahi, F.; Forbes, S.C.; Candow, D.G.; Mohammadgholian, E.; Amiri, M.; Jafari, N.; Rahimi, A.; et al. The effects of varying doses of caffeine on cardiac parasympathetic reactivation following an acute bout of anaerobic exercise in recreational athletes. J. Int. Soc. Sports Nutr. 2020, 17, 44. [Google Scholar] [CrossRef]
- Souza, D.; Casonatto, J.; Poton, R.; Willardson, J.; Polito, M. Acute effect of caffeine intake on hemodynamics after resistance exercise in young non-hypertensive subjects. Res. Sports Med. 2014, 22, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Apostolidis, A.; Mougios, V.; Smilios, I.; Rodosthenous, J.; Hadjicharalambous, M. Caffeine Supplementation: Ergogenic in Both High and Low Caffeine Responders. Int. J. Sport Physiol. 2019, 14, 650–657. [Google Scholar] [CrossRef]
- Brothers, R.M.; Christmas, K.M.; Patik, J.C.; Bhella, P.S. Heart rate, blood pressure and repolarization effects of an energy drink as compared to coffee. Clin. Physiol. Funct. Imaging 2017, 37, 675–681. [Google Scholar] [CrossRef]
- Aidar, F.J.; Dantas, E.F.; Almeida-Neto, P.F.; Neto, F.R.; Garrido, N.D.; Cabral, B.G.; Figueiredo, T.; Reis, V.M. Can Post-Exercise Hemodynamic Response Be Influenced by Different Recovery Methods in Paraplegic Sportsmen? Int. J. Environ. Res. Public Health 2022, 19, 1772. [Google Scholar] [CrossRef] [PubMed]
- Da Nóbrega, T.K.S.; Brasileiro-Santos, M.S.; Brito, L.F.; Oliveira, A.S.; Santos, A.C. Caffeine and Physical Exercise: A Systematic Review on Hemodynamic Aspects. Rev. Bras. Ciênc. Saúde 2011, 15, 95–102. [Google Scholar] [CrossRef]
- Antonio, T.T.D.; De Assis, M.R. Double-product and heart rate variation after isokinetic exercise in adults and elderly. Rev. Bras. Med. Esporte 2017, 23, 394–398. [Google Scholar] [CrossRef] [Green Version]
- Barbosa, D.J.N.; Pereira, L.N.; Cardoso, M.I.; Pereira, R.; Machado, M. Effect of caffeine on RAST performance and hemodynamic variables: A placebo-controlled study. Mov. Percept. 2008, 9, 75–93. [Google Scholar]
- Monteiro, B.M.; De Oliveira, A.A.R.; Neto, P.P. The use of the double product as a subjective marker of resistance exercise exertion for hypertensive patients. Motricidade 2018, 14, 87–90. [Google Scholar]
- Fornitano, L.D.; Godoy, M.F.D. High double product as a predictor of absence of major obstructive coronary artery disease in patients with a positive exercise stress test. Arq. Bras. Cardiol. 2006, 86, 139–144. [Google Scholar]
- Andrade, F.M.; Barbosa Júnior, A.O.; Pulcinelli, A.J. Comparative study of the double product in strength training in ascending and descending pyramidal series. Life Health 2002, 1, 1–9. [Google Scholar]
- Wilk, M.; Krzysztofik, M.; Filip, A.; Zajac, A.; Del Coso, J. The Effects of High Doses of Caffeine on Maximal Strength and Muscular Endurance in Athletes Habituated to Caffeine. Nutrients 2019, 11, 1912. [Google Scholar] [CrossRef]
- Bento, V.F.R.; Albino, F.B.; de Moura, K.F.; Maftum, G.J.; de Castro dos Santos, M.; Guarita-Souza, L.C.; Faria Neto, J.R.; Baena, C.P. Impact of physical activity interventions on blood pressure in Brazilian populations. Arq. Bras. Cardiol. 2015, 105, 301–308. [Google Scholar] [CrossRef]
- Bakker, E.A.; Sui, X.; Brellenthin, A.G.; Lee, D.C. Physical activity and fitness for the prevention of hypertension. Curr. Opin. Cardiol. 2018, 33, 394–401. [Google Scholar] [CrossRef]
- Grinberg, N.; Benkhedda, K.; Barber, J.; Krahn, A.D.; La Vieille, S. Effects of caffeinated energy drinks on cardiovascular responses during exercise in healthy adults: A systematic review and meta-analysis of randomized controlled trials. Appl. Physiol. Nutr. Metab. 2022, 47, 618–631. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Abdalla, M.A.; Zakhary, C.M.; Rushdi, H.; Hamdan, J.A.; Youssef, K.N.; Khan, S. The Relationship Between Caffeine and Caffeinated Drinks in Causing Intracranial Hemorrhage in the Elderly Aspirin-Taking Population: A Systematic Review. Cureus 2021, 9, 17783. [Google Scholar] [CrossRef]
- Surma, S.; Oparil, S. Coffee and Arterial Hypertension. Curr. Hypertens. Rep. 2021, 7, 38. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez-Hellín, J.; Varillas-Delgado, D. Energy Drinks and Sports Performance, Cardiovascular Risk, and Genetic Associations: Future Prospects. Nutrients 2021, 3, 715. [Google Scholar] [CrossRef] [PubMed]
- Kerrigan, S.; Lindsey, T. Fatal caffeine overdose: Two case reports. Forensic Sci. Int. 2005, 153, 67–69. [Google Scholar] [CrossRef] [PubMed]
- Sepkowitz, K.A. Energy drinks and caffeine-related adverse effects. JAMA 2013, 309, 243–244. [Google Scholar] [CrossRef]
- Parker, J.L.; Oltman, C.L.; Muller, J.M.; Myers, P.R.; Adams, H.R.; Laughlin, M.H. Effects of exercise training on regulation of tone in coronary arteries and arterioles. Med. Sci. Sports Exerc. 1994, 10, 1252–1261. [Google Scholar] [CrossRef]
- Porto, A.A.; Benjamim, C.J.R.; Gonzaga, L.A.; Luciano de Almeida, M.; Bueno Júnior, C.R.; Garner, D.M.; Valenti, V.E. Caffeine intake and its influences on heart rate variability recovery in healthy active adults after exercise: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1071–1082. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Features | (Mean ± SD) |
|---|---|
| Age (years) | 32.4 ± 8.5 |
| Body mass (kg) | 81.7 ± 21.9 |
| Experience (years) | 3.1 ± 1.0 |
| Systolic blood pressure (mmHg) | 126 ± 15 |
| Diastolic blood pressure (mmHg) | 75 ± 12 |
| 1RM test (bench press) (kg) | 126.9 ± 41.2 |
| 1RM test/body mass (kg) | 1.6 ± 0.4 |
| Side Effects | After | 24 H |
|---|---|---|
| Headache | 0 (0%) | 3 (21%) |
| Abdominal/gastrointestinal pain | 0 (0%) | 0 (0%) |
| Muscle pain | 6 (43%) | 5 (36%) |
| Increased energy and strength | 11 (79%) | 10 (71%) |
| Tachycardia/palpitations | 1 (7%) | 0 (0%) |
| Insomnia | 1 (7%) | 1 (7%) |
| Performance improvement | 13 (93%) | 9 (64%) |
| Increased production and elimination of urine | 4 (29%) | 3 (21%) |
| Increased worry/anxiety | 0 (0%) | 1 (7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menezes, J.L.; Aidar, F.J.; Badicu, G.; Cataldi, S.; Carvutto, R.; Silva, A.F.; Clemente, F.M.; Cerulli, C.; de Jesus, J.B.; Vieira-Souza, L.M.; et al. Does Caffeine Supplementation Associated with Paralympic Powerlifting Training Interfere with Hemodynamic Indicators? Biology 2022, 11, 1843. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11121843
Menezes JL, Aidar FJ, Badicu G, Cataldi S, Carvutto R, Silva AF, Clemente FM, Cerulli C, de Jesus JB, Vieira-Souza LM, et al. Does Caffeine Supplementation Associated with Paralympic Powerlifting Training Interfere with Hemodynamic Indicators? Biology. 2022; 11(12):1843. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11121843
Chicago/Turabian StyleMenezes, Jainara Lima, Felipe J. Aidar, Georgian Badicu, Stefania Cataldi, Roberto Carvutto, Ana Filipa Silva, Filipe Manuel Clemente, Claudia Cerulli, Joseane Barbosa de Jesus, Lucio Marques Vieira-Souza, and et al. 2022. "Does Caffeine Supplementation Associated with Paralympic Powerlifting Training Interfere with Hemodynamic Indicators?" Biology 11, no. 12: 1843. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11121843